
Epstein–Barr Virus-Positive Mucocutaneous Ulcer: A Unique and Curious Disease Entity

 , , ,
, , , 
Abstract
:1. Introduction
2. EBV Biology
3. EBV-Associated LPDs
4. What Is EBVMCU?
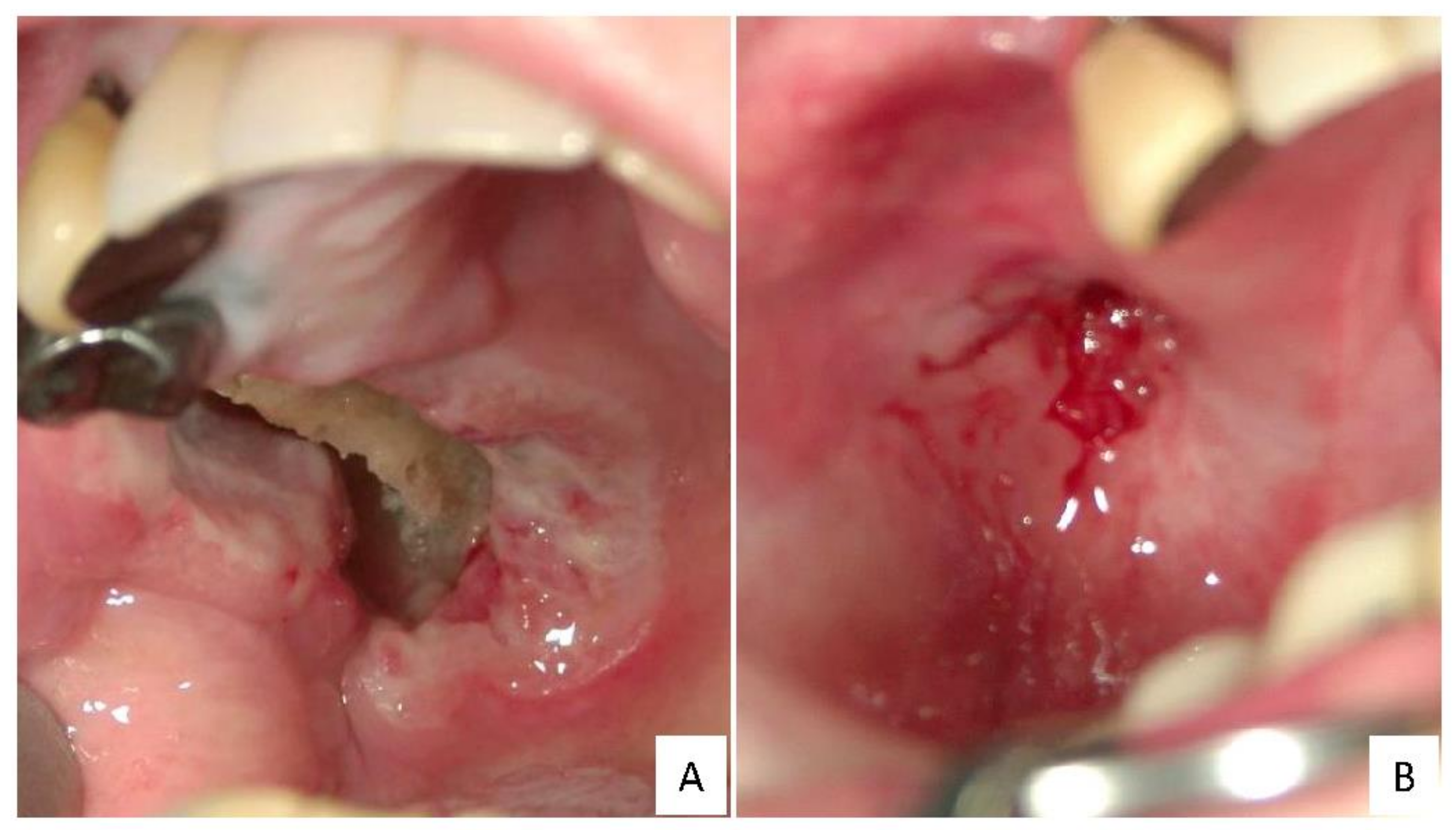
5. Clinical Findings for EBVMCU
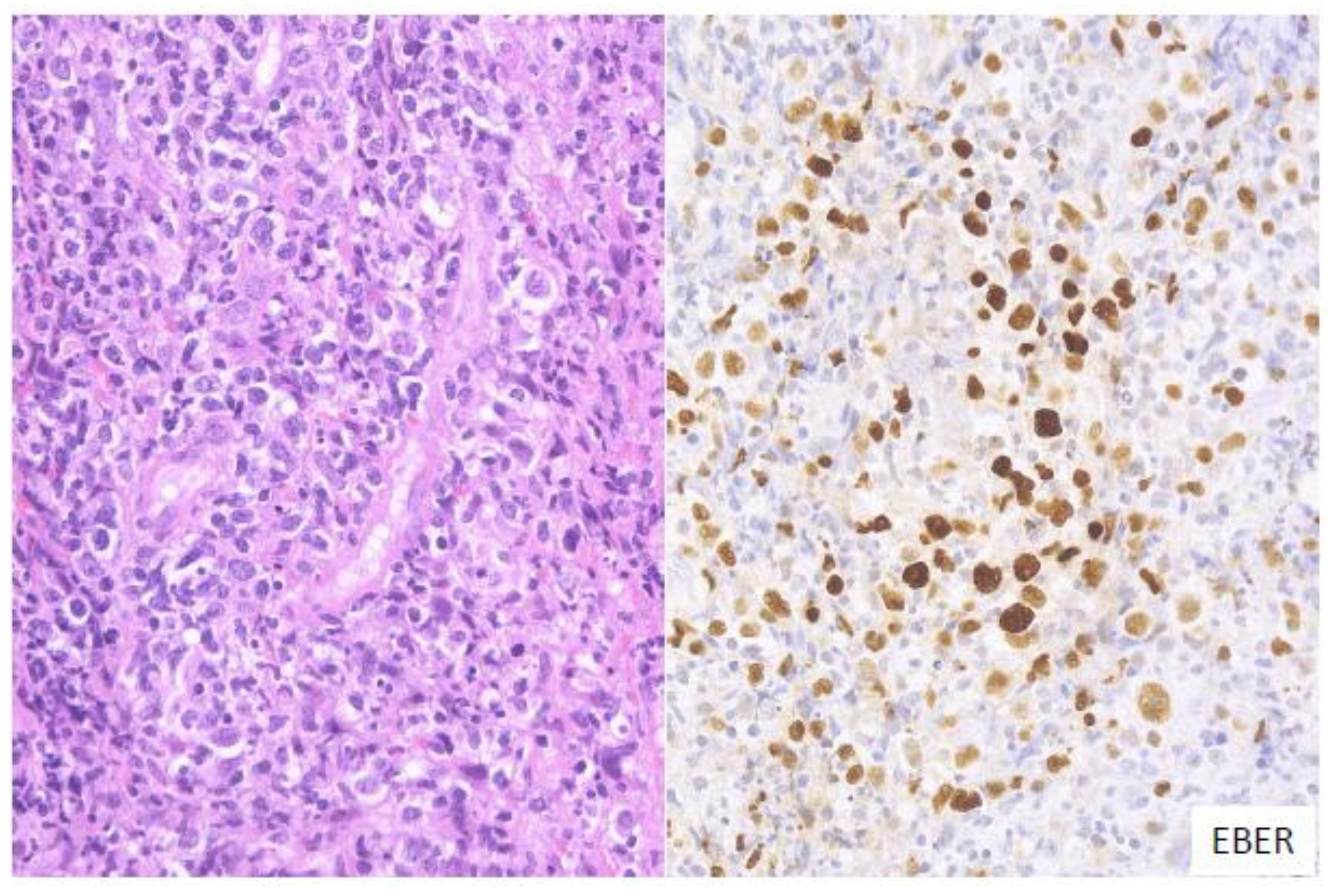
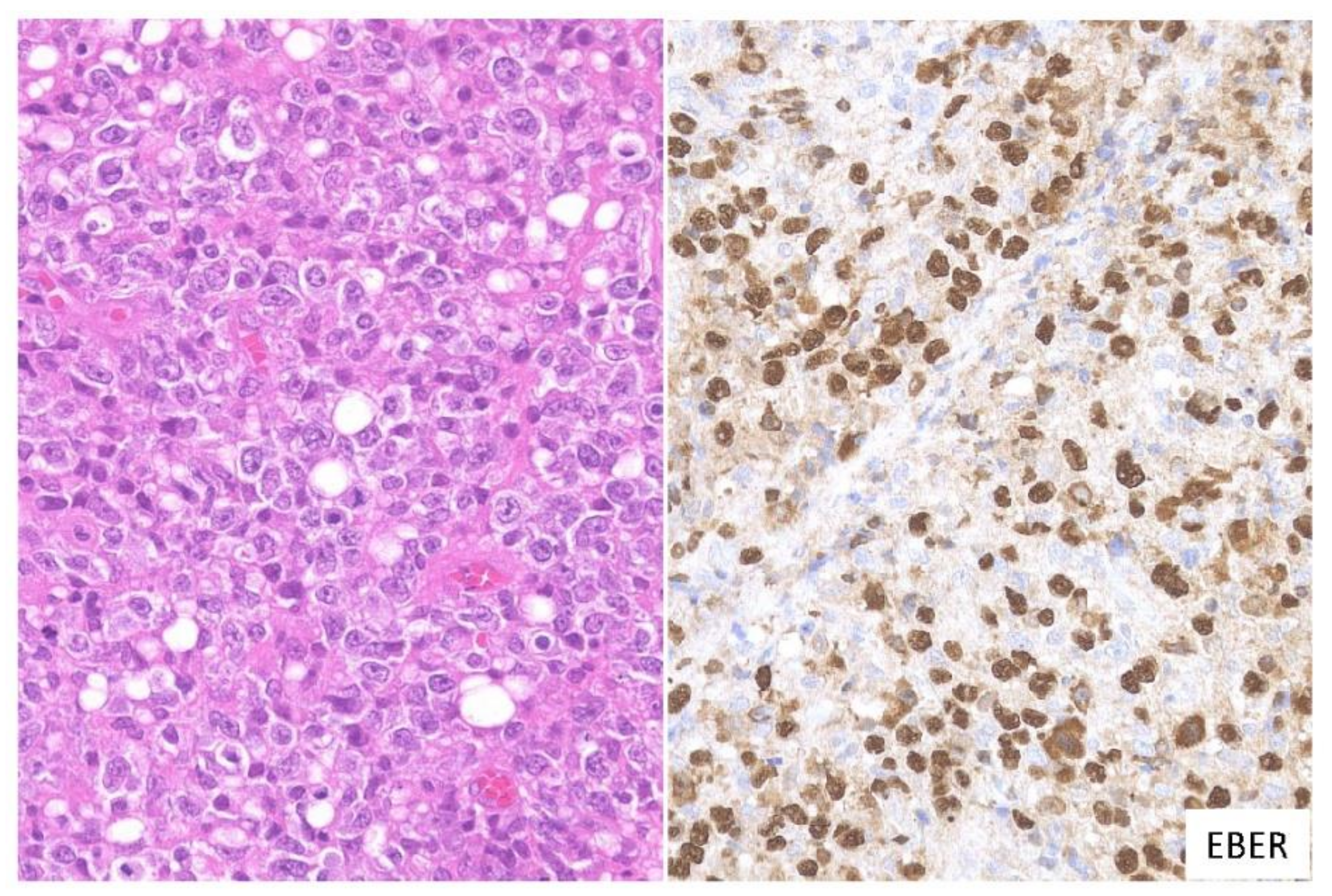
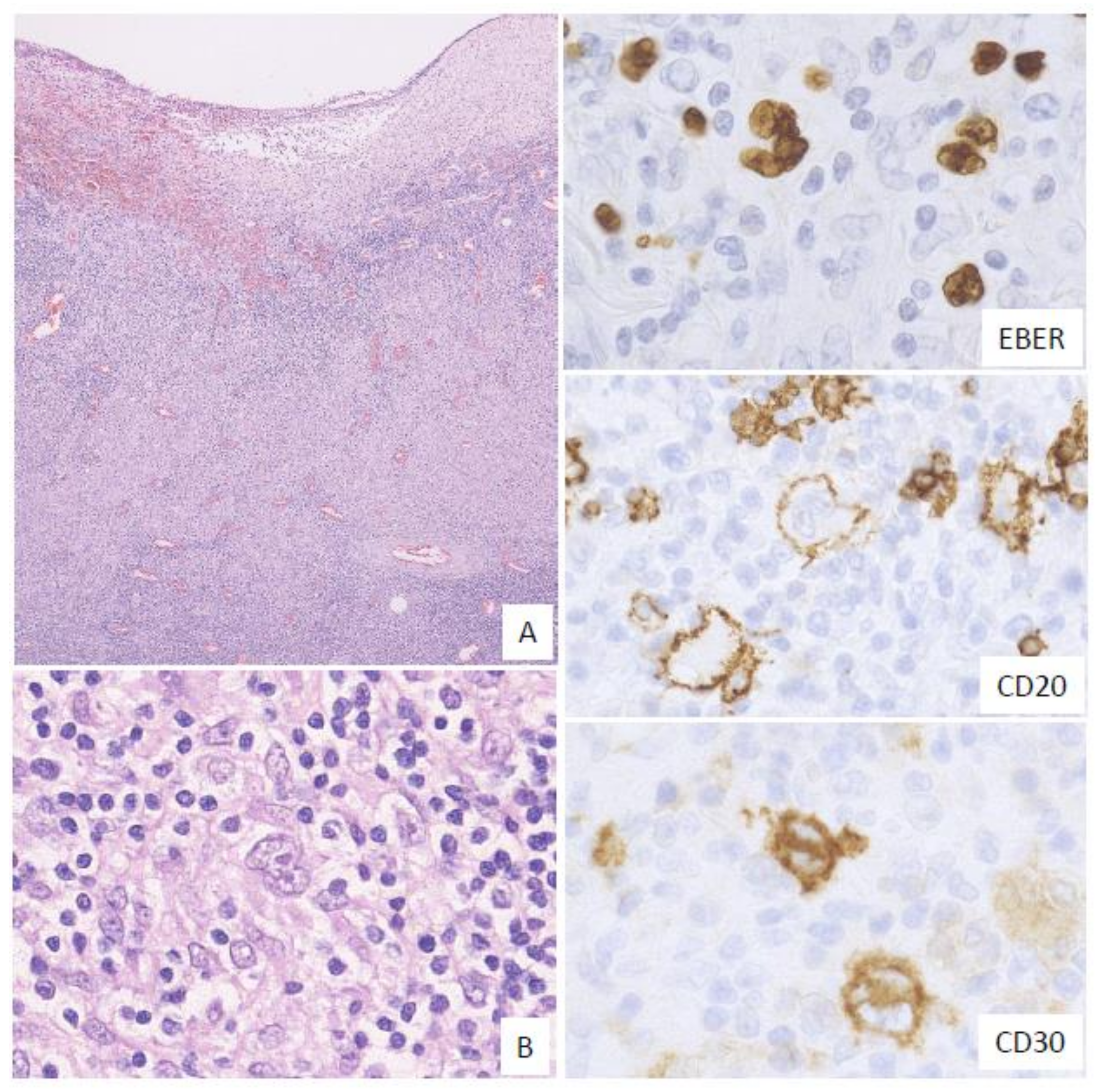
6. Pathological Findings for EBVMCU
6.1. Polymorphous
6.2. Large Cell-Rich
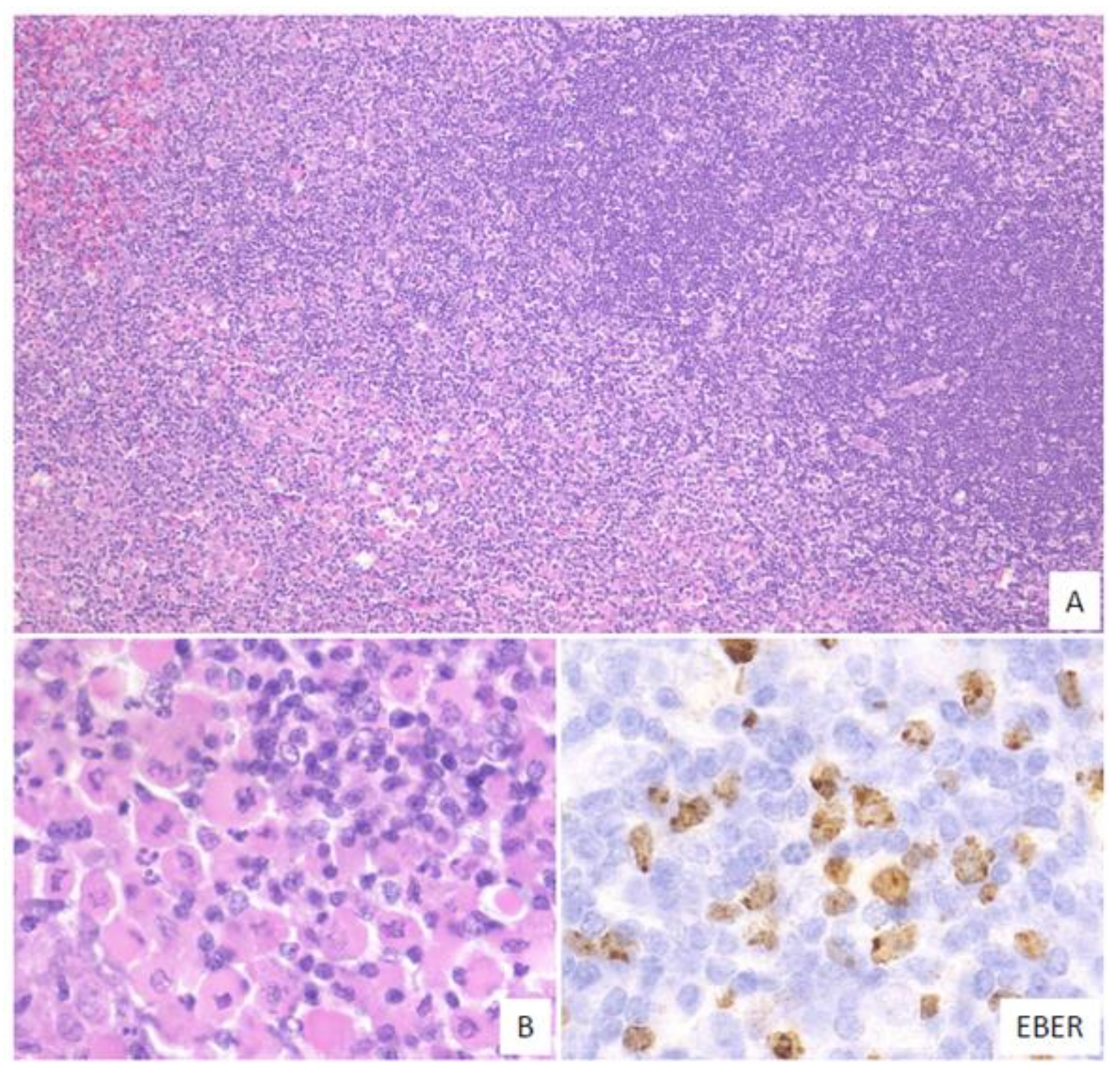
6.3. CHL-Like
6.4. Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma-Like
7. Genetic Findings for EBVMCU
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ikeda, T.; Gion, Y.; Yoshino, T.; Sato, Y. A review of EBV-positive mucocutaneous ulcers focusing on clinical and pathological aspects. J. Clin. Exp. Hematop. 2019, 59, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Liebowitz, D. Epstein–Barr Virus and a Cellular Signaling Pathway in Lymphomas from Immunosuppressed Patients. N. Engl. J. Med. 1998, 338, 1413–1421. [Google Scholar] [CrossRef]
- Komano, J.; Maruo, S.; Kurozumi, K.; Oda, T.; Takada, K. Oncogenic Role of Epstein-Barr Virus-Encoded RNAs in Burkitt’s Lymphoma Cell Line Akata. J. Virol. 1999, 73, 9827–9831. [Google Scholar] [CrossRef] [Green Version]
- Komano, J.; Maruo, S.; Takada, K. Epstein-Barr Virus Contributes to the Malignant Phenotype and to Apoptosis Resistance in Burkitt’s Lymphoma Cell Line Akata. J. Virol. 1998, 72, 9150–9156. [Google Scholar] [CrossRef] [Green Version]
- Roberts, T.K.; Chen, X.; Liao, J.J. Diagnostic and therapeutic challenges of EBV-positive mucocutaneous ulcer: A case report and systematic review of the literature. Exp. Hematol. Oncol. 2016, 5, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kutok, J.L.; Wang, F. Spectrum of Epstein-Barr Virus-Associated Diseases. Annu. Rev. Pathol. 2006, 1, 375–404. [Google Scholar] [CrossRef]
- Fernandez, A.F.; Rosales, C.; Lopez-Nieva, P.; Graña, O.; Ballestar, E.; Ropero, S.; Espada, J.; Melo, S.A.; Lujambio, A.; Fraga, M.F.; et al. The dynamic DNA methylomes of double-stranded DNA viruses associated with human cancer. Genome Res. 2009, 19, 438–451. [Google Scholar] [CrossRef] [Green Version]
- Rickinson, A.B. Co-infections, inflammation and oncogenesis: Future directions for EBV research. In Seminars in Cancer Biology; Academic Press: Cambridge, MA, USA, 2014; pp. 99–115. [Google Scholar]
- Odumade, O.A.; Hogquist, K.A.; Balfour, H.H., Jr. Progress and Problems in Understanding and Managing Primary Epstein-Barr Virus Infections. Clin. Microbiol. Rev. 2011, 24, 193–209. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; Ogata, Y. How Does Epstein-Barr Virus Contribute to Chronic Periodontitis? Int. J. Mol. Sci. 2020, 21, 1940. [Google Scholar] [CrossRef] [Green Version]
- Price, A.M.; Luftig, M.A. To Be or Not IIb: A Multi-Step Process for Epstein-Barr Virus Latency Establishment and Consequences for B Cell Tumorigenesis. PLoS Pathog. 2015, 11, e1004656. [Google Scholar] [CrossRef]
- Navari, M.; Etebari, M.; Ibrahimi, M.; Leoncini, L.; Piccaluga, P.P. Pathobiologic Roles of Epstein–Barr Virus-Encoded MicroRNAs in Human Lymphomas. Int. J. Mol. Sci. 2018, 19, 1168. [Google Scholar] [CrossRef] [Green Version]
- Oyama, T.; Yamamoto, K.; Asano, N.; Oshiro, A.; Suzuki, R.; Kagami, Y.; Morishima, Y.; Takeuchi, K.; Izumo, T.; Mori, S.; et al. Age-related EBV-associated B-cell lymphoproliferative disorders constitute a distinct clinicopathologic group: A study of 96 patients. Clin. Cancer Res. 2007, 13, 5124–5132. [Google Scholar] [CrossRef] [Green Version]
