
MMPs and TIMPs Expression Levels in the Periodontal Ligament during Orthodontic Tooth Movement: A Systematic Review of In Vitro and In Vivo Studies

 , , and
, , and
Abstract
:1. Introduction
2. Results
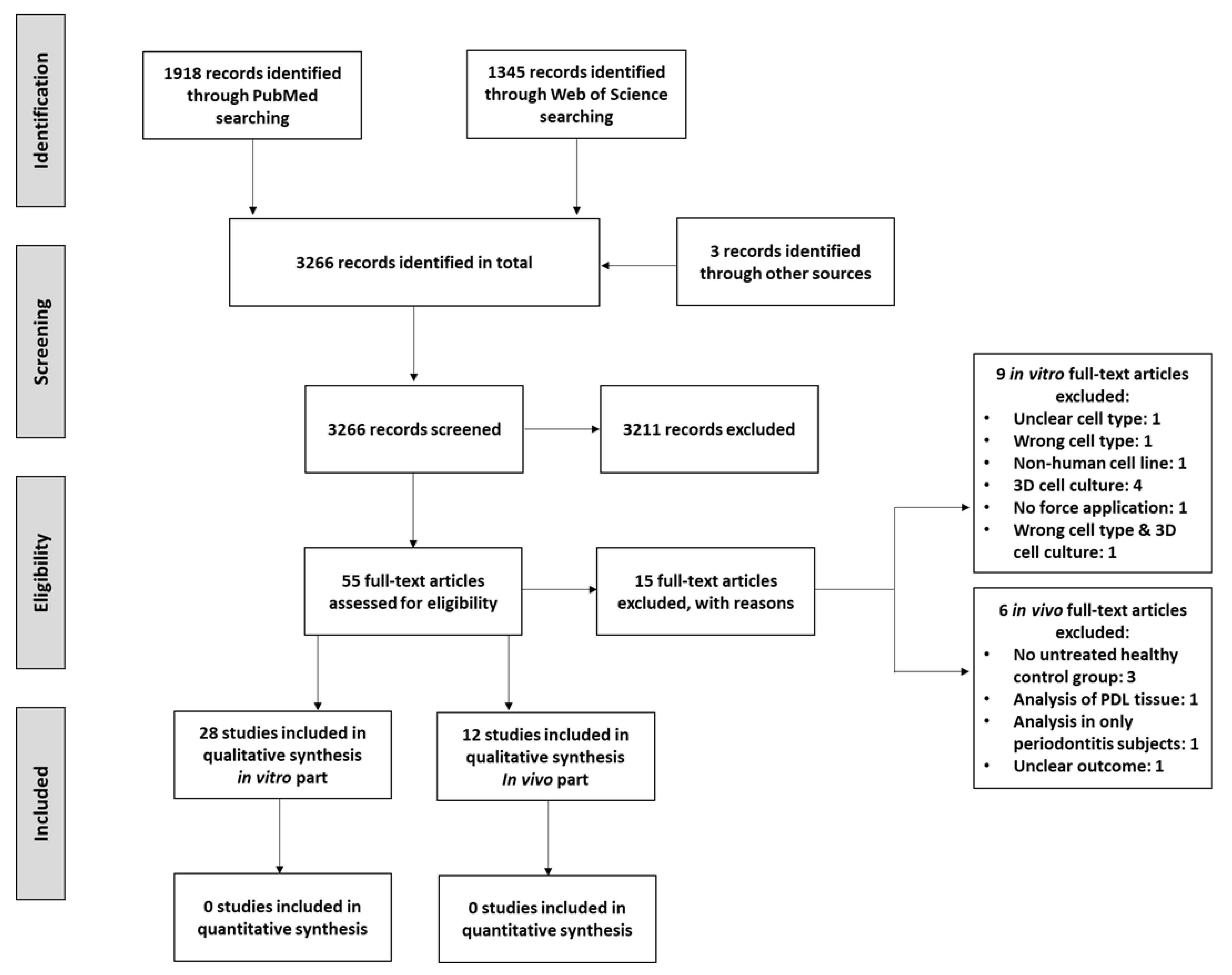
2.1. Systematic Search Results
2.2. In Vitro Studies
2.2.1. Sample Parameters
2.2.2. Intervention Parameters
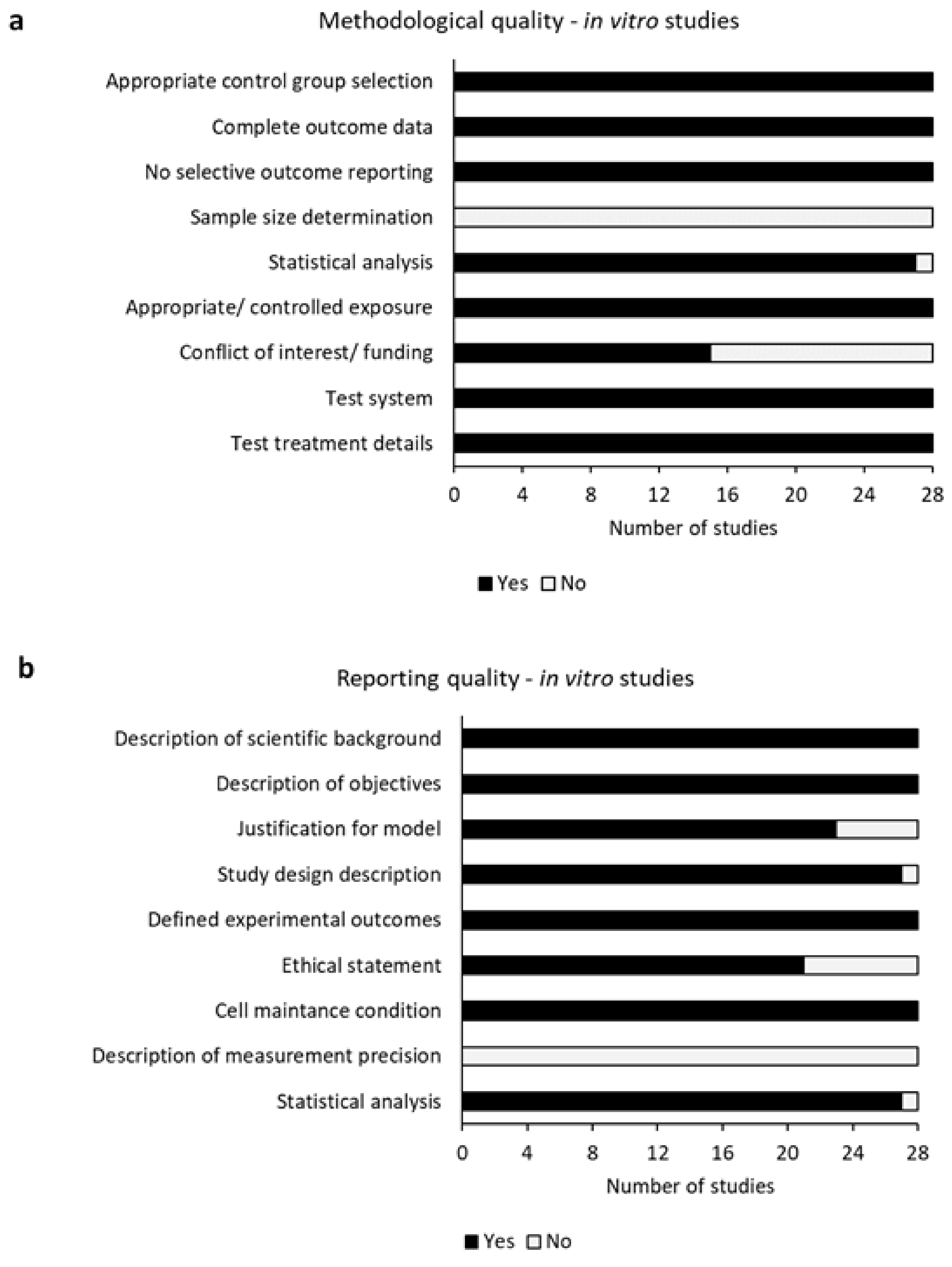
2.2.3. Risk of Bias Assessment
2.2.4. In Vitro MMPs Express Levels
2.2.5. In Vitro TIMPs Express Levels
2.3. In Vivo Studies
2.3.1. Patient Parameters
2.3.2. Intervention Parameters
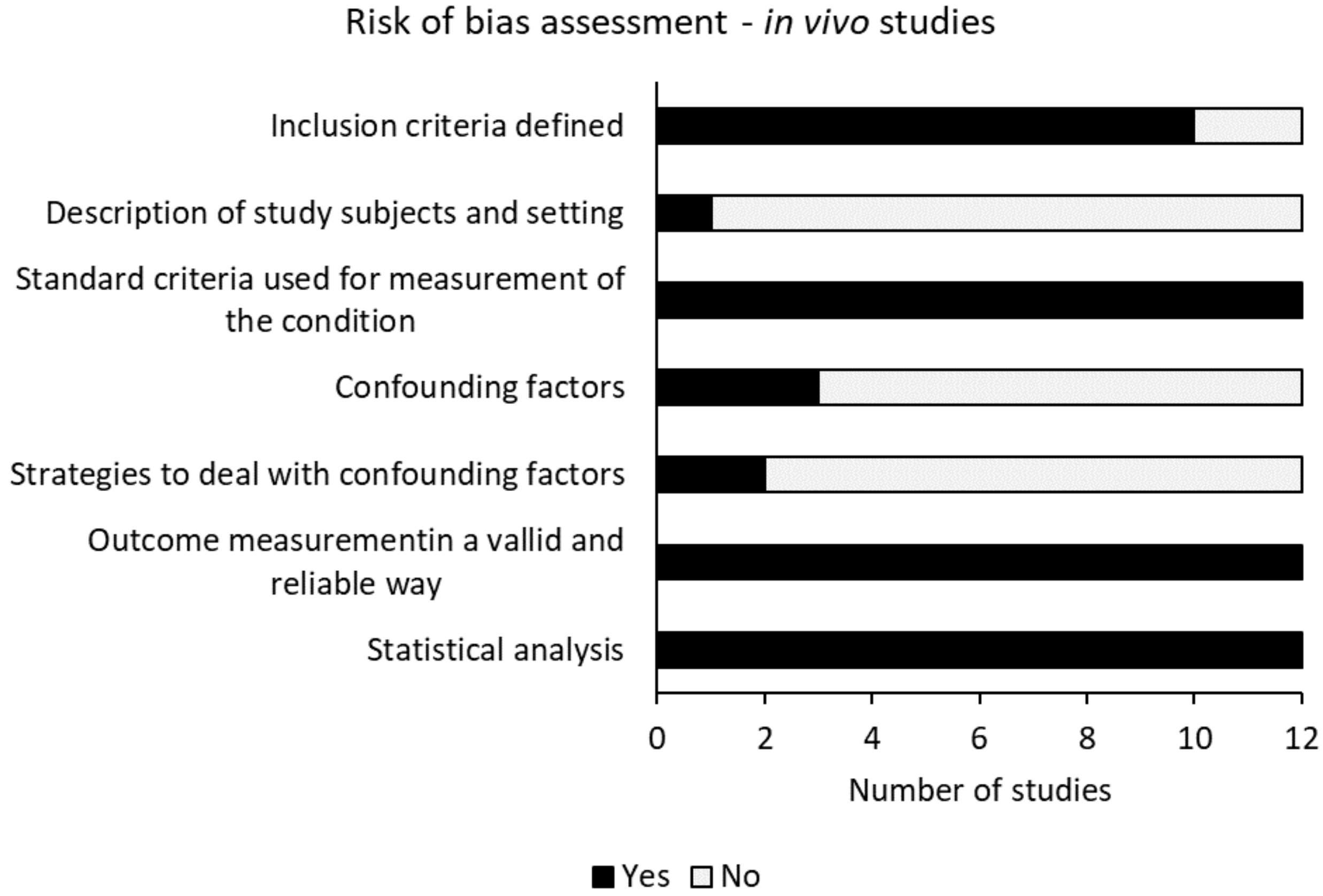
2.3.3. Risk of Bias Assessment
2.3.4. In Vivo MMPs Expression Levels
2.3.5. In Vivo TIMPs Expression Levels
3. Discussion
4. Materials and Methods
4.1. Database Search and Screening Strategy
4.2. Eligibility Criteria
4.3. Data Synthesis
4.4. Risk of Bias Assessment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wada, N.; Gronthos, S.; Bartold, P.M. Immunomodulatory effects of stem cells. Periodontol. 2000 2013, 63, 198–216. [Google Scholar] [CrossRef]
- Beertsen, W.; McCulloch, C.A.G.; Sodek, J. The periodontal ligament: A unique, multifunctional connective tissue. Periodontol. 2000 1997, 13, 20–40. [Google Scholar] [CrossRef]
- Tantilertanant, Y.; Niyompanich, J.; Everts, V.; Supaphol, P.; Pavasant, P.; Sanchavanakit, N. Cyclic tensile force-upregulated IL6 increases MMP3 expression by human periodontal ligament cells. Arch. Oral Biol. 2019, 107, 104495. [Google Scholar] [CrossRef]
- Kanzaki, H.; Chiba, M.; Shimizu, Y.; Mitani, H. Periodontal ligament cells under mechanical stress induce osteoclastogenesis by receptor activator of nuclear factor κB ligand up-regulation via prostaglandin E2 synthesis. J. Bone Miner. Res. 2002, 17, 210–220. [Google Scholar] [CrossRef] [Green Version]
- Kook, S.H.; Jang, Y.S.; Lee, J.C. Involvement of JNK-AP-1 and ERK-NF-κB signaling in tension-stimulated expression of Type i collagen and MMP-1 in human periodontal ligament fibroblasts. J. Appl. Physiol. 2011, 111, 1575–1583. [Google Scholar] [CrossRef] [Green Version]
- Rosselli-Murai, L.K.; Almeida, L.O.; Zagni, C.; Galindo-Moreno, P.; Padial-Molina, M.; Volk, S.L.; Murai, M.J.; Rios, H.F.; Squarize, C.H.; Castilho, R.M. Periostin responds to mechanical stress and tension by activating the MTOR signaling pathway. PLoS ONE 2013, 8, e83580. [Google Scholar] [CrossRef]
- Yamashiro, K.; Myokai, F.; Hiratsuka, K.; Yamamoto, T.; Senoo, K.; Arai, H.; Nishimura, F.; Abiko, Y.; Takashiba, S. Oligonucleotide array analysis of cyclic tension-responsive genes in human periodontal ligament fibroblasts. Int. J. Biochem. Cell Biol. 2007, 39, 910–921. [Google Scholar] [CrossRef]
- He, Y.; Macarak, E.J.; Korostoff, J.M.; Howard, P.S. Compression and tension: Differential effects on matrix accumulation by periodontal ligaments fibroblasts in vitro. Connect. Tissue Res. 2004, 45, 28–39. [Google Scholar] [CrossRef]
- Chen, Y.J.; Jeng, J.H.; Chang, H.H.; Huang, M.Y.; Tsai, F.F.; Jane Yao, C.C. Differential regulation of collagen, lysyl oxidase and MMP-2 in human periodontal ligament cells by low- and high-level mechanical stretching. J. Periodontal Res. 2013, 48, 466–474. [Google Scholar] [CrossRef]
- Cantarella, G.; Cantarella, R.; Caltabiano, M.; Risuglia, N.; Bernardini, R.; Leonardi, R. Levels of matrix metalloproteinases 1 and 2 in human gingival crevicular fluid during initial tooth movement. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 568-e11. [Google Scholar] [CrossRef] [PubMed]
- Cui, N.; Hu, M.; Khalil, R.A. Biochemical and Biological Attributes of Matrix Metalloproteinases. Prog. Mol. Biol. Transl. Sci. 2017, 147, 1–73. [Google Scholar] [PubMed] [Green Version]
- Ma, J.; Zhao, D.; Wu, Y.; Xu, C.; Zhang, F. Cyclic stretch induced gene expression of extracellular matrix and adhesion molecules in human periodontal ligament cells. Arch. Oral Biol. 2015, 60, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Grimm, S.; Wolff, E.; Walter, C.; Pabst, A.M.; Mundethu, A.; Jacobs, C.; Wehrbein, H.; Jacobs, C. Influence of clodronate and compressive force on IL-1ß-stimulated human periodontal ligament fibroblasts. Clin. Oral Investig. 2020, 24, 343–350. [Google Scholar] [CrossRef]
- Nettelhoff, L.; Grimm, S.; Jacobs, C.; Walter, C.; Pabst, A.M.; Goldschmitt, J.; Wehrbein, H. Influence of mechanical compression on human periodontal ligament fibroblasts and osteoblasts. Clin. Oral Investig. 2016, 20, 621–629. [Google Scholar] [CrossRef]
