Circulating Vitamin D Levels and DNA Repair Capacity in Four Molecular Subtypes of Women with Breast Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Plasma 25(OH)D Levels
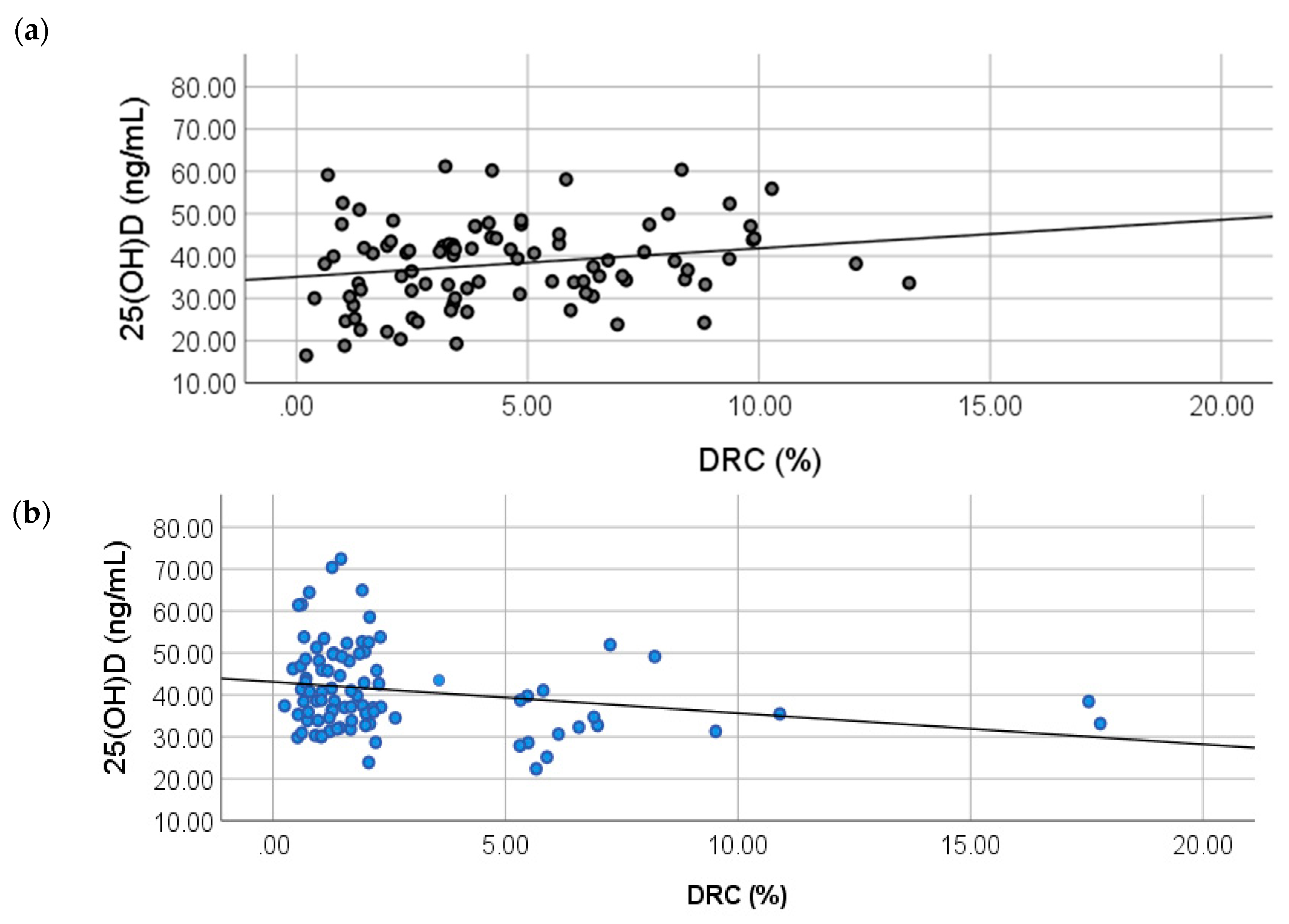
2.2. Correlation between 25(OH)D and DRC Levels
2.3. Relationship between Molecular Breast Cancer Subtypes and 25(OH)D Levels
3. Discussion
4. Materials and Methods
4.1. Patient Recruitment
4.2. Hormone Receptor Status
4.3. DNA Repair Capacity (DRC) Measurements
4.4. Calculation of DRC
4.5. Plasma 25-Hydroxyvitamin D Levels
4.6. Statistical Analyses
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Breast cancer |
| DRC | DNA repair capacity |
| LDRC | Low DRC |
| HDRC | High DRC |
| NER | Nucleotide excision repair |
| ER | Estrogen |
| PR | Progesterone |
| HER2 | Human epidermal growth factor receptor 2 |
| TN | Triple-negative |
| 25(OH)D | 25-hydroxyvitamin D |
| BMI | Body mass index |
| UV | Ultraviolet |
| IRB | Institutional Review Board |
| IHC | Immunohistochemistry |
| ASCO | American Society of Clinical Oncology |
| CAP | College of American Pathologists |
| FDA | Food and Drug Administration |
| FISH | Fluorescence In Situ Hybridization |
| HCR | Host-cell reactivation |
| CLIA | Clinical Laboratory Improvement Amendments |
| ANCOVA | Analysis of covariance |
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11; International Agency for Research on Cancer: Lyon, France, 2013. [Google Scholar]
- American Cancer Society. Breast Cancer Facts & Figures 2019–2020; American Cancer Society, Inc.: Atlanta, GA, USA, 2019. [Google Scholar]
- Martinez Tyson, D.; Medina-Ramirez, P.; Flores, A.M.; Siegel, R.; Aguado Loi, C. Unpacking Hispanic Ethnicity—Cancer Mortality Differentials among Hispanic Subgroups in the United States, 2004–2014. Front. Public Health 2018, 6, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasueda, A.; Urushima, H.; Ito, T. Efficacy and Interaction of Antioxidant Supplements as Adjuvant Therapy in Cancer Treatment: A Systematic Review. Integr. Cancer Ther. 2016, 15, 17–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, H.A.; Butrum, R.R.; Feldman, E.; Heber, D.; Nixon, D.; Picciano, M.F.; Rivlin, R.; Simopoulos, A.; Wargovich, M.J.; Weisburger, E.K.; et al. The Role of Dietary Supplements during Cancer Therapy. J. Nutr. 2003, 133, 3794S–3799S. [Google Scholar] [CrossRef] [Green Version]
- Jeon, S.-M.; Shin, E.-A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2018, 50, 20. [Google Scholar] [CrossRef] [Green Version]
- Kennel, K.A.; Drake, M.T. Vitamin D in the cancer patient. Curr. Opin. Support. Palliat. Care 2013, 7, 272–277. [Google Scholar] [CrossRef] [Green Version]
