1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) caused a pandemic of a coronavirus disease in 2019 (COVID-19) and an urgent need for the development of new treatment approaches [
1]. One of the main pathophysiologic mechanisms defining the disease’s severity is the overactivation of the immune system associated with an excessive release of cytokines and chemokines, also referred to as “cytokine storm syndrome” (CSS) [
2,
3]. This type of pronounced immune system reaction is not unique for SARS-CoV-2 infection but has also been described in other clinical situations, such as cytokine release syndrome (CRS) in patients receiving chimeric antigen receptor (CAR)-T cell or bispecific T cell-engaging antibody therapy [
4,
5], familiar hemophagocytic lymphohistiocytosis (HLH) [
6,
7], secondary HLH due to malignancies, and autoimmune disorders (macrophage activation syndrome, MAS) [
8,
9,
10], as well as systemic inflammatory response syndrome (SIRS) and acute respiratory distress syndrome (ARDS) in other infectious diseases [
11,
12,
13,
14]. In the case of COVID-19, CSS can develop within a few days after the disease’s onset, resulting in a significantly higher rate of patients’ in-hospital complications and mortality [
15,
16,
17].
Despite the negative impact of CSS on the prognosis in patients with COVID-19, the diagnostic criteria of its onset remain unclear. The standard clinical criteria of CSS for noninfectious diseases, such as CRS or HLH, cannot be fully applied to COVID-19 since they also include such parameters as fever and hypoxemia, induced by the viral dissemination even before the beginning of a cytokine storm [
5,
18,
19]. Moreover, many laboratory parameters change in the course of COVID-19, in particular, during the initial phase of the viral infection, thus making them unreliable for the prediction of CSS onset [
20,
21].
Nevertheless, similar to patients with CRS after CAR-T therapy, primary HLH, or non-COVID-19-related ARDS and SIRS [
22,
23,
24,
25,
26], COVID-19 patients with CSS are often treated with anti-cytokine therapies. However, in COVID-19-related cytokine storm, the levels of cytokines were found to be significantly lower than those observed in the other above-mentioned pathologies. Therefore, the specific effects of such treatment in COVID-19 patients remain to be elucidated.
Although clinical trials have revealed that immunomodulatory therapy can be a promising treatment option in COVID-19-associated CSS, the results of these trials are highly controversial [
27,
28,
29,
30,
31,
32,
33,
34,
35]. Discrepancies in trial outcomes can be associated with the different criteria used as indicators for tocilizumab therapy. Indeed, in some trials, HLH parameters, such as fever, leukopenia, increased ferritin, and LDH levels, were used, while others based the therapy solely on increased inflammatory markers, such as high-sensitivity C-reactive protein (hs-CRP) [
21,
36,
37,
38]. However, while these parameters correspond well to the development of multiorgan dysfunction and worse clinical prognosis, they do not always correlate with the patterns of hypercytokinemia that can be treated with targeted immunosuppression. Hence, identifying the key cytokine markers of CSS induced by SARS-CoV-2 infection is of utmost importance to provide more reliable indicators for specific immunomodulatory treatments. The identification of these parameters was the goal of the current study.
Specifically, we evaluated the cytokine/chemokine profile in hospitalized COVID-19 patients. We identified the cytokine clusters in mildly and severely ill patients and revealed critical laboratory parameters linked to CSS in severe COVID-19. Overall, our results provide an insight into the cytokine cascade in COVID-19 patients and suggest that IL-6 receptor blockage may be exploited as a rational strategy to suppress SARS-CoV-2–induced CSS when used according to the adapted laboratory criteria of CSS.
3. Discussion
Approximately 80% of severe and moderate COVID-19 cases are accompanied by the development of CSS due to excessive immune activation [
55,
56,
57,
58,
59]. It is associated with a systemic release of cytokines [
60,
61], causing multiorgan failure resulting in decreased patient survival [
62,
63,
64]. This syndrome has already been described for patients receiving CAR-T therapy and other anticancer treatments [
4,
5,
65] as well as in HLH syndromes [
66,
67], and different bacterial and viral infections [
13,
68,
69] including other coronaviruses [
70]. However, the laboratory signature of CSS in COVID-19 differs significantly from those of the other pathologies [
59]. In particular, the levels of pro-inflammatory cytokines were shown to be significantly lower in COVID-19 patients than in critically ill patients with ARDS or sepsis [
23,
26]. Moreover, the profile of cytokine changes depends on the specific disease, with IFN-γ playing the key role in primary HLH [
71], IL-18 in MAS [
72], and IL-6 in CRS [
73]. Even though it is caused by viral infections, the cytokine storm is characterized by different cytokine signatures in the cases of MERS [
74,
75,
76], SARS [
77,
78], and influenza [
20,
79,
80]. Thus, although it is regarded as a similar pathological state, the treatment of different CSSs has to be individualized according to the degree and difference in the cytokine cascade activation.
Despite the importance of the treatment strategy, there are still no unified criteria to diagnose cytokine storm syndromes. While the standard parameters defining CRS after specific T cell antibody therapy mostly include clinical characteristics of the patients, the criteria for HLH include laboratory markers such as cytopenia, elevated liver enzymes, ferritin, and CRP, as well as changes in coagulation factors [
4,
81]. It was shown that not all of these markers can be used as diagnostic criteria for the development of COVID-19-associated CSS. According to the initial trials, patients with severe and fatal disease showed an increased leukocyte count, decreased lymphocyte and platelet counts, increased biomarkers of inflammation, cardiac and muscle injury, liver and kidney function, and coagulation [
39,
40,
41,
43,
45,
52,
82,
83,
84,
85]. However, in the further larger studies, only a few of these markers were found to be independently associated with increased mortality [
51].
