Chondroitin Sulfate Prevents STZ Induced Diabetic Osteoporosis through Decreasing Blood Glucose, AntiOxidative Stress, Anti-Inflammation and OPG/RANKL Expression Regulation

Abstract
:1. Introduction
2. Results
2.1. CS Increased Body Weight and Decreased Water and Food Intake
2.2. CS Increased Bone-Mineral Density (BMD) of Diabetic Rats
2.3. CS Decreased Blood Glucose and Regulated Serum Bone Turn over Markers
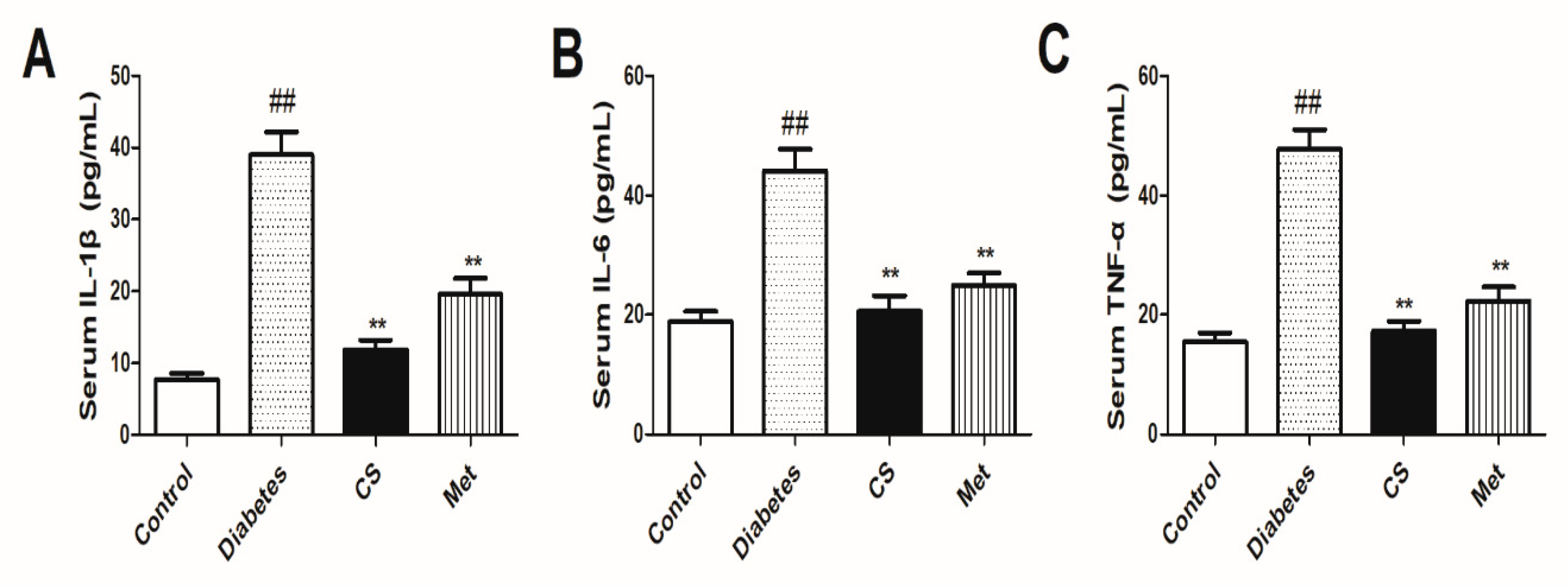
2.4. CS Decreased Serum Inflammatory Cytokines
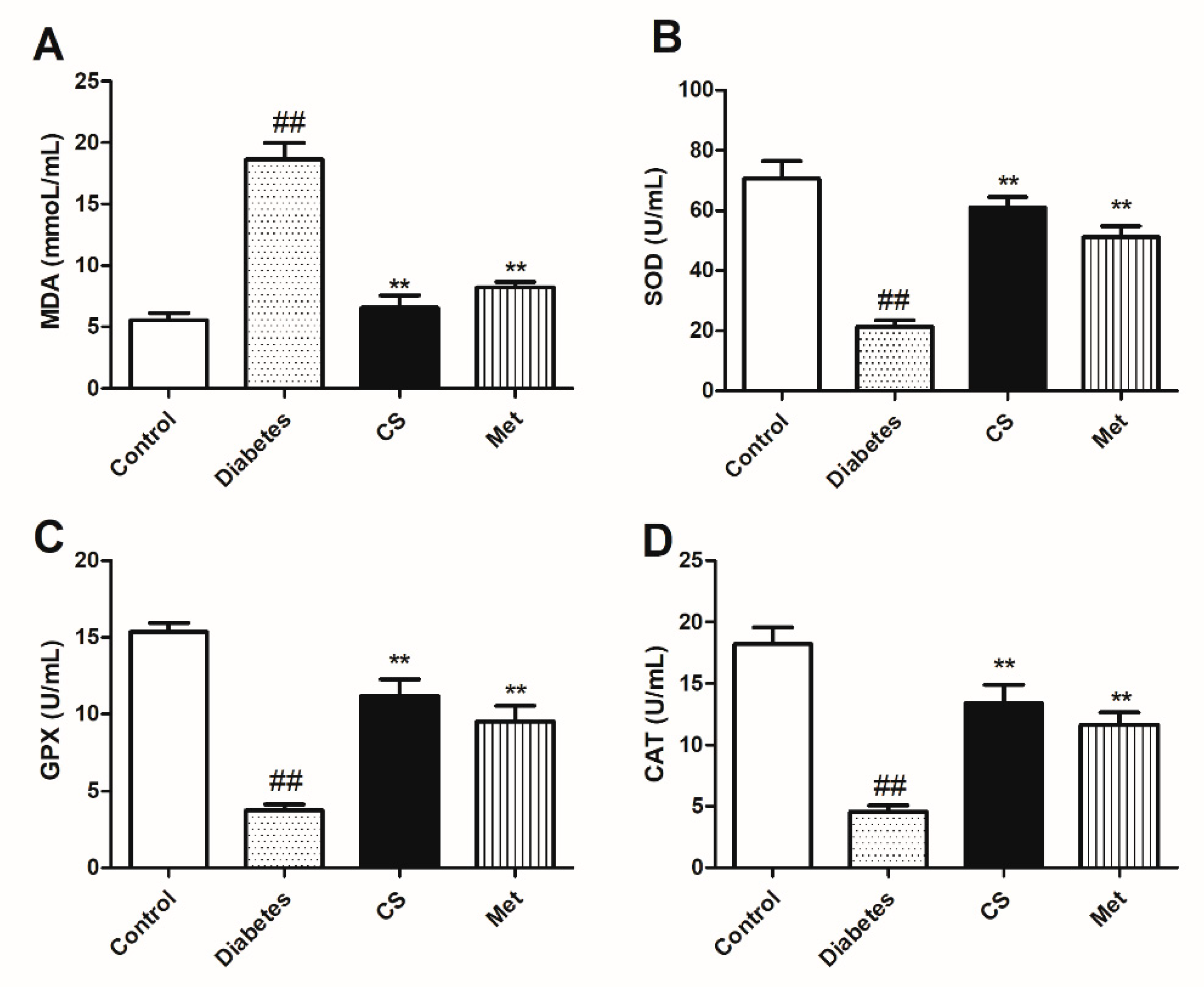
2.5. CS Inhibited Oxidative Stress of Diabetic Rats
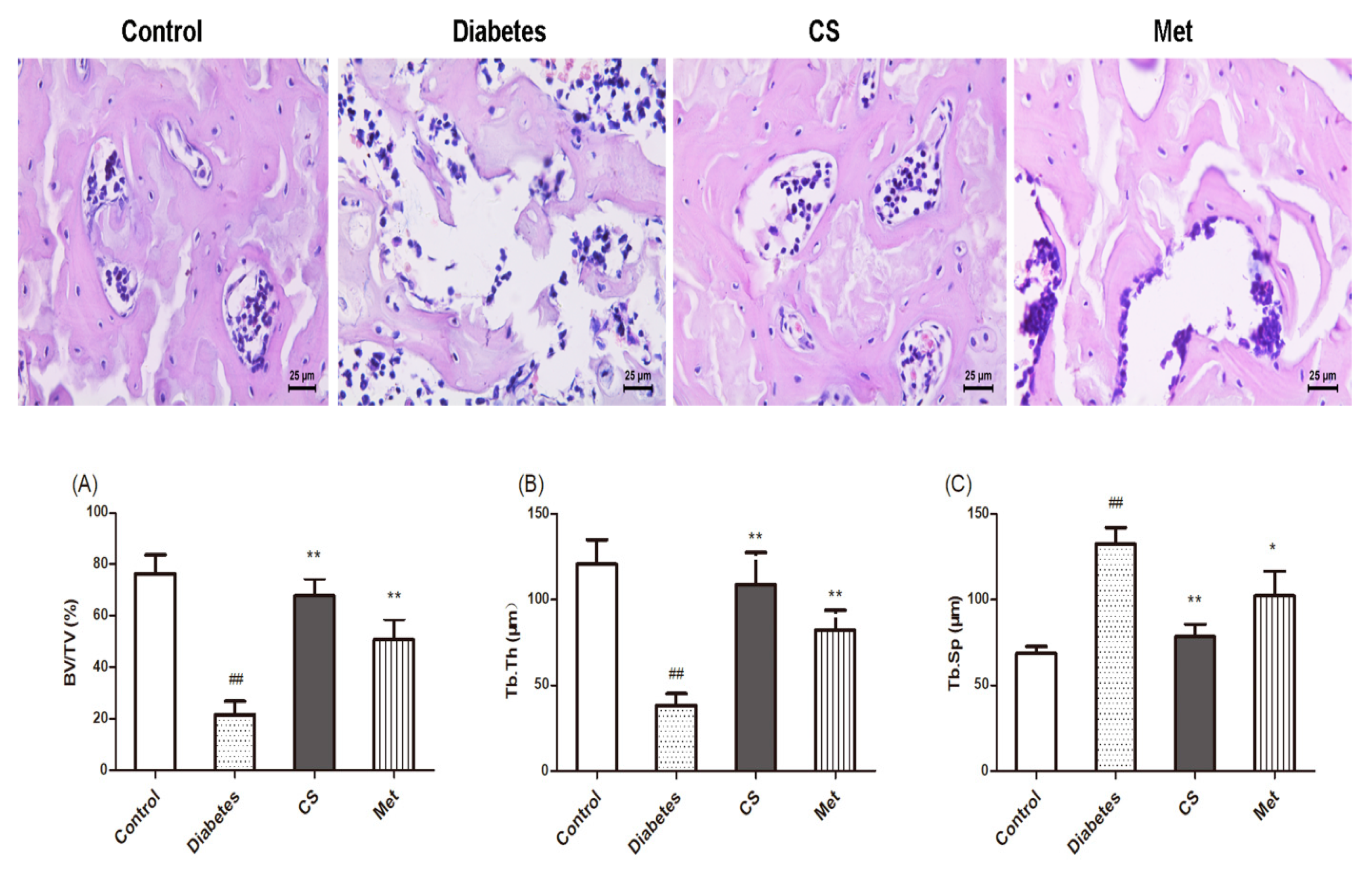
2.6. CS Repaired Bone Tissue Structure in Diabetic Rats
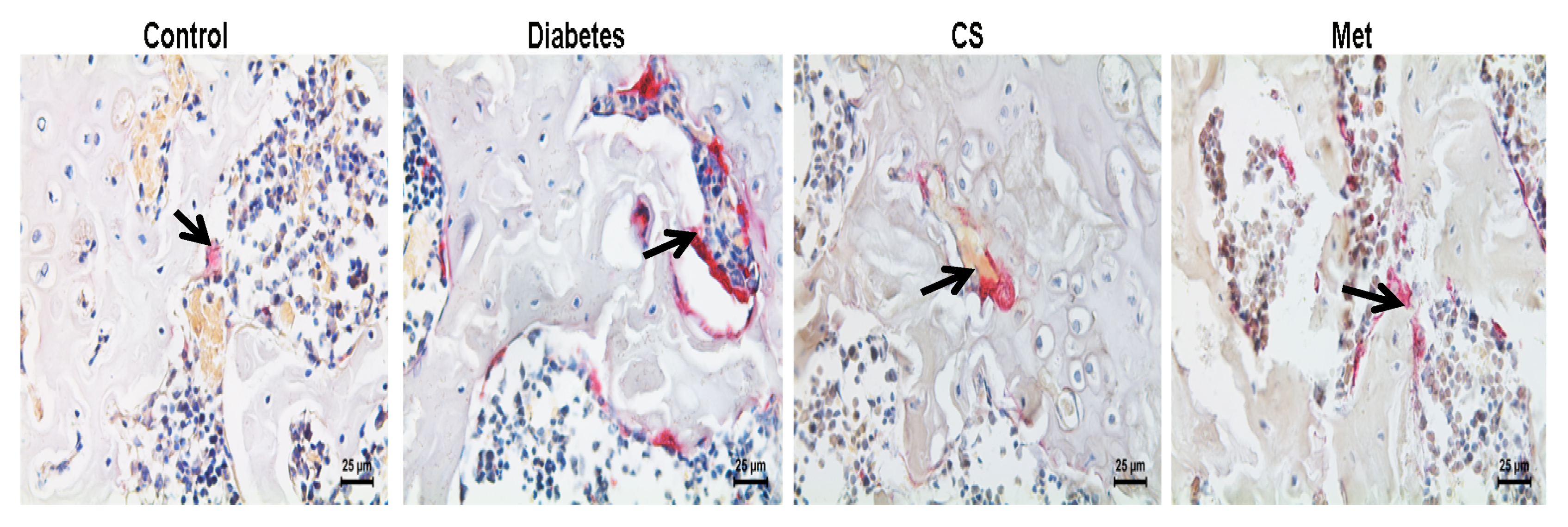
2.7. CS Inhibits Osteoclastogenesis in Diabetic Rats
2.8. CS Inhibits Bone Marrow Adipocytes in Diabetic Rats
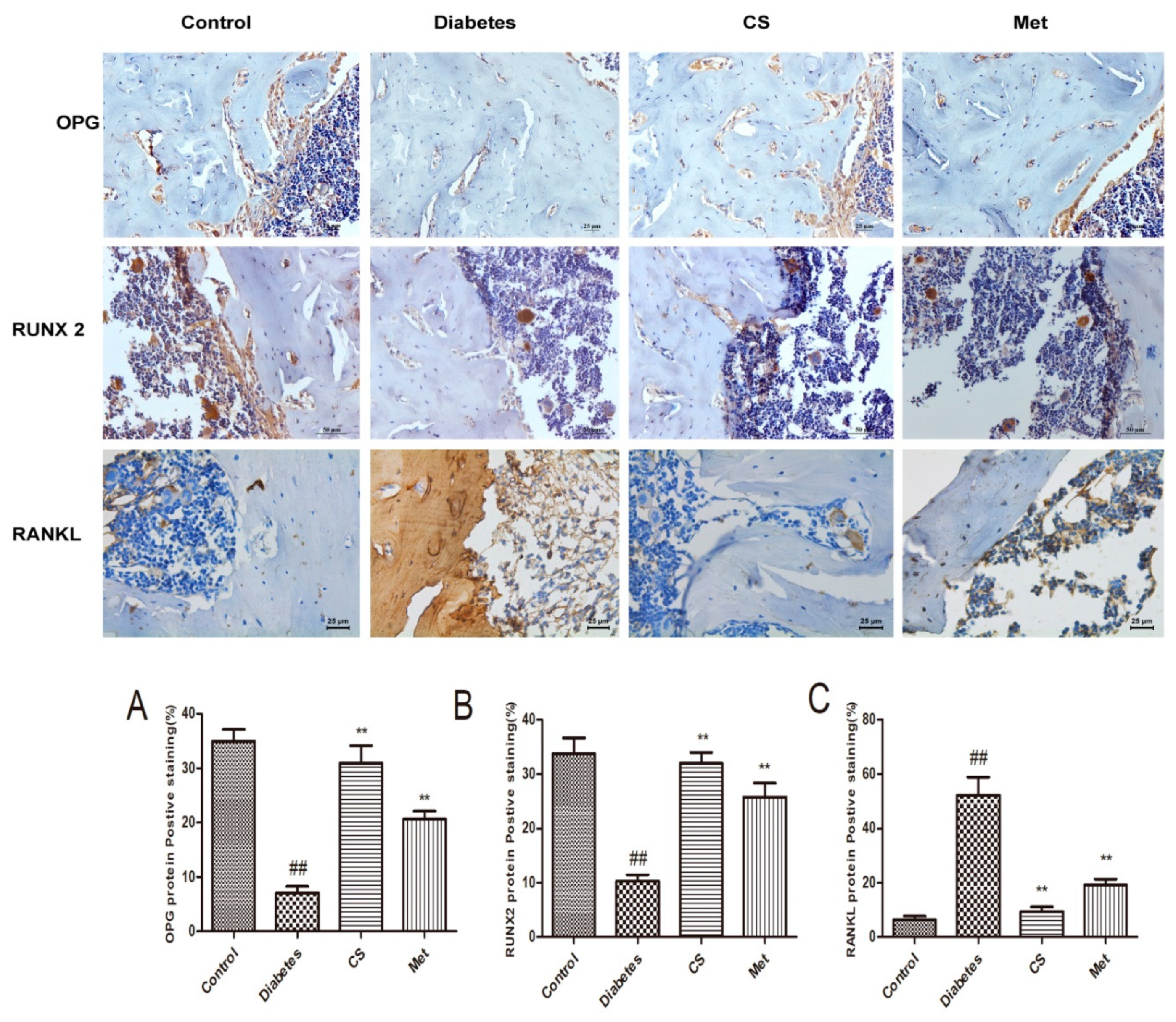
2.9. CS Regulated Bone OPG, RANKL and RUNX 2 in Diabetic Rats
3. Discussion
4. Materials and Methods
4.1. Animals and Reagents
4.2. Diabetes Model Induction and Treatment
4.3. Bone-Mineral Density Measurement
4.4. Serum Inflammatory Cytokines Detection
4.5. Serum Bone Turnover Marker Detection
4.6. Serum Oxidative Stress Index Detection
4.7. Bone Tissue Morphology and Bone Morphometric Parameters
4.8. Tibia Bone Marrow Adipocytes Observation
4.9. Bone TRAP Staining for Osteoclasts Observation
4.10. Bone OPG, RANKL, RUNX 2 Immunohistochemical Staining
4.11. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DOP | Diabetic osteoporosis |
| CS | Chondroitin sulfate |
| OPG | Osteoprotegerin |
| RANKL | Receptor activator of nuclear factor-κ B ligand |
| RUNX2 | Runt-related transcription factor 2 |
| STZ | Streptozotocin |
| CAT | Catalase |
| SOD | Superoxide dismutase |
| MDA | Malondialdehyde |
| GSH-Px | Glutathione peroxidase |
| AGEs | Advanced glycation end products |
| OS | Oxidative stress |
| CTX-1 | Cross-linked C-telopeptide of type I collagen |
| P1NP | Procollagen I N-terminal propeptide |
