Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis


Abstract
:1. Introduction
2. Results
2.1. Descriptive Results
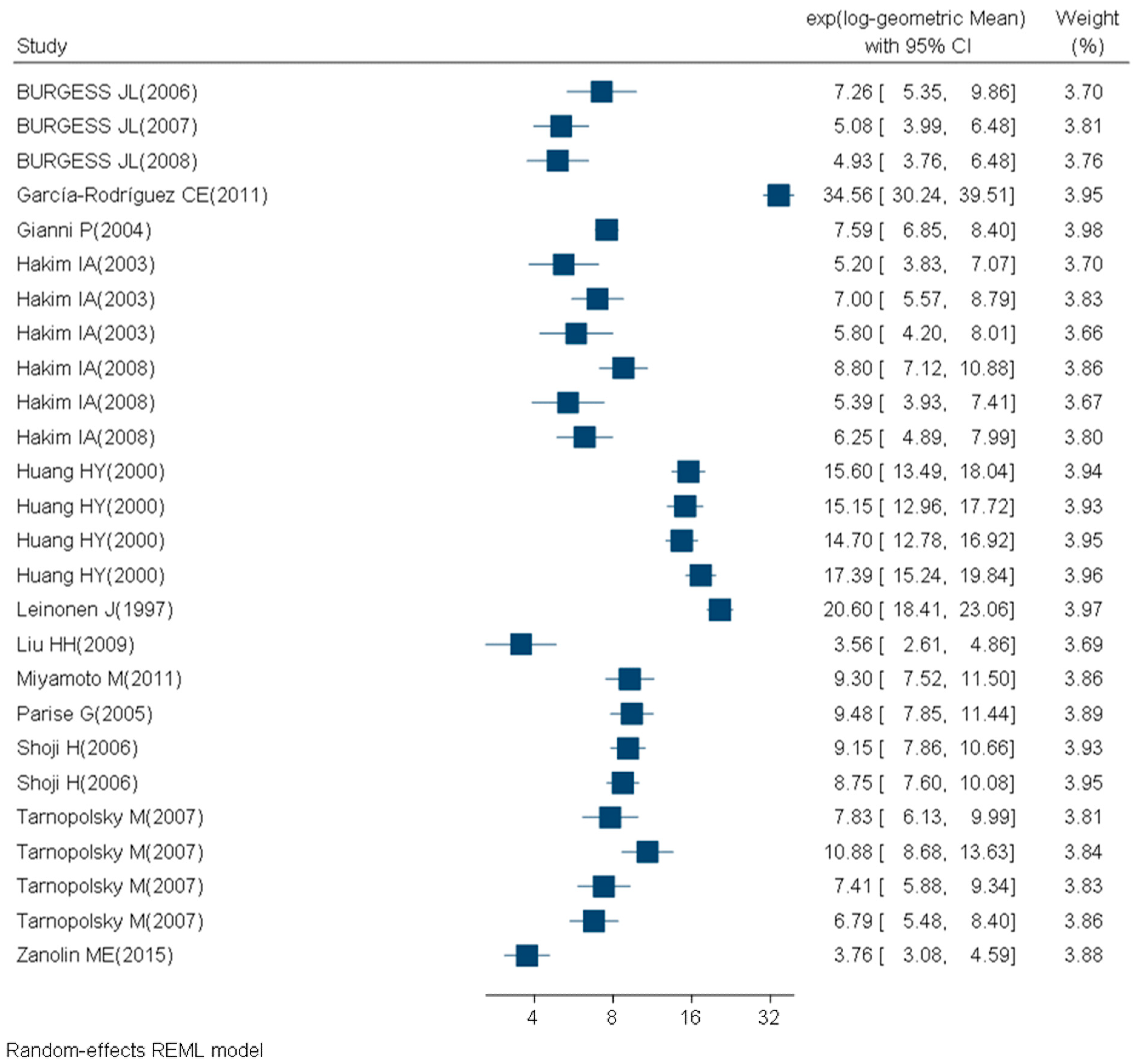
2.2. Meta-Analysis Results
3. Discussion
3.1. Interpretation of Findings
3.2. Quantification of 8-OHdG
3.3. Lack of Homogeneity in Data Collection and Reporting
3.4. Limitations
3.5. Recommendations
4. Materials and Methods
4.1. Literature Search
4.2. Study Selection
4.3. Data Extraction
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| 8-OHdG | 8-hydroxy-2-deoxyguanosine |
| ROS | Reactive oxygen species |
| GM | Geometric mean |
| GSD | Geometric standard deviation |
| BMI | Body mass index |
| SD | Standard deviation |
| SEM | Standard error of the mean |
| CV | Coefficient of variation |
| IQR | Interquartile range |
References
- Lushchak, V.I. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Biol. Interact. 2014, 224, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Shigenaga, M.K.; Gimeno, C.J.; Ames, B.N. Urinary 8-hydroxy-2’-deoxyguanosine as a biological marker of in vivo oxidative DNA damage. Proc. Natl. Acad. Sci. USA 1989, 86, 9697–9701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasai, H. Analysis of a form of oxidative DNA damage, 8-hydroxy-2’-deoxyguanosine, as a marker of cellular oxidative stress during carcinogenesis. Mutat. Res. 1997, 387, 147–163. [Google Scholar] [CrossRef]
- Beckman, K.B.; Ames, B.N. Oxidative decay of DNA. J. Biol. Chem. 1997, 272, 19633–19636. [Google Scholar] [CrossRef] [Green Version]
- Kasai, H.; Hayami, H.; Yamaizumi, Z.; Saito, H.; Nishimura, S. Detection and identification of mutagens and carcinogens as their adducts with guanosine derivatives. Nucleic Acids Res. 1984, 12, 2127–2136. [Google Scholar] [CrossRef] [Green Version]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, C. 8-hydroxy-2’ -deoxyguanosine (8-ohdg): A critical biomarker of oxidative stress and carcinogenesis. J. Environ. Sci. Health Part C Environ. Carcinog. Ecotoxicol. Rev. 2009, 27, 120–139. [Google Scholar] [CrossRef] [Green Version]
- Di Minno, A.; Turnu, L.; Porro, B.; Squellerio, I.; Cavalca, V.; Tremoli, E.; Di Minno, M.N. 8-hydroxy-2-deoxyguanosine levels and cardiovascular disease: A systematic review and meta-analysis of the literature. Antioxid. Redox Signal. 2016, 24, 548–555. [Google Scholar] [CrossRef] [Green Version]
- Neofytou, E.; Tzortzaki, E.G.; Chatziantoniou, A.; Siafakas, N.M. DNA damage due to oxidative stress in chronic obstructive pulmonary disease (copd). Int. J. Mol. Sci. 2012, 13, 16853–16864. [Google Scholar] [CrossRef] [Green Version]
- Abusoglu, S.; Celik, H.T.; Tutkun, E.; Yilmaz, H.; Serdar, M.A.; Bal, C.D.; Yildirimkaya, M.; Avcikucuk, M. 8-hydroxydeoxyguanosine as a useful marker for determining the severity of trichloroethylene exposure. Arch. Environ. Occup. Health 2014, 69, 180–186. [Google Scholar] [CrossRef]
- Sakano, N.; Wang, D.H.; Takahashi, N.; Wang, B.; Sauriasari, R.; Kanbara, S.; Sato, Y.; Takigawa, T.; Takaki, J.; Ogino, K. Oxidative stress biomarkers and lifestyles in japanese healthy people. J. Clin. Biochem. Nutr. 2009, 44, 185–195. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Moral, M.P.; Kannan, K. How stable is oxidative stress level? An observational study of intra- and inter-individual variability in urinary oxidative stress biomarkers of DNA, proteins, and lipids in healthy individuals. Environ. Int. 2019, 123, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Hopf, N.B.; Bourgkard, E.; Demange, V.; Hulo, S.; Sauvain, J.J.; Levilly, R.; Jeandel, F.; Robert, A.; Guichard, Y.; Pralong, J.A.; et al. Early effect markers and exposure determinants of metalworking fluids among metal industry workers: Protocol for a field study. JMIR Res. Protoc. 2019, 8, e13744. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, E.; Poland, C.; Guseva Canu, I.; Prina-Mello, A. The role of biological monitoring in nano-safety. Nano Today 2015, 10, 274–277. [Google Scholar] [CrossRef]
- Barregard, L.; Moller, P.; Henriksen, T.; Mistry, V.; Koppen, G.; Rossner, P., Jr.; Sram, R.J.; Weimann, A.; Poulsen, H.E.; Nataf, R.; et al. Human and methodological sources of variability in the measurement of urinary 8-oxo-7,8-dihydro-2’-deoxyguanosine. Antioxid. Redox Signal. 2013, 18, 2377–2391. [Google Scholar] [CrossRef]
- Zanolin, M.E.; Girardi, P.; Degan, P.; Rava, M.; Olivieri, M.; Di Gennaro, G.; Nicolis, M.; De Marco, R. Measurement of a urinary marker (8-hydroxydeoxy-guanosine, 8-ohdg) of DNA oxidative stress in epidemiological surveys: A pilot study. Int. J. Biol. Markers 2015, 30, e341–e345. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.S.; Olinski, R.; Loft, S. Measurement and meaning of oxidatively modified DNA lesions in urine. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossner, P., Jr.; Mistry, V.; Singh, R.; Sram, R.J.; Cooke, M.S. Urinary 8-oxo-7,8-dihydro-2’-deoxyguanosine values determined by a modified elisa improves agreement with hplc-ms/ms. Biochem. Biophys. Res. Commun. 2013, 440, 725–730. [Google Scholar] [CrossRef]
- Chamitava, L.; Garcia-Larsen, V.; Cazzoletti, L.; Degan, P.; Pasini, A.; Bellisario, V.; Corsico, A.G.; Nicolis, M.; Olivieri, M.; Pirina, P.; et al. Determination of adjusted reference intervals of urinary biomarkers of oxidative stress in healthy adults using gamlss models. PLoS ONE 2018, 13, e0206176. [Google Scholar] [CrossRef]
- Wang, D.H.; Yamada, A.; Miyanaga, M. Changes in urinary hydrogen peroxide and 8-hydroxy-2’-deoxyguanosine levels after a forest walk: A pilot study. Int. J. Environ. Res. Public Health 2018, 15, 1871. [Google Scholar] [CrossRef] [Green Version]
- Tada, S.; Shiota, A.; Hayashi, H.; Nakamura, T. Reference urinary biopyrrin level and physiological variation in healthy young adults: Relation of stress by learning. Heliyon 2020, 6, e03138. [Google Scholar] [CrossRef] [Green Version]