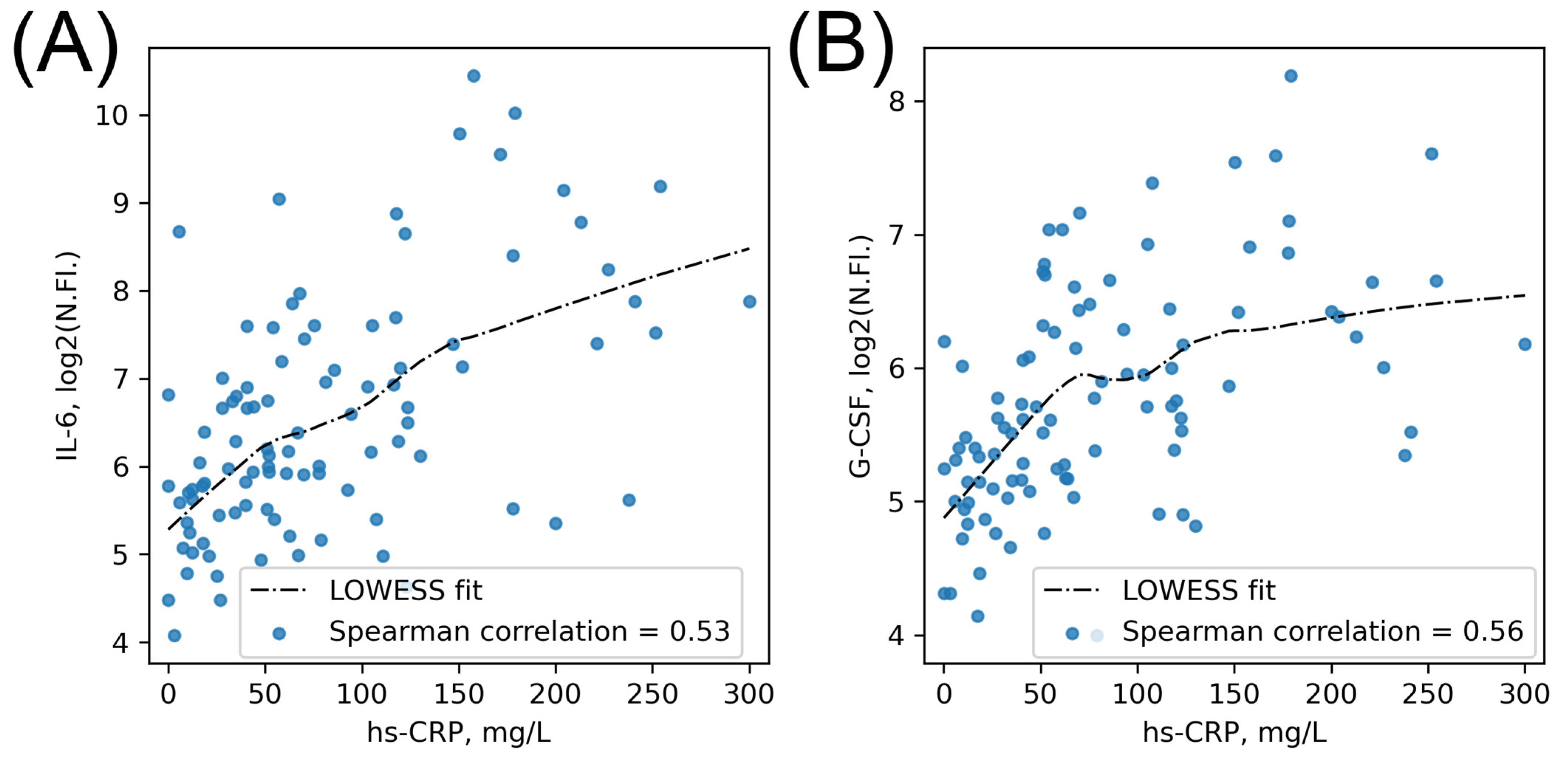
In analyses of the cytokine storm severity in COVID-19, most of the trials used the CRP level as a unified marker of inflammation. It was shown to be a significant prognostic marker for disease severity as well as mortality in COVID-19. Specifically, an hs-CRP level threshold of 91 mg/L was reported to be associated with the severe form of the disease [
86], while, in other studies, lower values of 66 mg/L or even 33 mg/L were found to be significant for patients’ prognosis [
87,
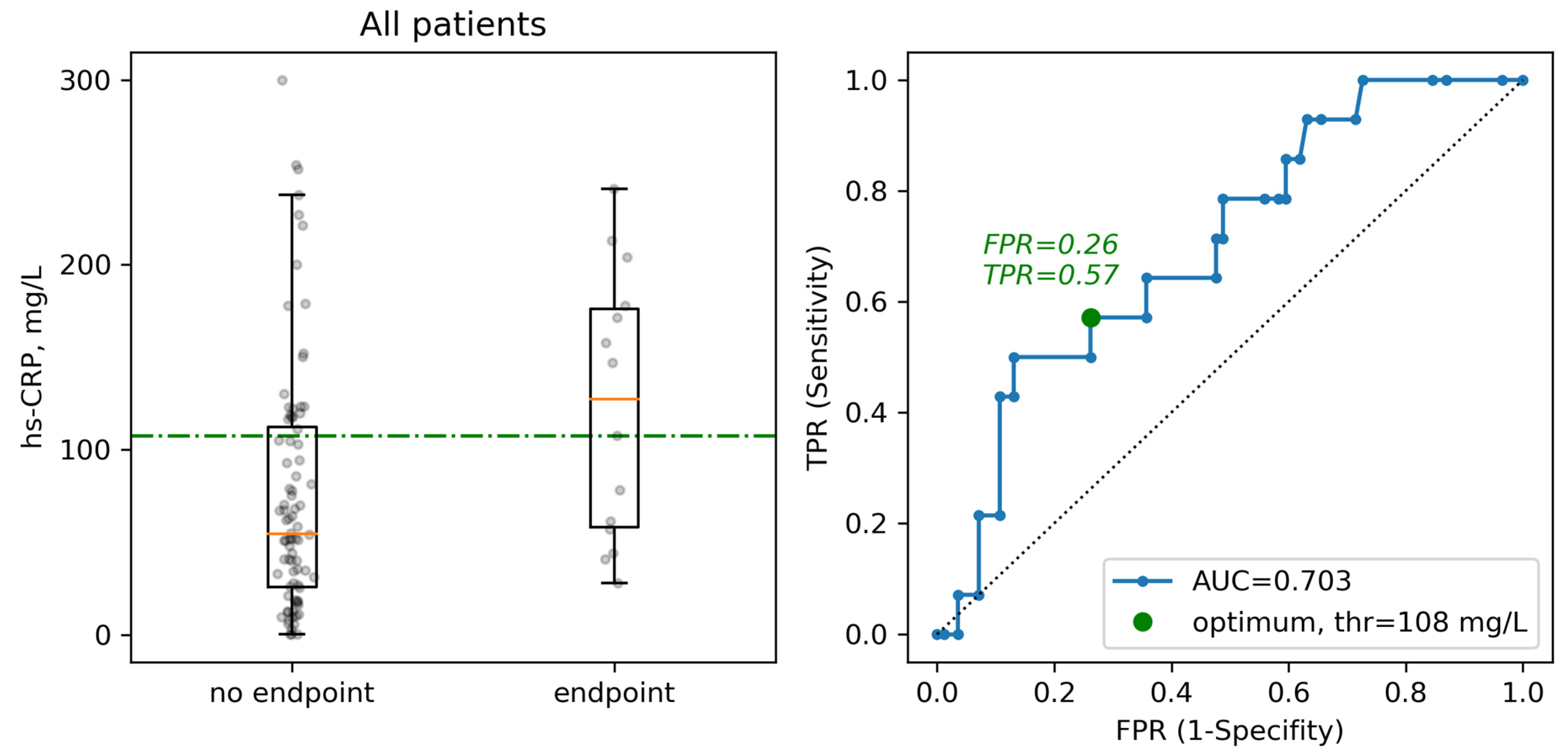
88]. In our trial, we found that a CRP level higher than 108 mg/L was linked to the mortality of the patients, which is in agreement with the threshold of 100 mg/L found in the published meta-analyses [
53]. However, when we assessed the interaction between the multi-cytokine signature of the storm and hs-CRP level, we found only a minor number of significant correlations. Moreover, clinical and laboratory criteria showed no strong correlations with cytokine levels. These data indicate the need for a further search of a better criterion or combination of criteria to define the cytokine storm development in COVID-19.
In research aimed at establishing the cytokine signature of COVID-19, several trials investigated clusters of cytokines to assess the development of the cytokine storm. In these trials, many CSS-related cytokines showed an increase corresponding to the severity of the disease [
89], providing proof of a severe general inflammatory activation in COVID-19 [
17,
90,
91]. Moreover, these cytokine levels correlated with each other, showing the concordance of the inflammatory changes during the CSS [