- Crew, K.D. Vitamin D: Are we ready to supplement for breast cancer prevention and treatment? ISRN Oncol. 2013, 2013, 483687. [Google Scholar] [CrossRef]
- Vergne, Y.; Matta, J.; Morales, L.; Vargas, W.; Alvarez-Garriga, C.; Bayona, M. Breast Cancer and DNA Repair Capacity: Association with Use of Multivitamin and Calcium Supplements. Integr. Med. 2013, 12, 38–46. [Google Scholar]
- Marteijn, J.A.; Lans, H.; Vermeulen, W.; Hoeijmakers, J.H. Understanding nucleotide excision repair and its roles in cancer and ageing. Nat. Rev. Mol. Cell Biol. 2014, 15, 465–481. [Google Scholar] [CrossRef]
- Wei, Q.; Cheng, L.; Hong, W.K.; Spitz, M.R. Reduced DNA repair capacity in lung cancer patients. Cancer Res. 1996, 56, 4103–4107. [Google Scholar]
- Wei, Q.; Matanoski, G.M.; Farmer, E.R.; Hedayati, M.A.; Grossman, L. DNA repair and aging in basal cell carcinoma: A molecular epidemiology study. Proc. Natl. Acad. Sci. USA 1993, 90, 1614–1618. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.J.; Hall, M.C.; Grossman, L.; Hedayati, M.; McCullough, D.L.; Lohman, K.; Case, L.D. Deficient Nucleotide Excision Repair Capacity Enhances Human Prostate Cancer Risk. Cancer Res. 2004, 64, 1197–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, J.M.; Ruiz, A.; Colen, R.; Lopez, I.D.; Grossman, L.; Matta, J.L. DNA repair and breast carcinoma susceptibility in women. Cancer 2004, 100, 1352–1357. [Google Scholar] [CrossRef] [PubMed]
- Matta, J.; Ortiz, C.; Encarnacion, J.; Dutil, J.; Suarez, E. Variability in DNA Repair Capacity Levels among Molecular Breast Cancer Subtypes: Triple Negative Breast Cancer Shows Lowest Repair. Int. J. Mol. Sci. 2017, 18, 1505. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.L.; Stevens, V.L.; Patel, R.; Jacobs, E.J.; Bain, E.B.; Horst, R.L.; Gapstur, S.M.; Thun, M.J.; Calle, E.E. Serum 25-hydroxyvitamin D concentrations and postmenopausal breast cancer risk: A nested case control study in the Cancer Prevention Study-II Nutrition Cohort. Breast Cancer Res. 2009, 11, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeb, K.K.; Trump, D.L.; Johnson, C.S. Vitamin D signalling pathways in cancer: Potential for anticancer therapeutics. Nat. Rev. Cancer 2007, 7, 684–700. [Google Scholar] [CrossRef]
- Palmieri, C.; MacGregor, T.; Girgis, S.; Vigushin, D. Serum 25-hydroxyvitamin D levels in early and advanced breast cancer. J. Clin. Pathol. 2006, 59, 1334–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peppone, L.J.; Rickles, A.S.; Janelsins, M.C.; Insalaco, M.R.; Skinner, K.S. The Association between Breast Cancer Prognostic Indicators and Serum 25-OH Vitamin D Levels. Ann. Surg. Oncol. 2012, 19, 2590–2599. [Google Scholar] [CrossRef] [Green Version]