- Bolcato-Bellemin, A.I.; Elkaim, R.; Abehsera, A.; Fausser, J.L.; Haikel, Y.; Tenenbaum, H. Expression of mRNAs encoding for α and β integrin subunits, MMPs and TIMPs in stretched human periodontal ligament and gingival fibroblasts. J. Dent. Res. 2000, 79, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.F.; Li, Y.H.; Ren, Y.J.; Cao, Z.G.; Long, X. The effect of a single nucleotide polymorphism in the matrix metalloproteinase-1 (MMP-1) promoter on force-induced MMP-1 expression in human periodontal ligament cells. Eur. J. Oral Sci. 2008, 116, 319–323. [Google Scholar] [CrossRef]
- Jacobs, C.; Walter, C.; Ziebart, T.; Grimm, S.; Meila, D.; Krieger, E.; Wehrbein, H. Induction of IL-6 and MMP-8 in human periodontal fibroblasts by static tensile strain. Clin. Oral Investig. 2014, 18, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.; Schramm, S.; Dirks, I.; Walter, C.; Pabst, A.; Meila, D.; Jacobs, C.; Wehrbein, H. Mechanical loading increases pro-inflammatory effects of nitrogen-containing bisphosphonate in human periodontal fibroblasts. Clin. Oral Investig. 2018, 22, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, R.A.; Lisboa, F.A.; De Castro Santos, G.; Andrade, M.V.M.; Cunha-Melo, J.R. Matrix metalloproteinase 2 activity decreases in human periodontal ligament fibroblast cultures submitted to simulated orthodontic force. In Vitro Cell. Dev. Biol. Anim. 2009, 45, 614–621. [Google Scholar] [CrossRef]
- Lisboa, R.A.; Andrade, M.V.; Cunha-Melo, J.R. Zimography is an effective method for detection of matrix metalloproteinase 2 (MMP-2) activity in cultured human fibroblasts. Acta Cir. Bras. 2013, 28, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, R.A.; Andrade, M.V.; Cunha-Melo, J.R. Toll-like receptor activation and mechanical force stimulation promote the secretion of matrix metalloproteinases 1, 3 and 10 of human periodontal fibroblasts via p38, JNK and NF-kB. Arch. Oral Biol. 2013, 58, 731–739. [Google Scholar] [CrossRef]
- Long, P.; Liu, F.; Piesco, N.P.; Kapur, R.; Agarwal, S. Signaling by mechanical strain involves transcriptional regulation of proinflammatory genes in human periodontal ligament cells in vitro. Bone 2002, 30, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Narimiya, T.; Wada, S.; Kanzaki, H.; Ishikawa, M.; Tsuge, A.; Yamaguchi, Y.; Nakamura, Y. Orthodontic tensile strain induces angiogenesis via type IV collagen degradation by matrix metalloproteinase-12. J. Periodontal Res. 2017, 52, 842–852. [Google Scholar] [CrossRef]
- Nemoto, T.; Kajiya, H.; Tsuzuki, T.; Takahashi, Y.; Okabe, K. Differential induction of collagens by mechanical stress in human periodontal ligament cells. Arch. Oral Biol. 2010, 55, 981–987. [Google Scholar] [CrossRef]
- Proff, P.; Reicheneder, C.; Faltermeier, A.; Kubein-Meesenburg, D.; Römer, P. Effects of mechanical and bacterial stressors on cytokine and growth-factor expression in periodontal ligament cells. J. Orofac. Orthop. Fortschr. Kieferorthop. 2014, 75, 191–202. [Google Scholar] [CrossRef]
- Redlich, M.; Roos, H.; Reichenberg, E.; Zaks, B.; Grosskop, A.; Bar Kana, I.; Pitaru, S.; Palmon, A. The effect of centrifugal force on mRNA levels of collagenase, collagen type-I, tissue inhibitors of metalloproteinases and β-actin in cultured human periodontal ligament fibroblasts. J. Periodontal Res. 2004, 39, 27–32. [Google Scholar] [CrossRef]
- Saminathan, A.; Vinoth, K.J.; Wescott, D.C.; Pinkerton, M.N.; Milne, T.J.; Cao, T.; Meikle, M.C. The effect of cyclic mechanical strain on the expression of adhesion-related genes by periodontal ligament cells in two-dimensional culture. J. Periodontal Res. 2012, 47, 212–221. [Google Scholar] [CrossRef]
- Schröder, A.; Gubernator, J.; Nazet, U.; Spanier, G.; Jantsch, J.; Proff, P.; Kirschneck, C. Effects of sodium chloride on the gene expression profile of periodontal ligament fibroblasts during tensile strainAuswirkungen von Natriumchlorid auf das Genexpressionsprofil parodontaler Ligamentfibroblasten bei Dehnung. J. Orofac. Orthop. Fortschr. Kieferorthop. 2020, 81, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, K.; Uno, K.; Zhang, G.X.; Tamura, M. Periodontal ligament cells under intermittent tensile stress regulate mRNA expression of osteoprotegerin and tissue inhibitor of matrix metalloprotease-1 and -2. J. Bone Miner. Metab. 2004, 22, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Wescott, D.C.; Pinkerton, M.N.; Gaffey, B.J.; Beggs, K.T.; Milne, T.J.; Meikle, M.C. Osteogenic gene expression by human periodontal ligament cells under cyclic tension. J. Dent. Res. 2007, 86, 1212–1216. [Google Scholar] [CrossRef]
- Zheng, L.; Huang, Y.; Song, W.; Gong, X.; Liu, M.; Jia, X.; Zhou, G.; Chen, L.; Li, A.; Fan, Y. Fluid shear stress regulates metalloproteinase-1 and 2 in human periodontal ligament cells: Involvement of extracellular signal-regulated kinase (ERK) and P38 signaling pathways. J. Biomech. 2012, 45, 2368–2375. [Google Scholar] [CrossRef]