| BMSCs | Bone marrow stromal cells |
| ALP | Alkaline phosphatase |
| TRACP 5b | Tartrate-resistant acid phosphatase 5b |
References
- Sumida, Y.; Shima, T.; Mitsumoto, Y.; Katayama, T.; Umemura, A.; Yamaguchi, K.; Itoh, Y.; Yoneda, M.; Okanoue, T. Epidemiology, pathogenesis, and diagnostic strategy of diabetic liver disease in Japan. Int. J. Mol. Sci. 2020, 21, 4337. [Google Scholar] [CrossRef] [PubMed]
- Montagnani, A.; Gonnelli, S.; Alessandri, M.; Nuti, R. Osteoporosis and risk of fracture in patients with diabetes: An update. Aging Clin. Exp. Res. 2011, 23, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.S.; He, J.; Han, H.; Zheng, H.X.; Hu, Q.Y.; Jiang, H.; Li, X.S. Anthocyanin-Rich extract from black rice (Oryza sativa L. Japonica) ameliorates diabetic osteoporosis in rats. Food Funct. 2019, 10, 5350–5360. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.S.; He, J.; Zheng, H.X.; Lan, S.Q. Icariin prevents diabetes-induced bone loss in rats by reducing blood glucose and suppressing bone turnover. Molecules 2019, 24, 1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napoli, N.; Chandran, M.; Pierroz, D.; Abrahamsen, B.; Schwartz, A.V.; Ferrari, S.L. Mechanisms of diabetes mellitus-induced bone fragility. Nat. Rev. Endocrinol. 2017, 13, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Rathinavelu, S.; Guidry-Elizondo, C.; Banu, J. Molecular modulation of osteoblasts and osteoclasts in type 2 diabetes. J. Diabetes Res. 2018, 2018, 6354787. [Google Scholar] [CrossRef] [PubMed]
- Kalyanaraman, H.; Schwaerzer, G.; Ramdani, G.; Castillo, F.; Scott, B.T.; Dillmann, W.; Sah, R.L.; Casteel, D.E.; Pilz, R.B. Protein kinase G activation reverses oxidative stress and restores osteoblast function and bone formation in male mice with type 1 diabetes. Diabetes 2018, 67, 607–623. [Google Scholar] [CrossRef] [Green Version]
- Guo, C.J.; Xie, J.J.; Hong, R.H.; Pan, H.S.; Zhang, F.G.; Liang, Y.M. Puerarin alleviates streptozotocin (STZ)-induced osteoporosis in rats through suppressing inflammation and apoptosis via HDAC1/HDAC3 signaling. Biomed. Pharmacother. 2019, 115, 108570. [Google Scholar] [CrossRef]