- Swami, S.; Raghavachari, N.; Muller, U.R.; Bao, Y.P.; Feldman, D. Vitamin D Growth Inhibition of Breast Cancer Cells: Gene Expression Patterns Assessed by cDNA Microarray. Breast Cancer Res. Treat. 2003, 80, 49–62. [Google Scholar] [CrossRef]
- James, S.Y.; Mackay, A.G.; Colston, K.W. Effects of 1,25 dihydroxyvitamin D3 and its analogues on induction of apoptosis in breast cancer cells. J. Steroid Biochem. Mol. Biol. 1996, 58, 395–401. [Google Scholar] [CrossRef]
- Matthews, D.; LaPorta, E.; Zinser, G.M.; Narvaez, C.J.; Welsh, J. Genomic Vitamin D signaling in Breast Cancer: Insights from Animal Models and Human Cells. J. Steroid Biochem. Mol. Biol. 2010, 121, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Welsh, J. Vitamin D and breast cancer: Insights from animal models. Am. J. Clin. Nutr. 2004, 80 (Suppl. 6), 1721S–1724S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crew, K.D.; Gammon, M.D.; Steck, S.E.; Hershman, D.L.; Cremers, S.; Dworakowski, E.; Shane, E.; Terry, M.B.; Desai, M.; Teitelbaum, S.L.; et al. Association between Plasma 25-Hydroxyvitamin D and Breast Cancer Risk. Cancer Prev. Res. 2009, 2, 598–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodwin, P.J.; Ennis, M.; Pritchard, K.I.; Koo, J.; Hood, N. Prognostic effects of 25-hydroxyvitamin D levels in early breast cancer. J. Clin. Oncol. 2009, 27, 3757–3763. [Google Scholar] [CrossRef] [PubMed]
- Lumachi, F.; Santeufemia, D.A.; Basso, S.M. Current medical treatment of estrogen receptor-positive breast cancer. World J. Biol. Chem. 2015, 6, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Lisse, T.S.; Hewison, M.; Adams, J.S. Hormone response element binding proteins: Novel regulators of vitamin D and estrogen signaling. Steroids 2011, 76, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Martinez, N.; Diaz, L.; Ordaz-Rosado, D.; Garcia-Quiroz, J.; Barrera, D.; Avila, E.; Halhali, A.; Medina-Franco, H.; Ibarra-Sanchez, M.J.; Esparza-Lopez, J.; et al. Calcitriol restores antiestrogen responsiveness in estrogen receptor negative breast cancer cells: A potential new therapeutic approach. BMC Cancer 2014, 14, 230. [Google Scholar] [CrossRef] [Green Version]
- Encarnacion, J.; Ortiz, C.; Vergne, R.; Vargas, W.; Coppola, D.; Matta, J.L. High DRC Levels Are Associated with Let-7b Overexpression in Women with Breast Cancer. Int. J. Mol. Sci. 2016, 17, 865. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Guo, X.; Yu, X.; Liu, S.; Cui, X.; Zhang, B.; Liang, H. 25-Hydroxyvitamin D and Total Cancer Incidence and Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients 2019, 11, 2295. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Suarez, I.; Redwood, A.B.; Grotsky, D.A.; Neumann, M.A.; Cheng, E.H.; Stewart, C.L.; Dusso, A.; Gonzalo, S. A new pathway that regulates 53BP1 stability implicates cathepsin L and vitamin D in DNA repair. EMBO J. 2011, 30, 3383–3396. [Google Scholar] [CrossRef] [Green Version]