- Zheng, L.; Shi, Q.; Na, J.; Liu, N.; Guo, Y.; Fan, Y. Platelet-Derived Growth Factor Receptor-α and β are Involved in Fluid Shear Stress Regulated Cell Migration in Human Periodontal Ligament Cells. Cell. Mol. Bioeng. 2019, 12, 85–97. [Google Scholar] [CrossRef]
- Ziegler, N.; Alonso, A.; Steinberg, T.; Woodnutt, D.; Kohl, A.; Müssig, E.; Schulz, S.; Tomakidi, P. Mechano-transduction in periodontal ligament cells identifies activated states of MAP-kinases p42/44 and p38-stress kinase as a mechanism for MMP-13 expression. BMC Cell Biol. 2010, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behm, C.; Nemec, M.; Blufstein, A.; Schubert, M.; Rausch-Fan, X.; Andrukhov, O.; Jonke, E. Interleukin-1β induced matrix metalloproteinase expression in human periodontal ligament-derived mesenchymal stromal cells under in vitro simulated static orthodontic forces. Int. J. Mol. Sci. 2021, 22, 1027. [Google Scholar] [CrossRef] [PubMed]
- Fujihara, C.; Yamada, S.; Ozaki, N.; Takeshita, N.; Kawaki, H.; Takano-Yamamoto, T.; Murakami, S. Role of mechanical stress-induced glutamate signaling-associated molecules in cytodifferentiation of periodontal ligament cells. J. Biol. Chem. 2010, 285, 28286–28297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacopian, N.; Nik, T.H.; Ghahremani, M.H.; Rahimi, H.R.; Ostad, S.N. Effects of continuous and interrupted forces on gene transcription in periodontal ligament cells in vitro. Acta Med. Iran. 2011, 49, 643–649. [Google Scholar]
- Alikhani, M.; Chou, M.Y.; Khoo, E.; Alansari, S.; Kwal, R.; Elfersi, T.; Almansour, A.; Sangsuwon, C.; Al Jearah, M.; Nervina, J.M.; et al. Age-dependent biologic response to orthodontic forces. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 632–644. [Google Scholar] [CrossRef]
- Surlin, P.; Silosi, I.; Rauten, A.M.; Cojocaru, M.; Foia, L. Involvement of TSP1 and MMP9/NGAL in angiogenesis during orthodontic periodontal remodeling. Sci. World J. 2014, 214, 421029. [Google Scholar] [CrossRef]
- Zhang, B.; Yang, L.; Zheng, W.; Lin, T. MicroRNA-34 expression in gingival crevicular fluid correlated with orthodontic tooth movement. Angle Orthod. 2020, 90, 702–706. [Google Scholar] [CrossRef] [Green Version]
- Apajalahti, S.; Sorsa, T.; Railavo, S.; Ingman, T. The in vivo levels of matrix metalloproteinase-1 and -8 in gingival crevicular fluid during initial orthodontic tooth movement. J. Dent. Res. 2003, 82, 1018–1022. [Google Scholar] [CrossRef]
- Bildt, M.M.; Bloemen, M.; Kuijpers-Jagtman, A.M.; Von Den Hoff, J.W. Matrix metalloproteinases and tissue inhibitors of metalloproteinases in gingival crevicular fluid during orthodontic tooth movement. Eur. J. Orthod. 2009, 31, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Capelli, J.; Kantarci, A.; Haffajee, A.; Teles, R.P.; Fidel, R.; Figueredo, C.M. Matrix metalloproteinases and chemokines in the gingival crevicular fluid during orthodontic tooth movement. Eur. J. Orthod. 2011, 33, 705–711. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.; Wilson, J.; Rock, P.; Chapple, I. Induction of cytokines, MMP9, TIMPs, RANKL and OPG during orthodontic tooth movement. Eur. J. Orthod. 2013, 35, 644–651. [Google Scholar] [CrossRef] [Green Version]
- Ingman, T.; Apajalahti, S.; Mäntylä, P.; Savolainen, P.; Sorsa, T. Matrix metalloproteinase-1 and -8 in gingival crevicular fluid during orthodontic tooth movement: A pilot study during 1 month of follow-up after fixed appliance activation. Eur. J. Orthod. 2005, 27, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribagin, L.S.; Rashkova, M.R. Matrix metalloproteinase-8 and interleukin-1beta in gingival fluid of children in the first three months of orthodontic treatment with fixed appliances. Folia Med. 2012, 54, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rody, W.J.; Wijegunasinghe, M.; Wiltshire, W.A.; Dufault, B. Differences in the gingival crevicular fluid composition between adults and adolescents undergoing orthodontic treatment. Angle Orthod. 2014, 84, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirozaki, M.U.; da Silva, R.A.B.; Romano, F.L.; da Silva, L.A.B.; De Rossi, A.; Lucisano, M.P.; Messora, M.R.; Feres, M.; Novaes Júnior, A.B. Clinical, microbiological, and immunological evaluation of patients in corrective orthodontic treatment. Prog. Orthod. 2020, 21, 6. [Google Scholar] [CrossRef]
- Ku, S.J.; Chang, Y.I.; Chae, C.H.; Kim, S.G.; Park, Y.W.; Jung, Y.K.; Choi, J.Y. Static tensional forces increase osteogenic gene expression in three-dimensional periodontal ligament cell culture. BMB Rep. 2009, 42, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Carano, A.; Siciliani, G. Effects of continuous and intermittent forces on human fibroblasts in vitro. Eur. J. Orthod. 1996, 18, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Grünheid, T.; Zentner, A. Extracellular matrix synthesis, proliferation and death in mechanically stimulated human gingival fibroblasts in vitro. Clin. Oral Investig. 2005, 9, 124–130. [Google Scholar] [CrossRef]
