Phosphatidylethanol in Blood as a Marker of Chronic Alcohol Use: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Results and Discussion
- – The formation, distribution and degradation of PEth in human blood (Section 2.1);
- – The presence and distribution of different PEth molecular species in human blood (Section 2.2);
- – The most diffused and efficient analytical methods devoted to the identification and quantisation of PEth in human blood (Section 2.3);
- – The diagnostic efficiency of PEth as a clinical marker of chronic excessive drinking (Section 2.4);
- – The potential utility of PEth as a marker of heavy episodic drinking or binge drinking (Section 2.5).
2.1. Phosphatidylethanol Definition, Formation and Degradation
2.1.1. PEth Formation Mechanism
2.1.2. PEth Formation in Human Blood
2.1.3. PEth Degradation Mechanism
2.1.4. PEth Degradation in Human Blood
2.2. Phosphatidylethanol Molecular Species
2.3. Analytical Techniques and Methods for PEth Identification and Quantization in Blood
- – Gas-chromatography coupled to mass spectrometry [63].
2.4. Diagnostic Efficiency of PEth as a Clinical Marker of Chronic Excessive Drinking
2.5. PEth as a Potential Marker of Heavy Episodic Drinking or “Binge Drinking”
3. Experimental Section
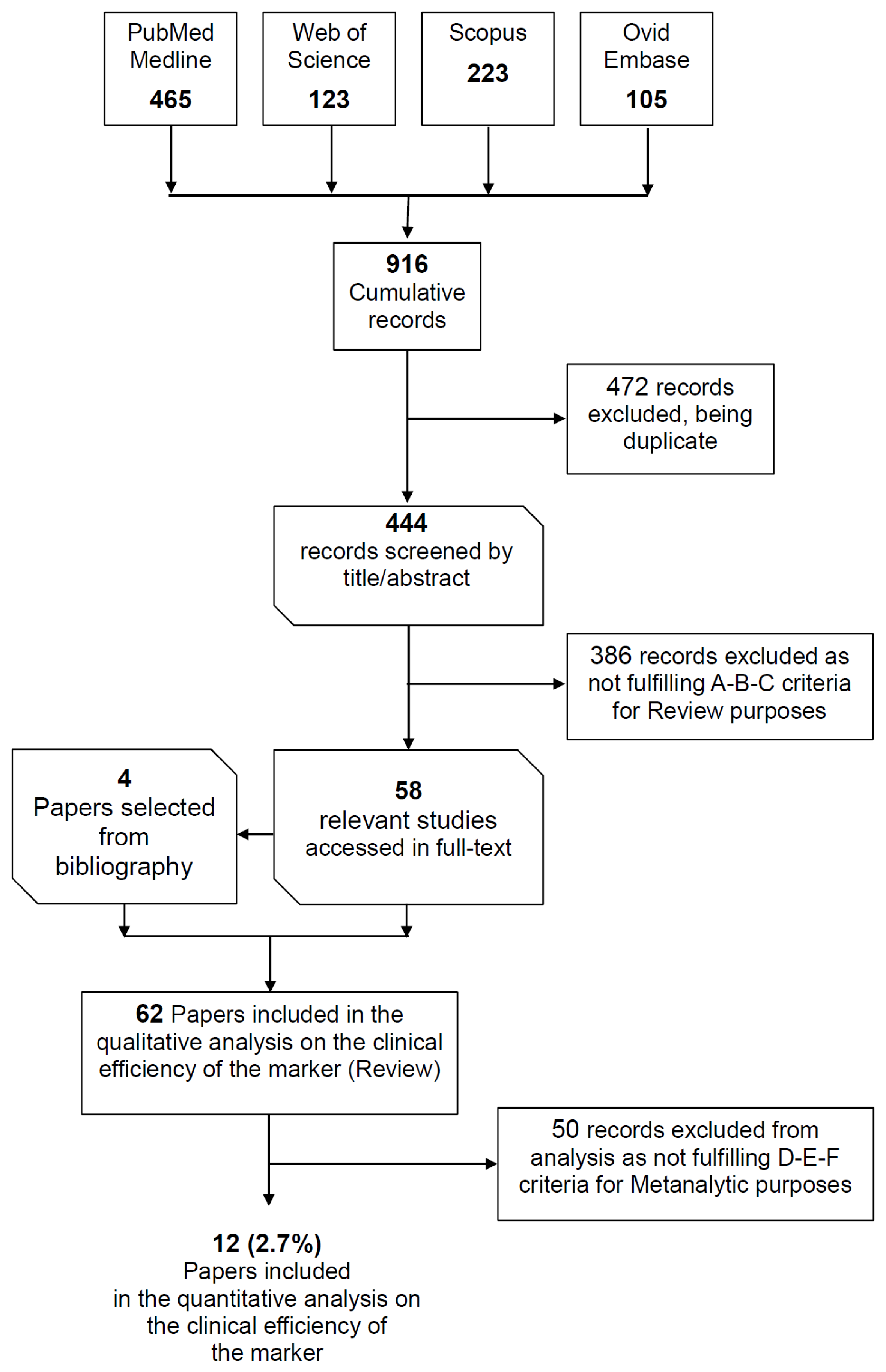
3.1. Search Strategy
3.2. Paper Selection
3.2.1. Inclusion criteria for review purposes
- Provide data on PEth concentration in human blood collected from alcohol dependent subjects, heavy drinkers, moderate drinkers, social drinkers or teetotalers.
- Provide data on PEth concentration in fluids or tissues of animals chronically exposed to ethanol.
- Describe an analytical method for the quantification of total PEth or PEth molecular species in human blood.
3.2.2. Exclusion criteria for review purposes
3.2.3. Inclusion criteria for meta-analytic purposes
- (D) Fulfilling criterion A for Review purposes.
