


Red Blood Cells: A Newly Described Partner in Central Retinal Vein Occlusion Pathophysiology?

Abstract
:1. Introduction
2. Central Retinal Vein Occlusion
3. Central Retinal Vein Occlusion: Not a Simple Thrombotic Disorder
4. Central Retinal Vein Occlusion: How to Treat?
5. Red Blood Cell Dysfunctions and Erythropathy
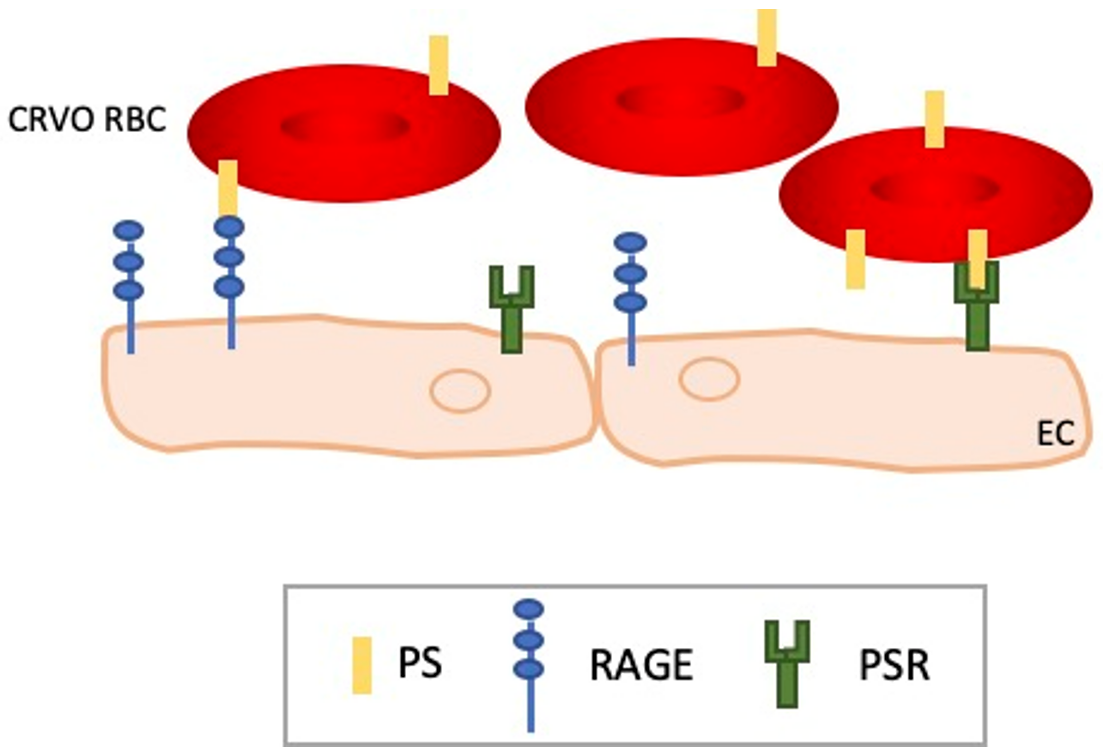
6. RBC Dysfunctions in CRVO
7. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, P.; Xu, Y.; Zha, M.; Zhang, Y.; Rudan, I. Global epidemiology of retinal vein occlusion: A systematic review and meta-analysis of prevalence, incidence, and risk factors. J. Glob. Health 2019, 9, 010427. [Google Scholar] [CrossRef] [PubMed]
- Cugati, S.; Wang, J.J.; Rochtchina, E.; Mitchell, P. Ten-year incidence of retinal vein occlusion in an older population: The Blue Mountains Eye Study. Arch. Ophthalmol. 2006, 124, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Laouri, M.; Chen, E.; Looman, M.; Gallagher, M. The burden of disease of retinal vein occlusion: Review of the literature. Eye 2011, 25, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Scott, I.U. Clinical practice. Retinal-Vein Occlusion N. Engl. J. Med. 2010, 363, 2135–2144. [Google Scholar] [CrossRef]
- Chen, H.-F.; Chen, M.-C.; Lai, C.-C.; Yeung, L.; Wang, N.-K.; Chen, H.S.-L.; Ku, W.-C.; Wu, S.-C.; Chang, S.H.L.; Chuang, L.-H. Neovascular glaucoma after central retinal vein occlusion in pre-existing glaucoma. BMC Ophthalmol. 2014, 14, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natural history and Clinical Management of Central Retinal Vein Occlusion. The Central Vein Occlusion Study Group. Arch. Ophthalmol. 1997, 115, 486–491. [Google Scholar] [CrossRef]
- Ponto, K.A.; Scharrer, I.; Binder, H.; Korb, C.; Rosner, A.K.; Ehlers, T.O.; Rieser, N.; Grübel, N.C.; Rossmann, H.; Wild, P.S.; et al. Hypertension and multiple cardiovascular risk factors increase the risk for retinal vein occlusions: Results from the Gutenberg Retinal Vein Occlusion Study. J. Hypertens. 2019, 37, 1372–1383. [Google Scholar] [CrossRef]
- Sivaprasad, S.; Amoaku, W.M.; Hykin, P.; Group, R.V.O.G. The Royal College of Ophthalmologists Guidelines on retinal vein occlusions: Executive summary. Eye 2015, 29, 1633–1638. [Google Scholar] [CrossRef] [Green Version]
- Bradshaw, S.E.; Gala, S.; Nanavaty, M.; Shah, A.; Mwamburi, M.; Kefalas, P. Systematic literature review of treatments for management of complications of ischemic central retinal vein occlusion. BMC Ophthalmol. 2016, 16, 104. [Google Scholar] [CrossRef]
- Scott, I.U.; Campochiaro, P.A.; Newman, N.J.; Biousse, V. Retinal vascular occlusions. Lancet 2020, 396, 1927–1940. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S. Classification of central retinal vein occlusion. Ophthalmology 1983, 90, 458–474. [Google Scholar] [CrossRef]