- Gion, Y.; Iwaki, N.; Takata, K.; Takeuchi, M.; Nishida, K.; Orita, Y.; Tachibana, T.; Yoshino, T.; Sato, Y. Clinicopathological analysis of methotrexate-associated lymphoproliferative disorders: Comparison of diffuse large B-cell lymphoma and classical Hodgkin lymphoma types. Cancer Sci. 2017, 108, 1271–1280. [Google Scholar] [CrossRef]
- Dojcinov, S.D.; Venkataraman, G.; Raffeld, M.; Pittaluga, S.; Jaffe, E.S. EBV Positive Mucocutaneous Ulcer—A Study of 26 Cases Associated with Various Sources of Immunosuppression. Am. J. Surg. Pathol. 2010, 34, 405–417. [Google Scholar] [CrossRef]
- Natkunam, Y.; Goodlad, J.R.; Chadburn, A.; Jong, D.; Gratzinger, D.; Chan, J.K.C.; Said, J.; Jaffe, E.S. EBV-Positive B-Cell Proliferations of Varied Malignant Potential. Am. J. Clin. Pathol. 2017, 147, 129–152. [Google Scholar] [CrossRef] [Green Version]
- Au, W.Y.; Loong, F.; Wan, T.S.; Tong, A.C. Multi-focal EBV-mucocutaneous ulcer heralding late-onset T-cell immunodeficiency in a women with lupus erythematosus. Int. J. Hematol. 2011, 94, 501–502. [Google Scholar] [CrossRef]
- Kleinman, S.; Jhaveri, D.; Caimi, P.; Cameron, R.; Lemonovich, T.; Meyerson, H.; Hostoffer, R.; Tcheurekdjian, H. A rare presentation of EBV+ mucocutaneous ulcer that led to a diagnosis of hypogammaglobulinemia. J. Allergy Clin. Immunol. Pract. 2014, 2, 810–812. [Google Scholar] [CrossRef]
- Hart, M.; Thakral, B.; Yohe, S.; Balfour, H.H., Jr.; Singh, C.; Spears, M.; McKenna, R.W. EBV-positive Mucocutaneous Ulcer in Organ Transplant Recipients: A Localized Indolent Posttransplant Lymphoproliferative Disorder. Am. J. Surg. Pathol. 2014, 38, 1522–1529. [Google Scholar] [CrossRef]
- Gali, V.; Bleeker, J.S.; Lynch, D. Epstein-Barr Virus Positive Mucocutaneous Ulcer: A Case Report. S. Dak. Med. 2018, 71, 252–255. [Google Scholar]
- Satou, A.; Kohno, A.; Fukuyama, R.; Elsayed, A.A.; Nakamura, S. Epstein-Barr virus-positive mucocutaneous ulcer arising in a post-hematopoietic cell transplant patient followed by polymorphic posttransplant lymphoproliferative disorder and cytomegalovirus colitis. Hum. Pathol. 2017, 59, 147–151. [Google Scholar] [CrossRef]
- Nelson, A.A.; Harrington, A.M.; Kroft, S.; Dahar, M.A.; Hamadani, M.; Dhakal, B. Presentation and management of post-allogeneic transplantation EBV-positive mucocutaneous ulcer. Bone Marrow Transplant. 2016, 51, 300–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunn, B.; Heerden, W.V. EBV-positive mucocutaneous ulcer of the oral cavity associated with HIV/AIDS. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 725–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaulard, P.; Swerdlow, S.H.; Harris, N.L.; Sundstrom, C.; Jaffe, E.S. EBV-positive mucocutaneous ulcer. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed.; Swerdlow, S.H., Campo, E., Harris, N.L., Eds.; International Agency for Research on Cancer: Lyon, France, 2016; pp. 307–308. [Google Scholar]
- Juan, A.; Lobaton, T.; Tapia, G.; Manosa, M.; Cabre, E.; Domenech, E. Epstein-Barr virus-positive mucocutaneous ulcer in Crohn’s disease. A condition to consider in immunosuppressed IBD patients. Dig. Liver Dis. 2017, 49, 934–937. [Google Scholar] [CrossRef]
- Moran, N.R.; Webster, B.; Lee, K.M.; Trotman, J.; Kwan, Y.-L.; Napoli, J.; Leong, R.W. Epstein Barr virus-positive mucocutaneous ulcer of the colon associated Hodgkin lymphoma in Crohn’s disease. World J. Gastroenterol. 2015, 21, 6072–6076. [Google Scholar] [CrossRef]
- Napoli, A.D.; Giubettini, M.; Duranti, E.; Ferrari, A.; Guglielmi, C.; Uccini, S.; Ruco, L. Iatrogenic EBV-positive lymphoproliferative disorder with features of EBV+ mucocutaneous ulcer: Evidence for concomitant TCRγ/IGH rearrangements in the Hodgkin-like neoplastic cells. Virchows Arch. 2011, 458, 631–636. [Google Scholar] [CrossRef]