- (E) Reporting integrable data on blood concentrations of PEth in humans.
- (F) Reporting integrable data on the daily alcohol intake (DAI) of the subjects recruited in the study.
3.2.4. Exclusion criteria for meta-analytic purposes
3.3. Data Extraction
- Category 1. Social drinkers (DAI ≤ 60 g).
- Category 2. Heavy drinkers (DAI > 60 g).
3.4. Statistical Analysis
4. Conclusions
- Define the molecular species of PEth that should be determined in blood when a mass spectrometric analytical method is used; it needs to be clarified if PEth 16:0/18:1 and 16:0/18:2 (the two most abundant homologues) are sufficient to resemble the total PEth concentration or whether it would be more appropriate to investigate and quantify multiple PEth molecular species; the data derived from our analysis suggest that at least 5 molecular species (PEth 16:0/18:1, 16:0/18:2, 16:0/20:4, 18:1/18:1, 18:1/18:2) could be used.
- Develop and market commercial reference substances for the PEth molecular species identified by point 1.
- Arrive at a consensus on the most appropriate cut-off for differentiating social alcohol use from heavy drinking.
- Characterize the kinetics of formation and degradation of the identified PEth species in order to determine whether they might be used for monitoring abstinence.
- Verify the correlation of blood PEth concentration with the amount of ethanol ingested in the previous two weeks.
Acknowledgments
- Conflict of InterestThe authors declare no conflict of interest.
- Authors’ ContributionG.V. and R.-B.B. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the analysis.Study concept and design: G.V. (concept); R.-B.B (design).Acquisition of data: G.V. (systematic search); R.-B.B, G.V., A.N., P.F. (data extraction and database construction); G.C., S.-D.F. (accuracy check).Analysis and interpretation of data: R.-B.B.Drafting of the manuscript: G.V., R.-B.B., G.C.Critical revision of the manuscript for important intellectual content: S.-D.F.Statistical analysis: R.-B.B.Obtaining funding: Grant n. 60A07-9371/12 of the University of Padova.Administrative, technical, or material support: None.Other (specify): None.
References
- Domino, K.B.; Hornbein, T.F.; Polissar, N.L.; Renner, G.; Johnson, J.; Alberti, S.; Hankes, L. Risk factors for relapse in health care professionals with substance use disorders. JAMA 2005, 293, 1453–1460. [Google Scholar]
- Li, T.K. Quantifying the risk for alcohol-use and alcohol-attributable health disorders: Present findings and future research needs. J. Gastroenterol. Hepatol 2008, 23, S2–S8. [Google Scholar]
- Ferrara, S.D.; Bajanowski, T.; Cecchi, R.; Boscolo-Berto, R.; Viel, G. Bio-medicolegal scientific research in Europe: A comprehensive bibliometric overview. Int. J. Legal. Med 2011, 125, 393–402. [Google Scholar]
- Ferrara, S.D.; Bajanowski, T.; Cecchi, R.; Snenghi, R.; Case, C.; Viel, G. Bio-medicolegal guidelines and protocols: Survey and future perspectives in Europe. Int. J. Legal. Med 2010, 124, 345–350. [Google Scholar]
- Bradley, K.A.; DeBenedetti, A.F.; Volk, R.J.; Williams, E.C.; Frank, D.; Kivlahan, D.R. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol. Clin. Exp. Res 2007, 31, 1208–1217. [Google Scholar]
- Ewing, J.A. Detecting alcoholism. The CAGE questionnaire. JAMA 1984, 252, 1905–1907. [Google Scholar]
- Ferrara, S.D. Alcohol, drugs and traffic safety. Br. J. Addict 1987, 82, 871–883. [Google Scholar]
- Favretto, D.; Nalesso, A.; Frison, G.; Viel, G.; Traldi, P.; Ferrara, S.D. A novel and an effective analytical approach for the LC-MS determination of ethyl glucuronide and ethyl sulfate in urine. Int. J. Legal Med 2010, 124, 161–164. [Google Scholar]
- Conigrave, K.M.; Degenhardt, L.J.; Whitfield, J.B.; Saunders, J.B.; Helander, A.; Tabakoff, B. CDT, GGT, and AST as markers of alcohol use: The WHO/ISBRA collaborative project. Alcohol. Clin. Exp. Res 2002, 26, 332–339. [Google Scholar]
- Musshoff, F. Chromatographic methods for the determination of markers of chronic and acute alcohol consumption. J. Chromatogr. B 2002, 781, 457–480. [Google Scholar]
- Bortolotti, F.; de Paoli, G.; Tagliaro, F. Carbohydrate-deficient transferrin (CDT) as a marker of alcohol abuse: A critical review of the literature 2001–2005. J. Chromatogr. B 2006, 841, 96–109. [Google Scholar]
- Golka, K.; Wiese, A. Carbohydrate-deficient transferrin (CDT)—A biomarker for long-term alcohol consumption. J. Toxicol. Environ. Health B 2004, 7, 319–337. [Google Scholar]
