
Exploring Potential Biomarkers in Oesophageal Cancer: A Comprehensive Analysis




Abstract
:1. Introduction
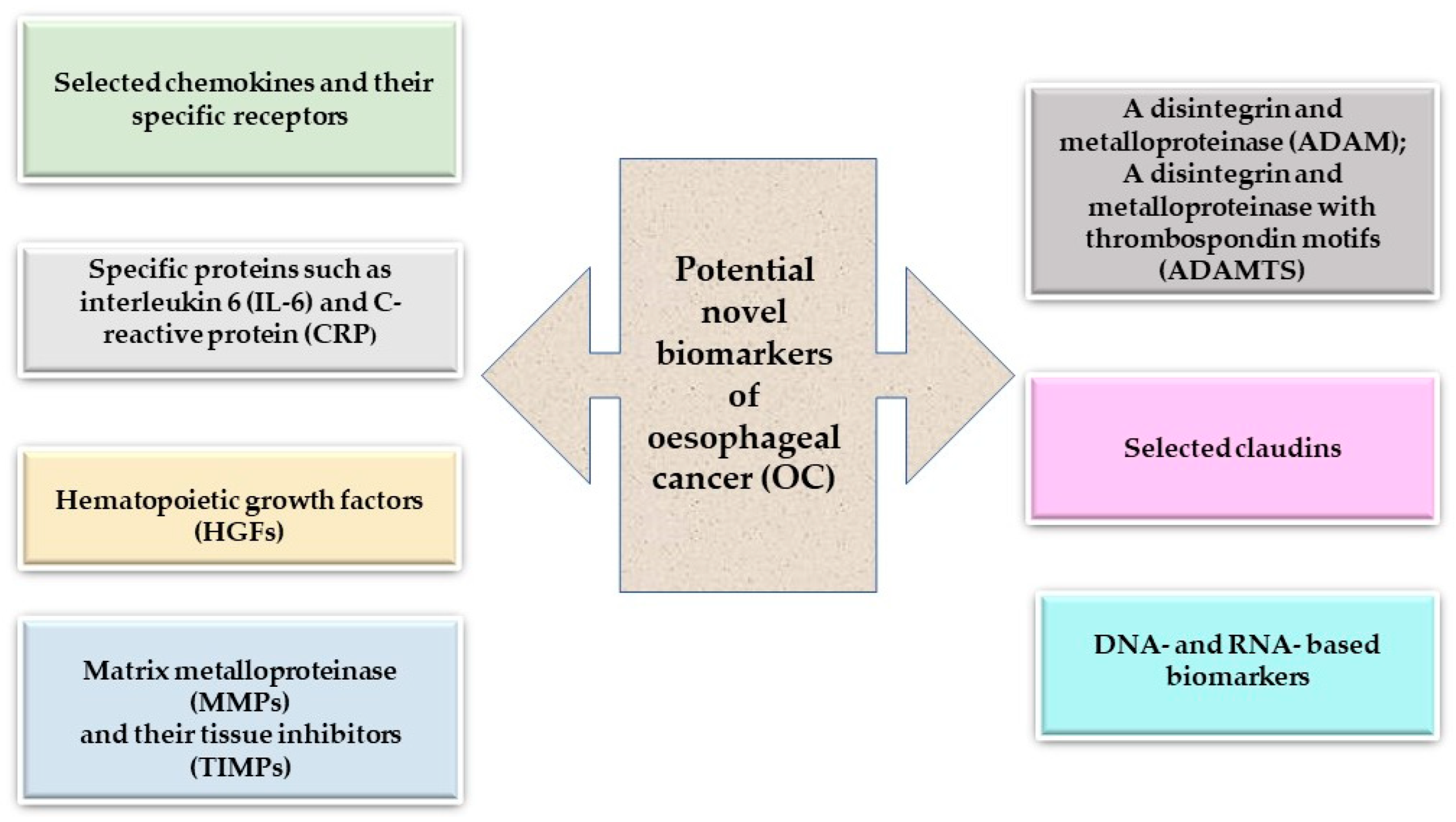
2. Specific Proteins as Potential Biomarkers of Oesophageal Cancer
2.1. Chemokines and Their Specific Receptors
2.2. Interleukin-6 (IL-6) and C-Reactive Protein (CRP)
2.3. Hematopoietic Growth Factors (HGFs)
2.4. Matrix Metalloproteinases (MMPs) and Their Tissue Inhibitors (TIMPs)
A Disintegrin and Metalloproteinase (ADAMs) Family
2.5. Claudins (CLDNs)
3. Molecular Biomarkers of Oesophageal Cancer (OC)
3.1. DNA-Based Biomarkers
3.2. RNA-Based Biomarkers
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lagergren, J.; Smyth, E.; Cunningham, D.; Lagergren, P. Ooesophageal Cancer. Lancet 2017, 390, 2383–2396. [Google Scholar] [CrossRef] [PubMed]
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of Oesophageal Cancer: Update in Global Trends, Etiology and Risk Factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef]
- Corley, D.A.; Kubo, A.; Levin, T.R.; Block, G.; Habel, L.; Rumore, G.; Quesenberry, C.; Buffler, P. Race, ethnicity, sex and temporal differences in Barrett’s oesophagus diagnosis: A large community-based study, 1994–2006. Gut 2009, 58, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, J.H.; Inadomi, J.M.; Scheiman, J.; Schoenfeld, P.; Appelman, H.; Zhang, M.; Metko, V.; Kao, J.Y. Association between Helicobacter pylori and Barrett’s esophagus, erosive esophagitis, and gastrooesophageal reflux symptoms. Clin. Gastroenterol. Hepatol. 2014, 12, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, M.; Roshandel, G.; McCormack, V.; Malekzadeh, G. Current Status and Future Prospects for Oesophageal Cancer. Cancers 2023, 15, 765. [Google Scholar] [CrossRef] [PubMed]
- Ellis, A.; Risk, J.M.; Maruthappu, T.; Kelsell, D.P. Tylosis with oesophageal cancer: Diagnosis, management and molecular mechanisms. Orphanet J. Rare Dis. 2015, 29, 126. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Oesophageal Cancer Collaborators. The global, regional, and national burden of ooesophageal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. 2020, 5, 582–597. [Google Scholar] [CrossRef]
- Daly, J.M.; Fry, W.A.; Little, A.G.; Winchester, D.P.; McKee, R.F.; Stewart, A.K.; Fremgen, A.M. Oesophageal cancer: Results of an American College of Surgeons patient care evaluation study. J. Am. Coll. Surg. 2000, 190, 562–572. [Google Scholar] [CrossRef]
- Enzinger, P.C.; Mayer, R.J. Oesophageal cancer. N. Engl. J. Med. 2003, 349, 2241–2252. [Google Scholar] [CrossRef]
- Thakkar, S.; Kaul, V. Endoscopic Ultrasound Staging of Oesophageal Cancer. Gastroenterol. Hepatol. 2020, 16, 14–20. [Google Scholar]
- Tan, C.; Qian, X.; Guan, Z.; Yang, B.; Ge, Y.; Wang, F.; Ca, J. Potential biomarkers for oesophageal cancer. Springerplus 2016, 5, 467. [Google Scholar] [CrossRef] [PubMed]
- Moody, S.; Senkin, S.; Islam, S.M.A.; Wang, J.; Nasrollahzadeh, D.; Penha, C.C.R.; Fitzgerald, S.; Bergstrom, E.N.; Atkins, J.; He, Y.; et al. Mutational Signatures in Oesophageal Squamous Cell Carcinoma from Eight Countries with Varying Incidence. Nat. Genet. 2021, 53, 1553–1563. [Google Scholar] [CrossRef] [PubMed]