92]. The previously established cytokine clusters included growth factors, mediators of tissue repair, immune effector modulators, and chemoattractants.
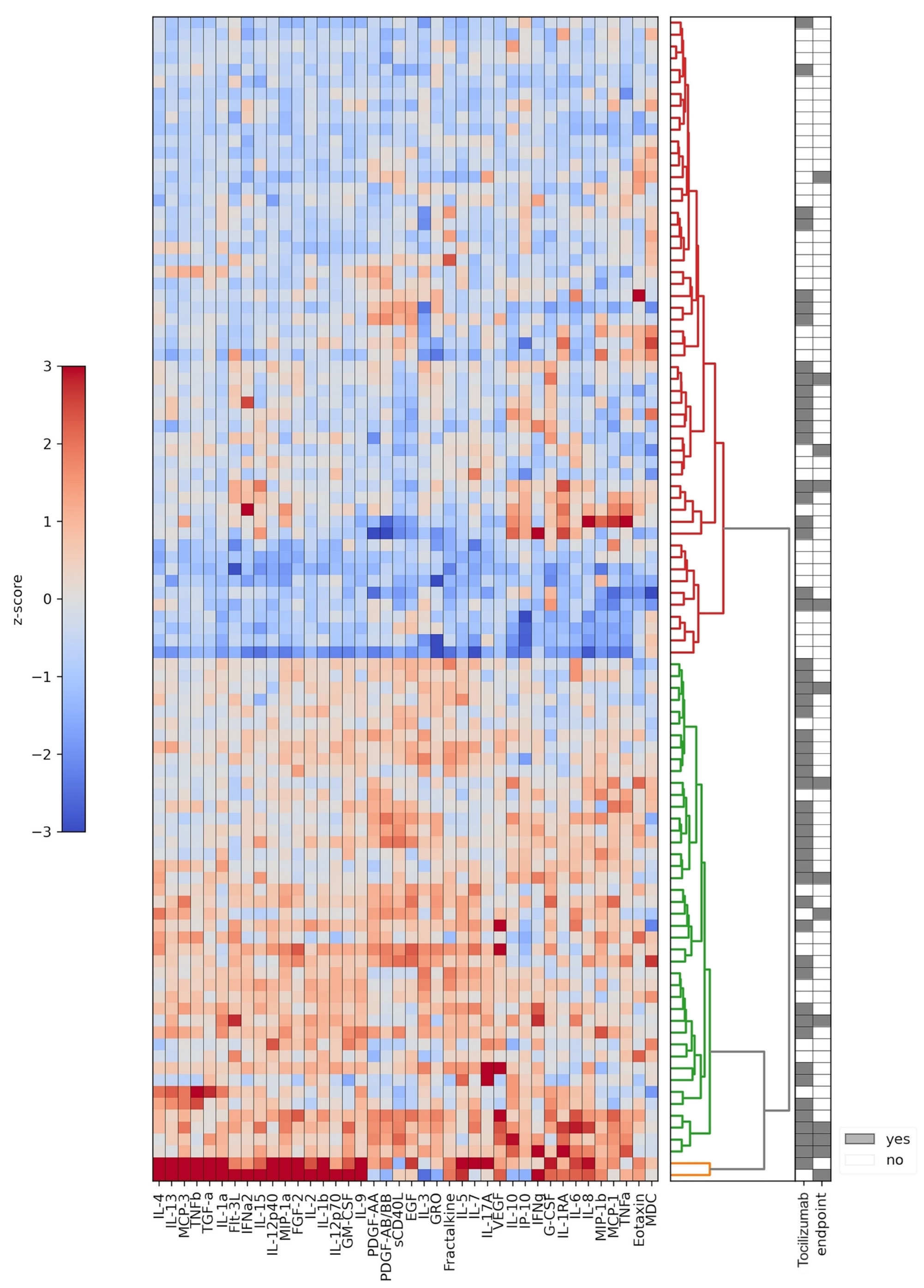
In our study, we assessed the development of the cytokine storm according to the clusters of circulating cytokines in the blood of the patients with proven COVID-19 within the first days after admission to hospital, before the initiation of the antiinflammatory therapy. While performing the randomization, we found that the patients could be separated into two distinct clusters according to their cytokine levels. Moreover, these clusters corresponded to the severity of the disease. We also showed that the clusterization of the cytokines according to the cytokine storm severity corresponded to the changes in many of the standard parameters, including leukocyte and neutrophil counts, levels of total protein, AST, LDH, ferritin, triglycerides, fibrinogen, prothrombin time, and hs-CRP, that were shown in previous trials to be associated with the disease severity or mortality. However, while it was applied without initial randomization, tocilizumab was used in the patients with more severe changes in clinical parameters but less pronounced laboratory changes, thus indicating an underestimation of the cytokine storm development in some patients with a less severe clinical state and the need for more specified laboratory markers to initiate the specific anti-cytokine therapy.
Many of the individual cytokines from the clusters correlated with the disease severity and mortality according to the recent trials, including TNF-α, IL-10, IL-15, IL-12, IL-2, IL-6, IFN-α, IFN-γ, and IL-1RA, as well as many chemokines [