- Dai, X.; Deng, S.; Wang, T.; Qiu, G.; Li, J.; Yang, B.; Feng, W.; He, X.; Deng, Q.; Ye, J.; et al. Associations between 25 lung cancer risk-related snps and polycyclic aromatic hydrocarbon-induced genetic damage in coke oven workers. Cancer Epidemiol. Biomark. Prev. 2014, 23, 986–996. [Google Scholar] [CrossRef] [Green Version]
- Duan, H.; Jia, X.; Zhai, Q.; Ma, L.; Wang, S.; Huang, C.; Wang, H.; Niu, Y.; Li, X.; Dai, Y.; et al. Long-term exposure to diesel engine exhaust induces primary DNA damage: A population-based study. Occup. Environ. Med. 2016, 73, 83–90. [Google Scholar] [CrossRef] [PubMed]
- El-Bayoumy, K.; Richie, J.P., Jr.; Boyiri, T.; Komninou, D.; Prokopczyk, B.; Trushin, N.; Kleinman, W.; Cox, J.; Pittman, B.; Colosimo, S. Influence of selenium-enriched yeast supplementation on biomarkers of oxidative damage and hormone status in healthy adult males: A clinical pilot study. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1459–1465. [Google Scholar]
- Guilbert, A.; De Cremer, K.; Heene, B.; Demoury, C.; Aerts, R.; Declerck, P.; Brasseur, O.; Van Nieuwenhuyse, A. Personal exposure to traffic-related air pollutants and relationships with respiratory symptoms and oxidative stress: A pilot cross-sectional study among urban green space workers. Sci. Total Environ. 2019, 649, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Hara, M.; Nishida, Y.; Shimanoe, C.; Otsuka, Y.; Nanri, H.; Yasukata, J.; Miyoshi, N.; Yamada, Y.; Horita, M.; Kawai, K.; et al. Intensity-specific effect of physical activity on urinary levels of 8-hydroxydeoxyguanosine in middle-aged japanese. Cancer Sci. 2016, 107, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.K.; Lin, C.W.; Chang, C.C.; Chen, P.F.; Wang, C.J.; Hsueh, Y.M.; Chiang, H.C. Heat acclimation decreased oxidative DNA damage resulting from exposure to high heat in an occupational setting. Eur. J. Appl. Physiol. 2012, 112, 4119–4126. [Google Scholar] [CrossRef]
- Ke, Y.; Huang, L.; Xia, J.; Xu, X.; Liu, H.; Li, Y.R. Comparative study of oxidative stress biomarkers in urine of cooks exposed to three types of cooking-related particles. Toxicol. Lett. 2016, 255, 36–42. [Google Scholar] [CrossRef]
- Kikuchi, H.; Nanri, A.; Hori, A.; Sato, M.; Kawai, K.; Kasai, H.; Mizoue, T. Lower serum levels of total cholesterol are associated with higher urinary levels of 8-hydroxydeoxyguanosine. Nutr. Metab. 2013, 10, 59. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Ku, S.Y.; Kang, J.W.; Kim, H.; Kim, Y.D.; Kim, S.H.; Choi, Y.M.; Kim, J.G.; Moon, S.Y. The 8-hydroxydeoxyguanosine concentrations according to hormone therapy and s326c polymorphism of ogg1 gene in postmenopausal women. Mol. Genet. Metab. 2011, 104, 644–647. [Google Scholar] [CrossRef]
- Kitamura, H.; Terunuma, N.; Kurosaki, S.; Hata, K.; Ide, R.; Kuga, H.; Kakiuchi, N.; Masuda, M.; Totsuzaki, T.; Osato, A.; et al. Cross-sectional study on respiratory effect of toner-exposed work in manufacturing plants, japan: Pulmonary function, blood cells, and biochemical markers. Hum. Exp. Toxicol. 2009, 28, 331–338. [Google Scholar] [CrossRef]
- Lee, C.Y.; Isaac, H.B.; Wang, H.; Huang, S.H.; Long, L.H.; Jenner, A.M.; Kelly, R.P.; Halliwell, B. Cautions in the use of biomarkers of oxidative damage; the vascular and antioxidant effects of dark soy sauce in humans. Biochem. Biophys. Res. Commun. 2006, 344, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Jia, X.; Chen, C.Y.O.; Blumberg, J.B.; Song, Y.; Zhang, W.; Zhang, X.; Ma, G.; Chen, J. Almond consumption reduces oxidative DNA damage and lipid peroxidation in male smokers. J. Nutr. 2007, 137, 2717–2722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.J.; Chen, S.T.; Wu, H.Y.; Hsu, H.C.; Chen, M.F.; Lee, Y.T.; Wu, K.Y.; Chien, K.L. Urinary biomarkers of oxidative and nitrosative stress and the risk for incident stroke: A nested case-control study from a community-based cohort. Int. J. Cardiol. 2015, 183, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Miyata, M.; Kasai, H.; Kawai, K.; Yamada, N.; Tokudome, M.; Ichikawa, H.; Goto, C.; Tokudome, Y.; Kuriki, K.; Hoshino, H.; et al. Changes of urinary 8-hydroxydeoxyguanosine levels during a two-day ultramarathon race period in japanese non-professional runners. Int. J. Sports Med. 2008, 29, 27–33. [Google Scholar] [CrossRef]
- Mizoue, T.; Tokunaga, S.; Kasai, H.; Kawai, K.; Sato, M.; Kubo, T. Body mass index and oxidative DNA damage: A longitudinal study. Cancer Sci. 2007, 98, 1254–1258. [Google Scholar] [CrossRef]
- Oba, S.; Inaba, Y.; Shibuya, T.; Oshima, J.; Seyama, K.; Kobayashi, T.; Kunugita, N.; Ino, T. Changes in oxidative stress levels during two weeks of smoking cessation treatment and their association with nutritional characteristics in japanese smokers. Exp. Ther. Med. 2019, 17, 2757–2764. [Google Scholar] [CrossRef] [Green Version]
- Pan, C.H.; Jeng, H.A.; Lai, C.H. Biomarkers of oxidative stress in electroplating workers exposed to hexavalent chromium. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 76–83. [Google Scholar] [CrossRef]
- Pan, C.H.; Chan, C.C.; Wu, K.Y. Effects on chinese restaurant workers of exposure to cooking oil fumes: A cautionary note on urinary 8-hydroxy-2’-deoxyguanosine. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3351–3357. [Google Scholar] [CrossRef] [Green Version]
- Prasad, S.B.; Vidyullatha, P.; Vani, G.T.; Devi, R.P.; Rani, U.P.; Reddy, P.P.; Prasad, H.M. Association of gene polymorphism in detoxification enzymes and urinary 8-ohdg levels in traffic policemen exposed to vehicular exhaust. Inhal. Toxicol. 2013, 25, 1–8. [Google Scholar]