- Secrier, M.; Li, X.; de Silva, N.; Eldridge, M.D.; Contino, G.; Bornschein, J.; MacRae, S.; Grehan, N.; O’Donovan, M.; Miremadi, A.; et al. Mutational Signatures in Oesophageal Adenocarcinoma Define Etiologically Distinct Subgroups with Therapeutic Relevance. Nat. Genet. 2016, 48, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Rogers, J.E.; Iwatsuki, M.; Yamashita, K.; Baba, H.; Ajani, J.A. Recent Advances in Treating Oesophageal Cancer. F1000Research 2020, 9, 1189. [Google Scholar] [CrossRef] [PubMed]
- Valiullina, A.K.; Zmievskaya, E.A.; Ganeeva, I.A.; Zhuravleva, M.N.; Garanina, E.E.; Rizvanov, A.A.; Petukhov, A.V.; Bulatov, E.R. Evaluation of CAR-T Cells’ Cytotoxicity against Modified Solid Tumor Cell Lines. Biomedicines 2023, 11, 626. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Nikliński, J.; Laudański, J.; Szmitkowski, M. Higher importance of interleukin 6 than classic tumor markers (carcinoembryonic antigen and squamous cell cancer antigen) in the diagnosis of oesophageal cancer patients. Dis. Esophagus 2012, 25, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Chela, H.K.; Gangu, K.; Ertugrul, H.; Juboori, A.A.; Daglilar, E.; Tahan, V. The 8th Wonder of the Cancer World: Oesophageal Cancer and Inflammation. Diseases 2022, 10, 44. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Vindrieux, D.; Escobar, P.; Lazenn, O.C.G. Emerging roles of chemokines in prostate cancer. Endocr. Relat. Cancer 2009, 16, 663–673. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Coussens, L.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- de Visser, K.E.; Eichten, A.; Coussens, L.M. Paradoxical roles of the immune system during cancer development. Nat. Rev. Cancer 2006, 6, 24–37. [Google Scholar] [CrossRef]
- Fagoonee, S.; Li, H.; Zhang, H.; Altruda, F.; Pellicano, R. Gastric cancer as a stem-cell disease: Data and hypotheses. Panminerva Med. 2014, 56, 289–300. [Google Scholar] [PubMed]
- Ozga, A.J.; Chow, M.T.; Luster, A.D. Chemokines and the immune response to cancer. Immunity 2021, 54, 859–874. [Google Scholar] [CrossRef] [PubMed]
- Kaifi, J.T.; Yekebas, E.F.; Schurr, P.; Obonyo, D.; Wachowiak, R.; Busch, P.; Heinecke, A.; Pantel, K.; Izbicki, J.R. Tumor-cell homing to lymph nodes and bone marrow and cxcr4 expression in esophageal cancer. J. Natl. Cancer Inst. 2005, 97, 1840–1847. [Google Scholar] [CrossRef]
- Wang, D.F.; Lou, N.; Zeng, C.G.; Zhang, X.; Chen, F.J. Expression of cxcl12/cxcr4 and its correlation to prognosis in esophageal squamous cell carcinoma. Chin. J. Cancer 2009, 28, 154–158. [Google Scholar]
- Lu, C.L.; Ji, Y.; Ge, D.; Guo, J.; Ding, J.Y. The expression of cxcr4 and its relationship with matrix metalloproteinase-9/vascular endothelial growth factor in esophageal squamous cell cancer. Dis. Esophagus 2011, 24, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Ogura, M.; Takeuchi, H.; Kawakubo, H.; Nishi, T.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Saikawa, Y.; Omori, T.; et al. Clinical significance of cxcl-8/cxcr-2 network in oesophageal squamous cell carcinoma. Surgery 2013, 154, 512–520. [Google Scholar] [CrossRef]
- Łukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Nikliński, J.; Laudański, J.; Siewko, M.; Szmitkowski, M. Comparative Evaluation of Serum C-Reactive Protein (CRP) Levels in the Different Histological Subtypes of Esophageal Cancer (Squamous Cell Carcinoma and Adenocarcinoma of Esophagus). J. Clin. Lab. Anal. 2012, 26, 73–81. [Google Scholar] [CrossRef]
- Łukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Szmitkowski, M. Stem cell factor in the serum of patients with oesophageal cancer in relation to its histological types. Arch. Med. Sci. 2017, 13, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Nikliński, J.; Laudański, J.; Szmitkowski, M. Clinical significance of serum macrophage-colony stimulating factor (M-CSF) in oesophageal cancer patients and its comparison with classical tumor markers. Clin. Chem. Lab. Med. 2010, 48, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ma, L.; Guo, L.; Duan, F.; Tang, F.; Zheng, P.; Zhao, Z.; Lu, G. Overexpression of MMP-2 and MMP-9 in oesophageal squamous cell carcinoma. Dis. Esophagus 2009, 22, 664–667. [Google Scholar] [CrossRef]
- Murray, G.I.; Duncan, M.E.; O’Neil, P.; McKay, J.A.; Melvin, W.T.; Fothergill, J.E. Matrix metalloproteinase-1 is associated with poor prognosis in ooesophageal cancer. J. Pathol. 1998, 185, 256–261. [Google Scholar] [CrossRef]
- Sharma, R.; Chattopadhyay, T.K.; Mathur, M.; Ralhan, R. Prognostic significance of stromelysin-3 and tissue inhibitor of matrix metal-loproteinase-2 in oesophageal cancer. Oncology 2004, 67, 300–309. [Google Scholar] [CrossRef]
- Lin, Y.S.; Kuo, T.T.; Lo, C.C.; Cheng, W.C.; Chang, W.C.; Tseng, G.C. ADAM9 functions as a transcriptional regulator to drive angiogenesis in oesophageal squamous cell carcinoma. Int. J. Biol. Sci. 2021, 17, 3898–3910. [Google Scholar] [CrossRef]
- Liu, L.; Yang, Z.; Ni, W.; Xuan, Y. ADAMTS-6 is a predictor of poor prognosis in patients with oesophageal squamous cell carcinoma. Exp. Mol. Pathol. 2018, 104, 134–139. [Google Scholar] [CrossRef]
- Usami, Y.; Chiba, H.; Nakayama, F.; Ueda, J.; Matsuda, Y.; Sawada, N.; Komori, T.; Ito, A.; Yokozaki, H. Reduced expression of claudin-7 correlates with invasion and metastasis in squamous cell carcinoma of the esophagus. Hum. Pathol. 2006, 37, 569–577. [Google Scholar] [CrossRef]
- Gomez, D.E.; Alonso, D.F.; Yoshiji, H.; Thorgeirsson, U.P. Tissue inhibitors of metalloproteinases: Structure, regulation and biological functions. Eur. J. Cell Biol. 1997, 74, 111–122. [Google Scholar]
- Chen, M.F.; Chen, P.T.; Lu, M.S.; Lin, P.Y.; Chen, W.C.; Lee, K.D. IL-6 expression predicts treatment response and outcome in squamous cell carcinoma of the esophagus. Mol. Cancer 2013, 12, 26. [Google Scholar] [CrossRef]
- Huang, Y.; Feng, J.F.; Liu, J.S.; Chen, Q.X. Prognostic role of serum C-reactive protein in oesophageal cancer: A systematic review and meta-analysis. Ther. Clin. Risk Manag. 2015, 11, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Szmitkowski, M. The Serum Concentrations of Chemokine CXCL12 and Its Specific Receptor CXCR4 in Patients with Oesophageal Cancer. Dis. Markers 2016, 2016, 7963895. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewicz-Zając, M.; Pączek, S.; Muszyński, P.; Kozłowski, M.; Mroczko, B. Comparison between clinical significance of serum CXCL8 and classical tumor markers in oesophageal cancer (OC) patients. Clin. Exp. Med. 2019, 19, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Łukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Nikliński, J.; Laudański, J.; Szmitkowski, M. Elevated levels of serum metalloproteinase 9 in patients with oesophageal squamous cell carcinoma. Pol. Arch. Med. Wewn. 2009, 119, 558–563. [Google Scholar] [PubMed]