- Ohata, Y.; Tatsuzawa, A.; Ohyama, Y.; Ichikawa, A.; Mochizuki, Y.; Ishibashi, S.; Itakura, Y.; Sakurai, U.; Sakamoto, K.; Ikeda, T.; et al. A distinctive subgroup of oral EBV+ B-cell neoplasm with polymorphous features is potentially identical to EBV+ mucocutaneous ulcer. Hum. Pathol. 2017, 69, 129–139. [Google Scholar] [CrossRef]
- Yamakawa, N.; Fujimoto, M.; Kawabata, D.; Terao, C.; Nishikori, M.; Nakashima, R.; Imura, Y.; Yukawa, N.; Yoshifuji, H.; Ohmura, K.; et al. A clinical, pathological, and genetic characterization of methotrexate associate lymphoproliferative disorders. J. Rheum. 2014, 41, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Hashizume, H.; Uchiyama, I.; Kawamura, T.; Suda, T.; Takigawa, M.; Tokura, Y. Epstein–Barr virus-positive mucocutaneous ulcers as a manifestation of methotrexate-associated B-cell lymphoproliferative disorders. Acta Derm. Venereol. 2012, 92, 27607. [Google Scholar] [CrossRef]
- Sadasivam, N.; Johnson, R.J.; Owen, R.G. Resolution of methotrexate-induced Epstein–Barr virus-associated mucocutaneous ulcer. Br. J. Haemotol. 2014, 165, 584. [Google Scholar] [CrossRef] [Green Version]
- Attard, A.A.; Praveen, P.; Dunn, P.J.S.; James, G.J. Epstein–Barr virus-positive mucocutaneous ulcer of the oral cavity: The importance of having a detailed clinical history to reach a correct diagnosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, e37–e39. [Google Scholar] [CrossRef]
- Matnani, R.; Peker, D. Azathioprine induced Epstein–Barr virus-positive mucocutaneous ulcer arising in perianal fistula and abscess associated with Crohn’s disease. J. Crohns Colitis 2014, 8, 1747–1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGinness, J.L.; Spicknall, K.E.; Mutasim, D.F. Azathioprine-induced EBV-positive mucocutaneous ulcer. J. Cutan. Pathol. 2012, 39, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, M.; John, D.; Lim, A.; Jaffe, E.S.; Aoki, J. Clonal Epstein–Barr viruspositive mucocutaneous ulcer mimicking a mature B-cell lymphoma in a patient with mycophenolate-induced immunosuppression. Leuk. Lymphoma. 2015, 56, 1908–1910. [Google Scholar] [CrossRef] [PubMed]
- Sadiku, S.; Kurshumliu, F.; Krasniqi, X.; Brovina, A.; Kryeziu, E.; Rrudhani, I.; Meqa, K.; Gashi-Luci, L.; Merz, H. Age-related Epstein–Barr virus-positive cutaneous ulcer arising after a self-limited subcutaneous abscess: A case report. J. Med. Case. Rep. 2012, 6, 288–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magalhaes, M.; Ghorab, Z.; Morneault, J.; Akinfolarin, J.; Bradley, G. Age-related Epstein-Barr virus-positive mucocutaneous ulcer: A case report. Clin. Case. Rep. 2015, 3, 531–534. [Google Scholar] [CrossRef]
- Soni, S.; Mercer, R.; Pattani, K.; Magill, J. Epstein–Barr virus positive mucocutaneous ulcer: A rare lesion presenting as a large lower lip mass. In Poster Presentation from the University of Central Florida College of Medicine; University of Central Florida: Orlando, FL, USA, 2014. [Google Scholar]
- Hujoel, I.A.; Rubio-Tapia, A.; Dao, L.N.; Porrata, L.F.; Kane, S.V. Epstein-Barr virus-positive mucocutaneous ulcer in an immunosuppressed patient. ACG Case Rep. J. 2018, 5, 5–7. [Google Scholar] [CrossRef]
- McCormack, C.; Huang, Q. EBV+ mucocutaneous ulcer: A new entity of WHO 2017. Blood 2018, 131, 1993. [Google Scholar] [CrossRef] [Green Version]
- Ravi, P.Y.; Sigamani, E.; Jeelani, Y.; Manipadam, M.T. Methotrexate-associated Epstein–Barr virus mucocutaneous ulcer: A case report and review of literature. Indian J. Pathol. Microbiol. 2018, 61, 255–257. [Google Scholar]