- Shimanoe, C.; Hara, M.; Nishida, Y.; Nanri, H.; Horita, M.; Yamada, Y.; Li, Y.S.; Kasai, H.; Kawai, K.; Higaki, Y.; et al. Perceived stress, depressive symptoms, and oxidative DNA damage. Psychosom. Med. 2018, 80, 28–33. [Google Scholar] [CrossRef]
- Traustadottir, T.; Davies, S.S.; Stock, A.A.; Su, Y.; Heward, C.B.; Roberts, L.J., 2nd; Harman, S.M. Tart cherry juice decreases oxidative stress in healthy older men and women. J. Nutr. 2009, 139, 1896–1900. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Chen, W.L.; Lin, C.M.; Lai, C.H.; Loh, C.H.; Chen, H.I.; Liou, S.H. The relationship between plasma and urinary 8-hydroxy-2-deoxyguanosine biomarkers measured by liquid chromatography tandem mass spectrometry. Environ. Sci. Pollut. Res. Int. 2016, 23, 17496–17502. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.; Hu, C.W.; Yeh, C.Y.; Chao, M.R.; Chen, C.C.; Huang, J.H.; Chang, S.H.; Lee, S.I.; Lee, H.S. Sulfotransferase 1a1 and glutathione s-transferase p1 genetic polymorphisms modulate the levels of urinary 8-hydroxy-2’-deoxyguanosine in betel quid chewers. Arch. Toxicol. 2008, 82, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.; Nanri, A.; Matsushita, Y.; Kasai, H.; Kawai, K.; Mizoue, T. Depressive symptoms and oxidative DNA damage in japanese municipal employees. Psychiatry Res. 2012, 200, 318–322. [Google Scholar] [CrossRef]
- Chen, C.S.; Yuan, T.H.; Shie, R.H.; Wu, K.Y.; Chan, C.C. Linking sources to early effects by profiling urine metabolome of residents living near oil refineries and coal-fired power plants. Environ. Int. 2017, 102, 87–96. [Google Scholar] [CrossRef]
- Jeng, H.A.; Pan, C.H.; Diawara, N.; Chang-Chien, G.P.; Lin, W.Y.; Huang, C.T.; Ho, C.K.; Wu, M.T. Polycyclic aromatic hydrocarbon-induced oxidative stress and lipid peroxidation in relation to immunological alteration. Occup. Environ. Med. 2011, 68, 653–658. [Google Scholar] [CrossRef] [Green Version]
- Liu, A.L.; Lu, W.Q.; Wang, Z.Z.; Chen, W.H.; Lu, W.H.; Yuan, J.; Nan, P.H.; Sun, J.Y.; Zou, Y.L.; Zhou, L.H.; et al. Elevated levels of urinary 8-hydroxy-2 -deoxyguanosine, lymphocytic micronuclei, and serum glutathione s-transferase in workers exposed to coke oven emissions. Environ. Health Perspect. 2006, 114, 673–677. [Google Scholar] [CrossRef] [Green Version]
- Mazlumoglu, M.R.; Ozkan, O.; Alp, H.H.; Ozyildirim, E.; Bingol, F.; Yoruk, O.; Kuduban, O. Measuring oxidative DNA damage with 8-hydroxy-2’-deoxyguanosine levels in patients with laryngeal cancer. Ann. Otol. Rhinol. Laryngol. 2017, 126, 103–109. [Google Scholar] [CrossRef]
- Toraason, M.; Butler, M.A.; Ruder, A.; Forrester, C.; Taylor, L.; Ashley, D.L.; Mathias, P.; Marlow, K.L.; Cheever, K.L.; Krieg, E.; et al. Effect of perchloroethylene, smoking, and race on oxidative DNA damage in female dry cleaners. Mutat. Res. 2003, 539, 9–18. [Google Scholar] [CrossRef]
- Boonla, C.; Hunapathed, C.; Bovornpadungkitti, S.; Poonpirome, K.; Tungsanga, K.; Sampatanukul, P.; Tosukhowong, P. Messenger rna expression of monocyte chemoattractant protein-1 and interleukin-6 in stone-containing kidneys. BJU Int. 2008, 101, 1170–1177. [Google Scholar] [CrossRef]
- Boonla, C.; Wunsuwan, R.; Tungsanga, K.; Tosukhowong, P. Urinary 8-hydroxydeoxyguanosine is elevated in patients with nephrolithiasis. Urol. Res. 2007, 35, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.Y.; Cui, Y.; Chen, L.; Song, J.; Sun, L. Urinary 8-hydroxydeoxyguanosine levels in diabetic retinopathy patients. Eur. J. Ophthalmol. 2008, 18, 94–98. [Google Scholar] [CrossRef]
- Eom, S.Y.; Yim, D.H.; Lee, C.H.; Choe, K.H.; An, J.Y.; Lee, K.Y.; Kim, Y.D.; Kim, H. Interactions between paraoxonase 1 genetic polymorphisms and smoking and their effects on oxidative stress and lung cancer risk in a korean population. PLoS ONE 2015, 10, e0119100. [Google Scholar] [CrossRef] [PubMed]
- Eom, S.Y.; Yim, D.H.; Moon, S.I.; Youn, J.W.; Kwon, H.J.; Oh, H.C.; Yang, J.J.; Park, S.K.; Yoo, K.Y.; Kim, H.S.; et al. Polycyclic aromatic hydrocarbon-induced oxidative stress, antioxidant capacity, and the risk of lung cancer: A pilot nested case-control study. Anticancer Res. 2013, 33, 3089–3097. [Google Scholar] [PubMed]
- Gianni, P.; Jan, K.J.; Douglas, M.J.; Stuart, P.M.; Tarnopolsky, M.A. Oxidative stress and the mitochondrial theory of aging in human skeletal muscle. Exp. Gerontol. 2004, 39, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Wei, J.; Yang, J.; Xu, J.; Pang, W.; Jiang, Y. Pomegranate juice is potentially better than apple juice in improving antioxidant function in elderly subjects. Nutr. Res. 2008, 28, 72–77. [Google Scholar] [CrossRef]
- Guo, X.; Cui, H.; Zhang, H.; Guan, X.; Zhang, Z.; Jia, C.; Wu, J.; Yang, H.; Qiu, W.; Zhang, C.; et al. Protective effect of folic acid on oxidative DNA damage: A randomized, double-blind, and placebo controlled clinical trial. Medicine 2015, 94, e1872. [Google Scholar] [CrossRef]
- Higashi, Y.; Sasaki, S.; Nakagawa, K.; Matsuura, H.; Oshima, T.; Chayama, K. Endothelial function and oxidative stress in renovascular hypertension. N. Engl. J. Med. 2002, 346, 1954–1962. [Google Scholar] [CrossRef]
- Huang, Y.W.; Jian, L.; Zhang, M.B.; Zhou, Q.; Yan, X.F.; Hua, X.D.; Zhou, Y.; He, J.L. An investigation of oxidative DNA damage in pharmacy technicians exposed to antineoplastic drugs in two chinese hospitals using the urinary 8-ohdg assay. Biomed. Environ. Sci. 2012, 25, 109–116. [Google Scholar]
- Inoue, K.; Sakano, N.; Ogino, K.; Sato, Y.; Wang, D.H.; Kubo, M.; Takahashi, H.; Kanbara, S.; Miyatake, N. Relationship between ceruloplasmin and oxidative biomarkers including ferritin among healthy japanese. J. Clin. Biochem. Nutr. 2013, 52, 160–166. [Google Scholar] [CrossRef] [Green Version]