- Favretto, D.; Nalesso, A.; Frison, G.; Viel, G.; Traldi, P.; Ferrara, S.D. No-discharge atmospheric pressure chemical ionization mass spectrometry of ethyl glucuronide and ethyl sulfate. J. Mass Spectrom 2010, 45, 121–124. [Google Scholar]
- Hoiseth, G.; Morini, L.; Polettini, A.; Christophersen, A.; Morland, J. Ethyl glucuronide in hair compared with traditional alcohol biomarkers—A pilot study of heavy drinkers referred to an alcohol detoxification unit. Alcohol. Clin. Exp. Res 2009, 33, 812–816. [Google Scholar]
- Litten, R.Z.; Bradley, A.M.; Moss, H.B. Alcohol biomarkers in applied settings: Recent advances and future research opportunities. Alcohol. Clin. Exp. Res 2010, 34, 955–967. [Google Scholar]
- Bordignon, M.; Viel, G.; Peserico, A.; Alaibac, M. Non-alcoholic fatty liver disease, alcohol intake and psoriasis. J. Hepatol 2010, 53, 587. [Google Scholar]
- Alling, C.; Gustavsson, L.; Anggard, E. An abnormal phospholipid in rat organs after ethanol. FEBS Lett 1983, 152, 24–28. [Google Scholar]
- Alling, C.; Gustavsson, L.; Mansson, J.E.; Benthin, G.; Anggard, E. Phosphatidylethanol formation in rat organs after ethanol treatment. Biochim. Biophys. Acta 1984, 793, 119–122. [Google Scholar]
- Benthin, G.; Anggard, E.; Gustavsson, L.; Alling, C. Formation of phosphatidylethanol in frozen kidneys from ethanol-treated rats. Biochim. Biophys. Acta 1985, 835, 385–389. [Google Scholar]
- Gustavsson, L.; Alling, C. Formation of phosphatidylethanol in rat brain by phospholipase D. Biochem. Biophys. Res. Commun 1987, 142, 958–963. [Google Scholar]
- Lundqvist, C.; Aradottir, S.; Alling, C.; Boyano-Adanez, M.C.; Gustavsson, L. Phosphatidylethanol formation and degradation in brains of acutely and repeatedly ethanol-treated rats. Neurosci. Lett 1994, 179, 127–131. [Google Scholar]
- Gustavsson, L.; Moehren, G.; Hoek, J.B. Phosphatidylethanol formation in rat hepatocytes. Ann. N. Y. Acad. Sci 1991, 625, 438–440. [Google Scholar]
- Kobayashi, M.; Kanfer, J.N. Phosphatidylethanol formation via transphosphatidylation by rat brain synaptosomal phospholipase D. J. Neurochem 1987, 48, 1597–1603. [Google Scholar]
- Mueller, G.C.; Fleming, M.F.; LeMahieu, M.A.; Lybrand, G.S.; Barry, K.J. Synthesis of phosphatidylethanol—A potential marker for adult males at risk for alcoholism. Proc. Natl. Acad. Sci. USA 1988, 85, 9778–9782. [Google Scholar]
- Gustavsson, L. ESBRA 1994 Award Lecture. Phosphatidylethanol formation: specific effects of ethanol mediated via phospholipase D. Alcohol Alcohol 1995, 30, 391–406. [Google Scholar]
- Colley, W.C.; Sung, T.C.; Roll, R.; Jenco, J.; Hammond, S.M.; Altshuller, Y.; Bar-Sagi, D.; Morris, A.J.; Frohman, M.A. Phospholipase D2, a distinct phospholipase D isoform with novel regulatory properties that provokes cytoskeletal reorganization. Curr. Biol 1997, 7, 191–201. [Google Scholar]
- Steed, P.M.; Clark, K.L.; Boyar, W.C.; Lasala, D.J. Characterization of human PLD2 and the analysis of PLD isoform splice variants. FASEB J 1998, 12, 1309–1317. [Google Scholar]
- Vinggaard, A.M.; Hansen, H.S. Bradykinin and vasopressin activate phospholipase D in rat Leydig cells by a protein kinase C-dependent mechanism. J. Endocrinol 1993, 136, 119–126. [Google Scholar]
- Shukla, S.D.; Sun, G.Y.; Wood, W.G.; Savolainen, M.J.; Alling, C.; Hoek, J.B. Ethanol and lipid metabolic signaling. Alcohol. Clin. Exp. Res 2001, 25, 33S–39S. [Google Scholar]
- Lundqvist, C.; Alling, C.; Aradottir, S.; Gustavsson, L. Agonist-stimulated and basal phosphatidylethanol formation in neutrophils from alcoholics. Alcohol. Clin. Exp. Res 1994, 18, 580–586. [Google Scholar]
- Magai, R.M.; Shukla, S.D. Metabolic fate of [14C]-ethanol into endothelial cell phospholipids including platelet-activating factor, sphingomyelin and phosphatidylethanol. J. Biomed. Sci 2001, 8, 143–150. [Google Scholar]
- Aradottir, S.; Moller, K.; Alling, C. Phosphatidylethanol formation and degradation in human and rat blood. Alcohol Alcohol 2004, 39, 8–13. [Google Scholar]
- Aradottir, S.; Lundqvist, C.; Alling, C. Phosphatidylethanol in rat organs after ethanol exposure. Alcohol. Clin. Exp. Res 2002, 26, 514–518. [Google Scholar]
- Isaksson, A.; Walther, L.; Hansson, T.; Andersson, A.; Alling, C. Phosphatidylethanol in blood (B-PEth): A marker for alcohol use and abuse. Drug Test Anal 2011, 3, 195–200. [Google Scholar]
- Selle, H.; Chapman, B.E.; Kuchel, P.W. Release of choline by phospholipase D and a related phosphoric diester hydrolase in human erythrocytes. 1H spin-echo n.m.r. studies. Biochem. J 1992, 284, 61–65. [Google Scholar]