- Gonzalo, S. Novel roles of 1alpha,25(OH)2D3 on DNA repair provide new strategies for breast cancer treatment. J. Steroid Biochem. Mol. Biol. 2014, 144, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Wang, E.W.; Collins, A.R.; Pang, M.Y.C.; Siu, P.P.M.; Lai, C.K.Y.; Woo, J.; Benzie, I.F.F. Vitamin D and oxidation-induced DNA damage: Is there a connection? Mutagenesis 2016, 31, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Abbas, S.; Chang-Claude, J.; Linseisen, J. Plasma 25-hydroxyvitamin D and premenopausal breast cancer risk in a German case-control study. Int. J. Cancer 2009, 124, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Engel, P.; Fagherazzi, G.; Boutten, A.; Dupré, T.; Mesrine, S.; Boutron-Ruault, M.-C.; Clavel-Chapelon, F. Serum 25(OH) Vitamin D and Risk of Breast Cancer: A Nested Case-Control Study from the French E3N Cohort. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2341–2350. [Google Scholar] [CrossRef] [Green Version]
- Rejnmark, L.; Tietze, A.; Vestergaard, P.; Buhl, L.; Lehbrink, M.; Heickendorff, L.; Mosekilde, L. Reduced Prediagnostic 25-Hydroxyvitamin D Levels in Women with Breast Cancer: A Nested Case-Control Study. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2655–2660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertone-Johnson, E.R.; Chen, W.Y.; Holick, M.F.; Hollis, B.W.; Colditz, G.A.; Willett, W.C.; Hankinson, S.E. Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D and Risk of Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1991–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Lee, Y.M.; Ko, B.S.; Lee, J.W.; Yu, J.H.; Son, B.H.; Gong, G.-Y.; Kim, S.B.; Ahn, S.H. Vitamin D Deficiency is Correlated with Poor Outcomes in Patients with Luminal-type Breast Cancer. Ann. Surg. Oncol. 2011, 18, 1830–1836. [Google Scholar] [CrossRef] [Green Version]
- Kawase, T.; Matsuo, K.; Suzuki, T.; Hirose, K.; Hosono, S.; Watanabe, M.; Inagaki, M.; Iwata, H.; Tanaka, H.; Tajima, K. Association between vitamin D and calcium intake and breast cancer risk according to menopausal status and receptor status in Japan. Cancer Sci. 2010, 101, 1234–1240. [Google Scholar] [CrossRef]
- Farrag, S.E.; Dwivedi, A.K.; Otoukesh, S.; Badri, N.J.; Sanchez, L.A.; Nahleh, Z.A. Prevalence of Low Vitamin D in Patients with Breast Cancer in a Predominantly Hispanic Population at the American-Mexican Border. Nutr. Cancer 2017, 69, 819–824. [Google Scholar] [CrossRef]