91,
92,
93,
94,
95]. Later studies underlined the significance of the other cytokines, such as IL-1β, sIL-2Rα, IL-17, IL-18, MCP-3, M-CSF, MIP-1α, G-CSF, IP-10, and MCP-1 [
17,
39,
96,
97]. IL-1β, IL-1RA, IL-6, IL-7, IL-10, IP-10, and TNF-α showed the strongest correlation with disease severity in several recent trials [
97]. Despite being lower than in the other cases of cytokine storm, i.e., HLH or CRS, these cytokines still indicate a worse prognosis for COVID-19 patients [
23].
Unfortunately, the data concerning the clinical impact of different cytokines remain highly controversial [
49,
50,
98,
99,
100]. For example, the levels of IL-6 were shown in several studies to be the main contributor to the prognosis in COVID-19 [
101,
102,
103,
104,
105,
106,
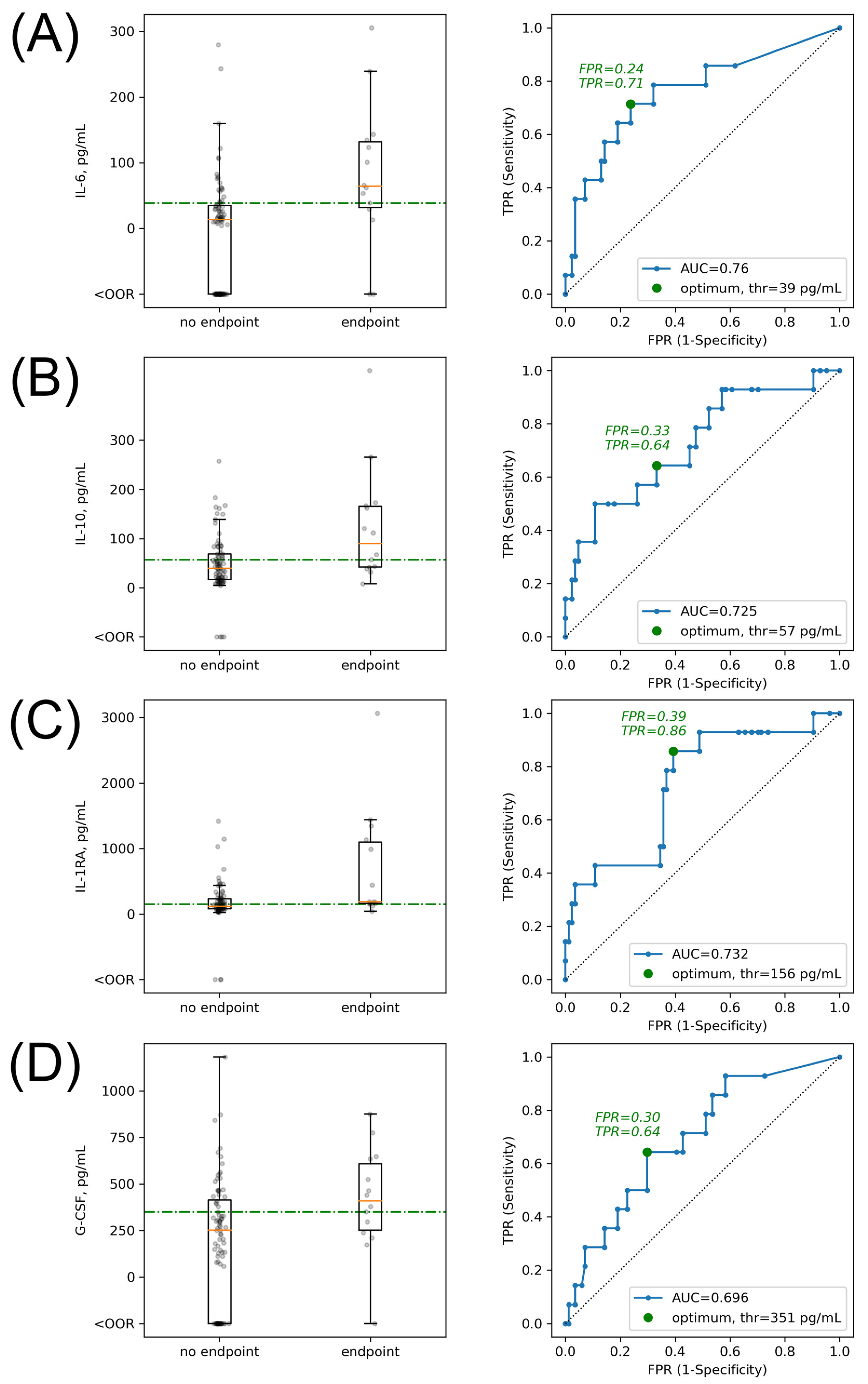
107], but at the same time, the threshold of IL-6 levels differed in these trials significantly, with a range from 30 pg/mL to 163.4 pg/mL [
108]. In our study, we found that a threshold of 39 pg/mL corresponded to the disease severity and mortality of the patients. However, we found no significant correlation of the IL-6 levels with clinical endpoints in the subgroup of patients treated with tocilizumab. We assume that the effect of IL-6 was masked because of the initial higher levels in this group of patients (with a threshold of 62 pg/mL) as well as due to the impact of the tocilizumab treatment, targeted against IL-6 receptors. Therefore, despite the general findings indicating the usefulness in measuring the serum IL-6 level [
46], its clinical implication to guide anti-cytokine treatment is still lacking a prospectively established threshold.