- Iwanaga, S.; Sakano, N.; Taketa, K.; Takahashi, N.; Wang, D.H.; Takahashi, H.; Kubo, M.; Miyatake, N.; Ogino, K. Comparison of serum ferritin and oxidative stress biomarkers between japanese workers with and without metabolic syndrome. Obes. Res. Clin. Pract. 2014, 8, e201–e298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamal, A.; Cincinelli, A.; Martellini, T.; Malik, R.N. Biomarkers of pah exposure and hematologic effects in subjects exposed to combustion emission during residential (and professional) cooking practices in pakistan. Environ. Sci. Pollut. Res. Int. 2016, 23, 1284–1299. [Google Scholar] [CrossRef] [Green Version]
- Kamal, A.; Cincinelli, A.; Martellini, T.; Malik, R.N. Linking mobile source-pahs and biological effects in traffic police officers and drivers in rawalpindi (pakistan). Ecotoxicol. Environ. Saf. 2016, 127, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Cincinelli, A.; Martellini, T.; Palchetti, I.; Bettazzi, F.; Malik, R.N. Health and carcinogenic risk evaluation for cohorts exposed to pahs in petrochemical workplaces in rawalpindi city (pakistan). Int. J. Environ. Health Res. 2016, 26, 37–57. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Hong, Y.C.; Lee, K.H.; Park, H.J.; Park, E.A.; Moon, H.S.; Ha, E.H. Oxidative stress in pregnant women and birth weight reduction. Reprod. Toxicol. 2005, 19, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Kiokias, S.; Gordon, M.H. Dietary supplementation with a natural carotenoid mixture decreases oxidative stress. Eur. J. Clin. Nutr. 2003, 57, 1135–1140. [Google Scholar] [CrossRef] [Green Version]
- Kocael, A.; Erman, H.; Zengin, K.; Kocael, P.C.; Korkmaz, G.G.; Gelisgen, R.; Taskin, M.; Ersan, Y.; Uzun, H. The effects on oxidative DNA damage of laparoscopic gastric band applications in morbidly obese patients. Can. J. Surg. 2014, 57, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Maruhashi, T.; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Kajikawa, M.; Matsumoto, T.; Kihara, Y.; Chayama, K.; et al. Hyperbilirubinemia, augmentation of endothelial function, and decrease in oxidative stress in gilbert syndrome. Circulation 2012, 126, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Mehrdad, R.; Aghdaei, S.; Pouryaghoub, G. Urinary 8-hydroxy-deoxyguanosine as a biomarker of oxidative DNA damage in employees of subway system. Acta Med. Iran. 2015, 53, 287–292. [Google Scholar]
- Nakanishi, S.; Suzuki, G.; Kusunoki, Y.; Yamane, K.; Egusa, G.; Kohno, N. Increasing of oxidative stress from mitochondria in type 2 diabetic patients. Diabetes Metab. Res. Rev. 2004, 20, 399–404. [Google Scholar] [CrossRef]
- Ogino, K.; Murakami, I.; Wang, D.H.; Tsukiyama, Y.; Takahashi, H.; Kubo, M.; Sakano, N.; Setiawan, H.; Bando, M.; Ohmoto, Y. Evaluation of serum arginase i as an oxidative stress biomarker in a healthy japanese population using a newly established elisa. Clin. Biochem. 2013, 46, 1717–1722. [Google Scholar] [CrossRef]
- Ogino, K.; Takahashi, N.; Takigawa, T.; Obase, Y.; Wang, D.H. Association of serum arginase i with oxidative stress in a healthy population. Free Radic. Res. 2011, 45, 147–155. [Google Scholar] [CrossRef]
- Qiu, C.; Hevner, K.; Abetew, D.; Enquobahrie, D.A.; Williams, M.A. Oxidative DNA damage in early pregnancy and risk of gestational diabetes mellitus: A pilot study. Clin. Biochem. 2011, 44, 804–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, Y.; Ogino, K.; Sakano, N.; Wang, D.H.; Yoshida, J.; Akazawa, Y.; Kanbara, S.; Inoue, K.; Kubo, M.; Takahashi, H. Evaluation of urinary hydrogen peroxide as an oxidative stress biomarker in a healthy japanese population. Free Radic. Res. 2013, 47, 181–191. [Google Scholar] [CrossRef] [Green Version]
- Sugita, M.; Kapoor, M.P.; Nishimura, A.; Okubo, T. Influence of green tea catechins on oxidative stress metabolites at rest and during exercise in healthy humans. Nutrition 2016, 32, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Takaki, J. Associations of job stress indicators with oxidative biomarkers in japanese men and women. Int. J. Environ. Res. Public Health 2013, 10, 6662–6671. [Google Scholar] [CrossRef] [PubMed]
- Vezzoli, A.; Dellanoce, C.; Mrakic-Sposta, S.; Montorsi, M.; Moretti, S.; Tonini, A.; Pratali, L.; Accinni, R. Oxidative stress assessment in response to ultraendurance exercise: Thiols redox status and ros production according to duration of a competitive race. Oxidative Med. Cell. Longev. 2016, 2016, 6439037. [Google Scholar] [CrossRef] [Green Version]
- Yao, Y.; Wang, D.; Ma, H.; Li, C.; Chang, X.; Low, P.; Hammond, S.K.; Turyk, M.E.; Wang, J.; Liu, S. The impact on t-regulatory cell related immune responses in rural women exposed to polycyclic aromatic hydrocarbons (pahs) in household air pollution in Gansu, China: A pilot investigation. Environ. Res. 2019, 173, 306–317. [Google Scholar] [CrossRef]
- Yavuzer, S.; Yavuzer, H.; Cengiz, M.; Erman, H.; Demirdag, F.; Doventas, A.; Balci, H.; Erdincler, D.S.; Uzun, H. The role of protein oxidation and DNA damage in elderly hypertension. Aging Clin. Exp. Res. 2016, 28, 625–632. [Google Scholar] [CrossRef]
- Yuan, L.; Meng, L.; Ma, W.; Xiao, Z.; Zhu, X.; Feng, J.F.; Yu, H.; Xiao, R. Impact of apple and grape juice consumption on the antioxidant status in healthy subjects. Int. J. Food Sci. Nutr. 2011, 62, 844–850. [Google Scholar] [CrossRef]
- Zhang, J.; Bao, J.; Wang, R.; Geng, Z.; Chen, Y.; Liu, X.; Xie, Y.; Jiang, L.; Deng, Y.; Liu, G.; et al. A multicenter study of biological effects assessment of pharmacy workers occupationally exposed to antineoplastic drugs in pharmacy intravenous admixture services. J. Hazard. Mater. 2016, 315, 86–92. [Google Scholar] [CrossRef]
- Burgess, J.L.; Meza, M.M.; Josyula, A.B.; Poplin, G.S.; Kopplin, M.J.; McClellen, H.E.; Stürup, S.; Lantz, R.C. Environmental arsenic exposure and urinary 8-ohdg in arizona and sonora. Clin. Toxicol. 2007, 45, 490–498. [Google Scholar] [CrossRef] [PubMed]