- Asadipooya, K.; Uy, E.M. Advanced glycation end products (AGEs), receptor for AGEs, diabetes, and bone: Review of the literature. J. Endocr. Soc. 2019, 3, 1799–1818. [Google Scholar] [CrossRef] [Green Version]
- Kanazawa, I. Interaction between bone and glucose metabolism. Endocr. J. 2017, 64, 1043–1053. [Google Scholar] [CrossRef] [Green Version]
- Loi, F.; Córdova, L.A.; Pajarinen, J.; Lin, T.H.; Yao, Z.; Goodman, S.B. Inflammation, fracture and bone repair. Bone 2016, 86, 119–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, S.S.; Hu, Y.; Xie, P.L. Omentin-1 prevents inflammation-induced osteoporosis by down-regulating the pro-inflammatory cytokines. Bone Res. 2018, 6, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginaldi, L.; De Martinis, M. Osteoimmunology and beyond. Curr. Med. Chem. 2016, 23, 3754–3774. [Google Scholar] [CrossRef] [Green Version]
- De Martinis, M.; Sirufo, M.M.; Nocelli, C.; Fontanella, L.; Ginaldi, L. Hyperhomocysteinemia is associated with inflammation, bone resorption, vitamin B12 and folate deficiency and MTHFR C677T polymorphism in postmenopausal women with decreased bone mineral density. Int. J. Environ. Res. Public Health 2020, 17, 4260. [Google Scholar] [CrossRef] [PubMed]
- Katayama, Y.; Naitoh, M.; Kubota, H.; Yamawaki, S.; Aya, R.; Ishiko, T.; Morimoto, N. Chondroitin sulfate promotes the proliferation of keloid fibroblasts through activation of the integrin and protein kinase B pathways. Int. J. Mol. Sci. 2020, 21, 1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rani, A.; Patel, S.; Goyal, A. Chondroitin sulfate (CS) lyases: Structure, function and application in therapeutics. Curr. Protein Pept. Sci. 2018, 19, 22–33. [Google Scholar] [CrossRef]