- Kumar, D.R.; Hanlin, E.; Glurich, I.; Mazza, J.J.; Yale, S.H. Virchow’s contribution to the understanding of thrombosis and cellular biology. Clin. Med. Res. 2010, 8, 168–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, M.H.; Balaratnasingam, C.; Yu, P.K.; Morgan, W.H.; McAllister, I.L.; Cringle, S.J.; Yu, D.-Y. Alterations to vascular endothelium in the optic nerve head in patients with vascular comorbidities. Exp. Eye Res. 2013, 111, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.C.; den Heijer, M.; Cruysberg, J.R.; Wollersheim, H.; Bredie, S.J. Retinal vein occlusion: A form of venous thrombosis or a complication of atherosclerosis? A meta-analysis of thrombophilic factors. Thromb. Haemost. 2005, 93, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Williamson, T.H. A “throttle” mechanism in the central retinal vein in the region of the lamina cribrosa. Br. J. Ophthalmol. 2007, 91, 1190–1193. [Google Scholar] [CrossRef] [Green Version]
- Paques, M.; Baillart, O.; Genevois, O.; Gaudric, A.; Levy, B.I.; Sahel, J. Systolodiastolic variations of blood flow during central retinal vein occlusion: Exploration by dynamic angiography. Br. J. Ophthalmol. 2005, 89, 1036–1040. [Google Scholar] [CrossRef] [Green Version]
- Green, W.R.; Chan, C.C.; Hutchins, G.M.; Terry, J.M. Central retinal vein occlusion: A prospective histopathologic study of 29 eyes in 28 cases. Retina 1981, 1, 27–55. [Google Scholar] [CrossRef]
- Rehak, M.; Krcova, V.; Slavik, L.; Fric, E.; Langova, K.; Ulehlova, J.; Rehak, J. The role of thrombophilia in patients with retinal vein occlusion and no systemic risk factors. Can. J. Ophthalmol. 2010, 45, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Williamson, T.H.; Rumley, A.; Lowe, G.D. Blood viscosity, coagulation, and activated protein C resistance in central retinal vein occlusion: A population controlled study. Br. J. Ophthalmol. 1996, 80, 203–208. [Google Scholar] [CrossRef]
- Greven, C.M.; Wall, A.B. Peripheral retinal neovascularization and retinal vascular occlusion associated with activated protein C resistance. Am. J. Ophthalmol. 1997, 124, 687–689. [Google Scholar] [CrossRef] [PubMed]
- Bertram, B.; Remky, A.; Arend, O.; Wolf, S.; Reim, M. Protein C, protein S, and antithrombin III in acute ocular occlusive diseases. Ger. J. Ophthalmol. 1995, 4, 332–335. [Google Scholar] [PubMed]
- Marcinkowska, A.; Cisiecki, S.; Rozalski, M. Platelet and Thrombophilia-Related Risk Factors of Retinal Vein Occlusion. J. Clin. Med. 2021, 10, 3080. [Google Scholar] [CrossRef] [PubMed]
- Romiti, G.F.; Corica, B.; Borgi, M.; Visioli, G.; Pacella, E.; Cangemi, R.; Proietti, M.; Basili, S.; Raparelli, V. Inherited and acquired thrombophilia in adults with retinal vascular occlusion: A systematic review and meta-analysis. J. Thromb. Haemost. 2020, 18, 3249–3266. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Schoene, N.; Harris, W. Mean platelet volume as an indicator of platelet activation: Methodological issues. Platelets 2002, 13, 301–306. [Google Scholar] [CrossRef]