- Metz, S.A.; Dunlop, M. Production of phosphatidylethanol by phospholipase D phosphatidyl transferase in intact or dispersed pancreatic islets: Evidence for the in situ metabolism of phosphatidylethanol. Arch. Biochem. Biophys 1990, 283, 417–428. [Google Scholar]
- Bruhl, A.; Faldum, A.; Loffelholz, K. Degradation of phosphatidylethanol counteracts the apparent phospholipase D-mediated formation in heart and other organs. Biochim. Biophys. Acta 2003, 1633, 84–89. [Google Scholar]
- Moehren, G.; Gustavsson, L.; Hoek, J.B. Activation and desensitization of phospholipase D in intact rat hepatocytes. J. Biol. Chem 1994, 269, 838–848. [Google Scholar]
- Pai, J.K.; Liebl, E.C.; Tettenborn, C.S.; Ikegwuonu, F.I.; Mueller, G.C. 12-O-tetradecanoylphorbol-13-acetate activates the synthesis of phosphatidylethanol in animal cells exposed to ethanol. Carcinogenesis 1987, 8, 173–178. [Google Scholar]
- Aradottir, S.; Asanovska, G.; Gjerss, S.; Hansson, P.; Alling, C. PHosphatidylethanol (PEth) concentrations in blood are correlated to reported alcohol intake in alcohol-dependent patients. Alcohol Alcohol 2006, 41, 431–437. [Google Scholar]
- Hansson, P.; Caron, M.; Johnson, G.; Gustavsson, L.; Alling, C. Blood phosphatidylethanol as a marker of alcohol abuse: Levels in alcoholic males during withdrawal. Alcohol Clin. Exp. Res 1997, 21, 108–110. [Google Scholar]
- Hartmann, S.; Aradottir, S.; Graf, M.; Wiesbeck, G.; Leech, O.; Ramskogler, K.; Wolfersdorf, M.; Alling, C.; Wurst, F.M. Phosphatidylethanol as a sensitive and specific biomarker: Comparison with gamma-glutamyl transpeptidase, mean corpuscular volume and carbohydrate-deficient transferrin. Addict. Biol 2007, 12, 81–84. [Google Scholar]
- Varga, A.; Hansson, P.; Lundqvist, C.; Alling, C. Phosphatidylethanol in blood as a marker of ethanol consumption in healthy volunteers: comparison with other markers. Alcohol. Clin. Exp. Res 1998, 22, 1832–1837. [Google Scholar]
- Wurst, F.M.; Alexson, S.; Wolfersdorf, M.; Bechtel, G.; Forster, S.; Alling, C.; Aradottir, S.; Jachau, K.; Huber, P.; Allen, J.P.; et al. Concentration of fatty acid ethyl esters in hair of alcoholics: Comparison to other biological state markers and self reported-ethanol intake. Alcohol Alcohol 2004, 39, 33–38. [Google Scholar]
- Wurst, F.M.; Thon, N.; Aradottir, S.; Hartmann, S.; Wiesbeck, G.A.; Leech, O.; Skala, K.; Wolfersdorf, M.; Weinmann, W.; Alling, C. Phosphatidylethanol: Normalization during detoxification, gender aspects and correlation with other biomarkers and self-reports. Addict. Biol 2010, 15, 88–95. [Google Scholar]
- Wurst, F.M.; Thon, N.; Weinmann, W.; Tippetts, S.; Marques, P.; Hahn, J.A.; Alling, C.; Aradottir, S.; Hartmann, S.; Lakshman, R. Characterization of sialic acid index of plasma apolipoprotein J and phosphatidylethanol during alcohol detoxification—A pilot study. Alcohol. Clin. Exp. Res 2012, 36, 251–257. [Google Scholar]
- Varga, A.; Hansson, P.; Johnson, G.; Alling, C. Normalization rate and cellular localization of phosphatidylethanol in whole blood from chronic alcoholics. Clin. Chim. Acta 2000, 299, 141–150. [Google Scholar]
- Gnann, H.; Weinmann, W.; Thierauf, A. Formation of phosphatidylethanol and its subsequent elimination during an extensive drinking experiment over 5 days. Alcohol. Clin. Exp. Res. 2012. [Google Scholar] [CrossRef]
- Bocckino, S.B.; Wilson, P.B.; Exton, J.H. Ca2+-mobilizing hormones elicit phosphatidylethanol accumulation via phospholipase D activation. FEBS Lett 1987, 225, 201–204. [Google Scholar]
- Helander, A.; Zheng, Y. Molecular species of the alcohol biomarker phosphatidylethanol in human blood measured by LC-MS. Clin. Chem 2009, 55, 1395–1405. [Google Scholar]
- Holbrook, P.G.; Pannell, L.K.; Murata, Y.; Daly, J.W. Molecular species analysis of a product of phospholipase D activation. Phosphatidylethanol is formed from phosphatidylcholine in phorbol ester- and bradykinin-stimulated PC12 cells. J. Biol. Chem 1992, 267, 16834–16840. [Google Scholar]
- Morrill, G.A.; Ma, G.; Kostellow, A. Molecular species analysis of 1,2-diacylglycerol released in response to progesterone binding to the amphibian oocyte plasma membrane. Cell. Signal 2000, 12, 787–796. [Google Scholar]
- Huusko, T.J.; Liisanantti, M.K.; Nissinen, A.E.; Kakko, S.; Savolainen, E.R.; Vuoristo, J.T.; Savolainen, M.J. Effects of phosphatidylethanol on mouse adipocyte differentiation and expression of stearoyl-CoA desaturase 1. Alcohol. Clin. Exp. Res 2007, 31, 376–382. [Google Scholar]