- Ju, C.; Hou, L.; Sun, F.; Zhang, Z.; Gao, H.; Wang, L.; Wang, D.; Lv, Y.; Zhao, X. Anti-Oxidation and anti-apoptotic effects of chondroitin sulfate on 6-hydroxydopamine-induced injury through the up-regulation of Nrf2 and inhibition of mitochondria-mediated pathway. Neurochem. Res. 2015, 40, 1509–1519. [Google Scholar] [CrossRef]
- Nagano, F.; Mizuno, T.; Mizumoto, S.; Yoshioka, K.; Takahashi, K.; Tsuboi, N.; Maruyama, S.; Yamada, S.; Nagamatsu, T. Chondroitin sulfate protects vascular endothelial cells from toxicities of extracellular histones. Eur. J. Pharmacol. 2018, 826, 48–55. [Google Scholar] [CrossRef]
- Motoab, M.; Takamizawac, N.; Shibuyad, T.; Nakamurab, A.; Katsurayaa, K.; Katsuyuki, K. Anti-Diabetic effects of chondroitin sulfate on normal and type 2 diabetic mice. J. Funct. Foods 2018, 40, 336–340. [Google Scholar]
- Gomes, C.L.R.; Leão, C.L.; Venturotti, C.; Barreira, A.L.; Guimarães, G.; Fonseca, R.S.; Mourão, P.A.S.; Delgado, A.G.; Takiya, C.M.; Leite, M. The protective role of fucosylated chondroitin sulfate, a distinct glycosaminoglycan, in a murine model of streptozotocin-induced diabetic nephropathy. PLoS ONE 2014, 9, e106929. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.; Chang, Y.; He, M.; Wang, J.; Wang, Y.; Xue, C. Fucosylated chondroitin sulfate from sea cucumber improves insulin sensitivity via activation of PI3K/PKB pathway. J. Food Sci. 2014, 79, 1424–1429. [Google Scholar] [CrossRef] [PubMed]
- Carnovali, M.; Luzi, L.; Banfi, G.; Mariotti, M. Chronic hyperglycemia affects bone metabolism in adult zebrafish scale model. Endocrine 2016, 54, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Xia, W. Assessment of bone quality in patients with diabetes mellitus. Osteoporos. Int. 2018, 29, 1721–1736. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Sugimoto, T. Advanced glycation end products, diabetes, and bone strength. Curr. Osteoporos. Rep. 2016, 14, 320–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Martinis, M.; Ginaldi, L.; Sirufo, M.M.; Pioggia, G.; Calapai, G.; Gangemi, S.; Mannucci, C. Alarmins in osteoporosis, RAGE, IL-1, and IL-33 pathways: A literature review. Medicina (Kaunas) 2020, 56, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karstoft, K.; Pedersen, B.K. Exercise and type 2 diabetes: Focus on metabolism and inflammation. Immunol. Cell Biol. 2016, 94, 146–150. [Google Scholar] [CrossRef]