- Moentenich, V.; Gebauer, F.; Comut, E.; Tuchscherer, A.; Bruns, C.; Schroeder, W.; Buettner, R.; Alakus, H.; Loeser, H.; Zander, T.; et al. Claudin 18.2 expression in oesophageal adenocarcinoma and its potential impact on future treatment strategies. Oncol. Lett. 2020, 19, 3665–3670. [Google Scholar] [PubMed]
- Miller, M.C.; Mayo, K.H. Chemokines from a structural perspective. Int. J. Mol. Sci. 2017, 18, 2088. [Google Scholar] [CrossRef] [PubMed]
- Zlotnik, A.; Burkhardt, A.M.; Homey, B. Homeostatic chemokine receptors and organ-specific metastasis. Nat. Rev. Immunol. 2011, 11, 597–606. [Google Scholar] [CrossRef]
- Zlotnik, A.; Yoshie, O. The chemokine superfamily revisited. Immunity 2012, 36, 705–716. [Google Scholar] [CrossRef]
- Mehrad, B.; Keane, M.P.; Strieter, R.M. Chemokines as mediators of angiogenesis. Thromb. Haemost. 2007, 97, 755–762. [Google Scholar] [CrossRef]
- Goto, M.; Liu, M. Chemokines and their receptors as biomarkers in oesophageal cancer. Esophagus 2020, 17, 113–121. [Google Scholar] [CrossRef]
- Niess, J.H.; Brand, S.; Gu, X.; Landsman, L.; Jung, S.; McCormick, B.A.; Vyas, J.M.; Boes, M.; Ploegh, H.L.; Fox, G.J.; et al. CX3CR1-mediated dendritic cell access to the intestinal lumen and bacterial clearance. Science 2005, 307, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Natsugoe, S.; Ishigami, S.; Matsumoto, M.; Okumura, H.; Setoyama, T.; Uchikado, Y.; Kita, Y.; Tamotsu, K.; Hanazono, K.; et al. Expression of CXCL12 and its receptor CXCR4 in oesophageal squamous cell carcinoma. Oncol. Rep. 2009, 21, 65–71. [Google Scholar] [PubMed]
- Łukaszewicz-Zając, M.; Mroczko, B.; Szmitkowski, M. Chemokines and their receptors in oesophageal cancer-the systematic review and future perspectives. Tumor Biol. 2015, 36, 5707–5714. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Matusiewicz, M.; Diakowska, D.; Grabowski, K.; Blachut, K.; Konieczny, D.; Kustrzeba-Wojcicka, I.; Terlecki, G.; Banas, T. Elevation of circulating interleukin-8 is related to lymph node and distant metastases in esophageal squamous cell carcinomas—Implication for clinical evaluation of cancer patient. Cytokine 2008, 41, 232–239. [Google Scholar] [CrossRef]
- Gockel, I.; Schimanski, C.C.; Heinrich, C.; Wehler, T.; Frerichs, K.; Drescher, D.; von Langsdorff, C.; Domeyer, M.; Biesterfeld, S.; Galle, P.R.; et al. Expression of chemokine receptor cxcr4 in esophageal squamous cell and adenocarcinoma. BMC Cancer 2006, 6, 290. [Google Scholar] [CrossRef] [PubMed]
- Signoret, N.; Hewlett, L.; Wavre, S.; Pelchen-Matthews, A.; Oppermann, M.; Marsh, M. Agonist-induced endocytosis of CC chemokine receptor 5 is clathrin dependent. Mol. Biol. Cell. 2005, 16, 902–917. [Google Scholar] [CrossRef] [PubMed]