- Wu, Y.; Sarkissyan, M.; Clayton, S.; Chlebowski, R.; Vadgama, J.V. Association of Vitamin D3 Level with Breast Cancer Risk and Prognosis in African-American and Hispanic Women. Cancers 2017, 9, 144. [Google Scholar] [CrossRef]
- Suarez-Martinez, E.B.; Perez, C.M.; Cruz, S.K.; Khorsandi, S.; Chardon, C.; Ferder, L. Importance of vitamin D and vitamin D levels status in Puerto Ricans. J. Health Care Poor Underserved 2013, 24 (Suppl. 4), 38–47. [Google Scholar] [CrossRef]
- Palacios, C.; Gil, K.; Pérez, C.M.; Joshipura, K. Determinants of Vitamin D Status among Overweight and Obese Puerto Rican Adults. Ann. Nutr. Metab. 2012, 60, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dávila, L.H.; Rivera, N.R.; Valentin, M.L.; Haddock, L.; Martínez, R.R.; Bossolo, A.G.; Vick, M.R. Prevalence of vitamin D insufficiency and deficiency among medical residents of the University Hospital in San Juan, Puerto Rico. Puerto Rico Health Sci. J. 2015, 34, 83–88. [Google Scholar]
- Janowsky, E.C.; Lester, G.E.; Weinberg, C.R.; Millikan, R.C.; Schildkraut, J.M.; Garrett, P.A.; Hulka, B.S. Association between low levels of 1,25-dihydroxyvitamin D and breast cancer risk. Public Health Nutr. 1999, 2, 283–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, S.; Kwan, M.L.; Ergas, I.J.; Roh, J.M.; Cheng, T.D.; Hong, C.C.; McCann, S.E.; Tang, L.; Davis, W.; Liu, S.; et al. Association of Serum Level of Vitamin D at Diagnosis with Breast Cancer Survival: A Case-Cohort Analysis in the Pathways Study. JAMA Oncol. 2017, 3, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Koh, B.S.; Yu, J.H.; Lee, J.W.; Son, B.H.; Kim, S.B.; Ahn, S.H. Changes in serum hydroxyvitamin D levels of breast cancer patients during tamoxifen treatment or chemotherapy in premenopausal breast cancer patients. Eur. J. Cancer 2014, 50, 1403–1411. [Google Scholar] [CrossRef]
- Kok, D.E.; van den Berg, M.M.G.A.; Posthuma, L.; van ’t Erve, I.; van Duijnhoven, F.J.B.; de Roos, W.K.; Grosfeld, S.; Los, M.; Sommeijer, D.W.; van Laarhoven, H.W.M.; et al. Changes in Circulating Levels of 25-hydroxyvitamin D3 in Breast Cancer Patients Receiving Chemotherapy. Nutr. Cancer 2019, 71, 756–766. [Google Scholar] [CrossRef] [Green Version]
- Ambrosone, C.B.; Zirpoli, G.R.; Hutson, A.D.; McCann, W.E.; McCann, S.E.; Barlow, W.E.; Kelly, K.M.; Cannioto, R.; Sucheston-Campbell, L.E.; Hershman, D.L.; et al. Dietary Supplement Use During Chemotherapy and Survival Outcomes of Patients with Breast Cancer Enrolled in a Cooperative Group Clinical Trial (SWOG S0221). J. Clin. Oncol. 2020, 38, 804–814. [Google Scholar] [CrossRef]