- Ikegwuonu, F.I.; Pai, J.K.; Mueller, G.C. Effects of steroids on the synthesis and metabolism of phosphatidylethanol in phorbol ester-activated lymphocytes. Carcinogenesis 1990, 11, 1927–1935. [Google Scholar]
- Gnann, H.; Engelmann, C.; Skopp, G.; Winkler, M.; Auwarter, V.; Dresen, S.; Ferreiros, N.; Wurst, F.M.; Weinmann, W. Identification of 48 homologues of phosphatidylethanol in blood by LC-ESI-MS/MS. Anal. Bioanal. Chem 2010, 396, 2415–2423. [Google Scholar]
- Gnann, H.; Weinmann, W.; Engelmann, C.; Wurst, F.M.; Skopp, G.; Winkler, M.; Thierauf, A.; Auwarter, V.; Dresen, S.; Bouzas, N.F. Selective detection of phosphatidylethanol homologues in blood as biomarkers for alcohol consumption by LC-ESI-MS/MS. J. Mass Spectrom 2009, 44, 1293–1299. [Google Scholar]
- Nalesso, A.; Viel, G.; Cecchetto, G.; Mioni, D.; Pessa, G.; Favretto, D.; Ferrara, S.D. Quantitative profiling of phosphatidylethanol molecular species in human blood by liquid chromatography high resolution mass spectrometry. J. Chromatogr. A 2011, 1218, 8423–8431. [Google Scholar]
- Zheng, Y.; Beck, O.; Helander, A. Method development for routine liquid chromatography-mass spectrometry measurement of the alcohol biomarker phosphatidylethanol (PEth) in blood. Clin. Chim. Acta 2011, 412, 1428–1435. [Google Scholar]
- Sarri, E.; Servitja, J.M.; Picatoste, F.; Claro, E. Two phosphatidylethanol classes separated by thin layer chromatography are produced by phospholipase D in rat brain hippocampal slices. FEBS Lett 1996, 393, 303–306. [Google Scholar]
- Gunnarsson, T.; Ekblad, L.; Karlsson, A.; Michelsen, P.; Odham, G.; Jergil, B. Separation of polyphosphoinositides using normal-phase high-performance liquid chromatography and evaporative light scattering detection or electrospray mass spectrometry. Anal. Biochem 1997, 254, 293–296. [Google Scholar]
- Gunnarsson, T.; Karlsson, A.; Hansson, P.; Johnson, G.; Alling, C.; Odham, G. Determination of phosphatidylethanol in blood from alcoholic males using high-performance liquid chromatography and evaporative light scattering or electrospray mass spectrometric detection. J. Chromatogr. B 1998, 705, 243–249. [Google Scholar]
- Varga, A.; Alling, C. Formation of phosphatidylethanol in vitro in red blood cells from healthy volunteers and chronic alcoholics. J. Lab. Clin. Med 2002, 140, 79–83. [Google Scholar]
- Yon, C.; Han, J.S. Analysis of trimethylsilyl derivatization products of phosphatidylethanol by gas chromatography-mass spectrometry. Exp. Mol. Med 2000, 32, 243–245. [Google Scholar]
- Varga, A.; Nilsson, S. Nonaqueous capillary electrophoresis for analysis of the ethanol consumption biomarker phosphatidylethanol. Electrophoresis 2008, 29, 1667–1671. [Google Scholar]
- Nalesso, A.; Viel, G.; Cecchetto, G.; Frison, G.; Ferrara, S.D. Analysis of the alcohol biomarker phosphatidylethanol by NACE with on-line ESI-MS. Electrophoresis 2010, 31, 1227–1233. [Google Scholar]
- Nissinen, A.E.; Makela, S.M.; Vuoristo, J.T.; Liisanantti, M.K.; Hannuksela, M.L.; Horkko, S.; Savolainen, M.J. Immunological detection of in vitro formed phosphatidylethanol—An alcohol biomarker—With monoclonal antibodies. Alcohol. Clin. Exp. Res 2008, 32, 921–928. [Google Scholar]
- Nissinen, A.E.; Laitinen, L.M.; Kakko, S.; Helander, A.; Savolainen, M.J.; Horkko, S. Low plasma antibodies specific for phosphatidylethanol in alcohol abusers and patients with alcoholic pancreatitis. Addict. Biol. 2011. [Google Scholar] [CrossRef]
- Tolonen, A.; Lehto, T.M.; Hannuksela, M.L.; Savolainen, M.J. A method for determination of phosphatidylethanol from high density lipoproteins by reversed-phase HPLC with TOF-MS detection. Anal. Biochem 2005, 341, 83–88. [Google Scholar]
- Faller, A.; Richter, B.; Kluge, M.; Koenig, P.; Seitz, H.K.; Thierauf, A.; Gnann, H.; Winkler, M.; Mattern, R.; Skopp, G. LC-MS/MS analysis of phosphatidylethanol in dried blood spots versus conventional blood specimens. Anal. Bioanal. Chem 2011, 401, 1163–1166. [Google Scholar]
- Marques, P.; Tippetts, S.; Allen, J.; Javors, M.; Alling, C.; Yegles, M.; Pragst, F.; Wurst, F. Estimating driver risk using alcohol biomarkers, interlock blood alcohol concentration tests and psychometric assessments: Initial descriptives. Addiction 2010, 105, 226–239. [Google Scholar]
- Marques, P.; Hansson, T.; Isaksson, A.; Walther, L.; Jones, J.; Lewis, D.; Jones, M. Detection of phosphatidylethanol (PEth) in the blood of drivers in an alcohol ignition interlock program. Traffic Inj. Prev 2011, 12, 136–141. [Google Scholar]
