
Acute Cardiovascular and Cardiorespiratory Effects of JWH-018 in Awake and Freely Moving Mice: Mechanism of Action and Possible Antidotal Interventions?

 , , , , ,
, , , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Vehicle
2.2. JWH-018
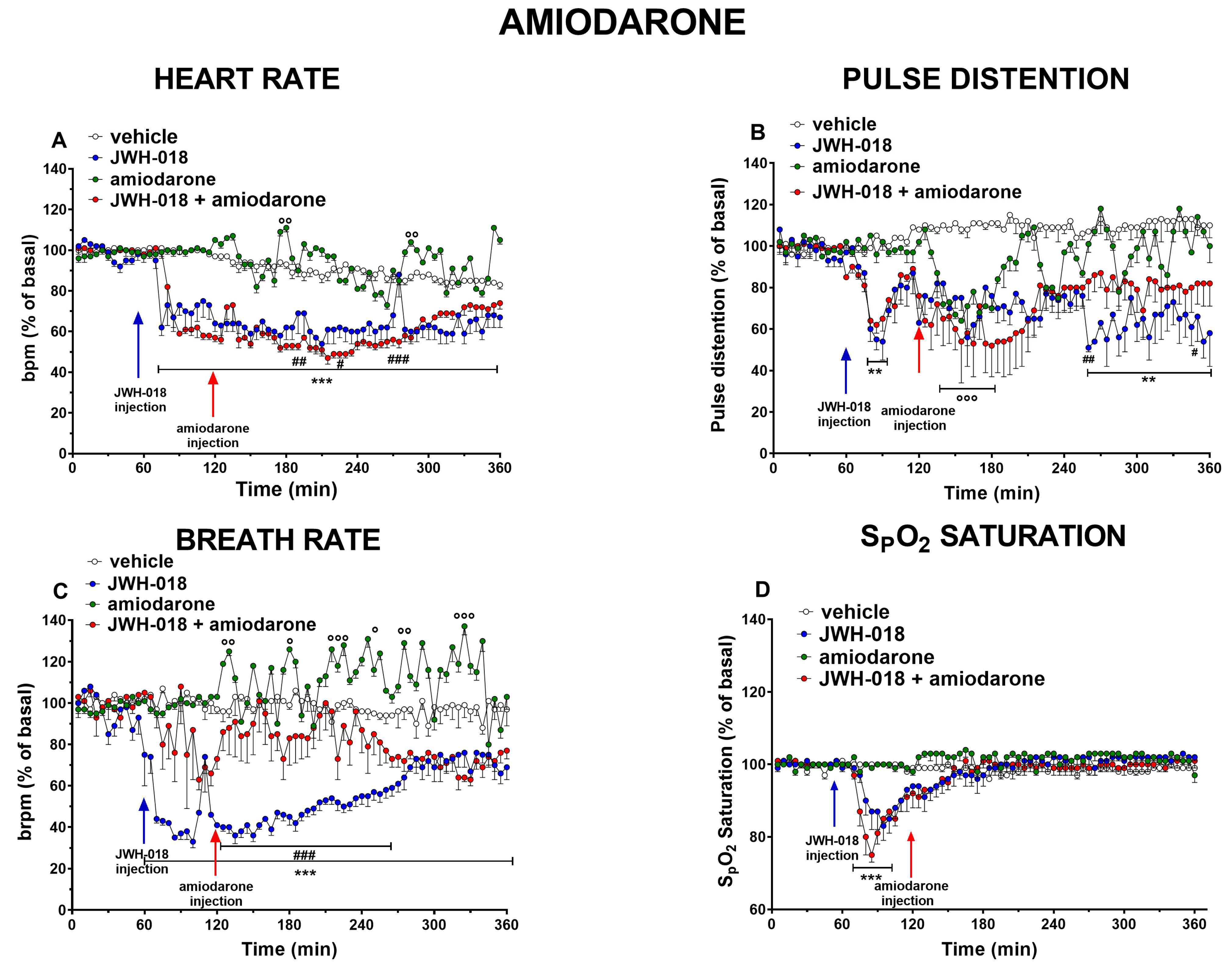
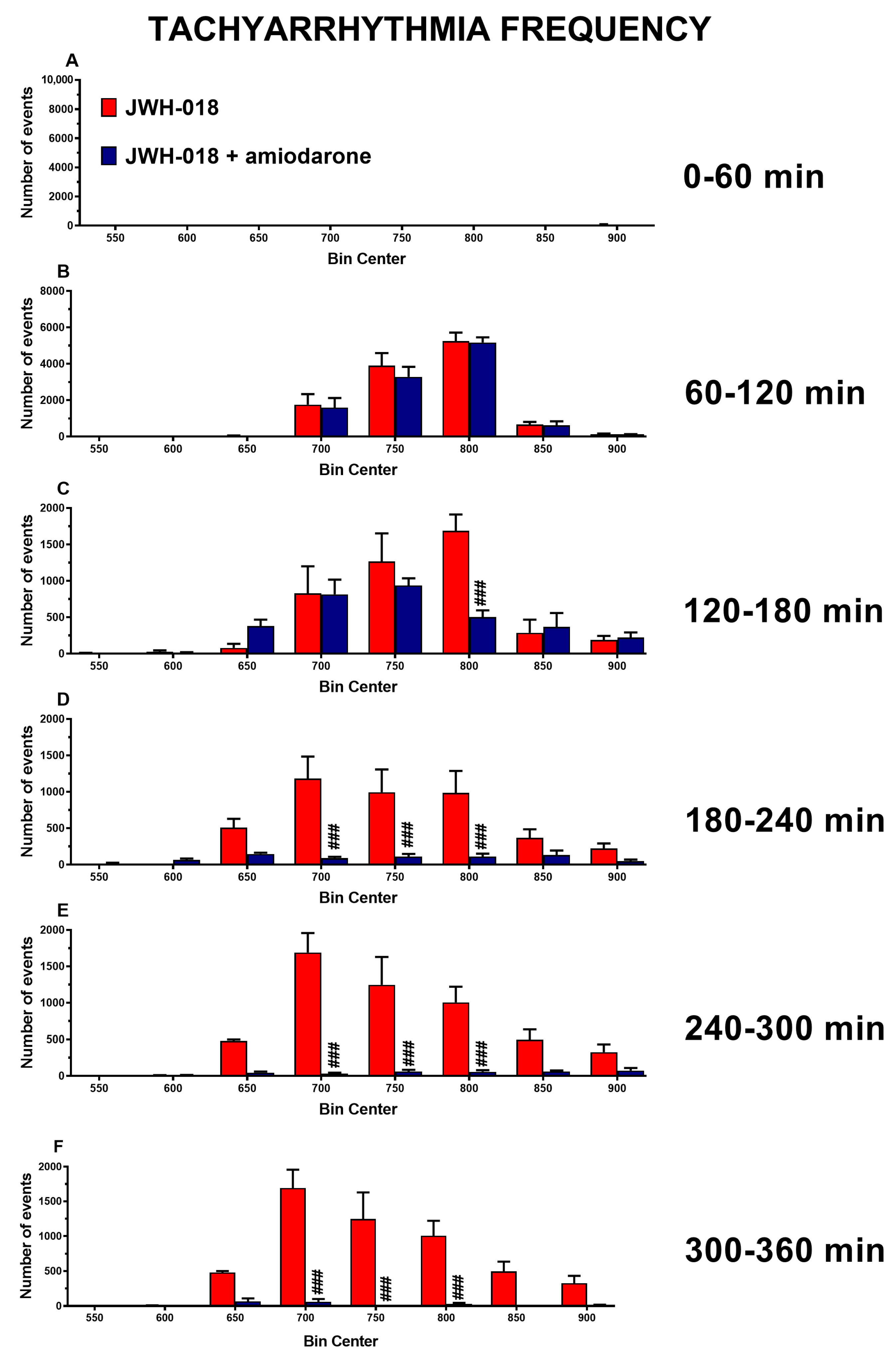
2.3. Amiodarone
2.4. Atropine
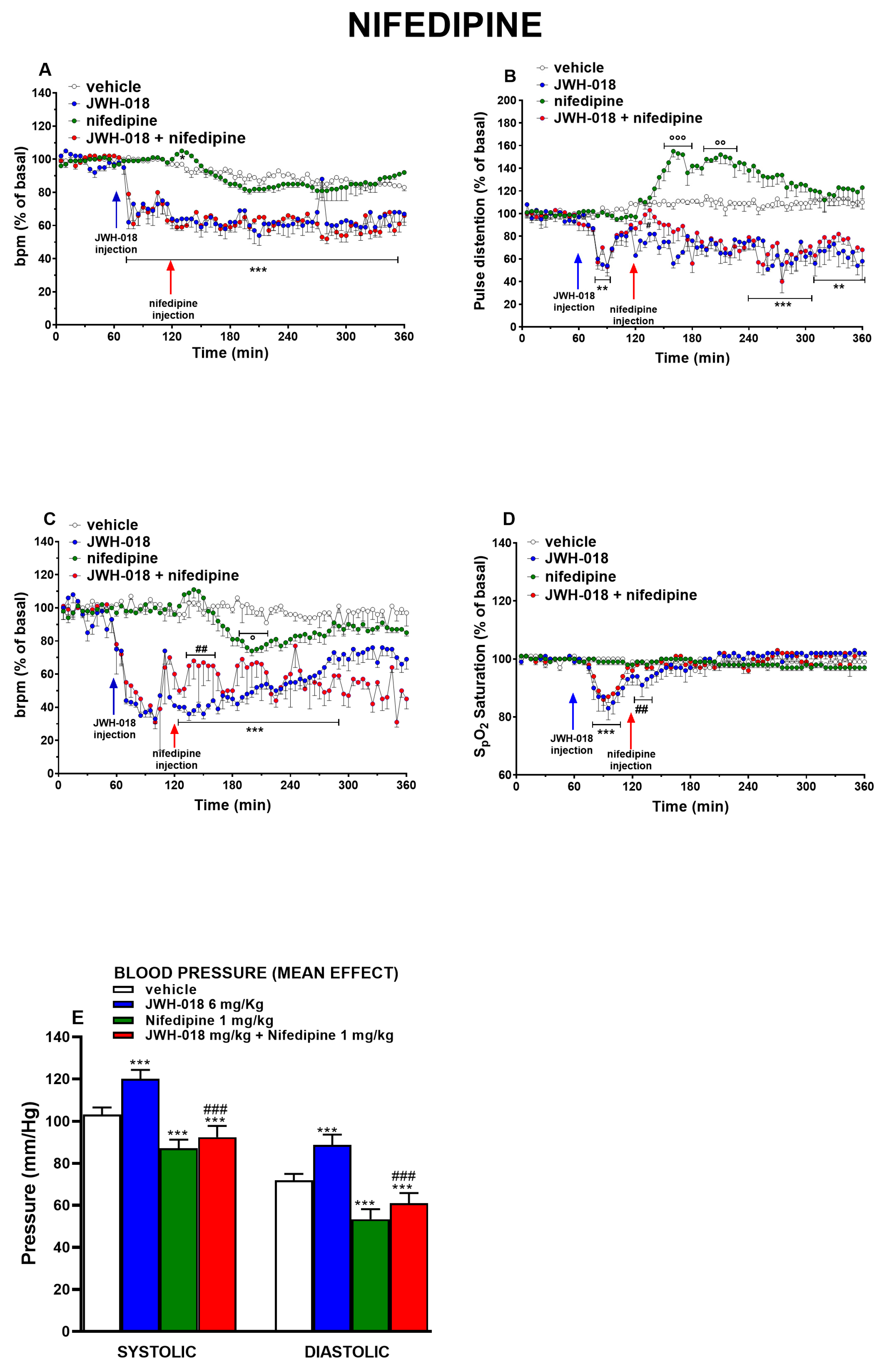
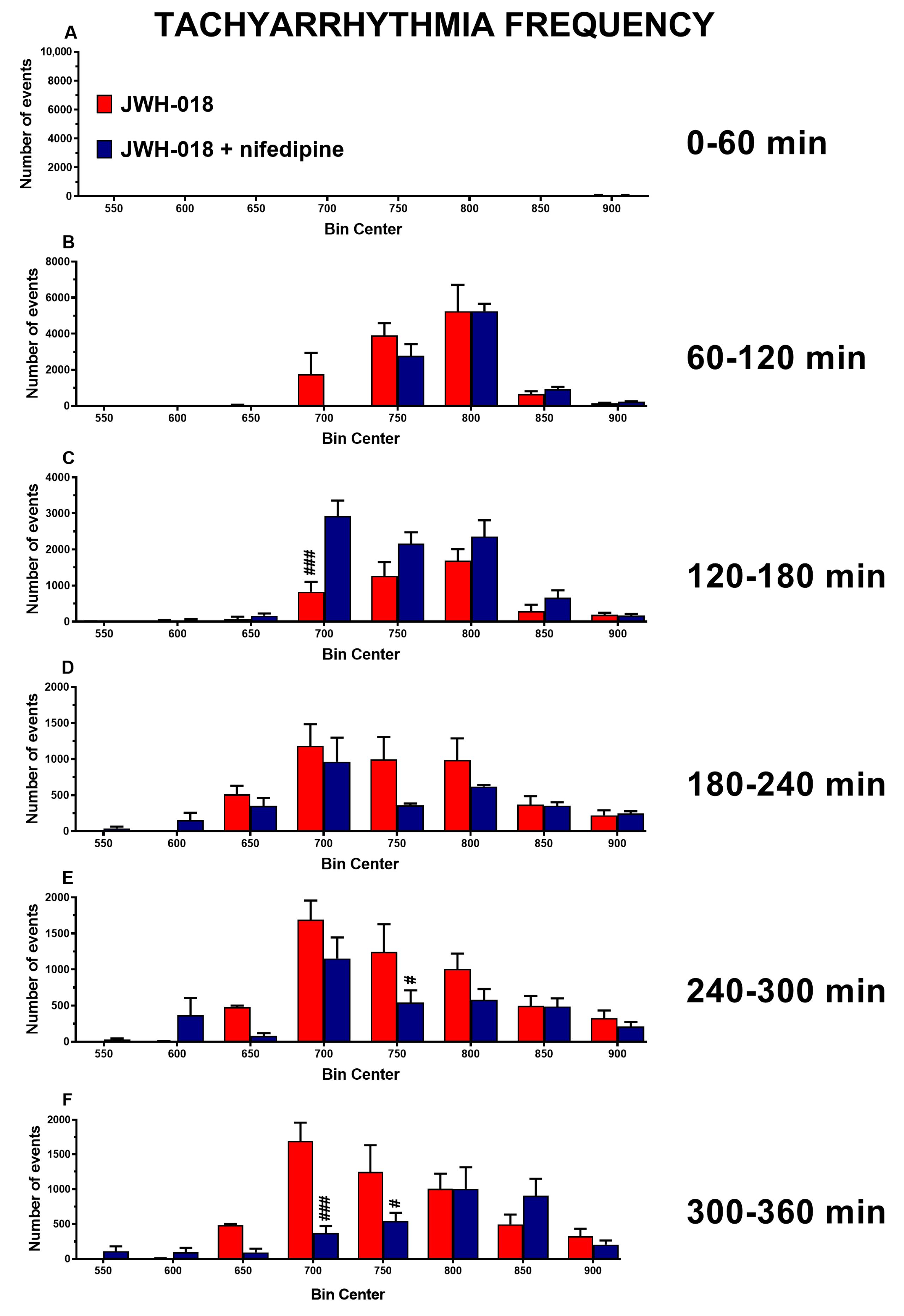
2.5. Nifedipine
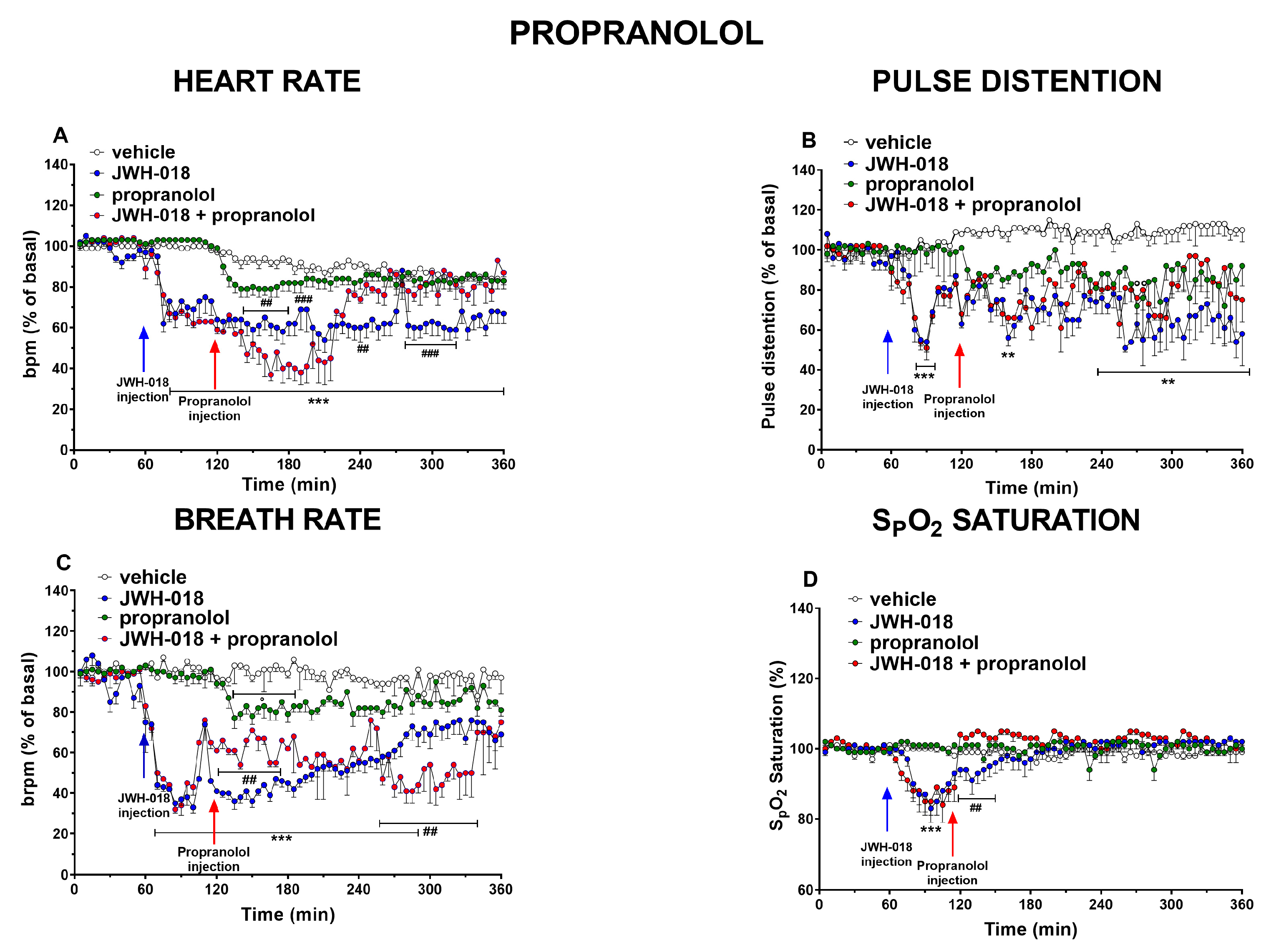
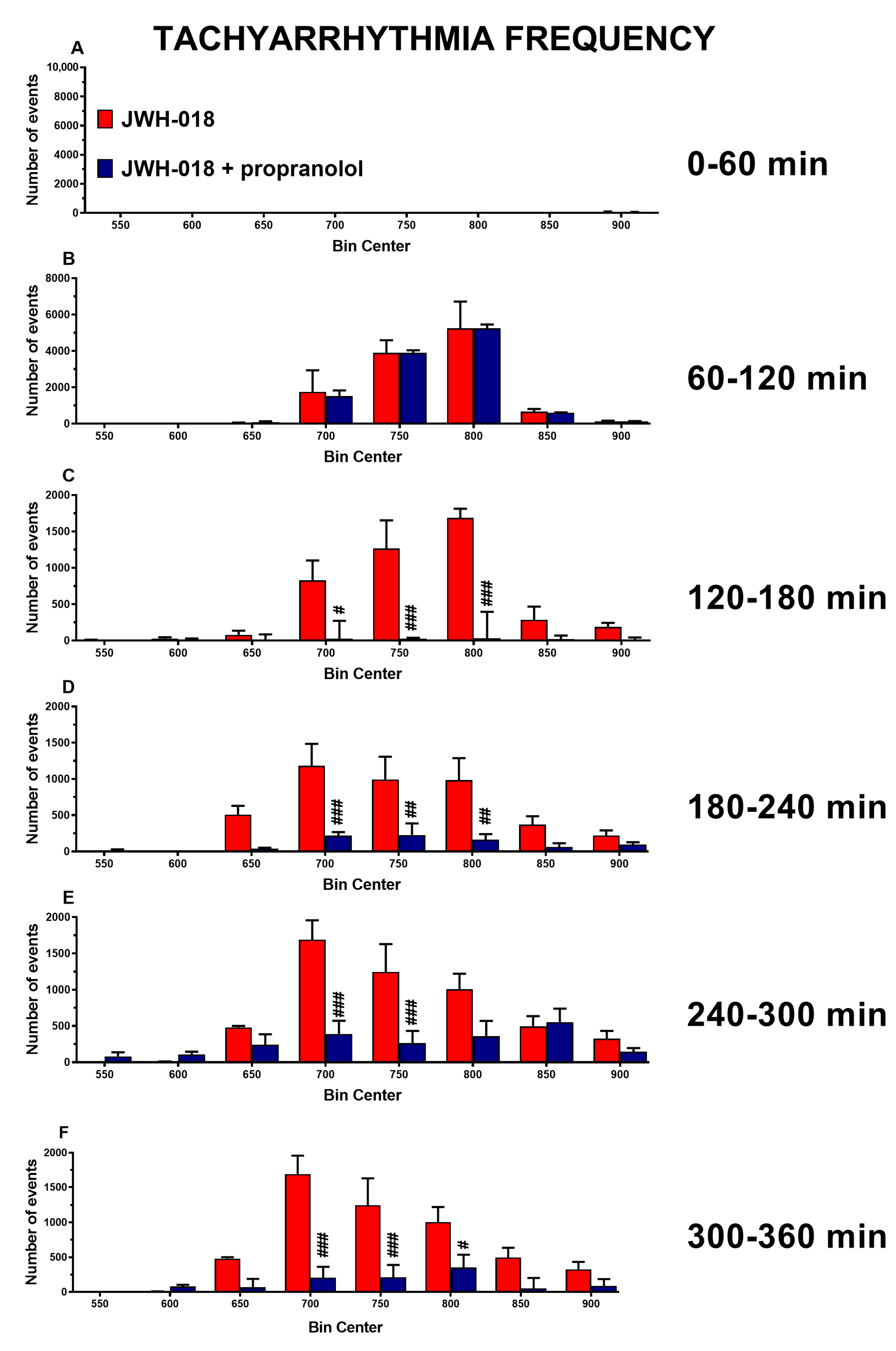
2.6. β1 β2 Blocker
3. Discussion
3.1. Amiodarone
3.2. Atropine
3.3. Nifedipine
3.4. Propranolol
4. Materials and Methods
4.1. Animals
4.2. Drug Preparation and Dose Selection
4.3. Evaluation of Cardiorespiratory Changes