- Pinna, A.; Porcu, T.; Marzano, J.; Boscia, F.; Paliogiannis, P.; Dore, S.; Alessio, G.; Carru, C.; Zinellu, A. Mean Platelet Volume, Red Cell Distribution Width, and Complete Blood Cell Count Indices in Retinal Vein Occlusions. Ophthalmic. Epidemiol. 2021, 28, 39–47. [Google Scholar] [CrossRef]
- Şahin, A.; Şahin, M.; Yüksel, H.; Türkcü, F.M.; Çınar, Y.; Cingü, A.K.; Arı, S.; Çaça, I. The mean platelet volume in patients with retinal vein occlusion. J. Ophthalmol. 2013, 2013, 236371. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, T.; Yilmaz, A. Altered platelet morphological parameters in patients with retinal vein occlusion. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 1934–1939. [Google Scholar]
- Hayreh, S.S.; Zimmerman, M.B.; Podhajsky, P. Hematologic abnormalities associated with various types of retinal vein occlusion. Graefes. Arch. Clin. Exp. Ophthalmol. 2002, 240, 180–196. [Google Scholar] [CrossRef]
- Paciullo, F.; Valeriani, E.; Porfidia, A.; Di Nisio, M.; Donadini, M.P.; Marcucci, R.; Prisco, D.; Cagini, C.; Gresele, P.; Ageno, W. Antithrombotic treatment of retinal vein occlusion: A position statement from the Italian Society on Thrombosis and Haemostasis (SISET). Blood Transfus. 2022, 20, 341–347. [Google Scholar] [CrossRef]
- Arrigo, A.; Bandello, F. Retinal vein occlusion: Drug targets and therapeutic implications. Expert. Opin. Ther. Targets 2021, 25, 847–864. [Google Scholar] [CrossRef] [PubMed]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Bhisitkul, R.B.; Shapiro, H.; Rubio, R.G. Vascular endothelial growth factor promotes progressive retinal nonperfusion in patients with retinal vein occlusion. Ophthalmology 2013, 120, 795–802. [Google Scholar] [CrossRef]
- Mir, T.A.; Kherani, S.; Hafiz, G.; Scott, A.W.; Zimmer-Galler, I.; Wenick, A.S.; Solomon, S.; Han, I.; Poon, D.; He, L.; et al. Changes in Retinal Nonperfusion Associated with Suppression of Vascular Endothelial Growth Factor in Retinal Vein Occlusion. Ophthalmology 2016, 123, 625–634.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.M.; Campochiaro, P.A.; Singh, R.P.; Li, Z.; Gray, S.; Saroj, N.; Rundle, A.C.; Rubio, R.G.; Murahashi, W.Y. Ranibizumab for macular edema following central retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology 2010, 117, 1124–1133.e1. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Brown, D.M.; Awh, C.C.; Lee, S.Y.; Gray, S.; Saroj, N.; Murahashi, W.Y.; Rubio, R.G. Sustained benefits from ranibizumab for macular edema following central retinal vein occlusion: Twelve-month outcomes of a phase III study. Ophthalmology 2011, 118, 2041–2049. [Google Scholar] [CrossRef]
- Sophie, R.; Hafiz, G.; Scott, A.W.; Zimmer-Galler, I.; Nguyen, Q.D.; Ying, H.; Do, D.V.; Solomon, S.; Sodhi, A.; Gehlbach, P.; et al. Long-term outcomes in ranibizumab-treated patients with retinal vein occlusion; the role of progression of retinal nonperfusion. Am. J. Ophthalmol. 2013, 156, 693–705. [Google Scholar] [CrossRef] [Green Version]