- García-Rodríguez, C.E.; Helmersson-Karlqvist, J.; Mesa, M.D.; Miles, E.A.; Noakes, P.S.; Vlachava, M.; Kremmyda, L.S.; Diaper, N.D.; Godfrey, K.M.; Calder, P.C.; et al. Does increased intake of salmon increase markers of oxidative stress in pregnant women? The salmon in pregnancy study. Antioxid. Redox Signal. 2011, 15, 2819–2823. [Google Scholar] [CrossRef] [PubMed]
- Hakim, I.A.; Chow, H.H.; Harris, R.B. Green tea consumption is associated with decreased DNA damage among gstm1-positive smokers regardless of their hogg1 genotype. J. Nutr. 2008, 138, 1567s–1571s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakim, I.A.; Harris, R.B.; Brown, S.; Chow, H.H.; Wiseman, S.; Agarwal, S.; Talbot, W. Effect of increased tea consumption on oxidative DNA damage among smokers: A randomized controlled study. J. Nutr. 2003, 133, 3303s–3309s. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.Y.; Helzlsouer, K.J.; Appel, L.J. The effects of vitamin c and vitamin e on oxidative DNA damage: Results from a randomized controlled trial. Cancer Epidemiol. Biomark. Prev. 2000, 9, 647–652. [Google Scholar]
- Leinonen, J.; Lehtimäki, T.; Toyokuni, S.; Okada, K.; Tanaka, T.; Hiai, H.; Ochi, H.; Laippala, P.; Rantalaiho, V.; Wirta, O.; et al. New biomarker evidence of oxidative DNA damage in patients with non-insulin-dependent diabetes mellitus. FEBS Lett. 1997, 417, 150–152. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.H.; Lin, M.H.; Liu, P.C.; Chan, C.I.; Chen, H.L. Health risk assessment by measuring plasma malondialdehyde (mda), urinary 8-hydroxydeoxyguanosine (8-oh-dg) and DNA strand breakage following metal exposure in foundry workers. J. Hazard. Mater. 2009, 170, 699–704. [Google Scholar] [CrossRef]
- Miyamoto, M.; Kotani, K.; Ishibashi, S.; Taniguchi, N. The relationship between urinary 8-hydroxydeoxyguanosine and metabolic risk factors in asymptomatic subjects. Med. Princ. Pract. 2011, 20, 187–190. [Google Scholar] [CrossRef]
- Parise, G.; Brose, A.N.; Tarnopolsky, M.A. Resistance exercise training decreases oxidative damage to DNA and increases cytochrome oxidase activity in older adults. Exp. Gerontol. 2005, 40, 173–180. [Google Scholar] [CrossRef]
- Shoji, H.; Franke, C.; Campoy, C.; Rivero, M.; Demmelmair, H.; Koletzko, B. Effect of docosahexaenoic acid and eicosapentaenoic acid supplementation on oxidative stress levels during pregnancy. Free Radic. Res. 2006, 40, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Tarnopolsky, M.; Zimmer, A.; Paikin, J.; Safdar, A.; Aboud, A.; Pearce, E.; Roy, B.; Doherty, T. Creatine monohydrate and conjugated linoleic acid improve strength and body composition following resistance exercise in older adults. PLoS ONE 2007, 2, e991. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.F.; Chung, W.Y.; Benzie, I.F. Urine 8-oxo-7,8-dihydro-2’-deoxyguanosine (8-oxodg), a specific marker of oxidative stress, using direct, isocratic lc-ms/ms: Method evaluation and application in study of biological variation in healthy adults. Clin. Chim. Acta Int. J. Clin. Chem. 2010, 411, 416–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreoli, R.; Mutti, A.; Goldoni, M.; Manini, P.; Apostoli, P.; De Palma, G. Reference ranges of urinary biomarkers of oxidized guanine in (2’-deoxy)ribonucleotides and nucleic acids. Free Radic. Biol. Med. 2011, 50, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Topic, A.; Francuski, D.; Markovic, B.; Stankovic, M.; Dobrivojevic, S.; Drca, S.; Radojkovic, D. Gender-related reference intervals of urinary 8-oxo-7,8-dihydro-2’-deoxyguanosine determined by liquid chromatography-tandem mass spectrometry in serbian population. Clin. Biochem. 2013, 46, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.D.; Olinski, R.; Loft, S.; Cooke, M.S. Toward consensus in the analysis of urinary 8-oxo-7,8-dihydro-2’-deoxyguanosine as a noninvasive biomarker of oxidative stress. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2010, 24, 1249–1260. [Google Scholar]
- Kanabrocki, E.L.; Murray, D.; Hermida, R.C.; Scott, G.S.; Bremner, W.F.; Ryan, M.D.; Ayala, D.E.; Third, J.L.; Shirazi, P.; Nemchausky, B.A.; et al. Circadian variation in oxidative stress markers in healthy and type ii diabetic men. Chronobiol. Int. 2002, 19, 423–439. [Google Scholar] [CrossRef]
- Poulsen, H.E.; Loft, S.; Prieme, H.; Vistisen, K.; Lykkesfeldt, J.; Nyyssonen, K.; Salonen, J.T. Oxidative DNA damage in vivo: Relationship to age, plasma antioxidants, drug metabolism, glutathione-s-transferase activity and urinary creatinine excretion. Free Radic. Res. 1998, 29, 565–571. [Google Scholar] [CrossRef]
- Hemmendinger, M.; Graille, M.; Wild, P.; Shoman, Y.; Bergamaschi, E.; Donato, F.; Hopf, N.; Guseva Canu, I. Baseline Values, between and within Subject Variability of Non-Invasive Biomarkers of Inflammation and Oxidative Stress: A Systematic Review and Meta-Analysis. PROSPERO 2020 CRD42020146623: 2020. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020146623 (accessed on 9 March 2020).
- Hemmendinger, M.; Wild, P.; Shoman, Y.; Graille, M.; Bergamaschi, E.; Hopf, N.; Guseva Canu, I. Reference ranges of oxidative stress biomarkers selected for non-invasive biological surveillance of nanotechnology workers: Study protocol and meta-analysis results for 8-ohdg in exhaled breath condensate. Toxicol. Lett. 2020, 327, 41–47. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graille, M.; Wild, P.; Sauvain, J.J.; Hemmendinger, M.; Guseva-Canua, I.; Hopf, N.B. Urinary 8-isoprostane as a biomarker for oxidative stress: A systematic review and meta-analysis. Toxicol. Lett. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, J.E.; Brennan, S.E.; Ryan, R.E.; Thomson, H.J.; Johnston, R.V. Summarizing study characteristics and preparing for synthesis. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019; pp. 229–240. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMI ≤ 25 | BMI > 25 | |||||