4.4. Data and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AM 251 | 1-(2,4-dichlorophenyl)-5-(4-iodophenyl)-4-methyl-N-(piperidin-1-yl)-1H-pyrazole-3-carboxamide |
| A-V | Atrio-Ventricular |
| BR | Breath Rate |
| CNS | Central Nervous System |
| CV | Cardiovascular |
| dPAG | Dorsal Periaqueductal Gray |
| HR | Heart Rate |
| JWH-018 | 1-pentyl-3-(1-naphthoyl)indole |
| NPS | Novel Psychoactive Substances |
| PD | Pulse Distention |
| S-A | Seno-Atrial |
| SCs | Synthetic Cannabinoids |
| SpO2 | Oxygen blood saturation |
| Δ9-THC | (-)-Δ9-THC or Dronabinol® |
References
- Pisarska, A.; Deluca, P.; Demetrovics, Z.; Moskalewicz, J.; ReDNet, G. Novel psychoactive substances (NPS)-knowledge and expe riences of drug users from Hungary, Poland, the UK and the USA. Neuropsychopharmacol. Hung. 2019, 21, 152–163. [Google Scholar]
- Kennedy, J.; Shanks, K.G.; Van Natta, K.; Prieto Conaway, M.C.; Wiseman, J.M.; Laughlin, B.; Kozak, M. Rapid screening and identification of novel psychoactive substances using PaperSpray interfaced to high resolution mass spectrometry. Clin. Mass Spectrom. 2016, 1, 3–10. [Google Scholar] [CrossRef]
- Locatelli, C.A.; Lonati, D.; Petrolini, V.M. New drugs of abuse and cardiovascular function. In Brain and Heart Dynamics; Govoni, S., Politi, P., Vanoli, E., Eds.; Springer: Cham, Switerland, 2020; pp. 1–27. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). European Drug Report 2021: Trends and Developments; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar]
- United Nations Office on Drugs and Crime (UNODC). Current NPS threats. Available online: https://www.unodc.org/documents/scientific/NPS_threats-IV.pdf (accessed on 12 January 2023).