- Stewart, S.H.; Reuben, A.; Brzezinski, W.A.; Koch, D.G.; Basile, J.; Randall, P.K.; Miller, P.M. Preliminary evaluation of phosphatidylethanol and alcohol consumption in patients with liver disease and hypertension. Alcohol Alcohol 2009, 44, 464–467. [Google Scholar]
- Stewart, S.H.; Law, T.L.; Randall, P.K.; Newman, R. Phosphatidylethanol and alcohol consumption in reproductive age women. Alcohol. Clin. Exp. Res 2010, 34, 488–492. [Google Scholar]
- Wurst, F.M.; Vogel, R.; Jachau, K.; Varga, A.; Alling, C.; Alt, A.; Skipper, G.E. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcohol. Clin. Exp. Res 2003, 27, 471–476. [Google Scholar]
- Comasco, E.; Nordquist, N.; Leppert, J.; Oreland, L.; Kronstrand, R.; Alling, C.; Nilsson, K.W. Adolescent alcohol consumption: biomarkers PEth and FAEE in relation to interview and questionnaire data. J. Stud. Alcohol. Drugs 2009, 70, 797–804. [Google Scholar]
- Hahn, J.A.; Dobkin, L.M.; Mayanja, B.; Emenyonu, N.I.; Kigozi, I.M.; Shiboski, S.; Bangsberg, D.R.; Gnann, H.; Weinmann, W.; Wurst, F.M. Phosphatidylethanol (PEth) as a Biomarker of Alcohol Consumption in HIV-Positive Patients in Sub-Saharan Africa. Alcohol. Clin. Exp. Res 2012, 36, 854–862. [Google Scholar]
- Kip, M.J.; Spies, C.D.; Neumann, T.; Nachbar, Y.; Alling, C.; Aradottir, S.; Weinmann, W.; Wurst, F.M. The usefulness of direct ethanol metabolites in assessing alcohol intake in nonintoxicated male patients in an emergency room setting. Alcohol. Clin. Exp. Res 2008, 32, 1284–1291. [Google Scholar]
- Viel, G.; Boscolo-Berto, R.; Cecchi, R.; Bajanowski, T.; Vieira, N.D.; Ferrara, S.D. Bio-medicolegal scientific research in Europe. A country-based analysis. Int. J. Legal. Med 2011, 125, 717–725. [Google Scholar]
- Boscolo-Berto, R.; Viel, G.; Montagnese, S.; Raduazzo, D.I.; Ferrara, S.D.; Dauvilliers, Y. Narcolepsy and effectiveness of gamma-hydroxybutyrate (GHB): A systematic review and meta-analysis of randomized controlled trials. Sleep Med. Rev 2012, 16, 431–443. [Google Scholar]
- Boscolo-Berto, R. Clinical testing and evidence-based medicine: when the absence of evidence doesn’t mean evidence of absence. G. Ital. Nefrol 2009, 26, 417. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar]



{kind=link}
{kind=link}
| Study | Year | Features of the study | Investigated population | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Main aim of interest | Inclusion criteria | Exclusion criteria | Duration of follow-up | Number of Subjects | Mean Age (Ys) * | Race | Comorbidities | Clinical setting | Subjects stratification | Type of controls | ||
| Aradottir et al. | 2006 | Diagnostic sensitivity of PEth and correlation to ethanol consumption (last 14 days) | Diagnosis of alcohol dependence based on DSM IV and ICD-10 | BrAC < 0.1 g/L Illicit Drugs Severe medical illness | - | 66 actively drinking patients attending a programme of consultation for problematic drinking (55 M/11 F) | 49.1 ± 9.9 | - | - | Outpatients Inpatients | By timeline follow-back: “Low” < 40 g (n = 10) | - |
| “Moderate” 40 to 80 g (n = 28) | ||||||||||||
| “High” 80 to 200 g (n = 60) | ||||||||||||
| 78 patients admitted to a detoxification unit (68 M/10 F) | 52.9 ± 8.5 | “Very High” > 200 g (n = 43) | ||||||||||
| Comasco et al. | 2009 | Comparison of diagnostic efficiency of PEth to clinical interview in detecting high alcohol consumers | Students with deviant behaviour as reported by the Survey of Adolescent Life in Vestmanland | - | - | 200 adolescent students (57 M/78 F) | - | - | - | Outpatients | By semistructured interview:
| - |
| Kip et al. | 2008 | Investigate the diagnostic performance of PEth | Negative BAC | Age < 18 y BAC > 0.1g/L Recent use of illicit drugs, Pain ≥ 3 on Visual Analogue Scale, Liver cirrhosis (Child B or C) and renal diseases, Mental illness, non-fluency of German language, police custody or inability to give informed consent | - | 52 Male patients presented at the Emergency room with angina pectoris (ICD 10 I20) or gastrointestinal complaints (ICD 10 K92.9) AUDIT < 8 (n = 52) | 61 (IQR 39–66) | - | Smokers 28.8% | Outpatients | By AUDIT: AUDIT < 8 (n = 52) | - |
| 22 Male patients presented at the Emergency room with angina pectoris (ICD 10 I20) or gastrointestinal complaints (ICD 10 K92.9) AUDIT ≥ 8 (n = 22) | 52 (IQR 38–64) | Smokers 50% | AUDIT ≥ 8 (n = 22) | |||||||||
| Nalesso et al. | 2011 | Correlate PEth to self-reports on alcohol assumption | - | BAC < 0.1 g/L | - | 11 Heavy drinkers admitted to a detoxification unit (7 M/4 F) | 49 (IQR 37–57)# | - | - | Inpatients | - | Intergroup |
| 8 Social drinkers (5 M/3 F) | 42 (IQR 32–56)# | Outpatients | ||||||||||