- Matta, J.; Echenique, M.; Negron, E.; Morales, L.; Vargas, W.; Gaetan, F.S.; Lizardi, E.R.; Torres, A.; Rosado, J.O.; Bolanos, G.; et al. The association of DNA Repair with breast cancer risk in women. A comparative observational study. BMC Cancer 2012, 12, 490. [Google Scholar] [CrossRef] [Green Version]
- Deng, H.W.; Li, J.; Li, J.L.; Johnson, M.; Gong, G.; Davis, K.M.; Recker, R.R. Change of bone mass in postmenopausal Caucasian women with and without hormone replacement therapy is associated with vitamin D receptor and estrogen receptor genotypes. Hum. Genet. 1998, 103, 576–585. [Google Scholar] [CrossRef]
- Yetley, E.A. Assessing the vitamin D status of the US population. Am. J. Clin. Nutr. 2008, 88, 558S–564S. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. Arch. Pathol. Lab. Med. 2014, 138, 241–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, M.E.; Hayes, D.F.; Wolff, A.C.; Mangu, P.B.; Temin, S. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer. J. Oncol. Pract. Am. Soc. Clin. Oncol. 2010, 6, 195–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez, P.; Taron, M.; Moran, T.; Fernandez, M.A.; Requena, G.; Rosell, R. A modified host-cell reactivation assay to quantify DNA repair capacity in cryopreserved peripheral lymphocytes. DNA Repair 2011, 10, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Athas, W.F.; Hedayati, M.A.; Matanoski, G.M.; Farmer, E.R.; Grossman, L. Development and field-test validation of an assay for DNA repair in circulating human lymphocytes. Cancer Res. 1991, 51, 5786–5793. [Google Scholar] [PubMed]
- Wang, L.; Wei, Q.; Shi, Q.; Guo, Z.; Qiao, Y.; Spitz, M.R. A modified host-cell reactivation assay to measure repair of alkylating DNA damage for assessing risk of lung adenocarcinoma. Carcinogenesis 2007, 28, 1430–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Controls | BC Cases | p-Value 1 |
|---|---|---|---|
| n = 92 (50.27%) | n = 91 (49.73%) | ||
| DRC | <0.0001 | ||
| Low (<3.8%) | 46 (25.13) | 74 (40.44) | |
| High (≥3.8%) | 46 (25.14) | 17 (9.29) | |
| Age | 0.6520 | ||
| 21–40 | 23 (12.57) | 19 (10.38) | |
| 41–60 | 54 (29.51) | 53 (28.96) | |
| 61+ | 15 (8.20) | 19 (10.38) | |
| BMI | 1.0000 | ||
| <25 kg/m2 | 31 (16.94) | 32 (17.49) | |
| ≥25 kg/m2 | 60 (32.79) | 59 (32.24) | |
| Missing | 1 (0.55) | - | |
| Ever been pregnant | 0.6775 | ||
| Yes | 80 (43.72) | 77 (42.08) | |
| No | 12 (6.56) | 14 (7.65) | |
| Ever breastfeed | 0.0528 | ||
| Yes | 47 (25.68) | 32 (17.49) | |
| No | 32 (17.49) | 42 (22.95) | |
| Missing | 13 (7.10) | 17 (9.29) | |
| Length of breastfeeding | 0.0281 | ||
| Never | 45 (24.59) | 59 (32.24) | |
| 1–5 months | 17 (9.29) | 26 (14.21) | |
| ≥6 months | 27 (14.75) | 6 (3.28) | |