- Karasawa, Y.; Tanaka, H.; Nakai, K.; Tanabe, N.; Kawato, T.; Maeno, M.; Shimizu, N. Tension Force Downregulates Matrix Metalloproteinase Expression and Upregulates the Expression of Their Inhibitors through MAPK Signaling Pathways in MC3T3-E1 cells. Int. J. Med. Sci. 2015, 12, 905. [Google Scholar] [CrossRef] [Green Version]
- Pei, D.; Wang, M.; Li, W.; Li, M.; Liu, Q.; Ding, R.; Zhao, J.; Li, A.; Li, J.; Xu, F.; et al. Remodeling of aligned fibrous extracellular matrix by encapsulated cells under mechanical stretching. Acta Biomater. 2020, 112, 202–212. [Google Scholar] [CrossRef]
- Von Den Hoff, J.W. Effects of mechanical tension on matrix degradation by human periodontal ligament cells cultured in collagen gels. J. Periodontal Res. 2003, 38, 449–457. [Google Scholar] [CrossRef]
- Watanabe, T.; Yasue, A.; Fujihara, S.; Tanaka, E. PERIOSTIN regulates MMP-2 expression via the αvβ3 integrin/ERK pathway in human periodontal ligament cells. Arch. Oral Biol. 2012, 57, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Nan, L.; Zheng, Y.; Liao, N.; Li, S.; Wang, Y.; Chen, Z.; Wei, L.; Zhao, S.; Mo, S. Mechanical force promotes the proliferation and extracellular matrix synthesis of human gingival fibroblasts cultured on 3D PLGA scaffolds via TGF-β expression. Mol. Med. Rep. 2019, 19, 2107–2114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saloom, H.F.; Carpenter, G.H.; Cobourne, M.T. A cross-sectional cohort study of gingival crevicular fluid biomarkers in normal-weight and obese subjects during orthodontic treatment with fixed appliances. Angle Orthod. 2019, 89, 930–935. [Google Scholar] [CrossRef] [Green Version]
- Rody, W.J.; Elmaraghy, S.; McNeight, A.M.; Chamberlain, C.A.; Antal, D.; Dolce, C.; Wheeler, T.T.; McGorray, S.P.; Shaddox, L.M. Effects of different orthodontic retention protocols on the periodontal health of mandibular incisors. Orthod. Craniofac. Res. 2016, 19, 198–208. [Google Scholar] [CrossRef]
- Saloom, H.F.; Papageorgiou, S.N.; Carpenter, G.H.; Cobourne, M.T. Impact of Obesity on Orthodontic Tooth Movement in Adolescents: A Prospective Clinical Cohort Study. J. Dent. Res. 2017, 96, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garlet, T.P.; Coelho, U.; Silva, J.S.; Garlet, G.P. Cytokine expression pattern in compression and tension sides of the periodontal ligament during orthodontic tooth movement in humans. Eur. J. Oral Sci. 2007, 115, 355–362. [Google Scholar] [CrossRef]
- Almeida, R.C.; Capelli, J.; Teles, R.P. Levels of gingival crevicular fluid matrix metalloproteinases in periodontally compromised teeth under orthodontic forces. Angle Orthod. 2015, 85, 1009–1014. [Google Scholar] [CrossRef] [Green Version]
- Canavarro, C.; Teles, R.P.; Capelli Júnior, J. Matrix metalloproteinases-1, -2, -3, -7, -8, -12, and -13 in gingival crevicular fluid during orthodontic tooth movement: A longitudinal randomized split-mouth study. Eur. J. Orthod. 2013, 35, 652–658. [Google Scholar] [CrossRef] [Green Version]
- Akashi, S.; Saitoh, S.; Wakabayashi, Y.; Kikuchi, T.; Takamura, N.; Nagai, Y.; Kusumoto, Y.; Fukase, K.; Kusumoto, S.; Adachi, Y.; et al. Lipopolysaccharide Interaction with Cell Surface Toll-like Receptor 4-MD-2. J. Exp. Med. 2003, 198, 1035–1042. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Yang, R.; Zhou, Y.H. Mechanobiology of periodontal ligament stem cells in orthodontic tooth movement. Stem Cells Int. 2018, 2018, 65312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bildt, M.M.; Henneman, S.; Maltha, J.C.; Kuijpers-Jagtman, A.M.; Von den Hoff, J.W. CMT-3 inhibits orthodontic tooth displacement in the rat. Arch. Oral Biol. 2007, 52, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Holliday, L.S.; Vakani, A.; Archer, L.; Dolce, C. Effects of matrix metalloproteinase inhibitors on bone resorption and orthodontic tooth movement. J. Dent. Res. 2003, 82, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Brauchli, L.M.; Senn, C.; Ball, J.; Wichelhaus, A. Force levels of 23 nickel-titanium open-coil springs in compression testing. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Rozman, J.; Mrvar, P.; Drevenšek, M.; Pečlin, P. Evaluation of NiTi Superelastic Retraction Coil Springs for orthodontic tooth movement in rats. Biomed. Mater. Eng. 2010, 20, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Nokhbehsaim, M.; Deschner, B.; Winter, J.; Bourauel, C.; Jäger, A.; Jepsen, S.; Deschner, J. Anti-inflammatory effects of EMD in the presence of biomechanical loading and interleukin-1β in vitro. Clin. Oral Investig. 2012, 16, 275–283. [Google Scholar] [CrossRef]