| 10 Teetotallers (6 M/4 F) | 32.5 (IQR 27–39)# | Outpatients | ||||||||||
| Stewart et al. | 2009 | Evaluate the relationship between PEth and recent drinking in patients with liver disease and hypertension | Recent drinking | Cognitive dysfunction precluding informed consent Abstainers | - | 21 Liver disease patients (13 M/8 F) | 50 (33–64)$ | 6 Hispanic white 15 non-Hispanic white | 21 Liver disease with Model for End-Stage Liver disease 16 (6–32)$; 5 with chronic Hepatitis C | Inpatients and Outpatients | By average drinks per day (each drink = 14 g): <14 gr (n = 17) | - |
| (14 ≤ x ≤ 42) g (n = 14) | ||||||||||||
| 21 Hypertension patients (15 M/6 F) | 60 (44–74)$ | 12 Hispanic white 9 non-Hispanic white | - | ≥ 42 g (n = 11) | ||||||||
| Varga et al. | 1998 | Investigate PEth levels after a limited ethanol intake | Abstainers or “small amount” alcohol consumers | - | 21 days | 17 Population with no or limited alcohol intake (11 M/6 F) | 25–47$ | - | - | Outpatients | 5 abstainers (3 M/2 F) | - |
| 19–31$ | 12 social drinkers (8 M/4 F) | |||||||||||
| Stewart et al. | 2010 | Evaluate the relationship between blood PEth and alcohol use in reproductive age women | Generally healthy women Age 18–35 ys Self-reported consumption of any amount on at least two days/wk | Pregnant women and abstainers | - | 80 healthy women (80 F) | 26 (IQR 23–30) | 71 Non-Hispanic white 6 Non-Hispanic-black 3 Others | - | Outpatients | By average drinks per day >1 (14 g) (n = 64) | - |
| >2 (28 g) (n = 28) | ||||||||||||
| All the cases | ||||||||||||
| Wurst et al.[45] | 2010 | Determine the correlation of PEth to self-reports | Alcohol dependent detoxification patients (ICD 10 F10.25) | Severe liver, renal and brain diseases, metabolic disorders, intake of illicit drugs, BAC < 0.1 g/L | 28 days | 57 alcohol dependent detoxification patients (48 M/9 F) | 43.6 ± 10.4 | - | - | Inpatients | - | - |
| Wurst et al. | 2004 | Evaluate the effect of using a low cut-off to identify heavy drinking/alcohol dependence by PEth in whole blood | Meeting ICD 10 criteria for alcohol-dependence | - | - | 18 detoxification patients (14 M/4 F) | 44 (24–55)$ | - | Smoked cigarettes per day: 20 ± 12.6 | Inpatients | - | - |
| Wurst et al. | 2012 | Explore Sensitivity and Specificity of PEth | Meeting ICD 10 F10.25 criteria | - | 28 days | 5 alcohol dependent patients (5 M/0 F) | 40 (IQR 36–58)# | - | - | Inpatients | - | - |
| Marques et al. | 2009 | Identify alcohol biomarkers related to driver’s BAC patterns from IIDs | With IIDs (ignition lock at 0.04 g/dL) | - | 8 months | 534 DUI offenders (464 M/70 F): 208 alcohol dependent 64 alcohol abusers | 38.7 ± 11.5 | 91% Caucasian 9% Others | - | Outpatients | By fail rates at interlock BrAC test: 0 lockouts (n = 136) | - |
| 0 < lockouts ≤ 1.45% (n = 268) | ||||||||||||
| > 1.45% lockouts (n = 104) | ||||||||||||
| Varga et al. | 2000 | Investigate elimination kinetics of PEth | Chronic alcoholics admitted to a detoxification unit | - | - | 6 Chronic alcoholics (6 M/0 F) | - | - | - | Inpatients | - | - |
| 7 days | 15 Chronic alcoholics (13 M/2 F) | |||||||||||
| Study | Year | Alcohol assumption | PEth Determination | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Methods for estimating alcohol use | Daily Mean Alcohol consumption before test (g/die) | Timing of blood retrieval | Biological assessment before blood retrieval | Type of sample | Form of Measured PEth | Analytical method LOQ # Cut-off ** | Concentration μM | Sensitivity | Specificity | PPV | NPV | Other markers | ||
| Aradottir et al. | 2006 | Timeline follow-back (14 days) | 103 ± 64 Outpatients 204 ± 126 Inpatients | Single retrieval | Negative BrAC within 10 previous hours | Whole Blood | Total PEth | HPLC-ELSD 0.22 μM #** | 3.4 ± 2.6 Outpatients 7.7 ± 3.2 Inpatients | 98% Outpatients 100% Inpatients | - | - | - | %CDT GGT MCV |
| 0–40$ | 100%° | - | - | - | ||||||||||
| 40–80$ | 96.9%° | |||||||||||||
| 80–200$ | 100%° | |||||||||||||
| >200$ | 100%° | |||||||||||||
| Comasco et al. | 2009 | Survey of adolescent life in Vestmanland (1 last year) Semi-structured interview | M = 6.2° F = 5.5° (daily mean during the last year) | Single retrieval | - | Whole Blood | Total PEth | HPLC-ELSD 0.30 μM #** | High alcohol consumers testing positive (n = 9) 0.4 (0.25–0.71)&$ | 9% | 96% | 69% | 49% | FAEE |
| Varga et al. | 1998 | Self Reported Consumption (3 weeks) | 47 g (M) or 32 g (F) (n = 5) | Hours: 0.5 – 1 – 2 – 4 | - | Whole blood | Total PEth | HPLC-ELSD 0.8 μM #** | - | - | 100% | - | - | CDT, GGT |