- Adamowicz, P. Blood concentrations of synthetic cannabinoids. Clin. Toxicol. 2021, 59, 246–251. [Google Scholar] [CrossRef]
- Theunissen, E.L.; Reckweg, J.T.; Hutten, N.R.P.W.; Kuypers, K.P.C.; Toennes, S.W.; Neukamm, M.A.; Halter, S.; Ramaekers, J.G. Psychotomimetic symptoms after a moderate dose of a synthetic cannabinoid (JWH-018): Implications for psychosis. Psychopharmacology 2021, 239, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Bretteville-Jensen, A.L.; Tuv, S.S.; Bilgrei, O.R.; Fjeld, B.; Bachs, L. Synthetic cannabinoids and cathinones: Prevalence and markets. Forensic Sci. Rev. 2013, 25, 7–26. [Google Scholar] [PubMed]
- Norman, C.; McKirdy, B.; Walker, G.; Dugard, P.; NicDaéid, N.; McKenzie, C. Large-scale evaluation of ion mobility spectrometry for the rapid detection of synthetic cannabinoid receptor agonists in infused papers in prisons. Drug Test Anal. 2021, 13, 644–663. [Google Scholar] [CrossRef] [PubMed]
- Tai, H.; Swartz, M.D.; Marsden, D.; Perry, C.L. The Future of Substance Abuse Now: Relationships among Adolescent Use of Vaping Devices, Marijuana, and Synthetic Cannabinoids. Subst. Use Misuse 2021, 56, 192–204. [Google Scholar] [CrossRef]
- Seely, K.A.; Lapoint, J.; Moran, J.H.; Fattore, L. Spice drugs are more than harmless herbal blends: A review of the pharmacology and toxicology of synthetic cannabinoids. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 39, 234–243. [Google Scholar] [CrossRef]
- Hermanns-Clausen, M.; Kneisel, S.; Szabo, B.; Auwärter, V. Acute toxicity due to the confirmed consumption of synthetic cannabinoids: Clinical and laboratory findings. Addiction 2013, 108, 534–544. [Google Scholar] [CrossRef]
- Gurney, S.M.; Scott, K.S.; Kacinko, S.L.; Presley, B.C.; Logan, B.K. Pharmacology, toxicology, and adverse effects of synthetic cannabinoid drugs. Forensic Sci. Rev. 2014, 26, 53–78. [Google Scholar]
- Forrester, M.B.; Kleinschmidt, K.; Schwarz, E.; Young, A. Synthetic cannabinoid exposures reported to Texas poison centers. J. Addict. Dis. 2011, 30, 351–358. [Google Scholar] [CrossRef]
- Harris, C.R.; Brown, A. Synthetic cannabinoid intoxication: A case series and review. J. Emerg. Med. 2013, 44, 360–366. [Google Scholar] [CrossRef]
- Tait, R.J.; Caldicott, D.; Mountain, D.; Hill, S.L.; Lenton, S. A systematic review of adverse events arising from the use of synthetic cannabinoids and their associated treatment. Clin. Toxicol. 2016, 54, 1–13. [Google Scholar] [CrossRef]
- Alon, M.H.; Saint-Fleur, M.O. Synthetic cannabinoid induced acute respiratory depression: Case series and literature review. Respir. Med. Case Rep. 2017, 22, 137–141. [Google Scholar] [CrossRef]
- Alipour, A.; Patel, P.B.; Shabbir, Z.; Gabrielson, S. Review of the many faces of synthetic cannabinoid toxicities. Ment. Health Clin. 2019, 9, 93–99. [Google Scholar] [CrossRef]
- Weresa, J.; Pędzińska-Betiuk, A.; Mińczuk, K.; Malinowska, B.; Schlicker, E. Why do marijuana and synthetic cannabimimetics induce acute myocardial infarction in healthy young people? Cells 2022, 11, 1142. [Google Scholar] [CrossRef]
- Kane, E.M.; Hinson, J.S.; Jordan, C.D.; Paziana, K.; Sauber, N.J.; Rothman, R.E.; Stolbach, A.I. Bradycardia and hypotension after synthetic cannabinoid use: A case series. Am. J. Emerg. Med. 2016, 34, 2055.e1–2055.e2. [Google Scholar] [CrossRef]
- Marchetti, B.; Bilel, S.; Tirri, M.; Arfè, R.; Corli, G.; Roda, E.; Locatelli, C.A.; Cavarretta, E.; De Giorgio, F.; Marti, M. The Old and the New: Cardiovascular and respiratory alterations induced by acute jwh-018 administration compared to δ9-thc-a preclinical study in mice. Int. J. Mol. Sci. 2023, 24, 1631. [Google Scholar] [CrossRef]
- Banister, S.D.; Wilkinson, S.M.; Longworth, M.; Stuart, J.; Apetz, N.; English, K.; Brooker, L.; Goebel, C.; Hibbs, D.E.; Glass, M.; et al. The synthesis and pharmacological evaluation of adamantane-derived indoles: Cannabimimetic drugs of abuse. ACS Chem. Neurosci. 2013, 4, 1081–1092. [Google Scholar] [CrossRef]
- Schindler, C.W.; Gramling, B.R.; Justinova, Z.; Thorndike, E.B.; Baumann, M.H. Synthetic cannabinoids found in “spice” products alter body temperature and cardiovascular parameters in conscious male rats. Drug Alcohol. Depend. 2017, 179, 387–394. [Google Scholar] [CrossRef]
- Schmid, K.; Niederhoffer, N.; Szabo, B. Analysis of the respiratory effects of cannabinoids in rats. Naunyn Schmiedebergs Arch. Pharmacol. 2003, 368, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Bilel, S.; Tirri, M.; Arfè, R.; Stopponi, S.; Soverchia, L.; Ciccocioppo, R.; Frisoni, P.; Strano-Rossi, S.; Miliano, C.; De-Giorgio, F.; et al. Pharmacological and behavioral effects of the synthetic cannabinoid AKB48 in rats. Front. Neurosci. 2019, 13, 1163. [Google Scholar] [CrossRef] [PubMed]
- Mir, A.; Obafemi, A.; Young, A.; Kane, C. Myocardial infarction associated with use of the synthetic cannabinoid K2. Pediatrics 2011, 128, e1622–e1627. [Google Scholar] [CrossRef] [PubMed]
- Shanks, K.G.; Dahn, T.; Terrell, A.R. Detection of JWH-018 and JWH-073 by UPLC-MS-MS in postmortem whole blood casework. J. Anal. Toxicol. 2012, 36, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Trecki, J.; Gerona, R.R.; Schwartz, M.D. Synthetic cannabinoid-related illnesses and deaths. N. Engl. J. Med. 2015, 373, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Al-Saffar, F.; Wannenburg, T. A Unique case of cardiac arrest following K2 abuse. Case Rep. Cardiol. 2014, 2014, 120607. [Google Scholar] [CrossRef]
- Ossato, A.; Vigolo, A.; Trapella, C.; Seri, C.; Rimondo, C.; Serpelloni, G.; Marti, M. JWH-018 impairs sensorimotor functions in mice. Neuroscience 2015, 300, 174–188. [Google Scholar] [CrossRef]
- Tsou, K.; Brown, S.; Sañudo-Peña, M.C.; Mackie, K.; Walker, J.M. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience 1998, 83, 393–411. [Google Scholar] [CrossRef]
- Niederhoffer, N.; Szabo, B. Cannabinoids cause central sympathoexcitation and bradycardia in rabbits. J. Pharmacol. Exp. Ther. 2000, 294, 707–713. [Google Scholar]