- Menten, P.; Wuyts, A.; Van Damme, J. Macrophage inflammatory protein-1. Cytokine Growth Factor Rev. 2002, 13, 455–481. [Google Scholar] [CrossRef]
- Wu, Y.C.; Shen, Y.C.; Chang, J.W.C.; Hsieh, J.J.; Chu, Y.; Wang, C.H. Autocrine CCL5 promotes tumor progression in esophageal squamous cell carcinoma in vitro. Cytokine 2018, 110, 94–103. [Google Scholar] [CrossRef]
- Dunbar, K.J.; Karakasheva, T.A.; Tang, Q.; Efe, G.; Lin, E.W.; Harris, M.; Sahu, V.; Sachdeva, U.M.; Hu, J.; Klein-Szanto, A.J.; et al. Tumor-Derived CCL5 Recruits Cancer-Associated Fibroblasts and Promotes Tumor Cell Proliferation in Esophageal Squamous Cell Carcinoma. Mol. Cancer Res. 2023, 21, 741–752. [Google Scholar] [CrossRef]
- Waugh, D.J.; Wilson, C. The interleukin-8 pathway in cancer. Clin. Cancer Res. 2008, 14, 6735–6741. [Google Scholar] [CrossRef]
- Shrivastava, M.S.; Hussain, Z.; Giricz, O.; Shenoy, N.; Polineni, R.; Maitra, A.; Verma, A. Targeting chemokine pathways in oesophageal adenocarcinoma. Cell Cycle 2014, 13, 3320–3327. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.H.; Schetter, A.J.; Chou, D.B.; Bowman, E.D.; Zhao, R.; Hawkes, J.E.; Mathe, E.A.; Kumamoto, K.; Zhao, Y.; Budhu, A.; et al. Inflammatory and microRNA gene expression as prognostic classifiers of Barrett’s associated oesophageal adenocarcinoma. Clin. Cancer Res. 2010, 16, 5824–5834. [Google Scholar] [CrossRef]
- Chen, C.C.; Chen, W.C.; Lu, C.H.; Wang, W.H.; Lin, P.Y.; Lee, K.D.; Chen, M.F. Significance of interleukin-6 signaling in the resistance of pharyngeal cancer to irradiation and the epidermal growth factor receptor inhibitor. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 1214–1224. [Google Scholar] [CrossRef] [PubMed]
- Santer, F.R.; Malinowska, K.; Culig, Z.; Cavarretta, I.T. Interleukin-6 trans-signalling differentially regulates proliferation, migration, adhesion and maspin expression in human prostate cancer cells. Endocr. Relat. Cancer 2010, 17, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xu, F.; Lu, T.; Duan, Z.; Zhang, Z. Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat. Rev. 2012, 38, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Hsieh, M.J.; Chiu, Y.C.; Li, S.H.; Huang, H.W.; Fang, F.M.; Huang, Y.J. Higher serum C-reactive protein concentration and hypoalbuminemia are poor prognostic indicators in patients with oesophageal cancer undergoing radiotherapy. Radiother. Oncol. 2009, 92, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Oka, M.; Iizuka, N.; Yamamoto, K.; Gondo, T.; Abe, T.; Hazama, S.; Akitomi, Y.; Koishihara, Y.; Ohsugi, Y.; Ooba, Y.; et al. The influence of interleukin-6 on the growth of human oesophageal cancer cell lines. J. Interferon Cytokine Res. 1996, 16, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.S.; Sun, C.F. C-reactive protein and malignancy: Clinico-pathological association and therapeutic implication. Chang Gung Med. J. 2009, 32, 471–482. [Google Scholar] [PubMed]
- Oka, M.; Yamamoto, K.; Takahashi, M.; Hakozaki, M.; Abe, T.; Iizuka, N.; Hazama, S.; Hirazawa, K.; Hayashi, H.; Tangoku, A.; et al. Relationship between serum levels of interleukin 6, various disease parameters and malnutrition in patients with oesophageal squamous cell carcinoma. Cancer Res. 1996, 56, 2776–2780. [Google Scholar]