Many hopes were invested in the application of direct anti-cytokine therapy in COVID-19 patients, especially of the IL-6 receptor blocker tocilizumab, which was previously widely used in CRS caused by CAR-T therapy [
109,
110]. Several trials reported a positive effect of tocilizumab therapy on the symptoms and respiratory function, as well as on mortality in COVID-19 patients [
111]. Despite showing heterogeneous results in the following randomized clinical trials [
27], IL-6 inhibitors were included in the current NIH COVID-19 guidelines for the treatment of severe and critical COVID-19.
In the recent meta-analysis, the most pronounced benefit of tocilizumab was shown in patients with hs-CRP levels greater than 100 mg/L, while it had no positive effect in patients with hs-CRP levels lower than 100 mg/L [
53]. In our study, we found no significant impact of hs-CRP levels on the prognosis in patients treated with tocilizumab, while there was a threshold hs-CRP level of 158 mg/L in that subgroup. On the other hand, in patients not receiving tocilizumab, the hs-CRP level threshold of 78 mg/L was statistically significant in defining the prognosis. For the all-patient group this threshold constituted 108 mg/L, corresponding to the commonly used threshold for the application of the anti-cytokine therapy in current clinical trials [
31]. Thus, we assume that an extreme elevation of the hs-CRP level higher than 158 mg/L might reflect the beginning of multiorgan damage, to which the targeted therapy with tocilizumab brings no additional benefit, while approximate values between 78–158 mg/L can be used as an indication for the initiation of the immunomodulatory therapy.