- Marahleh, A.; Kitaura, H.; Ohori, F.; Fujita, K.; Kawabata, T.; Kozawa, O.; Otsuka, T. TNF-α directly enhances osteocyte RANKL expression and promotes osteoclast formation. Front Immunol. 2019, 10, 2925. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; He, C. TNF-α and IL-6: The link between immune and bone system. Curr. Drug Targets 2020, 21, 213–227. [Google Scholar] [CrossRef]
- Shiratori, T.; Kyumoto-Nakamura, Y.; Kukita, A. IL-1β induces pathologically activated osteoclasts bearing extremely high levels of resorbing activity: A possible pathological subpopulation of osteoclasts, accompanied by suppressed expression of kindlin-3 and talin-1. J. Immunol. 2018, 200, 218–228. [Google Scholar] [CrossRef]
- Bacevic, M.; Brkovic, B.; Albert, A.; Rompen, E.; Radermecker, R.P.; Lambert, F. Does oxidative stress play a role in altered characteristics of diabetic bone? A systematic review. Calcif. Tissue Int. 2017, 101, 553–563. [Google Scholar] [CrossRef]
- Cheng, Y.Z.; Yang, S.L.; Wang, J.Y. Irbesartan attenuates advanced glycation end products-mediated damage in diabetes-associated osteoporosis through the AGEs/RAGE pathway. Life Sci. 2018, 205, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Starup-Linde, J.; Eriksen, S.A.; Lykkeboe, S.; Handberg, A.; Vestergaard, P. Biochemical markers of bone turnover in diabetes patients-A meta-analysis, and a methodological study on the effects of glucose on bone markers. Osteoporos. Int. 2014, 25, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Qi, S.S.; Chen, C. Salidroside improves bone histomorphology and prevents bone loss in ovariectomized diabetic rats by upregulating the OPG/RANKL ratio. Molecules 2018, 23, 2398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovács, B.; Vajda, E.; Nagy, E.E. Regulatory effects and interactions of the Wnt and OPG-RANKL-RANK signaling at the bone-cartilage interface in osteoarthritis. Int. J. Mol. Sci. 2019, 20, 4653. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wang, Z.; Duan, N.; Zhu, G.; Schwarz, E.M.; Xie, C. Osteoblast-Osteoclast interactions. Connect Tissue Res. 2018, 59, 99–107. [Google Scholar] [CrossRef]
- Conte, A.; Ghiraldini, B.; Casarin, R.C. Impact of type 2 diabetes on the gene expression of bone-related factors at sites receiving dental implants. Int. J. Oral Maxillofac. Surg. 2015, 44, 1302–1308. [Google Scholar] [CrossRef]
- Qi, S.S.; He, J.; Zheng, H.; Chen, C.; Jiang, H.; Lan, S. Zinc supplementation increased bone mineral density, improves bone histomorphology, and prevents bone loss in diabetic rat. Biol. Trace Elem. Res. 2020, 194, 493–501. [Google Scholar] [CrossRef]
- Yin, Q.; Wang, J.; Fu, Q.; Gu, S.; Rui, Y. CircRUNX2 through has-miR-203 regulates RUNX2 to prevent osteoporosis. J. Cell Mol. Med. 2018, 22, 6112–6121. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Chen, K.; Wei, B.; Liu, X.; Lei, Z.; Bai, X. Ginsenosides Rg3 attenuates glucocorticoid-induced osteoporosis through regulating BMP-2/BMPR1A/Runx2 signaling pathway. Chem. Biol. Interact. 2016, 256, 188–197. [Google Scholar] [CrossRef]
- Adil, M.; Khan, R.A.; Kalam, A.; Venkata, S.K.; Kandhare, A.D.; Ghosh, P.; Sharma, M. Effect of anti-diabetic drugs on bone metabolism: Evidence from preclinical and clinical studies. Pharmacol. Rep. 2017, 69, 1328–1340. [Google Scholar] [CrossRef]
- Wang, C.; Meng, H.; Wang, X.; Zhao, C.; Peng, J.; Wang, Y. Differentiation of bone marrow mesenchymal stem cells in osteoblasts and adipocytes and its role in treatment of osteoporosis. Med. Sci. Monit. 2016, 22, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Rivoira, M.; Rodríguez, V.; Picotto, G.; Battaglino, R. Naringin prevents bone loss in a rat model of type 1 Diabetes mellitus. Arch. Biochem. Biophys. 