- McDermott, R.S.; Deneux, L.; Mosseri, V.; Védrenne, J.; Clough, K.; Fourquet, A.; Rodriguez, J.; Cosset, J.-M.; Sastre, X.; Beuzeboc, P.; et al. Circulating macrophage colony stimulating factor as a marker of tumour progression. Eur. Cytokine Netw. 2002, 13, 121–127. [Google Scholar]
- Dunlop, R.J.; Campbell, C.W. Cytokines and advanced cancer. J. Pain Symptom Manag. 2000, 20, 214–232. [Google Scholar] [CrossRef] [PubMed]
- Oka, M.; Hirose, K.; Iizuka, N.; Aoyagi, K.; Yamamoto, K.; Abe, T.; Hazama, S.; Suzuki, T. Cytokine mRNA expression patterns in human esophageal cancer cell lines. J. Interferon Cytokine Res. 1995, 15, 1005–1009. [Google Scholar] [CrossRef] [PubMed]
- Rebernick, R.J.; Bell, H.N.; Bauer, T.M.; McEwen, D.; Werkman, D.F.; Chang, A.C.; Lin, J.; Reddy, R.M.; Kresty, L.; Lagisetty, K. Role of IL4 and GMCSF in Predicting Survival in Oesophageal Cancer. J. Am. Coll. Surg. 2023, 236, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Srivastava, S.K.; Chaudhuri, T.K.; Upadhyay, G. Multifaceted role of matrix metalloproteinases (MMPs). Front. Mol. Biosci. 2015, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Shim, K.N.; Jung, S.A.; Joo, Y.H.; Yoo, K. Clinical significance of tissue levels of matrix metalloproteinases and tissue inhibitors of metalloproteinases in gastric cancer. J. Gastroenterol. 2007, 42, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Groblewska, M.; Siewko, M.; Mroczko, B.; Szmitkowski, M. The role of matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) in the development of oesophageal cancer. Folia Histochem. Cytobiol. 2012, 50, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Di, D.; Luo, G.; Zheng, L.; Tan, Y.; Zhang, X.; Xu, N. Immunochemical Staining of MT2-MMP Correlates Positively to Angiogenesis of Human Esophageal Cancer. Anticancer Res. 2010, 30, 4363–4368. [Google Scholar] [PubMed]
- El-Shahat, M.; Lotfy, M.; Fahmy, L.; Abouel-Nour, M.F.; El-Kenawy Ael, M. Prognostic value of microvessel density, matrix metalloproteinase-9 and p53 protein expression in oesophageal cancer. J. Egypt Natl. Cancer Inst. 2004, 16, 224–230. [Google Scholar]
- van Goor, H.; Melenhorst, W.B.; Turner, A.J.; Holgate, S.T. Adamalysins in biology and disease. J. Pathol. 2009, 219, 277–286. [Google Scholar] [CrossRef]
- Gilpin, B.J.; Loechel, F.; Mattei, M.G.; Engvall, E.; Albrechtsen, R.; Wewer, U.M. A novel, secreted form of human ADAM 12 (meltrin alpha) provokes myogenesis in vivo. J. Biol. Chem. 1998, 273, 157–166. [Google Scholar] [CrossRef]
- White, J.M. ADAMs: Modulators of cell-cell and cell-matrix interactions. Curr. Opin. Cell Biol. 2003, 15, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.M.; Zhou, Z.; Sun, S.; Yu, L.; Sun, L.; Liu, J.; Yang, Z.; Ran, Y.; Yao, Y.; Hu, H. An ADAM12 and FAK positive feedback loop amplifies the interaction signal of tumor cells with extracellular matrix to promote oesophageal cancer metastasis. Cancer Lett. 2018, 422, 118–128. [Google Scholar] [CrossRef]
- Benarroch, E.E. ADAM proteins, their ligands, and clinical implications. Neurology 2012, 78, 914–920. [Google Scholar] [CrossRef]