- Da Monini, A.C.; Gandini, L.G.; Vianna, A.P.; Martins, R.P.; Jacob, H.B. Tooth movement rate and anchorage lost during canine retraction: A maxillary and mandibular comparison. Angle Orthod. 2019, 89, 559–565. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Samuel, G.O.; Hoffmann, S.; Wright, R.A.; Lalu, M.M.; Patlewicz, G.; Becker, R.A.; DeGeorge, G.L.; Fergusson, D.; Hartung, T.; Lewis, R.J.; et al. Guidance on assessing the methodological and reporting quality of toxicologically relevant studies: A scoping review. Environ. Int. 2016, 92, 630–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Cells | Teeth | Donor Gender | Donor Age | Number of Included Donors |
|---|---|---|---|---|---|---|
| Behm et al. | 2021 | Human PDL cells (hPDL-MSCs) | Third molars | - | - | 4 donors |
| Bolcato-Bellemin et al. | 2000 | Human PDL fibroblasts | - | Female | - | 1 donor |
| Chen et al. | 2013 | Human PDL fibroblasts | Premolars | - | “young” | 3 donors |
| Fujihara et al. | 2010 | Human PDL cells | - | - | - | - |
| Grimm et al. | 2020 | Human PDL fibroblasts | - | - | - | Commercially available HPdLFs |
| Hacopian et al. | 2011 | Human PDL fibroblasts | Premolars | - | - | 3 donors |
| Huang et al. | 2008 | Human PDL cells | Premolars | Female | 4.5 ± 1.8 years | 16 donors |
| Jacobs et al. | 2014 | Human PDL fibroblasts | - | - | - | Commercially available HPdLFs |
| Jacobs et al. | 2018 | Human PDL fibroblasts | - | - | - | Commercially available HPdLFs |
| Kook et al. | 2011 | Human PDL fibroblasts | - | Male | 20–30 years | - |
| Lisboa et al. | 2009 | Human PDL fibroblasts | Third molars | Male + female | - | 36 donors (43 teeth, only 26 used) |
| Lisboa et al. | 2013 | Human PDL fibroblasts | Third molars | - | - | - |
| Lisboa et al. | 2013 | Human PDL fibroblasts | Third molars | - | - | - |
| Long et al. | 2002 | Human PDL cells | Impacted healthy third molars | Male + female | 16 + 18 years | At least 3 donors |
| Ma et al. | 2015 | Human PDL cells | Premolars | Female | 11 years old | 1 donor |
| Narimiya et al. | 2017 | Human PDL cell line | - | - | - | Human immortalized PDL cell lines |
| Nemoto et al. | 2010 | Human PDL cells | Third molars | - | 2 × 20 years, 1 × 40 years | 3 donors |
| Nettelhoff et al. | 2016 | Human PDL fibroblasts | - | - | - | Commercially available HPdLFs |
| Proff et al. | 2014 | Human PDL fibroblasts | - | Male | 18–25 years | 4 donors |
| Redlich et al. | 2004 | Human PDL fibroblasts | Premolars | - | - | At least 3 donors |
| Saminathan et al. | 2012 | Human PDL cells | Premolars | - | - | - |
| Schröder et al. | 2020 | Human PDL fibroblasts | - | Male + female | 17–27 years | 6 donors |
| Tantilertanant et al. | 2019 | Human PDL cells | - | - | - | 3 donors |
| Tsuji et al. | 2004 | Human PDL cells | Premolars | - | “young” | - |
| Wescott et al. | 2007 | Human PDL fibroblasts | Premolars | - | - | - |
| Zheng et al. | 2012 | Human PDL cells | Third molars | - | 12–28 years | - |
| Zheng et al. | 2019 | Human PDL cells | Third molars | - | 12–28 years | >2 donors for each experiment |
| Ziegler et al. | 2010 | Human PDL fibroblasts | Premolars | - | 12–14 years | - |
| Author | Year | Strain Type | Mode | Frequency | Magnitude | Force Duration | Observation Time Points |
|---|---|---|---|---|---|---|---|
| Behm et al. | 2021 | Tension | Static | - | 6% elongation | 6 and 24 h | immediately after force application |
| Bolcato-Bellemin et al. | 2000 | Tension | Static | - | 20 kPa | 12 h | immediately after force application |
| Chen et al. | 2013 | Tension | Cyclic | 0.1 Hz (6 cycles/min), per cycle: 5 s stretching and 5 s relaxation | 3% and 10% elongation | 24 and 48 h | immediately after force application |
| Fujihara et al. | 2010 | Tension | Cyclic | 0.5 Hz (30 cycles/min) | 110% elongation | 0, 24, and 48 h | immediately after force application |
| Grimm et al. | 2020 | Compression | Static | - | 34.9 g/cm2 | 3 h | immediately after force application |
| Hacopian et al. | 2011 | Compression | Static Cyclic | - 30 min or 15 min with 5 min intervals | 36.3 g/cm2 36.3 g/cm2 | 30, 60 and 90 min 90 min | 24 h after force application 24 h after force application |
| Huang et al. | 2008 | Compression | Static | - | 26.5 g/cm2; 150 g (180 rpm) | 15, 30, 60, or 90 min | immediately after force application |
| Jacobs et al. | 2014 | Tension | Static | - | 1%, 5% and 10% elongation | 12 h | immediately after force application |
| Jacobs et al. | 2018 | Tension | Cyclic | - | 3% elongation | 12 h | immediately after force application |
| Kook et al. | 2011 | Tension | Static | - | 1.5% elongation | 1 h | 0–12 h after force application |
| Lisboa et al. | 2009 | Compression | Static | - | 141 g | 30, 60, 90, and 120 min | 24, 48, 72 h after force application |
| Lisboa et al. | 2013 | Compression | Static | - | 141 g | 30 min | 24 h after stimulation |