| Missing | 3 (1.64) | - | |
| Oral contraceptive use | 1.0000 | ||
| Yes | 47 (25.68) | 46 (25.14) | |
| No | 45 (24.59) | 44 (24.04) | |
| Missing | - | 1 (0.55) | |
| Age started oral contraceptive | 0.1446 | ||
| <20 | 14 (7.65) | 8 (4.37) | |
| ≥21 | 29 (15.85) | 36 (19.67) | |
| Missing | 4 (2.19) | 2 (1.09) | |
| Menopause | 0.8441 | ||
| Yes | 15 (8.20) | 16 (8.74) | |
| No | 75 (40.98) | 71 (38.80) | |
| Missing | 2 (1.09) | 4 (2.19) | |
| BC history in any family member | 0.2709 | ||
| Yes | 26 (14.21) | 33 (18.03) | |
| No | 66 (36.07) | 58 (31.69) | |
| Family history of cancer (not BC) | 0.2850 | ||
| Yes | 54 (29.51) | 61 (33.33) | |
| No | 38 (20.77) | 30 (16.39) | |
| Season of blood collection | 0.6768 | ||
| Spring (Feb–Apr) | 30 (16.39) | 23 (12.57) | |
| Summer (May–Jul) | 19 (10.38) | 24 (13.11) | |
| Fall (Aug–Oct) | 21 (11.48) | 22 (12.02) | |
| Winter (Nov–Jan) | 22 (12.02) | 22 (12.02) |
| Stratifications | 25(OH)D (ng/mL) (Mean ± SD) a | 25(OH)D (ng/mL) (Mean ± SD) * | p-Value | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Controls | 38.10 (9.95) | 38.55 (1.03) | 0.123 a, 0.001 * | 36.51 | 40.59 |
| BC Cases | 41.12 (10.25) | 40.82 (1.03) | 38.79 | 42.85 | |
| Controls LDRC | 35.41 (10.46) | 35.74(1.40) | 0.0001 a, 0.0001* | 32.98 | 38.43 |
| Controls HDRC | 41.18 (8.43) | 41.27 (1.41) | 38.49 | 44.05 | |
| BC Cases LDRC | 42.55 (10.25) | 42.36 (1.10) | 40.18 | 44.53 | |
| BC Cases HDRC | 34.90 (7.78) | 34.59 (2.30) | 30.06 | 39.13 | |
| Stratifications | Mean 25(OH)D Difference (ng/mL) | Significance b | 95% Confidence Interval for Difference b | ||
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Controls LDRC | Controls HDRC | −5.54 * | 0.006 | −9.45 | −1.63 |
| BC cases LDRC | −6.62 * | 0.0001 | −10.14 | −3.10 | |
| BC cases HDRC | 1.14 | 0.671 | −4.17 | 6.45 | |
| Controls HDRC | Controls LDRC | 5.54 * | 0.006 | 1.63 | 9.45 |
| BC cases LDRC | −1.09 | 0.545 | −4.62 | 2.45 | |
| BC cases HDRC | 6.68 * | 0.014 | 1.36 | 12.00 | |
| BC cases LDRC | Controls LDRC | 6.62 * | 0.0001 | 3.10 | 10.14 |
| Controls HDRC | 1.09 | 0.545 | −2.45 | 4.62 | |
| BC cases HDRC | 7.77 * | 0.003 | 2.74 | 12.80 | |
| BC cases HDRC | Controls LDRC | −1.14 | 0.617 | −6.45 | 4.17 |
| Controls HDRC | −6.68 * | 0.014 | −12.00 | −1.36 | |
| BC cases LDRC | −7.77 * | 0.003 | −12.80 | −2.74 | |
| Stratifications | R2 | Testing Significance | ||
|---|---|---|---|---|
| Model 1 | Model 2 | p-Value a | p-Value * | |
| Controls | 0.215 | - | 0.040 | 0.043 |
| BC Cases | - | −0.236 | 0.030 | 0.026 |
| Stratifications | 25(OH)D (ng/mL) (Mean ± SD) a | 25(OH)D (ng/mL) (Mean ± SD) * | p-Value | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Controls | 38.41 (10.46) | 35.51 (1.36) | 0.0025 a, 0.001 * | 32.81 | 38.211 |