- Dean, C.; Hillard, C.J.; Seagard, J.L.; Hopp, F.A.; Hogan, Q.H. Components of the cannabinoid system in the dorsal periaqueductal gray are related to resting heart rate. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 311, R254–R262. [Google Scholar] [CrossRef]
- Pacher, P.; Steffens, S.; Haskó, G.; Schindler, T.H.; Kunos, G. Cardiovascular effects of marijuana and synthetic cannabinoids: The good, the bad, and the ugly. Nat. Rev. Cardiol. 2018, 15, 151–166. [Google Scholar] [CrossRef]
- Steffens, S.; Pacher, P. Targeting cannabinoid receptor CB(2) in cardiovascular disorders: Promises and controversies. Br. J. Pharmacol. 2012, 167, 313–323. [Google Scholar] [CrossRef]
- Tahamtan, A.; Samieipoor, Y.; Nayeri, F.S.; Rahbarimanesh, A.A.; Izadi, A.; Rashidi-Nezhad, A.; Tavakoli-Yaraki, M.; Farahmand, M.; Bont, L.; Shokri, F.; et al. Effects of canna-binoid receptor type 2 in respiratory syncytial virus infection in human subjects and mice. Virulence 2018, 9, 217–230. [Google Scholar] [CrossRef]
- Beaconsfield, P.; Ginsburg, J.; Rainsbury, R. Marihuana smoking. Cardiovascular effects in man and possible mechanisms. N. Engl. J. Med. 1972, 287, 209–212. [Google Scholar] [CrossRef]
- Richards, J.R. Mechanisms for the risk of acute coronary syndrome and arrhythmia associated with phytogenic and synthetic cannabinoid use. J. Cardiovasc. Pharmacol. Ther. 2020, 25, 508–522. [Google Scholar] [CrossRef]
- Nerbonne, J.M.; Kass, R.S. Molecular physiology of cardiac repolarization. Physiol. Rev. 2005, 85, 1205–1253. [Google Scholar] [CrossRef]
- Masini, E.; Sgambellone, S.; Lanzi, C. Psychostimulants and cardiovascular function. In Brain and Heart Dynamics; Govoni, S., Politi, P., Vanoli, E., Eds.; Springer: Cham, Switzerland, 2020; pp. 829–841. [Google Scholar] [CrossRef]
- Ross, H.R.; Napier, I.; Connor, M. Inhibition of recombinant human T-type calcium channels by Delta9-tetrahydrocannabinol and cannabidiol. J. Biol. Chem. 2008, 283, 16124–16134. [Google Scholar] [CrossRef]
- Turkanis, S.A.; Partlow, L.M.; Karler, R. Delta-9-tetrahydrocannabinol depresses inward sodium current in mouse neuroblastoma cells. Neuropharmacology 1991, 30, 73–77. [Google Scholar] [CrossRef]
- Al Kury, L.T.; Voitychuk, O.I.; Yang, K.H.; Thayyullathil, F.T.; Doroshenko, P.; Ramez, A.M.; Shuba, Y.M.; Galadari, S.; Howarth, F.C.; Oz, M. Effects of the endogenous cannabinoid anandamide on voltage-dependent sodium and calcium channels in rat ventricular myocytes. Br. J. Pharmacol. 2014, 171, 3485–3498. [Google Scholar] [CrossRef]
- Barana, A.; Amorós, I.; Caballero, R.; Gómez, R.; Osuna, L.; Lillo, M.P.; Blázquez, C.; Guzmán, M.; Delpón, E.; Tamargo, J. Endocannabinoids and cannabinoid analogues block cardiac hKv1.5 channels in a cannabinoid receptor-independent manner. Cardiovasc. Res. 2010, 85, 56–67. [Google Scholar] [CrossRef]
- Motyka, M.A.; Al-Imam, A. Representations of psychoactive drugs’ use in mass culture and their impact on audiences. Int. J. Environ. Res. Public Health 2021, 18, 6000. [Google Scholar] [CrossRef] [PubMed]
- Borgonhi, E.M.; Volpatto, V.L.; Ornell, F.; Rabelo-da-Ponte, F.D.; Kessler, F.H.P. Multiple clinical risks for cannabis users during the COVID-19 pandemic. Addict. Sci. Clin. Pract. 2021, 16, 5. [Google Scholar] [CrossRef] [PubMed]
- Page, R.L., 2nd; Allen, L.A.; Kloner, R.A.; Carriker, C.R.; Martel, C.; Morris, A.A.; Piano, M.R.; Rana, J.S.; Saucedo, J.F.; American Heart Association Clinical Pharmacology Committee and Heart Failure and Transplantation Committee of the Council on Clinical Cardiology; et al. Medical marijuana, recreational cannabis, and cardiovascular health: A scientific statement from the american heart association. Circulation 2020, 142, e131–e152. [Google Scholar] [CrossRef] [PubMed]
- Adami, P.E.; Koutlianos, N.; Baggish, A.; Bermon, S.; Cavarretta, E.; Deligiannis, A.; Furlanello, F.; Kouidi, E.; Marques-Vidal, P.; Niebauer, J.; et al. Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: A position statement of the sport cardiology and exercise nucleus of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 559–575. [Google Scholar] [CrossRef]
- Von Der Haar, J.; Talebi, S.; Ghobadi, F.; Singh, S.; Chirurgi, R.; Rajeswari, P.; Kalantari, H.; Hassen, G.W. Synthetic cannabinoids and their effects on the cardiovascular system. J. Emerg. Med. 2016, 50, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Hancox, J.C.; Kalk, N.J.; Henderson, G. Synthetic cannabinoids and potential cardiac arrhythmia risk: An important message for drug users. Ther. Adv. Drug Saf. 2020, 11, 2042098620913416. [Google Scholar] [CrossRef]
- Cooper, Z.D. Adverse effects of synthetic cannabinoids: Management of acute toxicity and withdrawal. Curr. Psychiatry Rep. 2016, 18, 52. [Google Scholar] [CrossRef]
- Jones, J.D.; Nolan, M.L.; Daver, R.; Comer, S.D.; Paone, D. Can naloxone be used to treat synthetic cannabinoid overdose? Biol. Psychiatry 2017, 81, e51–e52. [Google Scholar] [CrossRef]
- Pryce, G.; Baker, D. Antidote to cannabinoid intoxication: The CB1 receptor inverse agonist, AM251, reverses hypothermic effects of the CB1 receptor agonist, CB-13, in mice. Br. J. Pharmacol. 2017, 174, 3790–3794. [Google Scholar] [CrossRef]
- Meredith, G.; DeLollis, M.; Shad, M.U. Potential treatment for overdose with synthetic cannabinoids. Med. Cannabis Cannabinoids 2020, 3, 74–75. [Google Scholar] [CrossRef]
- Trappe, H.J. Concept of the five ‘A’s for treating emergency arrhythmias. J. Emerg. Trauma Shock 2010, 3, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Dan, G.A.; Martinez-Rubio, A.; Agewall, S.; Boriani, G.; Borggrefe, M.; Gaita, F.; van Gelder, I.; Gorenek, B.; Kaski, J.C.; Kjeldsen, K.; et al. ESC Scientific Document Group. Antiarrhythmic drugs-clinical use and clinical decision making: A consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology (ESC) Working Group on Cardiovascular Pharmacology, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and International Society of Cardiovascular Pharmacotherapy (ISCP). Europace 2018, 20, 731–732an. [Google Scholar] [CrossRef] [PubMed]