- Evoy, K.E.; Abel, S.R. Aflibercept: Newly approved for the treatment of macular edema following central retinal vein occlusion. Ann. Pharmacother. 2013, 47, 819–827. [Google Scholar] [CrossRef]
- Sangroongruangsri, S.; Ratanapakorn, T.; Wu, O.; Anothaisintawee, T.; Chaikledkaew, U. Comparative efficacy of bevacizumab, ranibizumab, and aflibercept for treatment of macular edema secondary to retinal vein occlusion: A systematic review and network meta-analysis. Expert Rev. Clin. Pharmacol. 2018, 11, 903–916. [Google Scholar] [CrossRef] [Green Version]
- Korobelnik, J.-F.; Holz, F.G.; Roider, J.; Ogura, Y.; Simader, C.; Schmidt-Erfurth, U.; Lorenz, K.; Honda, M.; Vitti, R.; Berliner, A.J.; et al. Intravitreal Aflibercept Injection for Macular Edema Resulting from Central Retinal Vein Occlusion: One-Year Results of the Phase 3 GALILEO Study. Ophthalmology 2014, 121, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Jumper, J.M.; Dugel, P.U.; Chen, S.; Blinder, K.J.; Walt, J.G. Anti-VEGF treatment of macular edema associated with retinal vein occlusion: Patterns of use and effectiveness in clinical practice (ECHO study report 2). Clin. Ophthalmol. 2018, 12, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Scott, I.U.; Ip, M.S.; VanVeldhuisen, P.C.; Oden, N.L.; Blodi, B.A.; Fisher, M.; Chan, C.K.; Gonzalez, V.H.; Singerman, L.J.; Tolentino, M. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular Edema secondary to branch retinal vein occlusion: The Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 6. Arch. Ophthalmol. 2009, 127, 1115–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haller, J.A.; Bandello, F.; Belfort, R.; Blumenkranz, M.S.; Gillies, M.; Heier, J.; Loewenstein, A.; Yoon, Y.H.; Jiao, J.; Li, X.-Y.; et al. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion twelve-month study results. Ophthalmology 2011, 118, 2453–2460. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S. Photocoagulation for retinal vein occlusion. Prog. Retin Eye Res. 2021, 85, 100964. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Hafiz, G.; Mir, T.A.; Scott, A.W.; Solomon, S.; Zimmer-Galler, I.; Sodhi, A.; Duh, E.; Ying, H.; Wenick, A.; et al. Scatter Photocoagulation Does Not Reduce Macular Edema or Treatment Burden in Patients with Retinal Vein Occlusion: The RELATE Trial. Ophthalmology 2015, 122, 1426–1437. [Google Scholar] [CrossRef]
- Pernow, J.; Mahdi, A.; Yang, J.; Zhou, Z. Red blood cell dysfunction: A new player in cardiovascular disease. Cardiovasc. Res. 2019, 115, 1596–1605. [Google Scholar] [CrossRef] [Green Version]
- Simon, D.I.; Silverstein, R.L. Atherothrombosis: Seeing Red? Circulation 2015, 132, 1860–1862. [Google Scholar] [CrossRef] [Green Version]
- Weisel, J.W.; Litvinov, R.I. Red blood cells: The forgotten player in hemostasis and thrombosis. J. Thromb. Haemost. 2019, 17, 271–282. [Google Scholar] [CrossRef] [Green Version]