| Luminal A | 38.46 (6.79) | 38.73 (2.26) | 34.23 | 43.22 | |
| Luminal B | 40.99 (8.22) | 40.50(2.78) | 34.98 | 46.03 | |
| HER2+ | 48.83 (11.34) | 47.70 (3.14) | 41.46 | 53.94 | |
| Triple-negative | 44.71 (10.26) | 45.08 (2.24) | 40.62 | 49.53 | |
| Stratifications | Mean 25(OH)D Difference | Significance b | 95% Confidence Interval for Difference b | ||
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Controls | Luminal A | 3.21 | 0.225 | −8.45 | 2.01 |
| Luminal B | −4.99 | 0.110 | −11.14 | 1.16 | |
| HER2+ | −12.19 * | 0.001 | −19.01 | −5.38 | |
| TN | −9.57 * | 0.0001 | −14.78 | −4.36 | |
| Luminal A | Controls | 3.21 | 0.225 | −2.02 | 8.45 |
| Luminal B | −1.78 | 0.621 | −8.90 | 5.34 | |
| HER2+ | −8.98 * | 0.025 | −16.78 | −1.18 | |
| TN | −6.35 | 0.050 | −12.71 | 0.002 | |
| Luminal B | Controls | 4.99 | 0.110 | −1.16 | 11.14 |
| Luminal A | 1.78 | 0.621 | −5.34 | 8.90 | |
| HER2+ | −7.20 | 0.089 | −15.52 | 1.13 | |
| TN | −4.58 | 0.204 | −11.68 | 2.53 | |
| HER2+ | Controls | 12.19 * | 0.001 | 5.38 | 19.05 |
| Luminal A | 8.98 * | 0.025 | 1.18 | 16.78 | |
| Luminal B | 7.20 | 0.089 | −1.13 | 15.53 | |
| TN | 2.63 | 0.497 | −5.01 | 10.26 | |
| TN | Controls | 9.57 * | 0.0001 | 4.36 | 14.78 |
| Luminal A | 6.35 | 0.050 | −0.002 | 12.71 | |
| Luminal B | 4.58 | 0.204 | −2.53 | 11.68 | |
| HER2+ | −2.63 | 0.497 | −10.26 | 5.01 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Sánchez, C.; Encarnación-Medina, J.; Vergne, R.; Padilla, L.; Matta, J. Circulating Vitamin D Levels and DNA Repair Capacity in Four Molecular Subtypes of Women with Breast Cancer. Int. J. Mol. Sci. 2020, 21, 6880. https://doi.org/10.3390/ijms21186880
Ortiz-Sánchez C, Encarnación-Medina J, Vergne R, Padilla L, Matta J. Circulating Vitamin D Levels and DNA Repair Capacity in Four Molecular Subtypes of Women with Breast Cancer. International Journal of Molecular Sciences. 2020; 21(18):6880. https://doi.org/10.3390/ijms21186880
Chicago/Turabian StyleOrtiz-Sánchez, Carmen, Jarline Encarnación-Medina, Ralphdy Vergne, Luis Padilla, and Jaime Matta. 2020. "Circulating Vitamin D Levels and DNA Repair Capacity in Four Molecular Subtypes of Women with Breast Cancer" International Journal of Molecular Sciences 21, no. 18: 6880. https://doi.org/10.3390/ijms21186880
APA StyleOrtiz-Sánchez, C., Encarnación-Medina, J., Vergne, R., Padilla, L., & Matta, J. (2020). Circulating Vitamin D Levels and DNA Repair Capacity in Four Molecular Subtypes of Women with Breast Cancer. International Journal of Molecular Sciences, 21(18), 6880. https://doi.org/10.3390/ijms21186880