| Lisboa et al. | 2013 | Compression | Static | - | 141 g | 30 min | 24 h after stimulation |
| Long et al. | 2002 | Tension | Cyclic | 0.005 Hz | 1.8–12.5% elongation | 2, 24, 48 h | immediately after force application |
| Ma et al. | 2015 | Tension | Cyclic | 6 cycles/min, per cycle: 5 s stretch and 5 s relaxation | 10% elongation | 6 and 24 h | immediately after force application |
| Narimiya et al. | 2017 | Tension | Static | - | 15% elongation | 24 h | immediately after force application |
| Nemoto et al. | 2010 | Tension | Cyclic | 60 s/returns and 29 s resting time | stretch ratio: 105% stretch length: 1.6 mm | 1, 2, 3, 5 and 7 days | immediately after force application |
| Nettelhoff et al. | 2016 | Compression | Static | - | 2 cN/mm2 and 4 cN/mm2 | 12 h | immediately after force application |
| Proff et al. | 2014 | Compression | Static | - | 2 g/cm2 | 24 h | immediately after force application |
| Redlich et al. | 2004 | Compression | Static | - | 33.5 g/cm2; 167 g | 10, 20, 30, 60, 90 and 120 min | immediately after force application |
| Saminathan et al. | 2012 | Tension | Cyclic | 5 s every 90 s (0.2 Hz) | 12% elongation | 6, 12 and 24 h | immediately after force application |
| Schröder et al. | 2020 | Tension | Static | - | 16% elongation | 48 h | immediately after force application |
| Tantilertanant et al. | 2019 | Tension | Cyclic | 60 rpm | 10% elongation | 2 and 6 h | 2, 6, 24 and 48 h |
| Tsuji et al. | 2004 | Tension | Cyclic | 10 cycles/min, per cycle: 3 s strain and 3 s relaxation | 20% elongation | 48 h | immediately after force application |
| Wescott et al. | 2007 | Tension | Cyclic | 6 s strain every 90 s | 12% elongation | 6, 12, and 24 h | immediately after force application |
| Zheng et al. | 2012 | Steady laminar shear flow | Static | - | 6, 9 and 12 dyn/cm2 | 2, 4, 8 and 12 h | immediately after force application |
| Zheng et al. | 2019 | Steady laminar shear flow | Static | - | 6 dyn/cm2 | 4 h | immediately after force application |
| Ziegler et al. | 2010 | Tension | Static | - | 2.5% elongation | 0.25, 0.5, 1, 3, and 6 h | immediately after force application |
| Author | Year | Type of Screening | Outcome | ||||
|---|---|---|---|---|---|---|---|
| MMP-1 | MMP-2 | MMP-3 | MMP-8 | Other MMPs | |||
| Behm et al. | 2021 | qPCR and ELISA | = | = | |||
| Bolcato-Bellemin et al. | 2000 | RT-PCR | ↑ (12 h, 20 kPa) | ↑ (12 h, 20 kPa) | |||
| Chen et al. | 2013 | RT-PCR, zymogram | ↑ (24 + 48 h, 10%) | ||||
| Fujihara et al. | 2010 | Oligo-DNA chip analysis | MMP-15: ↑ (48 h, 110%) | ||||
| Grimm et al. | 2020 | RT-PCR | ↑ (3 h, 34.9 g/cm2) | ||||
| Hacopian et al. | 2011 | RT-PCR | ↑ (60 min, 36.3 g/cm2) | ||||
| Huang et al. | 2008 | RT-PCR, ELISA | ↑ (changes over time) | ||||
| Jacobs et al. | 2014 | ELISA | ↑ (12 h, 10%) | ||||
| Jacobs et al. | 2018 | ELISA | ↑ (12 h, 3%) | ||||
| Kook et al. | 2011 | RT-PCR | ↑ (1 h, 1.5%) | ||||
| Lisboa et al. | 2009 | Zymogram | ↓ (30–120 min, 141 g) | ||||
| Lisboa et al. | 2013 | ELISA, Western blot analysis | = | = | MMP-10: = | ||
| Lisboa et al. | 2013 | Zymogram | = | ||||
| Long et al. | 2002 | RT-PCR, Western blot analysis | = | = | |||
| Ma et al. | 2015 | RT-PCR array | ↓ (6 h, 10%) | ||||
| Narimiya et al. | 2017 | RT-PCR, ELISA | MMP-12: ↑ (24 h, 15%) | ||||
| Nemoto et al. | 2010 | RT-PCR | ↑ (1–7 d, 105%) | ↓ (1–7 d, 105%) | |||
| Nettelhoff et al. | 2016 | ELISA | ↑ (12 h, 5 + 10%) | ||||
| Proff et al. | 2014 | RT-PCR | MMP-13: ↑ (24 h, 2 g/cm2) | ||||
| Redlich et al. | 2004 | RT-PCR | ↑ (30 min, 33.5 g/cm2) | ||||
| Saminathan et al. | 2012 | RT-PCR | ↓ (24 h, 12%) | MMP-11: ↓ (12 h, 12%) MMP-15: ↓ (6 h, 12%) | |||
| Schröder et al. | 2020 | RT-PCR | = | ||||
| Tantilertanant et al. | 2019 | RT-PCR, ELISA | ↑ (6 h, 10%) | ↑ (6 h, 10%) | ↑ (6 h, 10%) | = | MMP-14: ↑ (6 h, 10%) |
| Tsuji et al. | 2004 | RT-PCR | = | = | |||
| Wescott et al. | 2007 | RT-PCR | = | = | MMP-9/10: = | ||
| Zheng et al. | 2012 | RT-PCR, Western blot analysis | ↑ (4 h, 6–12 dyn/cm2) | ↑ (8 h: 12 dyn/cm2) (12 h: 6 + 12 dyn/cm2) | |||
| Zheng et al. | 2019 | RT-PCR, Western Blot analysis | ↓ (4 h, 6 dyn/cm2) | ||||
| Ziegler et al. | 2010 | RT- PCR, Western blot analysis | MMP-10: ↓ (0.5 h, 2.5%) MMP-12: ↑ (0.5 h, 2–5%) MMP-13: ↑ (0.25 + 0.5 + 6 h, 2.5%) | ||||
| 8× ↑ 4× = | 4× ↑ 2× ↓ 4× = | 1× ↑ 1× ↓ 2× = | 4× ↑ 2× ↓ 3× = | 6× ↑ 3× ↓ 3× = | |||
| Author | Year | Type of Screening | Outcome | ||
|---|---|---|---|---|---|
| TIMP-1 | TIMP-2 | TIMP-3 | |||
| Behm et al. | 2021 | RT-PCR | = | ||
| Bolcato-Bellemin et al. | 2000 | RT-PCR | ↑ (12 h, 20 kPa) | ↑ (12 h, 20 kPa) | |
| Chen et al. | 2013 | RT-PCR | ↑ (24 h, 10%) | ||
| Fujihara et al. | 2010 | ||||
| Grimm et al. | 2020 | RT-PCR | ↓ (3 h, 34.9 g/cm2) | ||