- Daroontum, T.; Kohno, K.; Eladl, A.E.; Satou, A.; Sakakibara, A.; Matsukage, S.; Yakushiji, N.; Ya-In, C.; Nakamura, S.; Asano, N.; et al. Comparison of Epstein-Barr virus-positive mucocutaneous ulcer associated with treated lymphoma or methotrexate in Japan. Histopathology 2018, 72, 1115–1127. [Google Scholar] [CrossRef]
- Osman, M.; Salihi, M.A.; Sitta, E.A.; Hadidi, S.A. A rare case of Epstein-Barr virus mucocutaneous ulcer of the colon. BMJ Case Rep. 2017, 2017, bcr-2017. [Google Scholar] [CrossRef]
- Maffione, A.M.; Rampin, L.; Paolini, R.; Rodella, E.; Lisato, L.C.; Ballotta, M.R.; Pavanato, G.; Montesi, G.; Colletti, P.; Rubello, D. Epstein-Barr Virus-Positive Mucocutaneous Ulcer Mimicking Rectal Carcinoma at 18F-FDG PET/CT. Clin. Nucl. Med. 2017, 42, 645–646. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, T.; Paraneetharan; Brennan, P.A.; Ilankovan, V. Epstein-Barr-virus-related mucocutaneous ulceration that mimics oral squamous cell carcinoma: The importance of recognising this new condition. Br. J. Oral Maxillofac Surg. 2017, 55, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.J.; Fang, C.-L.; Chuang, S.S. Epstein-Barr virus-positive mucocutaneous ulcer. Kaohsiung J. Med. Sci. 2017, 33, 50–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vatsayan, A.; Gupta, A.; Ahuja, S.; Eglar, R.; Beck, R.C.; Matloub, Y. Epstein-Barr Virus-associated Mucocutaneous Ulcer in a Patient With T-Cell Acute Lymphoblastic leukemia: Importance of Accurate Diagnosis and Conservative Management. J. Pediatr. Hematol. Oncol. 2017, 39, e338–e341. [Google Scholar] [CrossRef]
- Au, J.K.; Said, J.W.; Sepahdari, A.R.; John, M.A.S. Head and Neck Epstein-Barr Virus Mucocutaneous Ulcer: Case Report and Literature Review. Laryngoscope 2016, 126, 2500–2504. [Google Scholar] [CrossRef]
- Nakauyaca, A.; Kalro, A.; Donaldson, E.; Patel, H. Fatal outcome of an Epstein-Barr virus positive mucocutaneous ulcer secondary to methotrexate. Intern. Med. J. 2016, 46, 1226–1228. [Google Scholar] [CrossRef]
- Sinit, R.B.; Horan, K.L.; Dorer, R.K.; Aboulafia, D.M. Epstein-Barr Virus-Positive Mucocutaneous Ulcer: Case Report and Review of the First 100 Published Cases. Clin. Lymphoma Myeloma Leuk. 2018, 19, e81–e92. [Google Scholar] [CrossRef]
- Pina-Oviedo, S.; Miranda, R.N.; Medeiros, L.J. Cancer therapy-associated lymphoproliferative disorders: An under-recognized type of immunodeficiency-associated lymphoproliferative disorder. Am. J. Surg. Pathol. 2018, 42, 116–129. [Google Scholar] [CrossRef]
- Mendes, L.S.T.; McCaul, J.; Wotherspoon, A.; Attygalle, A.D. Epstein-Barr virus-positive mucocutaneous ulcer with a background of Crohn’s disease and Waldenström macroglobulinaemia: A case report highlighting diagnostic pitfalls. Histopathology 2018, 72, 874–877. [Google Scholar] [CrossRef]
- Ikeda, T.; Gion, Y.; Sakamoto, M.; Tachibana, T.; Nishikori, A.; Nishimura, M.F.; Yoshino, T.; Sato, Y. Clinicopathological analysis of 34 Japanese patients with EBV-positive mucocutaneous ulcer. Mod. Pathol. 2020, 33, 2437–2448. [Google Scholar] [CrossRef]
- Gabsi, A.; Zenzri, Y.; Sahraoui, G.; Brahim, I.B.; Cherif, M.; Yahyaoui, Y.; Charaiet, N.; Mrad, K.; Chedly, C.; Maamer, A.B.; et al. Gastric EBV-positive mucocutaneous ulcer: A rare pathological entity. Clin. Case Rep. 2020, 8, 1130–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritter, C.G.; Cruz, C.D.; Zamboni, S.; Busato, V.B.; Silveira, R.G.; Provenzi, V.O.; Bredemeier, M. EBV-positive mucocutaneous ulcer in a patient with systemic lupus erythematosus. Rheumatology 2020, 59, 916. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.J.; Chiang, W.F.; Chen, T.S.; Kao, H.J.; Chuang, S.S. EBV positive mucocutaneous ulcer with plasmacytic/plasmablastic differentiation and MYC rearrangement: A diagnostic challenge and a mimic of plasmablastic lymphoma. Pathology 2019, 51, 648–650. [Google Scholar] [CrossRef] [PubMed]