| Days: 1 | <LOQ | |||||||||||||
| 3 | <LOQ | |||||||||||||
| 5 | <LOQ | |||||||||||||
| 63.5 ± 25.3 (n = 12) | Days: 1 | <LOQ | ||||||||||||
| 18 | 1.4 ± 0.6° | |||||||||||||
| 21 | 1.3 ± 0.5° | |||||||||||||
| Kip et al. | 2008 | AUDIT Self Reported Consumption (1 week) | 20 (IQR 0–43) | Single retrieval | Negative BAC | Whole blood | Total PEth | HPLC-ELSD 0.22 μM # | 0.0 (IQR 0.0–0.35) | - | - | - | - | %CDT GGT MCV EtG in serum and urine |
| 60 (IQR 43–100) | 0.33 (IQR 0.0–1.49) | |||||||||||||
| Nalesso et al. | 2011 | Self Reported Consumption (1 week)^ | 10 (IQR 9–15)° | Single retrieval | Negative BAC | Whole blood | 17 PEth molecular species | LC/HRMS 0.001 μM # | 2.8 ± 1.9° | 100% | - | - | - | - |
| 9 (IQR 4.5–13.5)° | 0.021 ± 0.033° | |||||||||||||
| 0° | <LLOQ° | |||||||||||||
| Stewart et al. | 2009 | Self Reported Consumption (2 weeks) | 11.8 (IQR 0–51.8)° | Single retrieval | - | Whole blood | 16:0/18:1 | LC/MS-MS 0.03 μM # | 0.06 (IQR 0–0.06)° | - | - | - | - | - |
| 26.7 (IQR 10.1–38.5)° | 0.14 (IQR 0.08–0.29)° | |||||||||||||
| 0.98 (IQR 0.47–1.71)° | ||||||||||||||
| Stewart et al. | 2010 | Self Reported Consumption (2 weeks) | 25.4 (IQR 14.6–98.4)° | Single retrieval | - | Whole blood | 16:0/18:1 | LC/MS-MS 0.03 μM # | <14 g/day 0.02 ± 0.04° | 61% | 95% | - | - | - |
| 44.2 (IQR 28.4–98.4)° | (14 < X < 28) g/day 0.07 ± 0.08° | 32% | 95% | |||||||||||
| 23 (IQR 15.1–38.1)° | >28 g/day 0.19 ± 0.18° | - | - | |||||||||||
| Wurst et al. | 2010 | Timeline follow-back (1 week) or AUDIT | 207.4 ± 115.9 | Days: 1 | - | Whole blood | Total PEth | HPLC-ELSD 0.30 μM #** | 4.7 ± 4.97 | 100% | - | - | - | %CDT GGT MCV |
| 3 | 3.09 (IQR 0.81–5.15)°& | 93.7% | ||||||||||||
| 5 | 2.42 (IQR 0.78–4.24)°& | 94.4% | ||||||||||||
| 7 | 1.69 (IQR 0.55–2.9)°& | 94.1% | ||||||||||||
| 14 | 0.88 (IQR 0.18–1.69)°& | 66.7% | ||||||||||||
| 28 | 0.81 (IQR 0.0–2.12)°& | 25% | ||||||||||||
| Wurst et al. | 2004 | Timeline follow-back (1 month) | 148 (32–253.3)$° | Single retrieval | - | Whole blood | Total PEth | HPLC-ELSD 0.30 μM #** | 0.0037 (IQR 0.00063–0.00868)° | 100% | - | - | - | FAEE |
| Wurst et al. | 2012 | Self Reported Consumption (1 week) AUDIT | 240 (IQR 160–352)° | Days: 1 | - | Whole blood | Total PEth | HPLC-ELSD 0.22 μM #** | 4.40 ± 2.45° | 100% | - | - | - | MCV, GGT, SIJ, UEtG, UEtS |
| 3 | ||||||||||||||
| 7 | 2.34 ± 1.57° | |||||||||||||
| 10 | ||||||||||||||
| 14 | 1.28 ± 0.67° | |||||||||||||
| 21 | 0.77 ± 0.35° | |||||||||||||
| 28 | 0.36 ± 0.25° | |||||||||||||
| Marques et al. | 2009 | TLFB (30 days) DSM-IV C-DIS (Module R) AUDIT DRINC TRI | 17.2 ± 17.22 (n = 120) | 1st day – 8th Month | - | Whole blood | Total PEth | HPLC-ELSD 0.22 μM #** | 0.43 ± 0.51 | - | - | - | - | MCV, ALT, AST, GGT, %CDT, FAEE hair, ETG urine, ETS urine, ETG hair |
| 20.7 ± 25.5 (n = 243) | 0.61 ± 0.61 | |||||||||||||
| 29.55 ± 25.2 (n = 99) | 1.45 ± 1.17 | |||||||||||||
| Varga et al. | 2000 | - | - | - | Negative BrAC | Whole blood Erythrocytes MN leukocytes PMN leukocytes Plasma | Total PEth | HPLC-ELSD 0.22 μM #** | D1: 2.5 ± 0.9 (n = 6) | - | - | - | - | CDT, GGT |
| 150–300 (range) | Days: 1 | D1: 5.1 ± 4.7 (n = 15) | ||||||||||||
| 3 | D3: 3.9 ± 2.8° (n = 13) | |||||||||||||
| 5 | D5: 2.5 ± 2.2° (n = 9) | |||||||||||||
| 7 | D7: 2.4 ± 2.5° (n = 10) | |||||||||||||
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Viel, G.; Boscolo-Berto, R.; Cecchetto, G.; Fais, P.; Nalesso, A.; Ferrara, S.D. Phosphatidylethanol in Blood as a Marker of Chronic Alcohol Use: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2012, 13, 14788-14812. https://doi.org/10.3390/ijms131114788
Viel G, Boscolo-Berto R, Cecchetto G, Fais P, Nalesso A, Ferrara SD. Phosphatidylethanol in Blood as a Marker of Chronic Alcohol Use: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2012; 13(11):14788-14812. https://doi.org/10.3390/ijms131114788
Chicago/Turabian StyleViel, Guido, Rafael Boscolo-Berto, Giovanni Cecchetto, Paolo Fais, Alessandro Nalesso, and Santo Davide Ferrara. 2012. "Phosphatidylethanol in Blood as a Marker of Chronic Alcohol Use: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 13, no. 11: 14788-14812. https://doi.org/10.3390/ijms131114788
APA StyleViel, G., Boscolo-Berto, R., Cecchetto, G., Fais, P., Nalesso, A., & Ferrara, S. D. (2012). Phosphatidylethanol in Blood as a Marker of Chronic Alcohol Use: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 13(11), 14788-14812. https://doi.org/10.3390/ijms131114788