|---|---|---|---|---|---|---|
| Analytical Techniques | All Participants | Smoking Status | All Participants | Smoking Status | ||
| Chemical | 3.9 * (3–5.5) (n ** = 31) | Nonsmokers | 4.3 | 2.8 (2.4–3.5) (n = 9) | Nonsmokers | 2.5 |
| (n = 14) | (2.9–5.5) | (n = 3) | (1.9–2.8) | |||
| Smokers | 22.2 | Smokers | 4.0 | |||
| (n = 2) | (3–41.4) | (n = 2) | (3.5–4.5) | |||
| Immunological | 9.0 (5.9–19.8) (n = 47) | Nonsmokers | 11.5 | 7.7 (5.8 – 10.9) (n = 26) | Nonsmokers | 9.3 |
| (n = 24) | (5.9–21.6) | (n = 13) | (7.8–14.7) | |||
| Smokers | NA | Smokers | 6.0 | |||
| (n = 0) | (n = 6) | (5.4–7) | ||||
| Reference | Study Group | Analytic Method | Sample | Country | Sample Size | Mean Age | Female | Male | Smoking Status | Mean BMI | AM | GM | IQR | Range | Median | CI | Units (8-OHdG/Creatinine) | Computed GM (ng/mg Creatinine) | GSD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [21] | Control group | HPLC | spot urine | China | 497 | 42.48 | 113 | 384 | 50% | 23.72 | 4.47 ± 1.26 * | nmol/mmol | 11 | 1 | |||||
| [22] | Control group | HPLC-MS/MS | spot urine | China | 106 | 31.62 | 0 | 106 | 52.8% | 23.79 | 3 ± 1.08 * | μg/g | 3 | 1 | |||||
| [23] | Selenium group baseline value | HPLC with EC detection | spot urine | USA | 17 | 30.7 | 0 | 17 | 0% | 24.2 | 3.16 ± 1.28 * | ng/mg | 3 | 1 | |||||
| [24] | Baseline value | UPLC-MS-MS in positive EI mode | spot urine | Belgium | 48 | 40 | 3 | 45 | 31.2% | 24.2 | 10.76 ± 2.83 * | 7.05–20.92 | μg/g | 10 | 1 | ||||
| [25] | Men baseline | HPLC | spot urine | Japan | 2370 | 60.7 | 0 | 2370 | 24.9% | 23.6 | 3.7 ± 1.6 * | ng/mg | 4 | 2 | |||||
| [25] | Women baseline | HPLC | spot urine | Japan | 4052 | 60.2 | 4052 | 0 | 4.7% | 22.2 | 4.1 ± 1.7 * | ng/mg | 4 | 2 | |||||
| [26] | Baseline value | LC-MS/MS | spot urine | Taiwan | 58 | 23.84 | 0 | 58 | 51.7% | 24.55 | 2.63–11.54 | 4.42 | µg/g | 16 | 2 | ||||
| [27] | Service staff group | HPLC | spot urine | China | 67 | 24.8 | 0 | 67 | 0% | 23.2 | 1.4 | 0.9–1.8 | μmol/mol | 2 | 3 | ||||
| [28] | All population | HPLC | spot urine | Japan | 503 | 42.4 | 209 | 294 | 27.4% | 22.5 | 2.37–4.03 | 0.8–10.0 | 3.01 | μg/g | 3 | 1 | |||
| [29] | Baseline value | HPLC | spot urine | Korea | 102 | 55 | 102 | 0 | 0% | 24.1 | 6.5 ± 3.9 * | μg/g | 6 | 2 | |||||
| [30] | Control group | HPLC | spot urine | Japan | 805 | 40.3 | 0 | 805 | 46.7% | 23.7 | 3.79 ± 1.44 * | ng/mg | 4 | 1 | |||||
| [31] | Baseline value | GC-MS | spot urine | Singapore | 24 | 22.8 | NA | NA | 0% | 21.6 | 2.02 ± 1.12 * | µmol/mol | 5 | 2 | |||||
| [32] | Non smoker group baseline | HPLC with EC detection | 24 h urine | China | 30 | 21.5 | 0 | 30 | 0% | 22.8 | 6.3 ± 0.5 ** | µmol/mol | 14 | 2 | |||||
| [32] | Smoker group baseline | HPLC with EC detection | 24 h urine | China | 60 | 21.8 | 0 | 60 | 100% | 22.6 | 18 ± 1 ** | µmol/mol | 41 | 2 | |||||
| [33] | Participants without stroke | LC–MS/MS | spot urine | Taiwan | 131 | 64.9 | 57 | 74 | 50% | 22.9 | 8.3–22.8 | 13 | μg/g | 13 | 2 | ||||
| [34] | Male baseline | HPLC-EC | spot urine | Japan | 79 | 47.9 | 0 | 79 | 0% | 22.3 | 2.81 ± 1.07 * | μg/g | 3 | 2 | |||||
| [34] | Female baseline | HPLC-EC | spot urine | Japan | 16 | 46.7 | 16 | 0 | 0% | 20.6 | 3.04 ± 1.42 * | μg/g | 3 | 1 | |||||
| [35] | Women baseline | HPLC | spot urine | Japan | 37 | 28–57 | 37 | 0 | 5.4% | 21.5 | 3.2–5.2 | 3.9 | μg/g | 4 | 1 | ||||
| [35] | Non smoking men group baseline | HPLC | spot urine | Japan | 87 | 28–57 | 0 | 87 | 0% | 24.2 | 2.9–4.7 | 3.6 | μg/g | 4 | 1 | ||||
| [36] | Baseline value | HPLC with an EC detector | spot urine | Japan | 23 | 46.8 | 11 | 12 | 100% | 23.6 | 3.02 | 2.24–4.07 | ng/mg | 5 | 1 | ||||
| [37] | Control group | LC–MS/MS | spot urine | Taiwan | 125 | 34.1 | 0 | 125 | 0% | 22.8 | 4.1 ± 2.1 * | μg/g | 4 | 2 | |||||
| [38] | Control group | HPLC-MS/MS | spot urine | China | 185 | 40.4 | 124 | 61 | 0% | 24.4 | 5.5 ± 2.2 * | µg/g | 6 | 2 | |||||
| [39] | Control group | LC EC | spot urine | India | 135 | 41.31 | 0 | 135 | 0% | 22.38 | 3.57 ± 0.63 * | μmol/mol | 9 | 1 | |||||
| [40] | All population | HPLC | spot urine | Japan | 6517 | 60.3 | 4064 | 2453 | 12.6% | 22.7 | 3.9 ± 1.6 * | ng/mg | 4 | 2 | |||||
| [41] | Placebo group end of study | LC-MS/MS | spot urine | USA | 12 | 69 | 6 | 6 | 0% | 25 | 2 ± 0.2 ** | µmol/mol | 5 | 1 | |||||
| [41] | Tart cherryjuice group end of study | LC-MS/MS | spot urine | USA | 12 | 69 | 6 | 6 | 0% | 25 | 1.8 ± 0.1 ** | µmol/mol | 4 | 1 | |||||
| [42] | Male group | LC-MS/MS | spot urine | China | 69 | 37.83 | 0 | 69 | 43.5% | 24.1 | 4.55 ± 4.44 * | μg/g | 3 | 2 | |||||
| [42] | Female group | LC-MS/MS | spot urine | China | 23 | 38.55 | 23 | 0 | 0% | 22.1 | 4.34 ± 3.85 * | μg/g | 3 | 2 | |||||
| [43] | Control group | LC–MS/MS | spot urine | Taiwan | 129 | 51.7 | 39 | 90 | 27.9% | 24.6 | 4.3 ± 0.5 ** | ng/mg | 3 | 3 | |||||
| [44] | Men group | HPLC | spot urine | Japan | 196 | 44.4 | 0 | 196 | 43.9% | 23.8 | 3.3 ± 1.1 * | µg/g | 3 | 1 | |||||
| [44] | Women group | HPLC | spot urine | Japan | 136 | 40.4 | 136 | 0 | 2.9% | 21 | 3.3 ± 1.1 * | µg/g | 3 | 1 |
| Reference | Study Group | Analytic Method | Sample | Country | Sample Size | Mean Age | Female | Male | Smoking Status | Mean BMI | AM | IQR | Median | Units (8-OHdG/Creatinine) | Computed GM (ng/mg Creatinine) | GSD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [45] | Elderly low expose group | LC–MS/MS | spot urine | Taiwan | 71 | 66.36 | 36 | 35 | 9.9% | 26.36 | 3.16 ± 4.07 * | μg/g | 3 | 2 | ||
| [23] | Placebo group | HPLC with EC detection | spot urine | USA | 19 | 31.1 | 0 | 19 | 0% | 25.2 | 4.18 ± 4.78 * | ng/mg | 3 | 2 | ||
| [46] | Control group | LC/MS/MS | spot urine | Taiwan | 168 | 43.2 | NA | NA | 34% | 26.4 | 10.61 ± 7.77 * | µmol/mol | 21 | 2 | ||