- Le Gall, S.M.; Bobe, P.; Reiss, K. ADAMs 10 and 17 represent differentially regulated components of a general shedding machinery for membrane proteins such as transforming growth factor alpha, L-selectin, and tumor necrosis factor alpha. Mol. Biol. Cell. 2009, 20, 1785–1794. [Google Scholar] [CrossRef]
- Saftig, P.; Reiss, K. The “A Disintegrin and Metalloproteases” ADAM10 and ADAM17: Novel drug targets with therapeutic potential? Eur. J. Cell Biol. 2011, 90, 527–535. [Google Scholar] [CrossRef]
- Liu, H.B.; Yang, Q.C.; Shen, Y.; Zhu, Y.; Zhang, X.J.; Chen, H. A disintegrin and metalloproteinase 17 mRNA and protein expression in oesophageal squamous cell carcinoma, as well as its clinicopathological factors and prognosis. Mol. Med. Rep. 2015, 11, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Cal, S.; López-Otín, C. ADAMTS proteases and cancer. Matrix Biol. 2015, 44, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Le Bras, G.F.; Taylor, C.; Koumangoye, R.B.; Revetta, F.; Loomans, H.A.; Andl, C.D. TGFβ loss activates ADAMTS-1-mediated EGF-dependent invasion in a model of oesophageal cell invasion. Exp. Cell Res. 2015, 330, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.J. Emerging Roles of Claudins in Human Cancer. Int. J. Mol. Sci. 2013, 14, 18148–18180. [Google Scholar] [CrossRef]
- Hennessy, B.T.; Gonzalez-Angulo, A.M.; Stemke-Hale, K.; Gilcrease, M.Z.; Krishnamurthy, S.; Lee, J.S. Characterization of a naturally occurring breast cancer subset enriched in epithelial-to-mesenchymal transition and stem cell characteristics. Cancer Res. 2009, 69, 4116–41124. [Google Scholar] [CrossRef]
- Turksen, K. Claudins and cancer stem cells. Stem Cell Rev. 2011, 7, 797–798. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Lin, X.; Manorek, G.; Howell, S.B. Claudin-3 and claudin-4 regulate sensitivity to cisplatin by controlling expression of the copper and cisplatin influx transporter CTR1. Mol. Pharmacol. 2013, 83, 85–94. [Google Scholar] [CrossRef]
- Turksen, K.; Troy, T.C. Barriers built on claudins. J. Cell Sci. 2004, 117, 2435–2447. [Google Scholar] [CrossRef] [PubMed]
- Abu-Farsakh, S.; Wu, T.; Lalonde, A.; Sun, J.; Zhou, Z. High expression of Claudin-2 in oesophageal carcinoma and precancerous lesions is significantly associated with the bile salt receptors VDR and TGR5. BMC Gastroenterol. 2017, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Gyõrffy, H.; Holczbauer, A.; Nagy, P.; Szabó, Z.; Kupcsulik, P.; Páska, C.; Papp, J.; Schaff, Z.; Kiss, A. Claudin expression in Barrett’s esophagus and adenocarcinoma. Virchows Arch. 2005, 447, 961–968. [Google Scholar] [CrossRef]
- Xi, Y.; Lin, Y.; Guo, W.; Wang, X.; Zhao, H.; Miao, C.; Liu, W.; Liu, Y.; Liu, T.; Luo, Y.; et al. Multi-omic characterization of genome-wide abnormal DNA methylation reveals diagnostic and prognostic markers for oesophageal squamous-cell carcinoma. Signal Transduct. Target. Ther. 2022, 7, 53. [Google Scholar] [CrossRef]
- Müller, D.; Győrffy, B. DNA Methylation-Based Diagnostic, Prognostic, and Predictive Biomarkers in Colorectal Cancer. Biochim. Biophys. Acta Rev. Cancer 2022, 1877, 188722. [Google Scholar]
- Zhou, C.; Li, J.; Li, Q. CDKN2A methylation in esophageal cancer: A meta-analysis. Oncotarget 2017, 8, 50071–50083. [Google Scholar] [CrossRef]