- Coelho, K.M.P.A.; Bublitz, G.S.; Franca, P.H.C.; Stall, J.; Hanauer, A.D.; Sangueza, J.M. Epstein-Barr Virus-Positive Mucocutaneous Ulcer in a Pediatric Patient-Case Report. Am. J. Dermatopathol. 2020, 42, e49–e52. [Google Scholar] [CrossRef] [PubMed]
- Hamanaka, S.; Nakagawa, T.; Ota, S.; Iida, M.; Ohta, Y.; Isshiki, Y.; Kasamatsu, S.; Ishigami, H.; Taida, T.; Okimoto, K.; et al. Immunomodulator-associated Epstein-Barr virus-positive mucocutaneous ulcer in a patient with refractory Crohn’s disease. Clin. J. Gastroenterol. 2019, 12, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Karube, K.; Takatori, M.; Kohno, K.; Tomoyose, T.; Ohshiro, K.; Nakazato, I. Co-occurrence of EBV-positive classic Hodgkin lymphoma and B-cell lymphomas of different clonal origins: A case report and literature review. Pathol. Int. 2020, 70, 893–898. [Google Scholar] [CrossRef]
- Zanelli, M.; Zizzo, M.; Foroni, M.; Marco, L.D.; Martino, G.; Ascani, S. EBV-positive mucocutaneous ulcer within colonic diverticulitis mimicking diffuse large B cell lymphoma. Ann. Hematol. 2019, 98, 1795–1797. [Google Scholar] [CrossRef]
- Moriya, K.; Kikuti, Y.Y.; Carreras, J.; Kondo, Y.; Shiraiwa, S.; Nakamura, N. Methotrexate-associated lymphoproliferative disorder demonstrating composite lymphoma of EBV-negative diffuse large B-cell lymphoma and EBV-positive mucocutaneous ulcer. J. Clin. Exp. Hematop. 2020, 60, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Lacet, D.F.R.; Oliveira, C.C. Challenging diagnoses in oral ulcers with large atypical CD30+ cells: EBV-positive mucocutaneous ulcer differentials. J. Clin. Exp. Hematop. 2020, 60, 21–23. [Google Scholar] [CrossRef] [Green Version]
- Miyagi, S.; Ishikawa, E.; Nakamura, M.; Shimada, K.; Yamamura, T.; Furukawa, K.; Tanaka, T.; Mabuchi, S.; Tsuyuki, Y.; Kohno, K.; et al. Reappraisal of Primary Epstein-Barr Virus [EBV]-positive Diffuse Large B-Cell Lymphoma of the Gastrointestinal Tract: Immunosuppressed and nonimmunosuppressed stage I and II-IV patients. Am. J. Surg. Pathol. 2020, 44, 1173–1183. [Google Scholar] [CrossRef]
- Satou, A.; Banno, S.; Hanamura, I.; Takahashi, E.; Takahara, T.; Nobata, H.; Katsuno, T.; Takami, A.; Ito, Y.; Ueda, R.; et al. EBV-positive mucocutaneous ulcer arising in rheumatoid arthritis patients treated with methotrexate: Single center series of nine cases. Pathol. Int. 2019, 69, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daroontum, T.; Kohno, K.; Inaguma, Y.; Okamoto, A.; Okamoto, M.; Kimura, Y.; Nagahama, M.; Sakakibara, A.; Satou, A.; Nakamura, S. Epstein-Barr virus [EBV]-positive diffuse large B-cell lymphoma arising in patient with a history of EBV-positive mucocutaneous ulcer and EBV-positive nodal polymorphous B-lymphoproliferative disorder. Pathol. Int. 2019, 69, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsumi, M.; Yoshimura, T.; Tatsumi, N.; Nakaya, Y.; Fuseya, H.; Horiuchi, M.; Yoshida, M.; Hayashi, Y.; Nakao, T.; Inoue, T.; et al. Aggressive Tongue Root Epstein-Barr Virus-Positive Mucocutaneous Ulcer Treated With Rituximab Alone. Clinical Lymphoma. Myeloma Leuk. 2020, 20, e291–e294. [Google Scholar] [CrossRef] [PubMed]
- Goel, D.; Singh, M. EBV positive mucocutaneous ulcer of palate: A mimicker of malignancy. Indian J. Pathol. Microbiol. 2019, 62, 632–634. [Google Scholar] [CrossRef] [PubMed]