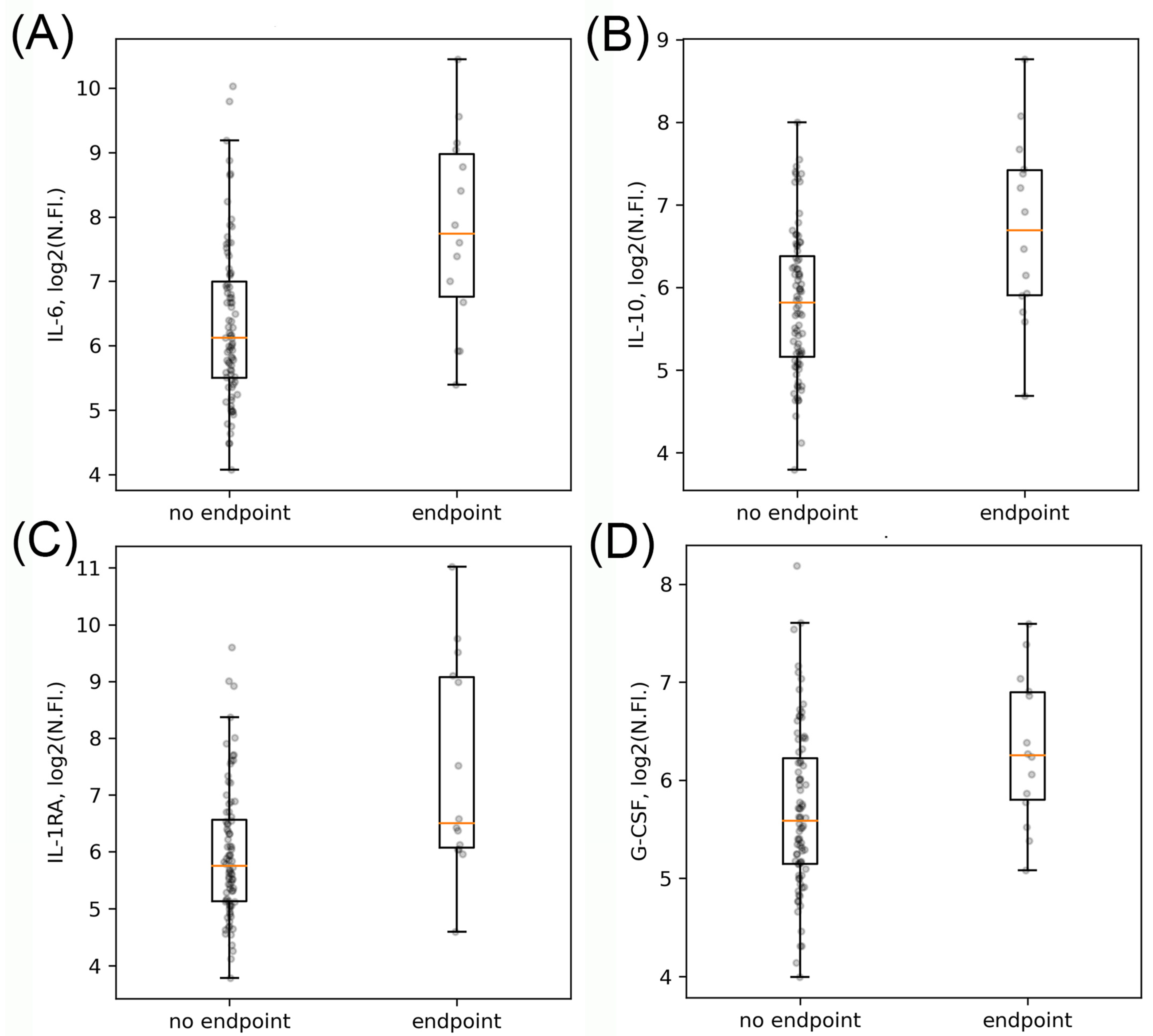
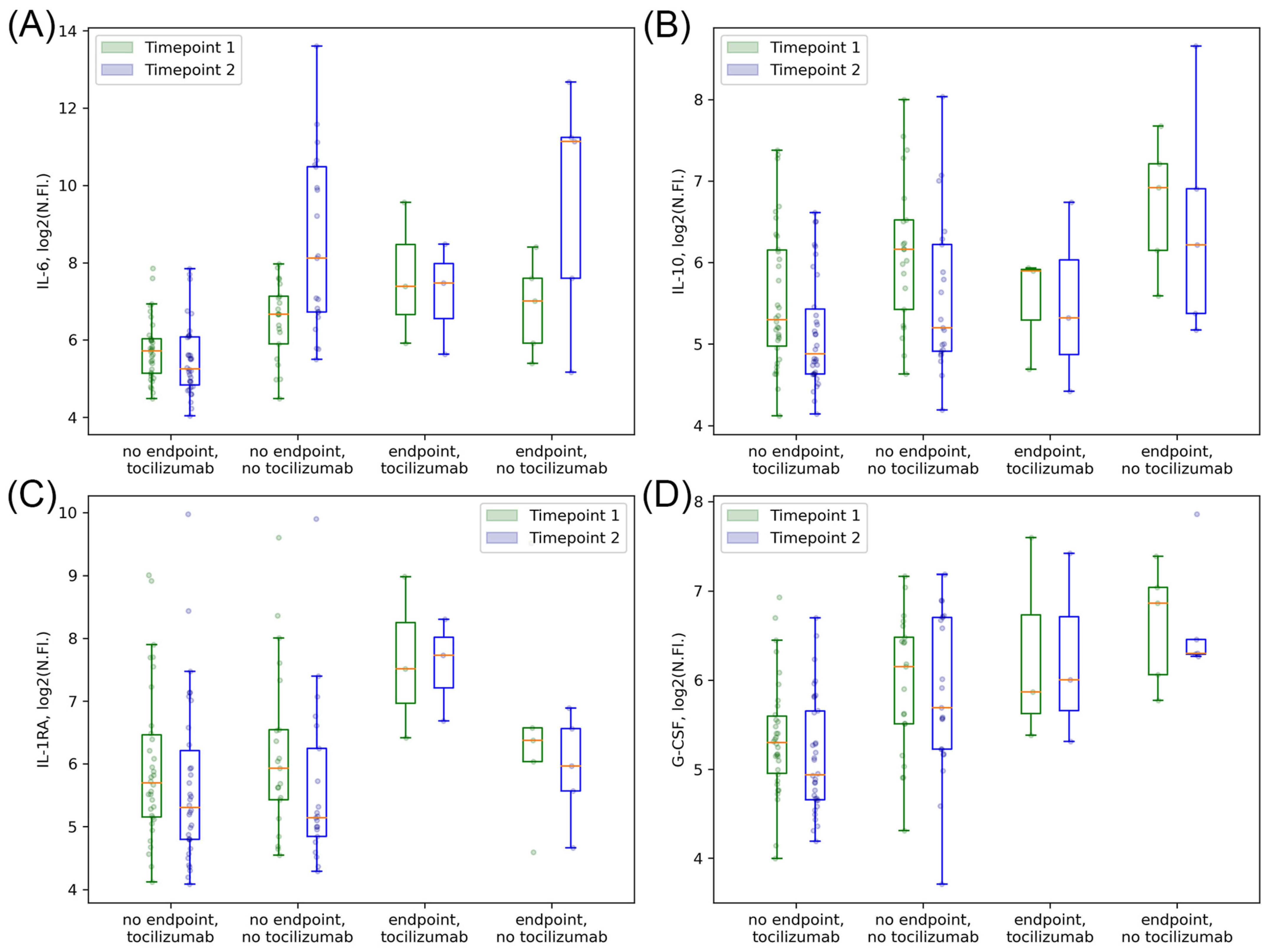
In our study, not only did we investigate the effect of tocilizumab on the prognosis of patients, but we also tried to identify the main cytokines that can predict the effectiveness of this therapy. We found that while many cytokines, including IL-6, showed an impact on the prognosis of COVID-19 patients, only two of them, IL-1RA and IL-10, were of clinical significance in the subgroup of patients receiving tocilizumab therapy. At the same time, IL-6 had a borderline significance for the prognosis in that subgroup of patients. The importance of IL-6 and IL-10 as major pro- and antiinflammatory cytokines was shown in many trials on COVID-19 [
49,
50,
98,
99,
112,
113] with meta-analyses showing the prevalent role of these two cytokines in disease severity and prognosis [
106]. However, when analyzed according to the time from disease onset, the IL-6 elevation was found only at the late stage of severe COVID-19 while IL-10 and IL-1RA levels were significantly associated with disease severity and patients’ outcomes already at the first week after symptom onset [
114].
Moreover, according to our data, IL-1RA was the only cytokine that showed a prognostic significance after separation into groups of patients with and without tocilizumab therapy as well as a significant dynamic decrease in patients receiving tocilizumab, especially in those with the worse prognosis. IL-1RA was shown to control inflammatory responses during the early stages of immune activation [
115] while binding to the IL-1R and modulating the production of IL-1 and type I IFN [
116], two important cytokines involved in the early phase of coronavirus infection [
117,
118]. Finally, because of the difference in the IL-1RA serum concentrations in severe and mild COVID-19, it is assumed that higher levels of IL-1RA observed in severe cases suggest an overactive immune response, which may contribute to the inflammation-induced tissue damage and therefore correlate well with the prognosis [
114].