| Hacopian et al. | 2011 | RT-PCR | = | ||
| Huang et al. | 2008 | ||||
| Jacobs et al. | 2014 | ELISA | ↑ (12 h, 10%) | ||
| Jacobs et al. | 2018 | ELISA | ↑ (12 h, 3%) | ||
| Kook et al. | 2011 | ||||
| Lisboa et al. | 2009 | ||||
| Lisboa et al. | 2013 | ||||
| Lisboa et al. | 2013 | ||||
| Long et al. | 2002 | RT-PCR, Western blot analysis | = | = | |
| Ma et al. | 2015 | RT-PCR array | ↑ (6 + 24 h, 10%) | = | = |
| Narimiya et al. | 2017 | RT-PCR | = | = | = |
| Nemoto et al. | 2010 | ||||
| Nettelhoff et al. | 2016 | ELISA | ↓ (12 h, 5 + 10%) | ||
| Proff et al. | 2014 | ||||
| Redlich et al. | 2004 | RT-PCR | ↑ (10–60 min, 33.5 g/cm2) | ↑ (10–60 min, 33.5 g/cm2) | |
| Saminathan et al. | 2012 | RT-PCR | = | = | = |
| Schröder et al. | 2020 | ||||
| Tantilertanant et al. | 2019 | RT-PCR | = | = | |
| Tsuji et al. | 2004 | RT-PCR | ↑ (48 h, 20%) | ↑ (48 h, 20%) | |
| Wescott et al. | 2007 | ||||
| Zheng et al. | 2012 | RT-PCR | ↑ (6 dyn/cm2: 8 + 12 h (9 dyn/cm2: 8 + 12 h) (12 dyn/cm2: 4 + 8 + 12 h) | ↓ (6 dyn/cm2: 8 + 12 h) (9 dyn/cm2: 12 h) (12 dyn/cm2: 2 + 8+ 12 h) | |
| Zheng et al. | 2019 | ||||
| Ziegler et al. | 2010 | ||||
| 7× ↑ 2× ↓ 6× = | 4× ↑ 1× ↓ 5× = | 3× = | |||
| Author | Year | Gender | Age | Sample Size |
|---|---|---|---|---|
| Alikhani et al. | 2018 | - | 11–45 years | 18 |
| Apajalahti et al. | 2003 | 3 males, 8 females | 10-14 and 37-38 years | 11 |
| Bildt et al. | 2009 | 2 males, 6 females | 10–18 years | 8 |
| Cantarella et al. | 2006 | 3 males, 8 females | 13–15 years | 11 |
| Capelli et al. | 2011 | 3 males, 11 females | 12–28 years | 14 |
| Grant et al. | 2013 | - | 12–20 years | 21 |
| Ingman et al. | 2005 | 2 males, 3 females | 11, 12, 13, 13 and 36 years | 5 |
| Ribagin et al. | 2012 | 6 males, 6 females | 11–15 years | 12 |
| Rody et al. | 2014 | 3 males, 7 females 4 males, 6 females | 13–15 years 21–39 years | 10 adolescents 10 adults |
| Shirozaki et al. | 2020 | - | 11–44 years | 28 |
| Surlin et al. | 2014 | 6 males, 10 females | 13–17 years | 16 |
| Zhang et al. | 2020 | - | 12–18 years | 20 |
| Author | Year | Teeth | Sample | Appliance Type | Force | Duration | Observation Time | Control |
|---|---|---|---|---|---|---|---|---|
| Alikhani et al. | 2018 | canines | GCF | nickel-titanium closing-coil spring; sequential archwires from 0.016-in nickel-titanium to 0.017 × 0.025-in stainless steel | 50 cN | 56 days | before, 1, 7, 14, and 28 days after the canine retraction | sample collection immediately before canine retraction |
| Apajalahti et al. | 2003 | upper incisor, upper canine or lower central incisor | GCF | fixed appliance | - | - | before OTM and every hour for 8 h following application | systemically healthy patients without OTM |
| Bildt et al. | 2009 | mostly upper first premolars | GCF | super-elastic nickel-titanium coil springs | 150 cN | 4 weeks | 4 weeks after starting force application | teeth without appliances |
| Cantarella et al. | 2006 | Left upper canines | GCF | 0.016-in circular cross-sectional dimension, nickel-titanium orthodontic wire, nickel-titanium coil spring | 150 g | - | 1, 2, 3, 4, 8 h | antagonistic tooth with no appliance |
| Capelli et al. | 2011 | upper canines | GCF | - | 150 g | - | 7 days before OTM, day of OTM, 1 h, 24 h, 2 weeks, 3 weeks and 80 days after application | sample collection 7 days before orthodontic force applied |
| Grant et al. | 2013 | upper canines | GCF | MBT prescription brackets and elastomeric modules, archwire sequence 0.014 nickel-titanium → 0.018 nickel-titanium → 0.018 stainless steel; 9mm nickel-titanium closing coil spring | 100 g | - | 4 h, 7 days and 42 days | sample collection from test teeth before orthodontic force applied; untreated second molars |
| Ingman et al. | 2005 | upper or lower central incisor or upper canine | GCF | fixed appliance treatment (mini-mat brackets, 0.018-inch slot) | - | 1 month | just before appliance and then every 24 h | one upper central incisor from each of three healthy females (mean age 36 years) without OTM |
| Ribagin et al. | 2012 | first molar (central incisor or canines) | GCF | - | - | >3 months | before OTM (up to 1 week), 24 h after placement, 1 week after last visit, 3 months after placement | sample collection before OTM |
| Rody et al. | 2014 | upper arch (upper incisors) | GCF | conventional fixed edgewise bracket system, 0.014-in, 0.018-in, 0.01630.022-in and 0.01930.025-in nickel-titanium | - | 20 weeks | Immediately before bonding and after 3, 6, 18 and 20 weeks | mandibular incisors, free from any orthodontic appliance |
| Shirozaki et al. | 2020 | upper and lower first molars and upper and lower left central incisors | GCF | brackets (0.022″ × 0.028″ slot of stainless steel with stainless steel wires (0.016″, 0.018″, 0.020″, or 0.019″ × 0.025″) and 4 bands in the first molars | - | - | before, 6 and 12 months after bracket bonding | sample collection before treatment |