- Huisjes, R.; Bogdanova, A.; van Solinge, W.W.; Schiffelers, R.M.; Kaestner, L.; van Wijk, R. Squeezing for Life-Properties of Red Blood Cell Deformability. Front. Physiol. 2018, 9, 656. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, A.M.; Braunmuller, S.; Wan, J.; Franke, T.; Stone, H.A. The effects of membrane cholesterol and simvastatin on red blood cell deformability and ATP release. Microvasc. Res. 2012, 83, 347–351. [Google Scholar] [CrossRef]
- McMahon, T.J. Red Blood Cell Deformability, Vasoactive Mediators, and Adhesion. Front. Physiol. 2019, 10, 1417. [Google Scholar] [CrossRef] [PubMed]
- Furie, B.; Furie, B.C. Mechanisms of thrombus formation. N. Engl. J. Med. 2008, 359, 938–949. [Google Scholar] [CrossRef]
- Kato, G.J.; Piel, F.B.; Reid, C.D.; Gaston, M.H.; Ohene-Frempong, K.; Krishnamurti, L.; Smith, W.R.; Panepinto, J.A.; Weatherall, D.J.; Costa, F.F.; et al. Sickle cell disease. Nat. Rev. Dis. Primers 2018, 4, 18010. [Google Scholar] [CrossRef] [Green Version]
- Telen, M.J. Erythrocyte adhesion receptors: Blood group antigens and related molecules. Transfus. Med. Rev. 2005, 19, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Colin, Y.; Le Van Kim, C.; El Nemer, W. Red cell adhesion in human diseases. Curr. Opin. Hematol. 2014, 21, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Collec, E.; Connes, P.; Akker, E.V.D.; De Villemeur, T.B.; Belmatoug, N.; Von Lindern, M.; Ameziane, N.; Hermine, O.; Colin, Y.; et al. Abnormal properties of red blood cells suggest a role in the pathophysiology of Gaucher disease. Blood 2013, 121, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Dupuis, L.; Chipeaux, C.; Bourdelier, E.; Martino, S.; Reihani, N.; Belmatoug, N.; De Villemeur, T.B.; Hivert, B.; Moussa, F.; Le Van Kim, C.; et al. Effects of sphingolipids overload on red blood cell properties in Gaucher disease. J. Cell. Mol. Med. 2020, 24, 9726–9736. [Google Scholar] [CrossRef]
- Adar, T.; Ben-Ami, R.; Elstein, D.; Zimran, A.; Berliner, S.; Yedgar, S.; Barshtein, G. Aggregation of red blood cells in patients with Gaucher disease. Br. J. Haematol. 2006, 134, 432–437. [Google Scholar] [CrossRef]
- Kuhn, V.; Diederich, L.; Keller, T.C.S.; Kramer, C.M.; Lückstädt, W.; Panknin, C.; Suvorava, T.; Isakson, B.E.; Kelm, M.; Cortese-Krott, M.M. Red Blood Cell Function and Dysfunction: Redox Regulation, Nitric Oxide Metabolism, Anemia. Antioxid. Redox Signal. 2017, 26, 718–742. [Google Scholar] [CrossRef] [Green Version]
- Salgado, M.T.; Cao, Z.; Nagababu, E.; Mohanty, J.G.; Rifkind, J.M. Red blood cell membrane-facilitated release of nitrite-derived nitric oxide bioactivity. Biochemistry 2015, 54, 6712–6723. [Google Scholar] [CrossRef]
- Chabanel, A.; Glacet-Bernard, A.; Lelong, F.; Taccoen, A.; Coscas, G.; Samama, M.M. Increased red blood cell aggregation in retinal vein occlusion. Br. J. Haematol. 1990, 75, 127–131. [Google Scholar] [CrossRef]
- Arend, O.; Remky, A.; Jung, F.; Kiesewetter, H.; Reim, M.; Wolf, S. Role of rheologic factors in patients with acute central retinal vein occlusion. Ophthalmology 1996, 103, 80–86. [Google Scholar] [CrossRef]