Overall, most of the individual cytokines in our study showed no significant effect on the prognosis of patients receiving tocilizumab therapy. Therefore, we assume that a cytokine signature including several potent individual cytokines (i.e., Il-6, IL-1RA, and IL-10) in addition to the standard laboratory markers might be a more useful tool in the stratification of patients with COVID-19 and CCS that will benefit from the immunomodulatory therapy.
4. Materials and Methods
We performed a non-randomized observational trial of patients admitted to Davydovsky Moscow City Clinical Hospital and to Moscow Clinical Hospital №40 from April to December 2020 with an initial diagnosis of COVID-19 infection. During this time period, we included prospectively 140 patients, whom we followed up during the hospitalization and analysed their outcomes in correlation to their clinical and laboratory characteristics as well as therapy received.
Inclusion criteria were:
positive results of polymerase chain reaction (PCR) or IgM measurement for SARS-CoV-2;
COVID-19 pneumonia defined by computed tomography (CT);
moderate or severe course of the disease (criteria are summarized in
Table 9 [
119]);
signed informed written consent;
age > 18.
Exclusion criteria were:
presence of acute or chronic infectious diseases other than COVID-19;
presence of acute and chronic systemic inflammatory diseases or any type of cancer;
negative PCR or antibody test for SARS-CoV-2.
Upon hospitalization, patients were treated according to the Russian National Clinical COVID-19 Recommendations, including IL-6 receptor blocking antibody tocilizumab and steroids. Of the 140 patients included because of the presence of COVID-19 symptoms, 11.4% further tested negative for SARS-CoV-2 by PCR or antibody test and therefore were excluded from the analysis. During the follow-up period, we further excluded all patients receiving any other immunomodulatory therapy, such as other anti-cytokine drugs or antibiotics with immunomodulatory effect, cytokine adsorption techniques, or reconvalescent plasma. After exclusion of patients with non-specified immunomodulatory therapy, we performed an analysis of 98 patients receiving either no immunomodulatory therapy (
n = 46) or tocilizumab therapy (
n = 52) together and in separated subgroups with and without anti-cytokine therapy. We also performed a separate analysis of patients dependent on the utilization of steroid therapy. General patient characteristics are presented in
Table 10.