- Pugh, M.R.; Leopold, G.D.; Morgan, M.; Christian, A.D.; Hewett, R.; Durai, D.; Wagstaff, J.; Harris, D.; Dojcinov, S.D. Epstein-Barr Virus-Positive Mucocutaneous Ulcers Complicate Colitis Caused by Immune Checkpoint Regulator Therapy and Associate With Colon Perforation. Clin. Gastroenterol. Hepatol. 2020, 18, 1785–1795. [Google Scholar] [CrossRef]
- Morita, N.; Okuse, C.; Suetani, K.; Nakano, H.; Hiraishi, T.; Ishigooka, S.; Mori, S.; Shimamura, T.; Asakura, T.; Koike, J.; et al. A rare case of Epstein-Barr virus-positive mucocutaneous ulcer that developed into an intestinal obstruction: A case report. BMC Gastroenterol. 2020, 20, 9. [Google Scholar] [CrossRef]
- Yamada, T.; Kitamura, N.; Sasabe, E.; Yamamoto, T. Plasmablastic lymphoma of the upper gingiva in an HIV-negative elderly patient. Oral Maxillofac. Surg. Cases 2015, 1, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Igawa, T.; Sato, Y.; Kawai, H.; Kondo, E.; Takeuchi, M.; Miyata-Takata, T.; Takata, K.; Yoshino, T. Spontaneous regression of plasmablastic lymphoma in an elderly human immunodeficiency virus [HIV]-negative patient. Diagn. Pathol. 2015, 10, 183. [Google Scholar] [CrossRef] [Green Version]
- Yordanova, K.; Stilgenbauer, S.; Bohle, R.M.; Lesan, V.; Thurner, L.; Kaddu-Mulindwa, D.; Bittenbring, J.T.; Scharberger, M.; Aßmann, G.; Bewarder, M. Spontaneous regression of a plasmablastic lymphoma with MYC rearrangement. Br. J. Haematol. 2019, 186, e163–e225. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, J.; Kamamoto, M.; Takagi, Y.; Hanada, H.; Kurokawa, Y.; Fujiwara, S. A case of EBV-positive plasmablastic lymphoma in the mandibular gingiva of an elderly HIV-negative patient. Jpn. J. Oral Maxillofac. Surg. 2019, 65, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Asano, N.; Tatematsu, A.; Oyama, T.; Kitamura, K.; Suzuki, K.; Yamamoto, K.; Sakamoto, N.; Taniwaki, M.; Kinoshita, T.; et al. Plasmablastic lymphoma of the elderly: A clinicopathological comparison with age-related Epstein–Barr virus-associated B cell lymphoproliferative disorder. Histopathology 2012, 61, 1183–1197. [Google Scholar] [PubMed]
- Dojcinov, S.D.; Venkataraman, G.; Pittaluga, S.; Wlodarska, I.; Schrager, J.A.; Raffeld, M.; Hills, R.K.; Jaffe, E.S. Age-related EBV-associated lymphoproliferative disorders in the Western population: A spectrum of reactive lymphoid hyperplasia and lymphoma. Blood 2011, 117, 4726–4735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, S.; Suzuki, K.; Yoshimoto, K.; Kaneko, Y.; Yamaoka, K.; Shimizu, T.; Mori, T.; Okamoto, S.; Kameyama, K.; Amano, K.; et al. Restoration of Decreased T Helper 1 and CD8+ T Cell Subsets Is Associated With Regression of Lymphoproliferative Disorders Developed During Methotrexate Treatment. Front Immunol. 2018, 9, 621. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, H.A.H.; Menasce, L.P.; Pomplun, S.; Burke, M.; Bower, M.; Naresh, K.N. Presence of monoclonal T-cell populations in B-cell post-transplant lymphoproliferative disorders. Mod. Pathol. 2011, 24, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Ghia, P.; Prato, G.; Stella, S.; Scielzo, C.; Geuna, M.; Caligaris-Cappio, F. Age-dependent accumulation of monoclonal CD4+CD8+ double positive T lymphocytes in the peripheral blood of the elderly. Br. J. Haematol. 2007, 139, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, A.; Kohno, K.; Eladl, A.E.; Klaisuwan, T.; Ishikawa, E.; Suzuki, Y.; Shimada, S.; Nakaguro, M.; Shimoyama, Y.; Takahara, T.; et al. Immunohistochemical assessment of the diagnostic utility of PD-L1: A preliminary analysis of anti-PD-L1 antibody [SP142] for lymphoproliferative diseases with tumour and non-malignant Hodgkin-Reed-Sternberg [HRS]-like cells. Histopathology 2018, 72, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, A.; Pittaluga, S.; Abdullah, S.; Steinberg, S.M.; Pham, T.A.; Davies-Hill, T.; Xi, L.; Raffeld, M.; Jaffe, E.S. EBV-positive large B-cell lymphomas in young patients: A nodal lymphoma with evidence for a tolerogenic immune environment. Blood 2015, 126, 863–872. [Google Scholar] [CrossRef] [Green Version]