- Dominic, P.; Ahmad, J.; Awwab, H.; Bhuiyan, M.S.; Kevil, C.G.; Goeders, N.E.; Murnane, K.S.; Patterson, J.C.; Sandau, K.E.; Gopinathannair, R.; et al. Stimulant drugs of abuse and cardiac arrhythmias. Circ. Arrhythm. Electrophysiol. 2022, 15, e010273. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.; Ojetti, V.; Migneco, A.; Serra, M.; Ancona, C.; De Lorenzo, A.; Gentiloni Silveri, N. Use of amiodarone in emergency. Eur. Rev. Med. Pharmacol. Sci. 2005, 9, 183–190. [Google Scholar] [PubMed]
- Mujović, N.; Dobrev, D.; Marinković, M.; Russo, V.; Potpara, T.S. The role of amiodarone in contemporary management of complex cardiac arrhythmias. Pharmacol. Res. 2020, 151, 104521. [Google Scholar] [CrossRef]
- Niederhoffer, N.; Szabo, B. Effect of the cannabinoid receptor agonist WIN55212-2 on sympathetic cardiovascular regulation. Br. J. Pharmacol. 1999, 126, 457–466. [Google Scholar] [CrossRef]
- Kodama, I.; Kamiya, K.; Toyama, J. Cellular electropharmacology of amiodarone. Cardiovasc. Res. 1997, 35, 13–29. [Google Scholar] [CrossRef]
- Campbell, N.; Agarwal, K.; Alidoost, M.; Miskoff, J.A.; Hossain, M. Acute fulminant hepatic failure and renal failure induced by oral amiodarone: A case report and literature review. Cureus 2020, 12, e8311. [Google Scholar] [CrossRef]
- Richards, J.R.; Bing, M.L.; Moulin, A.K.; Elder, J.W.; Rominski, R.T.; Summers, P.J.; Laurin, E.G. Cannabis use and acute coronary syndrome. Clin. Toxicol. 2019, 57, 831–841. [Google Scholar] [CrossRef]
- Yamanoglu, A.; Celebi Yamanoglu, N.G.; Evran, T.; Sogut, O. How much can synthetic cannabinoid damage the heart? A case of cardiogenic shock following resistant ventricular fibrillation after synthetic cannabinoid use. J. Clin. Ultrasound. 2018, 46, 605–609. [Google Scholar] [CrossRef]
- Sampat, P.J.; Riaz, S.; Bisen, M.; Carhart, R. An unusual case of ventricular tachycardia in a young patient associated with cannabis use. Case Rep. Cardiol. 2020, 2020, 8813930. [Google Scholar] [CrossRef] [PubMed]
- Billington, C.K.; Penn, R.B.; Hall, I.P. β2 agonists. Handb. Exp. Pharmacol. 2017, 237, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Vaillancourt, M.; Chia, P.; Sarji, S.; Nguyen, J.; Hoftman, N.; Ruffenach, G.; Eghbali, M.; Mahajan, A.; Umar, S. Autonomic nervous system involvement in pulmonary arterial hypertension. Respir. Res. 2017, 18, 201. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Nappe, T.M. Alpha receptor agonist toxicity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Manresa, F.; Dorca, J.; Rodriguez Sanchon, B.; Romero Colomer, P. Recurrent form of amiodarone-induced pneumonitis. Chest 1984, 86, 944. [Google Scholar] [CrossRef]
- Deşer, S.B.; Yücel, S.M. Management of hyperacute amiodarone-induced pulmonary toxicity. J. Cardio-Vasc.-Thorac. Anaesth. Intensive Care Soc. 2018, 24, 187–189. [Google Scholar] [CrossRef]
- Lemaire-Hurtel, A.S. Drugs involved in drug-facilitated crime—Pharmacological aspects. In Toxicological Aspects of Drug-Facilitated Crimes; Klintz, P., Ed.; Academic Press: Cambridge, MA, USA, 2014; pp. 47–49. [Google Scholar] [CrossRef]
- Coon, G.A.; Clinton, J.E.; Ruiz, E. Use of atropine for brady-asystolic prehospital cardiac arrest. Ann. Emerg. Med. 1981, 10, 462–467. [Google Scholar] [CrossRef]
- Swart, G.; Brady, W.J., Jr.; DeBehnke, D.J.; Ma, O.J.; Aufderheide, T.P. Acute myocardial infarction complicated by hemodynamically unstable bradyarrhythmia: Prehospital and ED treatment with atropine. Am. J. Emerg. Med. 1999, 17, 647–652. [Google Scholar] [CrossRef]
- Brady, W.J., Jr.; Harrigan, R.A. Diagnosis and management of bradycardia and atrioventricular block associated with acute coronary ischemia. Emerg. Med. Clin. N. Am. 2001, 19, 371–384. [Google Scholar] [CrossRef]
- Carleton, R.A.; Miller, P.H.; Graettinger, J.S. Effects of ouabain, atropine, and ouabain and atropine on A-V nodal conduction in man. Circ. Res. 1967, 20, 283–288. [Google Scholar] [CrossRef]
- Gravenstein, J.S.; Ariet, M.; Thornby, J.I. Atropine on the electrocardiogram. Clin. Pharmacol. Ther. 1969, 10, 660–666. [Google Scholar] [CrossRef]
- Lowenstein, J.; Steele, J.M., Jr. Appraisal and reappraisal of cardiac therapy: Prazosin. Am. Heart J. 1978, 95, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Ishii, M.; Kurachi, Y. Muscarinic acetylcholine receptors. Curr. Pharm. Des. 2006, 12, 3573–3581. [Google Scholar] [CrossRef] [PubMed]
- Neeld, J.B., Jr.; Allen, A.T.; Coleman, E.; Frederickson, E.L.; Goldberg, L.I. Cardiac rate and rhythm changes with atropine and methscopolamine. Clin. Pharmacol. Ther. 1975, 17, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Rosen, K.M.; Loeb, H.S.; Sinno, M.Z.; Rahimtoola, S.H.; Gunnar, R.M. Cardiac conduction in patients with symptomatic sinus node disease. Circulation 1971, 43, 836–844. [Google Scholar] [CrossRef]
- Schweitzer, P.; Mark, H. The effect of atropine on cardiac arrhythmias and conduction. Part 1. Am. Heart J. 1980, 100, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Anzillotti, L.; Marezza, F.; Calò, L.; Banchini, A.; Cecchi, R. A case report positive for synthetic cannabinoids: Are cardiovascular effects related to their protracted use? Leg. Med. 2019, 41, 101637. [Google Scholar] [CrossRef]
- Coffman, J.D.; Cohen, R.A. Cholinergic vasodilator mechanism in human fingers. Am. J. Physiol. 1987, 252 Pt 2, H594–H597. [Google Scholar] [CrossRef]
- Laitinen, L.A.; Laitinen, M.V.; Widdicombe, J.G. Parasympathetic nervous control of tracheal vascular resistance in the dog. J. Physiol. 1987, 385, 135–146. [Google Scholar] [CrossRef]
- Cabrera, E.; Levenson, J.; Armentano, R.; Barra, J.; Pichel, R.; Simon, A. Constricting and stiffening action of atropine on aortic response to angiotensin in dogs. Hypertension 1988, 11 Pt 2, I103–I107. [Google Scholar] [CrossRef]
- Abraham, S.; Cantor, E.H.; Spector, S. Studies on the hypotensive response to atropine in hypertensive rats. J. Pharmacol. Exp. Ther. 1981, 218, 662–668. [Google Scholar]
- Larson, R.A.; Chapleau, M.W. Increased cardiac sympathetic activity: Cause or compensation in vasovagal syncope? Clin. Auton. Res. 2018, 28, 265–266. [Google Scholar] [CrossRef]