In all patients, we assessed standard clinical characteristics, such as grade of pneumonia on CT scan, temperature, respiratory rate, and oxygen saturation, as well as standard laboratory parameters, including complete blood count (hemoglobin level, erythrocyte count, platelet count, white blood cell, and lymphocyte/neutrophil count), biochemical parameters (total protein, bilirubin, creatinine, glucose, aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), ferritin, triglycerides), coagulation parameters (fibrinogen, D-dimer, prothrombin time (PT)), and hs-CRP. Blood samples collected in EDTA tubes during the standard blood testing were further used for a multiplexed assessment of 41 cytokines with a bead-based assay. Blood tests were assessed twice: the first time within the first 5 days after admission (in patients receiving immunomodulatory therapy, within 24 h before the first administration of the treatment), timepoint 1, and the second time within 3–5 days after the first blood test, timepoint 2.
4.1. Blood Collection
The utilization of blood samples for research purposes was approved by the Moscow city ethics committee. To obtain plasma for the cytokine analysis we used blood samples collected in vacuum tubes with EDTA (Sarstedt, Nuembrecht, Germany). After collection, blood samples were centrifuged in a bucket rotor centrifuge for 10 min at 1000× g at room temperature (RT). We transferred the upper plasma layer into a new tube while leaving approximately 1 mL of plasma above the blood cells intact to reduce cellular contamination. Transferred plasma was pipetted thoroughly, aliquoted by 300 µL, and stored at −80 °C until further analysis.
4.2. Cytokine Measurement
Forty-one cytokines in blood were measured with a commercial kit MILLIPLEX MAP Human Cytokine/Chemokine Magnetic Bead Panel (Merck Millipore, Burlington, MA, USA). The cytokine panel included interleukin-1α (IL-1α), IL-1β, IL-1RA, IL-2, IL-3, IL-4, IL-5, IL-6, IL-7, IL-8, IL-9, IL-10, IL-12 (p40), IL-12 (p70), IL-13, IL-15, IL-17A, fractalkine (CX3CL1), growth-regulated alpha (GRO-α or CXCL1), interferon-γ-induced protein-10 (IP-10 or CXCL10), monocyte chemoattractant protein-1 (MCP-1 or CCL2), MCP-3 (CCL7), macrophage inflammatory protein-1α (MIP-1α or CCL3), MIP-1β (CCL4), regulated on activation normally T cell expressed and secreted (RANTES or CCL5), eotaxin (CCL11), macrophage-derived chemokine (MDC or CCL22), soluble CD40-ligand (sCD40L), epidermal growth factor (EGF), fibroblast growth factor-2 (FGF-2), Fms-like tyrosine kinase 3 ligand (Flt-3L), vascular endothelial growth factor (VEGF), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), platelet-derived growth factor-AA (PDGF-AA), PDGF-AB/BB, transforming growth factor-α (TGF-α), interferon-α2 (IFN-α2), IFN-γ, and tumor necrosis factor-α (TNF-α) and TNF-β.
The standard curve was built up from 8 standard dilutions in triplicate, with the 1st–3rd standard dilutions with dilution factor 5 and the 4th–8th dilutions with dilution factor 4. We used a serum matrix diluted in an assay buffer to mimic the matrix effect on the standard curve, controls, and blank wells. Thus, 25 µL of standards and controls were diluted with 25 µL of serum matrix. Plasma was diluted 4 times in an assay buffer to reduce the matrix effect and added in a volume of 50 µL to each well. We added 15 µL of 41-plex magnetic beads to each well and incubated for 18 h at 4 °C. Beads were washed twice with an automatic magnetic washer (Biotek ELx405, Winooski, VT, USA) and incubated with detection antibodies for 1 h at 25 °C. Antibodies were diluted with wash buffer 1.93 times and added in the amount of 25 µL per well. After incubation, we added 15 µL of Streptavidin-PE solution to each well and incubated the final solution for 30 min at 25 °C. Then, beads were washed twice, resuspended in the sheath fluid, and analyzed with a Luminex 200 instrument (Luminex Corp, Austin, TX, USA). For the analysis, we collected 100 beads per region. During the analysis, we used 5PL fit for the standard curve. We excluded RANTES from the analysis because of a high inhibition level.
4.3. Clinical Endpoints Assessment
We analyzed a short-term combined clinical endpoint for all the patients as:
4.4. Statistical Analysis
We performed statistical analysis with Python-3. The expression values obtained in the present study were in most cases not normally distributed according to the Shapiro–Wilk test, and therefore are represented as medians and interquartile ranges (Q25–Q75). Age is presented as mean and standard deviation. Since distributions were not normal, for comparison of several groups we used the Mann–Whitney rank test with continuity correction. For the analysis of categorical parameters, we used a two-tailed Fisher’s Exact Test with 2 × 2 frequency tables. To overcome errors from multiple comparisons we performed a Benjamini–Hochberg FDR correction with a calculation of critical values for each comparison matched with corresponding p-values; we calculated adjusted p-values and compared them with a critical value of 0.05; below, “p-value” refers to Benjamini–Hochberg-adjusted p-values, if not stated otherwise. For a heatmap data visualization, p-values are shown as log10 from original p-values, where log10 p-values ≤ 1.3 correspond to original p-values < 0.05. For the age distribution, we made the assumption of its normality and analyzed this distribution using the t-test.
In many cases, cytokine levels were outside the limits of detection of the Luminex device, which did not allow their quantitative analysis: 12.5% of all measurements were either below or above limits of detection, with more than 25% of values systematically missing for several cytokines. Therefore, following the published method [
120], for assessing the cytokine levels we additionally used log2 of pre-normalized fluorescence intensity values. These values were used for quantitative comparison of cytokine levels between different subgroups of patients; it was additionally
z-score normalized and used as a basis for hierarchical clustering analysis. For the assessment of clinically significant thresholds associated with clinical endpoints, we performed ROC analysis; however, because of the size of the experimental group, we did not split the data into training and testing subsets.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}