2018, 637, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Piccinin, M.A.; Khan, Z.A. Pathophysiological role of enhanced bone marrow adipogenesis in diabetic complications. Adipocytes 2014, 3, 263–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.T.; Ji, B.Y.; Zhang, Y.C. Role of metformin on osteoblast differentiation in type 2 diabetes. Biomed. Res. Int. 2019, 2019, 9203934. [Google Scholar]
- Bahrambeigi, S.; Yousefi, B.; Rahimi, M.; Shafiei-Irannejad, V. Metformin, an old antidiabetic drug with new potentials in bone disorders. Biomed. Pharmacother. 2019, 109, 1593–1601. [Google Scholar] [CrossRef]
- Zheng, L.; Shen, X.; Ye, J.; Xie, Y.; Yan, S. Metformin alleviates hyperglycemia-induced apoptosis and differentiation suppression in osteoblasts through inhibiting the TLR4 signaling pathway. Life Sci. 2019, 216, 29–38. [Google Scholar] [CrossRef]
- Rani, A.; Baruah, R.; Goyal, A. Physicochemical, antioxidant and biocompatible properties of chondroitin sulphate isolated from chicken keel bone for potential biomedical applications. Carbohydr. Polym. 2017, 159, 11–19. [Google Scholar] [CrossRef]
- Zou, Z.; Wei, M.; Fang, J.; Dai, W.; Sun, T.; Liu, Q.; Gong, G.; Liu, Y.; Song, S.; Ma, F.; et al. Preparation of chondroitin sulfates with different molecular weights from bovine nasal cartilage and their antioxidant activities. Int. J. Biol. Macromol. 2020, 152, 1047–1055. [Google Scholar] [CrossRef]
- De Martinis, M.; Sirufo, M.M.; Ginaldi, L. Osteoporosis: Current and emerging therapies targeted to immunological checkpoints. Curr. Med. Chem. 2019. [Google Scholar] [CrossRef]
- Revell, P.A. Histomorphometry of bone. J. Clin. Pathol. 1983, 36, 1323–1331. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | Diabetes | CS | Met |
|---|---|---|---|---|
| Blood glucose (mg dL−1) | 91.76 ± 6.94 | 401.85 ± 21.41 ## | 302.56 ± 16.77 ** | 226.74 ± 15.79 ** |
| ALP (U dL−1) | 89.78 ± 9.56 | 197.54 ± 11.70 ## | 99.89 ± 912 ** | 143.51 ± 7.34 * |
| CTX-1 (ng mL−1) | 31.20 ± 4.57 | 126.14 ± 13.32 ## | 46.89 ± 6.01 ** | 74.31 ± 7.68 ** |