| Surlin et al. | 2014 | upper canines | GCF | brackets Roth 0.018 inch with 0.012-inch nickel-titanium archwire and a laceback made from 0.010-inch stainless wire | - | until completion of OTM | 1 h before application, 1 h, 4 h, 8 h, 24 h, 72 h, 1 and 2 weeks after force application | contralateral canines (no force applied) |
| Zhang et al. | 2020 | canines | GCF | - | - | - | day of application, 1 h, 24 h, 1 week, 4 weeks and 12 weeks after force application | contralateral teeth of same arch without orthodontic treatment and sample collection before treatment |
| Author | Year | Type of Screening | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|
| MMP-1 | MMP-2 | MMP-3 | MMP-8 | MMP-9 | MMP-13 | MMP-14 | |||
| Alikhani et al. | 2018 | Glass slide-based protein assay | ↑ (after 1 + 7 + 14 days) | ||||||
| Apajalahti et al. | 2003 | Immunofluorometric assay, western blot analysis | not detectable | ↑ (after 4–8 h) | |||||
| Bildt et al. | 2009 | Zymogram, western blot analysis | compression/tension: ↑ (after 4 weeks) | compression/tension: ↑ (after 4 weeks) | not detectable | compression: ↑ (after 4 weeks) | not detectable | ||
| Cantarella et al. | 2006 | Western blot analysis | compression: ↑ (after 1 + 2 + 3 h) tension: ↑ (after 1 + 2 h) | compression: ↑ (after 1 + 2 + 3 + 4 + 8 h) tension: ↑ (after 1 + 2 + 3 + 4 h) | |||||
| Capelli et al. | 2011 | Multiplexed bead immunoassay | compression: changes over time | compression: changes over time | compression: changes over time | ||||
| Grant et al. | 2013 | Luminex multi-analyte technology | compression/tension: ↑ (changes over time) | ||||||
| Ingman et al. | 2005 | Immunofluorometric assay, western blot analysis | not detectable | ↑ | |||||
| Ribagin et al. | 2012 | ELISA | ↓ (1 week) ↑ (after 3 months) | ||||||
| Rody et al. | 2014 | Microarray assay | = | ||||||
| Shirozaki et al. | 2020 | Milliplex TM Map, multiplexing analyser MAGPIX | = | ||||||
| Surlin et al. | 2014 | ELISA | ↑ (after 4 + 8 h and 1 + 2 weeks) | ||||||
| Zhang et al. | 2020 | Multiplex Luminex, Taqman microRNA assays | compression/tension: ↑ (after 24 h + 1 + 4 weeks) | compression/tension: ↑ (after 24 h + 1 + 4 weeks) | compression/tension: ↑ (after 24 h + 1 + 4 weeks) | compression/tension: ↑ (after 24 h + 1 + 4 weeks) | compression/tension: ↑ (after 24 h + 1 + 4 weeks) | compression/tension: ↑ (after 24 h + 1 + 4 weeks) | compression/tension: ↑ (after 24 h + 1 + 4 weeks) |
| 3× ↑ 2× not detectable | 3× ↑ | 1× ↑ | 4× ↑ 1× ↓ 1× = 1× not detectable | 5× ↑ 1× = | 1× ↑ 1× not detectable | 1× ↑ | |||
| Author | Year | Type of Screening | Outcome | |
|---|---|---|---|---|
| TIMP-1 | TIMP-2 | |||
| Alikhani et al. | 2018 | |||
| Apajalahti et al. | 2003 | |||
| Bildt et al. | 2009 | Reverse zymogram | compression/tension: ↑ (after 4 weeks) | not detectable |
| Cantarella et al. | 2006 | |||
| Capelli et al. | 2011 | |||
| Grant et al. | 2013 | Luminex multi-analyte technology | compression/tension: ↑ (changes over time) | compression/tension: ↑ (changes over time) |
| Ingman et al. | 2005 | |||
| Ribagin et al. | 2012 | |||
| Rody et al. | 2014 | |||
| Shirozaki et al. | 2020 | |||
| Surlin et al. | 2014 | |||
| Zhang et al. | 2020 | |||
| 2× ↑ | 1× ↑ 1× not detectable | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behm, C.; Nemec, M.; Weissinger, F.; Rausch, M.A.; Andrukhov, O.; Jonke, E. MMPs and TIMPs Expression Levels in the Periodontal Ligament during Orthodontic Tooth Movement: A Systematic Review of In Vitro and In Vivo Studies. Int. J. Mol. Sci. 2021, 22, 6967. https://doi.org/10.3390/ijms22136967
Behm C, Nemec M, Weissinger F, Rausch MA, Andrukhov O, Jonke E. MMPs and TIMPs Expression Levels in the Periodontal Ligament during Orthodontic Tooth Movement: A Systematic Review of In Vitro and In Vivo Studies. International Journal of Molecular Sciences. 2021; 22(13):6967. https://doi.org/10.3390/ijms22136967
Chicago/Turabian StyleBehm, Christian, Michael Nemec, Fabian Weissinger, Marco Aoqi Rausch, Oleh Andrukhov, and Erwin Jonke. 2021. "MMPs and TIMPs Expression Levels in the Periodontal Ligament during Orthodontic Tooth Movement: A Systematic Review of In Vitro and In Vivo Studies" International Journal of Molecular Sciences 22, no. 13: 6967. https://doi.org/10.3390/ijms22136967
APA StyleBehm, C., Nemec, M., Weissinger, F., Rausch, M. A., Andrukhov, O., & Jonke, E. (2021). MMPs and TIMPs Expression Levels in the Periodontal Ligament during Orthodontic Tooth Movement: A Systematic Review of In Vitro and In Vivo Studies. International Journal of Molecular Sciences, 22(13), 6967. https://doi.org/10.3390/ijms22136967