- Doherty, P.A.; McCarthy, L.E.; Borison, H.L. Respiratory and cardiovascular depressant effects of nabilone, N-methyllevonantradol and delta 9-tetrahydrocannabinol in anesthetized cats. J. Pharmacol. Exp. Ther. 1983, 227, 508–516. [Google Scholar]
- Richardson, C.A.; Herbert, D.A.; Mitchell, R.A. Modulation of pulmonary stretch receptors and airway resistance by parasympathetic efferents. J. Appl Physiol. Respir. Environ. Exerc. Physiol. 1984, 57, 1842–1849. [Google Scholar] [CrossRef]
- Stewart, H.J. The effect of increased heart rate due to the injection of atropine on the oxygen saturation of the arterial and venous blood of patients with heart disease. J. Clin. Investig. 1926, 3, 241–251. [Google Scholar] [CrossRef]
- Khan, K.M.; Patel, J.; Schaefer, T.J. Nifedipine. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ralevic, V.; Kendall, D.A. Cannabinoid modulation of perivascular sympathetic and sensory neurotransmission. Curr. Vasc. Pharmacol. 2009, 7, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Dean, C. Cannabinoid and GABA modulation of sympathetic nerve activity and blood pressure in the dorsal periaqueductal gray of the rat. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 301, R1765–R1772. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.D. Does Tail-cuff plethysmography provide a reliable estimate of central blood pressure in mice? J. Am. Heart Assoc. 2017, 6, e006554. [Google Scholar] [CrossRef]
- Pogwizd, S.M.; Schlotthauer, K.; Li, L.; Yuan, W.; Bers, D.M. Arrhythmogenesis and contractile dysfunction in heart failure: Roles of sodium-calcium exchange, inward rectifier potassium current, and residual beta-adrenergic responsiveness. Circ. Res. 2001, 88, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Bers, D.M. Cardiac excitation-contraction coupling. Nature 2002, 415, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.L.; Binger, C.A. The response to respiratory resistance: A comparison of the effects produced by partial obstruction in the inspiratory and expiratory phases of respiration. J. Exp. Med. 1927, 45, 1065–1080. [Google Scholar] [CrossRef]
- Fanta, C.H.; Watson, J.W.; Lacouture, P.G.; Drazen, J.M. In vivo bronchodilator activity of nifedipine in the guinea pig. Am. Rev. Respir. Dis. 1987, 136, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Flores-Soto, E.; Reyes-García, J.; Sommer, B.; Montaño, L.M. Sarcoplasmic reticulum Ca(2+) refilling is determined by L-type Ca(2+) and store operated Ca(2+) channels in guinea pig airway smooth muscle. Eur. J. Pharmacol. 2013, 721, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Rubini, A.; Catena, V.; Del Monte, D.; Bosco, G. The effects of nifedipine on respiratory mechanics investigated by theend-inflation occlusion method in the rat. J. Enzyme Inhib. Med. Chem. 2017, 32, 1–4. [Google Scholar] [CrossRef]
- Watanabe, K.; Kimura, Y.; Abiko, Y. Nifedipine increases oxygen saturation level of myoglobin in the rat heart during hypoxia. Arch. Int. Pharmacodyn. Ther. 1986, 284, 297–312. [Google Scholar] [PubMed]
- Al-Majed, A.A.; Bakheit, A.H.H.; Abdel Aziz, H.A.; Alajmi, F.M.; AlRabiah, H. Propranolol. Profiles Drug Subst. Excip. Relat. Methodol. 2017, 42, 287–338. [Google Scholar] [CrossRef] [PubMed]
- Vaile, J.C.; Fletcher, J.; Al-Ani, M.; Ross, H.F.; Littler, W.A.; Coote, J.H.; Townend, J.N. Use of opposing reflex stimuli and heart rate variability to examine the effects of lipophilic and hydrophilic beta-blockers on human cardiac vagal control. Clin. Sci. 1999, 97, 585–593. [Google Scholar] [CrossRef]
- Randall, M.D.; Harris, D.; Kendall, D.A.; Ralevic, V. Cardiovascular effects of cannabinoids. Pharmacol. Ther. 2002, 95, 191–202. [Google Scholar] [CrossRef]
- Santosh, P.J.; Bell, L.; Lievesley, K.; Singh, J.; Fiori, F. Paradoxical physiological responses to propranolol in a Rett syndrome patient: A case report. BMC Pediatr. 2016, 16, 194. [Google Scholar] [CrossRef]
- Harrison, D.C.; Griffin, J.R.; Fiene, T.J. Effects of beta-adrenergic blockade with propranolol in patients with atrial arrhythmias. N. Engl. J. Med. 1965, 273, 410–415. [Google Scholar] [CrossRef]
- Zilm, D.H.; Jacob, M.S.; MacLeod, S.M.; Sellers, E.M.; Ti, T.Y. Propranolol and chlordiazepoxide effects on cardiac arrhythmias during alcohol withdrawal. Alcohol. Clin. Exp. Res. 1980, 4, 400–405. [Google Scholar] [CrossRef]
- Morganroth, J.; Horowitz, L.N.; Anderson, J.; Turlapaty, P. Comparative efficacy and tolerance of esmolol to propranolol for control of supraventricular tachyarrhythmia. Am. J. Cardiol. 1985, 56, 33F–39F. [Google Scholar] [CrossRef]
- Kubik, M.M.; Gill, B.; Dawes, P.M. Propranolol in cardiac arrhythmias: A comparative study of the conventional and long-acting formulations. Curr. Med. Res. Opin. 1986, 10, 215–220. [Google Scholar] [CrossRef]
- Bhagat, B.D. Mechanism of the antihypertensive effect of propranolol. Gen. Pharmacol. 1979, 10, 291–296. [Google Scholar] [CrossRef]
- Karnani, N.G.; Reisfield, G.M.; Wilson, G.R. Evaluation of chronic dyspnea. Am. Fam. Physician 2005, 71, 1529–1537. [Google Scholar] [PubMed]
- Kupper, N.; Bonhof, C.; Westerhuis, B.; Widdershoven, J.; Denollet, J. Determinants of dyspnea in chronic heart failure. J. Card. Fail. 2016, 22, 201–209. [Google Scholar] [CrossRef]
- Antonelli-Incalzi, R.; Pedone, C. Respiratory effects of beta-adrenergic receptor blockers. Curr. Med. Chem. 2007, 14, 1121–1128. [Google Scholar] [CrossRef]
- Khambatta, H.J.; Stone, J.G.; Askanazi, J.; Khan, E. Propranolol increases oxygen utilization during hypoxia. Br. J. Anaesth. 1987, 59, 1171–1176. [Google Scholar] [CrossRef]
- Narkiewicz, K.; Kjeldsen, S.E.; Oparil, S.; Hedner, T. Beta-blockers as sub-optimal treatment for hypertension: Time for first-line therapy revision? Blood Press. 2006, 15, 323–324. [Google Scholar] [CrossRef] [PubMed]
- DAWN. The DAWN. Report: Drug-Related Emergency Department Visits Involving Synthetic Cannabinoids; Substance Abuse and Mental Health Services Administration (SAMHSA), Center for Behavioral Health Statistics and Quality: Rockville, MD, USA, 2012. [Google Scholar]