- Mannini, L.; Marcucci, R.; Bolli, P.; Sodi, A.; Giambene, B.; Menchini, U.; Gensini, G.F.; Abbate, R.; Prisco, D.; Sofi, F. Role of haemorheological factors in patients with retinal vein occlusion. Thromb. Haemost. 2007, 98, 1215–1219. [Google Scholar] [CrossRef]
- Becatti, M.; Marcucci, R.; Gori, A.M.; Mannini, L.; Grifoni, E.; Liotta, A.A.; Sodi, A.; Tartaro, R.; Taddei, N.; Rizzo, S.; et al. Erythrocyte oxidative stress is associated with cell deformability in patients with retinal vein occlusion. J. Thromb. Haemost. 2016, 14, 2287–2297. [Google Scholar] [CrossRef] [Green Version]
- Glacet-Bernard, A.; Atassi, M.; Fardeau, C.; Romanet, J.-P.; Tonini, M.; Conrath, J.; Denis, P.; Mauget-Faÿsse, M.; Coscas, G.; Soubrane, G.; et al. Hemodilution therapy using automated erythrocytapheresis in central retinal vein occlusion: Results of a multicenter randomized controlled study. Graefes. Arch. Clin. Exp. Ophthalmol. 2011, 249, 505–512. [Google Scholar] [CrossRef]
- Donati, G.; Mavrakanas, N.; Pournaras, C.-J. Isovolumic hemodilution in the management of the acute phase of central retinal vein occlusion: A pilot study. J. Fr. Ophtalmol. 2009, 32, 750–756. [Google Scholar] [CrossRef]
- Douat, J.; Ancele, E.; Cournot, M.; Pagot-Mathis, V.; Mathis, A.; Quintyn, J.C. Treatment of central retinal vein occlusion by isovolemic hemodilution. J. Fr. Ophtalmol. 2007, 30, 1007–1012. [Google Scholar] [CrossRef]
- Wiek, J.; Schade, M.; Wiederholt, M.; Arntz, H.R.; Hansen, L.L. Haemorheological changes in patients with retinal vein occlusion after isovolaemic haemodilution. Br. J. Ophthalmol. 1990, 74, 665–669. [Google Scholar] [CrossRef] [Green Version]
- Michiels, J.J.; Berneman, Z.N.; Schroyens, W.; Van Vliet, H.H. Pathophysiology and treatment of platelet-mediated microvascular disturbances, major thrombosis and bleeding complications in essential thrombocythaemia and polycythaemia vera. Platelets 2004, 15, 67–84. [Google Scholar] [CrossRef]
- Elliott, M.A.; Tefferi, A. Thrombosis and haemorrhage in polycythaemia vera and essential thrombocythaemia. Br. J. Haematol. 2005, 128, 275–290. [Google Scholar] [CrossRef]
- Orkin, S.H. Diversification of haematopoietic stem cells to specific lineages. Nat. Rev. Genet. 2000, 1, 57–64. [Google Scholar] [CrossRef]
- Polycythaemia Vera. In Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues; Jaffe, E.S.; Harris, N.L.; Stein, H.; Vardiman, J.W. (Eds.) IARC: Lyon, France, 2001. [Google Scholar]
- Héron, E.; Marzac, C.; Feldman-Billard, S.; Girmens, J.-F.; Paques, M.; Delarue, R.; Piette, J.-C.; Casadevall, N.; Hermine, O. Endogenous erythroid colony formation in patients with retinal vein occlusion. Ophthalmology 2007, 114, 2155–2161. [Google Scholar] [CrossRef]
- James, C.; Ugo, V.; Casadevall, N.; Constantinescu, S.N.; Vainchenker, W. A JAK2 mutation in myeloproliferative disorders: Pathogenesis and therapeutic and scientific prospects. Trends Mol. Med. 2005, 11, 546–554. [Google Scholar] [CrossRef]