| [47] | Control group | HPLC | spot urine | China | 31 | 38.7 | 0 | 31 | 19.4% | ≤24 38.7% >24 61.3% | 1.0–4.0 | 1.3 | µmol/mol | 3 | 3 | |
| [48] | Control non smoker group | HPLC–ECD | spot urine | Turkey | 19 | 54.8 | 3 | 16 | 0% | 29.1 | 2.1 ± 1 * | μg/g | 2 | 1 | ||
| [48] | Control ex-smoker group | HPLC–ECD | spot urine | Turkey | 21 | 57.5 | 3 | 18 | 0% | 27.2 | 2.6 ± 0.8 * | μg/g | 2 | 2 | ||
| [48] | Control smoker group | HPLC– ECD | spot urine | Turkey | 24 | 51.1 | 4 | 20 | 100% | 26.5 | 4.2 ± 2.8 * | μg/g | 3 | 2 | ||
| [35] | Smoking men group baseline | HPLC | spot urine | Japan | 40 | 28–57 | 0 | 40 | 100% | 25.1 | 3.6–5.6 | 4.5 | μg/g | 4 | 1 | |
| [49] | Control group baseline | HPLC | spot urine | USA | 20 | 39 | 20 | 0 | 50% | 29 | 2.8 ± 1.7 * | µg/g | 2 | 2 |
| Reference | Study Group | Sample | Country | Sample Size | Mean Age | Female | Male | Smoking Status | Mean BMI | AM | GM | IQR | Range | Median | CI | Units (8-OHdG/Creatinine) | Computed GM (ng/mg Creatinine) | GSD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [50] | Healthy control group | 24 h urine | Thailand | 30 | 41.43 | 19 | 11 | NA | 22.56 | 4.32 ± 4.93 * | μg/g | 3 | 2 | |||||
| [51] | Healthy control group | 24 h urine | Thailand | 30 | 41.43 | 19 | 11 | NA | 22.56 | 5.27 ± 2.77 * | μg/g | 5 | 2 | |||||
| [52] | Control group | spot urine | China | 35 | 60 | 15 | 20 | 0% | 22.9 | 11.9 ± 4.9 * | ng/mg | 11 | 1 | |||||
| [53] | Control group | spot urine | Korea | 416 | 64.4 | 92 | 324 | 28.1% | 23.7 | 5.06 | 4.55–5.62 | μg/g | 5 | 2 | ||||
| [54] | Control group | spot urine | Korea | 140 | 68.8 | 32 | 108 | 65.5% | 22.46 | 4.88 | 4.43–5.38 | μg/g | 5 | 1 | ||||
| [55] | Healthy young group | 24 h urine | Canada | 12 | 22.8 | 0 | 12 | 0% | 25 | 5333 ± 1191 * | ng/g | 5 | 1 | |||||
| [56] | Apple group final value | spot urine | China | 13 | 62.8 | 3 | 10 | 0% | 24.2 | 824.41 ± 343.66 * | ng/mmol | 7 | 1 | |||||
| [56] | Pomegranate group final value | spot urine | China | 13 | 64.1 | 3 | 10 | 0% | 23 | 651.57 ± 332.44 * | ng/mmol | 5 | 2 | |||||
| [57] | placebo group baseline value | spot urine | China | 150 | 51.58 | 92 | 58 | 41.3% | 23.8 | 60.89 ± 1.62* | 58.19 | ng/mg | 61 | 2 | ||||
| [57] | Baseline line value Low FA group | spot urine | China | 145 | 48.9 | 87 | 58 | 33.8% | 24.5 | 55.48 ± 1.74 * | 53.51 | ng/mg | 55 | 2 | ||||
| [57] | Baseline value high FA group | spot urine | China | 143 | 48.66 | 94 | 49 | 30.1% | 24.6 | 55.81 ± 1.72 * | 54.73 | ng/mg | 56 | 2 | ||||
| [58] | Control group | 24 h urine | Japan | 15 | 40 | 6 | 9 | 0% | 23.2 | 9.7 ± 4.6 * | ng/mg | 9 | 2 | |||||
| [59] | Control group I | spot urine | China | 20 | 25.55 | 17 | 3 | 0% | 19.74 | 10.68 ± 1.07 ** | ng/mg | 10 | 2 | |||||
| [59] | Control group II | spot urine | China | 20 | 24.5 | 15 | 5 | 0% | 20.09 | 11.96 ± 0.73 ** | ng/mg | 12 | 1 | |||||
| [60] | Male group | spot urine | Japan | 195 | 41.7 | 0 | 195 | 49.7% | 23.6 | 9.35 ± 3.66 * | ng/mg | 9 | 1 | |||||
| [60] | Female group | spot urine | Japan | 194 | 41.7 | 194 | 0 | 29.9% | 22.1 | 10.97 ± 5 * | ng/mg | 10 | 2 | |||||
| [61] | Non MS group | spot urine | Japan | 638 | 40.8 | 385 | 253 | 27.3% | 22.3 | 9.28 ± 4.15 * | ng/mg | 8 | 2 | |||||
| [62] | Male control | spot urine | Pakistan | 34 | 39.7 | 0 | 34 | 0% | 19.85 | 24.5 ± 6.6 * | 11.08–33.85 | 25.72 | ng/mg | 26 | 1 | |||
| [62] | Female control | spot urine | Pakistan | 32 | 39.52 | 32 | 0 | 0% | 20.83 | 24.5 ± 6.33 * | 11.1–33.85 | 24.47 | ng/mg | 24 | 1 | |||
| [63] | Control group | spot urine | Pakistan | 34 | 39.7 | 0 | 34 | 0% | 20.9 | 24 ± 4 * | 9–30 | 25 | ng/mg | 25 | 1 | |||
| [64] | Control group | spot urine | Pakistan | 34 | 37 | 0 | 34 | 0% | 20.8 | 25.8 ± 7 * | 9.1–33.9 | 27.9 | ng/mg | 28 | 1 | |||
| [65] | Pregnant women | spot urine | Korea | 261 | 29.6 | 261 | 0 | 0% | 21 | 20.8 ± 14.2 * | µg/g | 17 | 2 | |||||
| [66] | Control group baseline | spot urine | UK | 32 | 31.7 | 15 | 17 | 0% | 22.4 | 21.6 ± 12.6 * | ng/mg | 19 | 2 | |||||
| [66] | Test group baseline | spot urine | UK | 32 | 31.7 | 15 | 17 | 0% | 22.4 | 24 ± 13.3 * | ng/mg | 21 | 2 | |||||
| [67] | Control group | spot urine | Turkey | 20 | 40.7 | 10 | 10 | NA | 22.52 | 7.84 ± 7.04 * | ng/mg | 6 | 2 | |||||
| [68] | Control group | spot urine | Japan | 108 | 23 | 0 | 108 | NA | 22.5 | 10.4 ± 3.2 * | ng/mg | 10 | 1 | |||||
| [69] | Non exposed group | spot urine | Iran | 43 | 35.58 | 0 | 43 | 21% | 19–24 | 54.16 ± 26.98 * | ng/mg | 48 | 2 | |||||
| [70] | Control group | spot urine | Japan | 52 | 62.4 | 27 | 25 | 0% | 24 | 8.8 ± 0.5 ** | ng/mg | 8 | 1 | |||||
| [71] | Male group | spot urine | Japan | 276 | 42.1 | 0 | 276 | NA | 23.8 | 8.8 ± 0.2 ** | ng/mg | 8 | 1 | |||||
| [71] | Female group | spot urine | Japan | 445 | 42.7 | 445 | 0 | NA | 21.9 | 9.8 ± 0.2 ** | ng/mg | 9 | 2 | |||||
| [72] | Male healthy population | spot urine | Japan | 142 | 43.6 | 0 | 142 | 31% | 22.4 | 11.5 ± 5.2 * | ng/mg | 10 | 2 | |||||
| [72] | Female healthy population | spot urine | Japan | 136 | 43.4 | 136 | 0 | 52.2% | 23.8 | 9.4 ± 3.4 * | ng/mg | 9 | 1 | |||||
| [73] | Control group | spot urine | USA | 43 | 32.6 | 43 | 0 | 0% | 23.2 | 6.31 ± 2.49 * | ng/mg | 6 | 1 | |||||
| [74] | Male group | spot urine | Japan | 323 | 42 | 0 | 323 | 42.7% | 23.7 | 8.85 ± 3.29 | ng/mg | 8 | 1 | |||||
| [74] | Female group | spot urine | Japan | 443 | 42.7 | 443 | 0 | 13.5% | 21.9 | 9.89 ± 4.54 * | ng/mg | 9 | 2 | |||||
| [75] | Green tea catechin-no exercise group baseline value | spot urine | Japan | 8 | 22.4 | 0 | 8 | 0% | >18 <25 | 15.9 ± 3.6 * | ng/mg | 16 | 1 | |||||
| [75] | Green tea catechin-exercise group baseline value | spot urine | Japan | 8 | 21.1 | 0 | 8 | 0% | >18 <25 | 22.9 ± 7.9 * | ng/mg | 22 | 1 | |||||