- Fogel, J.S.; Kelly, T.H.; Westgate, P.M.; Lile, J.A. Sex differences in the subjective effects of oral Δ9-THC in cannabis users. Pharmacol. Biochem. Behav. 2017, 152, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Nia, A.B.; Mann, C.; Kaur, H.; Ranganathan, M. Cannabis use: Neurobiological, behavioral, and sex/gender considerations. Curr. Behav. Neurosci. Rep. 2018, 5, 271–280. [Google Scholar] [PubMed]
- Wiley, J.L.; Walentiny, D.M.; Wright, M.J., Jr.; Beardsley, P.M.; Burston, J.J.; Poklis, J.L.; Lichtman, A.H.; Vann, R.E. Endocannabinoid contribution to Δ9-tetrahydrocannabinol discrimination in rodents. Eur. J. Pharmacol. 2014, 737, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Wiley, J.L.; Lefever, T.W.; Marusich, J.A.; Craft, R.M. Comparison of the discriminative stimulus and response rate effects of Δ9-tetrahydrocannabinol and synthetic cannabinoids in female and male rats. Drug Alcohol. Depend. 2017, 172, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Jouanjus, E.; Raymond, V.; Lapeyre-Mestre, M.; Wolff, V. What is the current knowledge about the cardiovascular risk for users of cannabis-based products? A Systematic Review. Curr. Atheroscler. Rep. 2017, 19, 26. [Google Scholar] [CrossRef]
- Zuurman, L.; Ippel, A.E.; Moin, E.; van Gerven, J.M. Biomarkers for the effects of cannabis and THC in healthy volunteers. Br. J. Clin. Pharmacol. 2009, 67, 5–21. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. Statistical power analysis for the behavioral sciences. SAGE Encycl. Res. Des. 1969, 26, 588. [Google Scholar] [CrossRef]
- Weinstein, A.M.; Rosca, P.; Fattore, L.; London, E.D. Synthetic cathinone and cannabinoid designer drugs pose a major risk for public health. Front. Psychiatry 2017, 8, 156. [Google Scholar] [CrossRef]
- Reagan-Shaw, S.; Nihal, M.; Ahmad, N. Dose translation from animal to human studies revisited. FASEB J. 2008, 22, 659–661. [Google Scholar] [CrossRef]
- Psychonautwiki. JWH-018. Available online: https://psychonautwiki.org/wiki/JWH-018 (accessed on 12 January 2023).
- Riva, E.; Hearse, D.J. Anti-arrhythmic effects of amiodarone and desethylamiodarone on malignant ventricular arrhythmias arising as a consequence of ischaemia and reperfusion in the anaesthetised rat. Cardiovasc. Res. 1989, 23, 331–339. [Google Scholar] [CrossRef]
- Vulliemoz, Y.; Verosky, M. Effect of clonidine on myocardial cyclic GMP content of clonidine in the mouse-activation of central and peripheral alpha adrenoceptors. J. Pharmacol. Exp. Ther. 1989, 251, 884–887. [Google Scholar]
- Pozsgai, G.; Bodkin, J.V.; Graepel, R.; Bevan, S.; Andersson, D.A.; Brain, S.D. Evidence for the phatophysiological relevance of TRPA1 receptors in the cardiovascular system in vivo. Cardiovas. Res. 2010, 87, 760–768. [Google Scholar] [CrossRef]
- Altamirano, F.; Valladares, D.; Henríquez-Olguín, C.; Casas, M.; López, J.R.; Allen, P.D.; Jaimovich, E. Nifedipine treatment reduces resting calcium concentration, oxidative and apoptotic gene expression, and improves muscle function in dystrophic mdx mice. PLoS ONE 2013, 8, e81222. [Google Scholar] [CrossRef]
- Deten, A.; Volz, H.C.; Holzl, A.; Briest, W.; Zimmer, H.G. Effect of propranolol on cardiac cytokine expression after myocardial infarction in rats. Mol. Cell Biochem. 2003, 251, 127–137. [Google Scholar] [CrossRef]
- Ossato, A.; Bilel, S.; Gregori, A.; Talarico, A.; Trapella, C.; Gaudio, R.M.; De-Giorgio, F.; Tagliaro, F.; Neri, M.; Fattore, L.; et al. Neurological, sensorimotor and cardiorespiratory alterations induced by methoxetamine, ketamine and phencyclidine in mice. Neuropharmacology 2018, 141, 167–180. [Google Scholar] [CrossRef]
- Foti, F.; Marti, M.; Ossato, A.; Bilel, S.; Sangiorgi, E.; Botrè, F.; Cerbelli, B.; Baldi, A.; De-Giorgio, F. Phenotypic effects of chronic and acute use of methiopropamine in a mouse model. Int. J. Leg. Med. 2019, 133, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Bilel, S.; Tirri, M.; Arfè, R.; Sturaro, C.; Fantinati, A.; Cristofori, V.; Bernardi, T.; Boccuto, F.; Cavallo, M.; Cavalli, A.; et al. In vitro and in vivo pharmaco-toxicological characterization of 1-cyclohexyl-x-methoxybenzene derivatives in mice: Comparison with tramadol and PCP. Int. J. Mol. Sci. 2021, 22, 7659. [Google Scholar] [CrossRef] [PubMed]
- Bilel, S.; Azevedo Neto, J.; Arfè, R.; Tirri, M.; Gaudio, R.M.; Fantinati, A.; Bernardi, T.; Boccuto, F.; Marchetti, B.; Corli, G.; et al. In vitro and in vivo pharmaco-dynamic study of the novel fentanyl derivatives: Acrylfentanyl, Ocfentanyl and Furanylfentanyl. Neuropharmacology 2022, 209, 109020. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchetti, B.; Bilel, S.; Tirri, M.; Corli, G.; Roda, E.; Locatelli, C.A.; Cavarretta, E.; De-Giorgio, F.; Marti, M. Acute Cardiovascular and Cardiorespiratory Effects of JWH-018 in Awake and Freely Moving Mice: Mechanism of Action and Possible Antidotal Interventions? Int. J. Mol. Sci. 2023, 24, 7515. https://doi.org/10.3390/ijms24087515
Marchetti B, Bilel S, Tirri M, Corli G, Roda E, Locatelli CA, Cavarretta E, De-Giorgio F, Marti M. Acute Cardiovascular and Cardiorespiratory Effects of JWH-018 in Awake and Freely Moving Mice: Mechanism of Action and Possible Antidotal Interventions? International Journal of Molecular Sciences. 2023; 24(8):7515. https://doi.org/10.3390/ijms24087515
Chicago/Turabian StyleMarchetti, Beatrice, Sabrine Bilel, Micaela Tirri, Giorgia Corli, Elisa Roda, Carlo Alessandro Locatelli, Elena Cavarretta, Fabio De-Giorgio, and Matteo Marti. 2023. "Acute Cardiovascular and Cardiorespiratory Effects of JWH-018 in Awake and Freely Moving Mice: Mechanism of Action and Possible Antidotal Interventions?" International Journal of Molecular Sciences 24, no. 8: 7515. https://doi.org/10.3390/ijms24087515
APA StyleMarchetti, B., Bilel, S., Tirri, M., Corli, G., Roda, E., Locatelli, C. A., Cavarretta, E., De-Giorgio, F., & Marti, M. (2023). Acute Cardiovascular and Cardiorespiratory Effects of JWH-018 in Awake and Freely Moving Mice: Mechanism of Action and Possible Antidotal Interventions? International Journal of Molecular Sciences, 24(8), 7515. https://doi.org/10.3390/ijms24087515