| Osteocalcin (ng mL−1) | 16.78 ± 3.41 | 52.42 ± 5.31 ## | 20.46 ± 3.59 ** | 29.41 ± 6.48 ** |
| TRACP 5b (U dL−1) | 2.41 ± 0.44 | 5.37 ± 1.20 ## | 2.87 ± 0.59 ** | 3.96 ± 1.13 * |
| PINP (μg L−1) | 29.67 ± 3.95 | 69.80 ± 8.47 ## | 33.59 ± 3.90 ** | 51.78 ± 6.51 * |
| RUNX 2 (ng mL−1) | 13.10 ± 3.18 | 3.64 ± 0.57 ## | 10.89 ± 2.91 ** | 6.48 ± 2.10 * |
| OPG (ng mL−1) | 8.90 ± 1.48 | 2.39 ± 0.69 ## | 7.54 ± 0.94 ** | 4.89 ± 1.04 * |
| RANKL (ng mL−1) | 2.01 ± 0.38 | 9.45 ± 1.76 ## | 3.38 ± 0.57 ** | 5.80 ± 1.67 * |
| OPG/RANKL ratio | 4.36 ± 0.41 | 0.27 ± 0.08 ## | 2.51 ± 0.33 ** | 0.89 ± 0.04 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, H.X.; Chen, D.J.; Zu, Y.X.; Wang, E.Z.; Qi, S.S. Chondroitin Sulfate Prevents STZ Induced Diabetic Osteoporosis through Decreasing Blood Glucose, AntiOxidative Stress, Anti-Inflammation and OPG/RANKL Expression Regulation. Int. J. Mol. Sci. 2020, 21, 5303. https://doi.org/10.3390/ijms21155303
Zheng HX, Chen DJ, Zu YX, Wang EZ, Qi SS. Chondroitin Sulfate Prevents STZ Induced Diabetic Osteoporosis through Decreasing Blood Glucose, AntiOxidative Stress, Anti-Inflammation and OPG/RANKL Expression Regulation. International Journal of Molecular Sciences. 2020; 21(15):5303. https://doi.org/10.3390/ijms21155303
Chicago/Turabian StyleZheng, Hong Xing, De Jing Chen, Yue Xin Zu, En Zhu Wang, and Shan Shan Qi. 2020. "Chondroitin Sulfate Prevents STZ Induced Diabetic Osteoporosis through Decreasing Blood Glucose, AntiOxidative Stress, Anti-Inflammation and OPG/RANKL Expression Regulation" International Journal of Molecular Sciences 21, no. 15: 5303. https://doi.org/10.3390/ijms21155303
APA StyleZheng, H. X., Chen, D. J., Zu, Y. X., Wang, E. Z., & Qi, S. S. (2020). Chondroitin Sulfate Prevents STZ Induced Diabetic Osteoporosis through Decreasing Blood Glucose, AntiOxidative Stress, Anti-Inflammation and OPG/RANKL Expression Regulation. International Journal of Molecular Sciences, 21(15), 5303. https://doi.org/10.3390/ijms21155303