- Kiyasu, J.; Miyoshi, H.; Hirata, A.; Arakawa, F.; Ichikawa, A.; Niino, D.; Sugita, Y.; Yufu, Y.; Choi, I.; Abe, Y.; et al. Expression of programmed cell death ligand 1 is associated with poor overall survival in patients with diffuse large B-cell lymphoma. Blood 2015, 126, 2193–2201. [Google Scholar] [CrossRef]
- Sakakibara, A.; Kohno, K.; Ishikawa, E.; Suzuki, Y.; Shimada, S.; Eladl, A.E.; Elsayed, A.A.; Daroontum, T.; Satou, A.; Takahara, T.; et al. Age-related EBV-associated B-cell lymphoproliferative disorders and other EBV + lymphoproliferative diseases: New insights into immune escape and immunodeficiency through staining with anti-PD-L1 antibody clone SP142. Pathol. Int. 2020, 70, 481–492. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| B-cell Lymphoproliferative Disorders | ||
| EBV-positive diffuse large B-cell lymphoma, NOS | ||
| EBV-positive mucocutaneous ulcer | ||
| Diffuse large B-cell lymphoma associated with chronic inflammation | ||
| Lymphomatoid granulomatous | ||
| Plasmablastic lymphoma | ||
| Burkitt lymphoma | ||
| Classic Hodgkin lymphoma | ||
| Immunodeficiency-associated lymphoproliferative disorders | ||
| LPD associated with primary immune deficiencies | ||
| Lymphomas associated with HIV | ||
| Post-transplant lymphoproliferative disorders | ||
| Other iatrogenic immunodeficiency-associated lymphoproliferative disorders | ||
| T/NK-cell Lymphoproliferative Disorders | ||
| EBV-positive T-cell and NK cell lymphoproliferative diseases of childhood | ||
| Aggressive NK-cell leukemia | ||
| Extranodal NK/T-cell lymphoma, nasal type | ||
| Primary EBV-positive nodal T- or NK-cell lymphoma | ||
| Chronic active EBV infection | ||
| Epithelial Cell Malignant Tumors | ||
| Carcinoma (nasopharynx, salivary, thymus, lung, stomach, breast, urinary bladder, kidney, uterine cervix, colon) | ||
| Mesenchymal Tumors | ||
| Smooth muscle tumor (leiomyoma/leiomyosarcoma) | ||
| Inflammatory pseudotumor | ||
| Inflammatory pseudotumor-like follicular dendritic cell sarcoma | ||
| Number of Cases (%) | Mean Age (Years) | Age Range (Years) | Sex (Male, %/Female, %) | |
|---|---|---|---|---|
| Iatrogenic Immunodeficiency-Associated EBVMCU (n = 119) | ||||
| Oropharyngeal | 85 (45.7) | 73 | 17–91 | 32 (37.6)/53 (62.4) |
| Skin | 14 (7.5) | 63 | 47–80 | 3 (21.4)/11 (78.6) |
| Gastrointestinal | 20 (10.8) | 67.5 | 26–81 | 14 (70.0)/6 (30.0) |
| EBVMCU due to age-associated immunosenescence (n = 46) | ||||
| Oropharyngeal | 31 (16.7) | 79 | 51–101 | 17 (54.8)/14 (45.2) |
| Skin | 4 (2.2) | 77 | 74–88 | 3 (75.0)/1 (25.0) |
| Gastrointestinal | 11 (5.9) | 72 | 42–84 | 5 (45.5)/6 (54.5) |
| EBVMCU with post-solid organ or bone marrow transplant (n = 12) | ||||
| Oropharyngeal | 6 (3.2) | 57.5 | 18–70 | 4 (66.7)/2 (33.3) |
| Gastrointestinal | 6 (3.2) | 57.5 | 32–70 | 3 (50.0)/3 (50.0) |
| HIV/AIDS-Associated EBVMCU (n = 2) | ||||
| Palate | 2 cases (54-year-old male, 36-year-old female)23 | |||
| Primary Immunodeficiency-Associated EBVMCU (n = 4) | ||||
| Gingiva | 45-year-old female with T-cell deficiency17 | |||
| Esophagus | 61-year-old male with hypogammaglobunemia18 | |||
| Nasopharyngeal | 16-year-old male with CHARGE syndrome16 | |||
| Skin | 5-month-old boy with premature birth57 | |||