| [75] | Placebo group | spot urine | Japan | 8 | 21.1 | 0 | 8 | 0% | >18 <25 | 18 ± 6.2 * | ng/mg | 17 | 1 | |||||
| [76] | Men group | spot urine | Japan | 272 | 43.5 | 0 | 272 | 60.7% | 23.7 | 8.86 ± 3.36 * | 2.13–21.87 | μg/g | 8 | 1 | ||||
| [76] | Women group | spot urine | Japan | 295 | 40.3 | 295 | 0 | 15.6% | 21.7 | 9.25 ± 4.03 * | 0.05–25.56 | μg/g | 8 | 2 | ||||
| [77] | Baseline value 50km group | spot urine | Italy | 6 | 41.83 | NA | NA | 0% | 21.08 | 4.38 ± 1.16 * | ng/mg | 4 | 1 | |||||
| [78] | Summer Non heating season | spot urine | China | 34 | 47.9 | 34 | 0 | 0% | 23.2 | 12.7 ± 4.7 * | 2.60, 25.8 | 13.6 | ng/mg | 9 | 2 | |||
| [79] | Healthy volunteers Young group | spot urine | Turkey | 30 | 41.6 | 22 | 8 | 0% | 22.1 | 3.24 ± 1.54 * | ng/mg | 3 | 2 | |||||
| [79] | Healthy volunteers Elderly group | spot urine | Turkey | 30 | 69.1 | 20 | 10 | 0% | 23.6 | 5.74 ± 2.68 * | ng/mg | 5 | 2 | |||||
| [80] | Baseline value | spot urine | China | 25 | 20.9 | 12 | 13 | 0% | 20.67 | 3765.63 ± 958.14 * | ng/mmol | 32 | 1 | |||||
| [15] | Women group | spot urine | Italy | 33 | 30 | 33 | 0 | 29% | 20.7 | 3.68–7.20 | 5.21 | ng/mg | 4 | 2 | ||||
| [81] | Non exposed group | spot urine | China | 143 | 27.89 | 100 | 43 | 8% | 21.03 | 17.36 ± 13.5 * | ng/mg | 14 | 2 |
| Reference | Study Group | Sample | Country | Sample Size | Mean Age | Female | Male | Smoking Status | MeanBMI | AM | IQR | Range | Median | Units (8-OHdG/Creatinine) | Computed GM (ng/mg Creatinine) | GSD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [82] | Cocorit communities | spot urine | Mexico | 10 | 45.9 | 5 | 5 | 30% | 27 | 8.2 ± 4.3 * | μg/g | 7 | 2 | |||
| [82] | Pueblo Yaqui communities | spot urine | Mexico | 15 | 35.3 | 9 | 6 | 7% | 26.7 | 5.7 ± 2.9 * | μg/g | 5 | 2 | |||
| [82] | Campo 47 | spot urine | Mexico | 15 | 39.5 | 10 | 5 | 40% | 29.8 | 5.7 ± 3.3 * | μg/g | 5 | 2 | |||
| [83] | Control group | spot urine | UK | 61 | 28.4 | 61 | 0 | 9% | 26 | 39.83 ± 2.92 ** | ng/mg | 35 | 2 | |||
| [55] | Healthy older group | 24 h urine | Canada | 12 | 71.8 | 0 | 12 | 0% | 28.8 | 7714 ± 1402 * | ng/g | 8 | 1 | |||
| [84] | Water group baseline value | spot urine | USA | 42 | 18–79 | 32 | 10 | 100% | 25.9 | 8.7 ± 1.3 ** | ng/mg | 5 | 3 | |||
| [84] | Green tea group baseline value | spot urine | USA | 35 | 18–79 | 27 | 8 | 100% | 26.5 | 10.8 ± 1.3 ** | ng/mg | 9 | 2 | |||
| [84] | Black tea baseline value | spot urine | USA | 43 | 18–79 | 31 | 12 | 100% | 26.7 | 9.5 ± 2.1 ** | ng/mg | 6 | 2 | |||
| [85] | Water group baseline value | spot urine | USA | 45 | 49.8 | 32 | 13 | 100% | 26.9 | 9.5 ± 1.3 ** | ng/mg | 6 | 3 | |||
| [85] | Black tea baseline value | spot urine | USA | 46 | 52.1 | 34 | 12 | 100% | 27.2 | 10.8 ± 2.5 ** | ng/mg | 7 | 2 | |||
| [85] | Green tea group baseline value | spot urine | USA | 42 | 51.6 | 32 | 10 | 100% | 27.2 | 8.7 ± 1.8 ** | ng/mg | 5 | 3 | |||
| [86] | Placebo group baseline value | 24 h urine | USA | 47 | 58.1 | 23 | 24 | 0% | 28.9 | 17.6 ± 10.4 * | ng/mg | 15 | 2 | |||
| [86] | Vit C group baseline value | 24 h urine | USA | 46 | 61.2 | 26 | 20 | 0% | 28.7 | 19.3 ± 9.3 * | ng/mg | 17 | 2 | |||
| [86] | Vit E group baseline value | 24 h urine | USA | 45 | 55.5 | 29 | 16 | 0% | 28.6 | 16.5 ± 8.4 * | ng/mg | 15 | 2 | |||
| [86] | Vit C + Vit E baseline value | 24 h urine | USA | 46 | 57.7 | 24 | 22 | 0% | 28.9 | 17.7 ± 9.5 * | ng/mg | 16 | 2 | |||
| [87] | Control group | 24 h urine | Finland | 100 | 65 | 46 | 54 | 18% | 27.7 | 24.3 ± 15.2 * | ng/mg | 21 | 2 | |||
| [88] | Control group | spot urine | Taiwan | 27 | 49 | 0 | 27 | 55.6% | 25.8 | 5 ± 4.92 * | µg/g | 4 | 2 | |||
| [89] | All population | spot urine | Japan | 90 | 52 | 60 | 30 | 0% | 25.2 | 5.8–23.2 | 0.90–48.0 | 9.3 | ng/mg | 9 | 3 | |
| [90] | Baseline value | spot urine | Canada | 28 | 68.5 | NA | NA | 0% | 27.1 | 10783 ± 5856 * | ng/g | 9 | 2 | |||
| [91] | control group baseline | spot urine | Spain | 23 | 30.42 | 23 | 0 | 0% | 25.32 | 9.29 ± 0.69 ** | ng/mg | 9 | 1 | |||
| [91] | DHA group baseline | spot urine | Spain | 23 | 29.97 | 23 | 0 | 0% | 25.62 | 9.81 ± 0.79 ** | ng/mg | 9 | 1 | |||
| [92] | Placebo group men | 24 h urine | Canada | 8 | 74.8 | 0 | 8 | 0% | 25.9 | 8329 ± 3032 * | ng/g | 8 | 1 | |||
| [92] | Placebo group women | 24 h urine | Canada | 10 | 68.3 | 10 | 0 | 0% | 25.2 | 11622 ± 4379 * | ng/g | 7 | 1 | |||
| [92] | Intervention group men baseline | 24 h urine | Canada | 11 | 71.8 | 0 | 11 | 0% | 27.8 | 7245 ± 2703 * | ng/g | 11 | 1 | |||
| [92] | Intervention group women baseline | 24 h urine | Canada | 10 | 69.5 | 10 | 0 | 0% | 25.5 | 7942 ± 3071 * | ng/g | 7 | 1 | |||
| [15] | Men group early morning | spot urine | Italy | 22 | 34 | 0 | 22 | 38.1% | 25.3 | 2.76–5.25 | 3.76 | ng/mg | 5 | 2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graille, M.; Wild, P.; Sauvain, J.-J.; Hemmendinger, M.; Guseva Canu, I.; Hopf, N.B. Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 3743. https://doi.org/10.3390/ijms21113743
Graille M, Wild P, Sauvain J-J, Hemmendinger M, Guseva Canu I, Hopf NB. Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis. International Journal of Molecular Sciences. 2020; 21(11):3743. https://doi.org/10.3390/ijms21113743
Chicago/Turabian StyleGraille, Melanie, Pascal Wild, Jean-Jacques Sauvain, Maud Hemmendinger, Irina Guseva Canu, and Nancy B. Hopf. 2020. "Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis" International Journal of Molecular Sciences 21, no. 11: 3743. https://doi.org/10.3390/ijms21113743
APA StyleGraille, M., Wild, P., Sauvain, J. -J., Hemmendinger, M., Guseva Canu, I., & Hopf, N. B. (2020). Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis. International Journal of Molecular Sciences, 21(11), 3743. https://doi.org/10.3390/ijms21113743