- Baxter, E.J.; Scott, L.M.; Campbell, P.J.; East, C.; Fourouclas, N.; Swanton, S.; Vassiliou, G.S.; Bench, A.J.; Boyd, E.M.; Curtin, N.; et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet 2005, 365, 1054–1061. [Google Scholar] [CrossRef]
- Wautier, M.P.; Heron, E.; Picot, J.; Colin, Y.; Hermine, O.; Wautier, J.L. Red blood cell phosphatidylserine exposure is responsible for increased erythrocyte adhesion to endothelium in central retinal vein occlusion. J. Thromb. Haemost. 2011, 9, 1049–1055. [Google Scholar] [CrossRef]
- Bratton, D.L.; Henson, P.M. Apoptotic cell recognition: Will the real phosphatidylserine receptor(s) please stand up? Curr. Biol. 2008, 18, R76-9. [Google Scholar] [CrossRef] [Green Version]
- Su, Y.; Deng, X.; Ma, R.; Dong, Z.; Wang, F.; Shi, J. The Exposure of Phosphatidylserine Influences Procoagulant Activity in Retinal Vein Occlusion by Microparticles, Blood Cells, and Endothelium. Oxid. Med. Cell. Longev. 2018, 2018, 3658476. [Google Scholar] [CrossRef]


{kind=link}
| Reference | CRVO Occurrence Hypothesis |
|---|---|
| Kang et al., 2013 [14] | Thrombus formation |
| Janssen et al., 2005 [15] | |
| Rehak et al., 2010 [19] | |
| Williamson et al., 1996 [20] | |
| Greven et al., 1997 [21] | |
| Bertram et al., 1995 [22] | |
| Paques et al., 2005 [17] | Blood flow slow down |
| Green et al., 1981 [18] | |
| Park et al., 2002 [25] | Platelet dysfunctions |
| Pinna et al., 2021 [26] | |
| Sahin et al., 2013 [27] | |
| Yilmaz et al., 2016 [28] | |
| Hayreh et al., 2002 [29] | |
| Chabanel et al., 1990 [61] | Blood viscosity |
| Arend et al., 1996 [62] | |
| Sofi et al., 2007 [63] | |
| Becatti et al., 2016 [64] | |
| Glacet-Bernard et al., 2011 [65] | |
| Donati et al., 2009 [66] | |
| Douat et al., 2007 [67] | |
| Heron et al., 2007 [73] | Abnormal erythroid differentiation |
| Wautier et al., 2011 [76] | Erythroid PS-mediated mechanism |
| Su et al., 2018 [78] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laurance, S.; Marin, M.; Colin, Y. Red Blood Cells: A Newly Described Partner in Central Retinal Vein Occlusion Pathophysiology? Int. J. Mol. Sci. 2023, 24, 1072. https://doi.org/10.3390/ijms24021072
Laurance S, Marin M, Colin Y. Red Blood Cells: A Newly Described Partner in Central Retinal Vein Occlusion Pathophysiology? International Journal of Molecular Sciences. 2023; 24(2):1072. https://doi.org/10.3390/ijms24021072
Chicago/Turabian StyleLaurance, Sandrine, Mickaël Marin, and Yves Colin. 2023. "Red Blood Cells: A Newly Described Partner in Central Retinal Vein Occlusion Pathophysiology?" International Journal of Molecular Sciences 24, no. 2: 1072. https://doi.org/10.3390/ijms24021072
APA StyleLaurance, S., Marin, M., & Colin, Y. (2023). Red Blood Cells: A Newly Described Partner in Central Retinal Vein Occlusion Pathophysiology? International Journal of Molecular Sciences, 24(2), 1072. https://doi.org/10.3390/ijms24021072