| Chronic Antigenic Stimulation-Associated EBVMCU (n = 1) | ||||
| Sinus | 59-year-old female | |||
| EBVMCU of Unclear Etiology (n = 2) | ||||
| Oropharyngeal | 2 cases (49-year-old female, 49-year-old female) [5,16] | |||
| Total | 186 | 71 | 0.4–101 | 84 (45.2)/102 (54.8) |
| SR/CR | PR | SD | PD | RR | NR | |||
|---|---|---|---|---|---|---|---|---|
| Iatrogenic Immunodeficiency-Associated EBVMCU (n = 119) | ||||||||
| RIS (n = 73, 61.3%) | 57 | 10 | - | 2 | - | 4 | ||
| RIS, Rituximab (n = 5, 4.2%) | 4 | - | - | - | 1 | - | ||
| RIS, Chemotherapy (n = 6, 5.0%) | 6 | - | - | - | - | - | ||
| RIS, Resection (n = 2, 1.7%) | 2 | - | - | - | - | - | ||
| Chemotherapy (n = 5, 4.2%) | 3 | - | - | 1 | - | 1 | ||
| Antibody therapy (n = 1, 0.8%) | 0 | - | - | - | - | 1 | ||
| Resection (n = 8, 6.7%) | 1 | - | - | - | - | 7 | ||
| None (n = 8, 6.7%) | 5 | - | - | 1 | 2 | - | ||
| NR (n = 11, 9.2%) | 2 | - | - | - | - | 9 | ||
| EBVMCU due to age-associated immunosenescence (n = 46) | ||||||||
| Rituximab (n = 1, 2.2%) | 1 | - | - | - | - | - | ||
| Chemotherapy (n = 13, 28.3%) | 11 | - | - | - | - | 2 | ||
| RT (n = 4, 8.7%) | 4 | - | - | - | - | - | ||
| Chemotherapy, RT (n = 1, 2.2%) | 1 | - | - | - | - | - | ||
| Chemotherapy, RT, and Resection (n = 1, 2.2%) | 1 | - | - | - | - | - | ||
| Resection (n = 6, 13.0%) | 4 | - | - | - | - | 2 | ||
| None (n = 12, 26.1%) | 8 | - | 1 | - | 3 | - | ||
| NR (n = 8, 17.4%) | - | - | - | - | - | 8 | ||
| EBVMCU with post-solid organ or bone marrow transplant (n = 12) | ||||||||
| RIS (n = 6, 50.0%) | 6 | - | - | - | - | - | ||
| RIS, Rituximab (n = 3, 25.0%) | 3 | - | - | - | - | - | ||
| RIS, Resection (n = 1, 8.3%) | 1 | - | - | - | - | - | ||
| None (n = 1, 8.3%) | 1 | - | - | - | - | - | ||
| NR (n = 1, 8.3%) | - | - | - | - | - | 1 | ||
| HIV/AIDS-Associated EBVMCU (n = 2) | ||||||||
| NR (n = 2, 100%) | - | - | - | - | - | 2 | ||
| Primary Immunodeficiency-Associated EBVMCU (n = 4) | ||||||||
| Rituximab (n = 1, 25.0%) | 1 | - | - | - | - | - | ||
| Rituximab, brentuximab, IVIG (n = 1, 25.0%) | - | - | - | 1 | - | - | ||
| Chemotherapy and HSCT (n = 1, 25.0%) | - | - | - | - | 1 | - | ||
| Resection (n = 1, 25.0%) | 1 | - | - | - | - | - | ||
| Chronic Antigenic Stimulation-Associated EBVMCU (n = 1) | ||||||||
| RT (n = 1, 100.0%) | 1 | - | - | - | - | - | ||
| EBVMCU of Unclear Etiology (n = 2) | ||||||||
| RT (n = 1, 50.0%) | - | - | - | - | 1 | - | ||
| Rituximab, RT (n = 1, 50.0%) | 1 | - | - | - | - | - | ||
| Total | 125 | 10 | 1 | 5 | 8 | 37 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, T.; Gion, Y.; Nishimura, Y.; Nishimura, M.F.; Yoshino, T.; Sato, Y. Epstein–Barr Virus-Positive Mucocutaneous Ulcer: A Unique and Curious Disease Entity. Int. J. Mol. Sci. 2021, 22, 1053. https://doi.org/10.3390/ijms22031053
Ikeda T, Gion Y, Nishimura Y, Nishimura MF, Yoshino T, Sato Y. Epstein–Barr Virus-Positive Mucocutaneous Ulcer: A Unique and Curious Disease Entity. International Journal of Molecular Sciences. 2021; 22(3):1053. https://doi.org/10.3390/ijms22031053
Chicago/Turabian StyleIkeda, Tomoka, Yuka Gion, Yoshito Nishimura, Midori Filiz Nishimura, Tadashi Yoshino, and Yasuharu Sato. 2021. "Epstein–Barr Virus-Positive Mucocutaneous Ulcer: A Unique and Curious Disease Entity" International Journal of Molecular Sciences 22, no. 3: 1053. https://doi.org/10.3390/ijms22031053
APA StyleIkeda, T., Gion, Y., Nishimura, Y., Nishimura, M. F., Yoshino, T., & Sato, Y. (2021). Epstein–Barr Virus-Positive Mucocutaneous Ulcer: A Unique and Curious Disease Entity. International Journal of Molecular Sciences, 22(3), 1053. https://doi.org/10.3390/ijms22031053