- Kamb, A.; Shattuck-Eidens, D.; Eeles, R.; Liu, Q.; Gruis, N.A.; Ding, W.; Hussey, C.; Tran, T.; Miki, Y.; Weaver-Feldhaus, J.; et al. Analysis of the p16 gene (CDKN2) as a candidate for the chromosome 9p melanoma susceptibility locus. Nat. Genet. 1994, 8, 23–26. [Google Scholar] [CrossRef]
- Foulkes, W.D.; Flanders, T.Y.; Pollock, P.M.; Hayward, N.K. The CDKN2A (p16) gene and human cancer. Mol. Med. 1997, 3, 5–20. [Google Scholar] [CrossRef]
- Zhao, R.; Choi, B.Y.; Lee, M.H.; Bode, A.M.; Dong, Z. Implications of genetic and epigenetic alterations of CDKN2A (p16(INK4a)) in cancer. EBioMedicine 2016, 8, 30–39. [Google Scholar] [CrossRef]
- Hibi, K.; Taguchi, M.; Nakayama, H.; Takase, T.; Kasai, Y.; Ito, K.; Akiyama, S.; Nakao, A. Molecular detection of p16 promoter methylation in the serum of patients with oesophageal squamous cell carcinoma. Clin. Cancer Res. 2001, 7, 3135–3138. [Google Scholar] [PubMed]
- Guo, M.; Ren, J.; House, M.G.; Qi, Y.; Brock, M.V.; Herman, J.G. Accumulation of promoter methylation suggests epigenetic progression in squamous cell carcinoma of the esophagus. Clin. Cancer Res. 2006, 12, 4515–4522. [Google Scholar] [CrossRef]
- Li, B.; Wang, B.; Niu, L.J.; Jiang, L.; Qiu, C.C. Hypermethylation of multiple tumor-related genes associated with DNMT3b up-regulation served as a biomarker for early diagnosis of oesophageal squamous cell carcinoma. Epigenetics 2011, 6, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Xing, D.; Tan, W.; Wei, Q.; Lin, D. Methylenetetrahydrofolate reductase polymorphisms increase risk of oesophageal squamous cell carcinoma in a Chinese population. Cancer Res. 2001, 61, 3272–3275. [Google Scholar]
- Weaver, J.M.; Ross-Innes, C.S.; Shannon, N.; Lynch, A.G.; Forshew, T.; Barbera, M.; Murtaza, M.; Ong, C.-A.J.; Lao-Sirieix, P.; Dunning, M.J.; et al. Ordering of mutations in preinvasive disease stages of esophageal carcinogenesis. Nat. Genet. 2014, 46, 837–843. [Google Scholar] [CrossRef]
- Madani, K.; Zhao, R.; Lim, H.J.; Casson, A.G. Prognostic value of p53 mutations in oesophageal adenocarcinoma: Final results of a 15-year prospective study. Eur. J. Cardio-Thorac. Surg. 2010, 37, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Murugaesu, N.; Wilson, G.A.; Birkbak, N.J.; Watkins, T.B.; McGranahan, N.; Kumar, S.; Abbassi-Ghadi, N.; Salm, M.; Mitter, R.; Horswell, S.; et al. Tracking the genomic evolution of esophageal adenocarcinoma through neoadjuvant chemotherapy. Cancer Discov. 2015, 5, 821–831. [Google Scholar] [CrossRef]
- Singhi, A.D.; Foxwell, T.J.; Nason, K.; Cressman, K.L.; McGrath, K.M.; Sun, W.; Bahary, N.; Zeh, H.J.; Levy, R.M.; Luketich, J.D.; et al. Smad4 loss in esophageal adenocarcinoma is associated with an increased propensity for disease recurrence and poor survival. Am. J. Surg. Pathol. 2015, 39, 487–495. [Google Scholar] [CrossRef]
- Liu, W.J.; Zhao, Y.; Chen, X.; Miao, M.L.; Zhang, R.Q. Epigenetic modifications in oesophageal cancer: An evolving biomarker. Front. Genet. 2022, 13, 1087479. [Google Scholar] [CrossRef]
- Luo, M.; Li, Y.; Shi, X.; Yang, W.; Zhou, F.; Sun, N.; He, J. Aberrant methylation of EYA4 promotes epithelial-mesenchymal transition in oesophageal squamous cell carcinoma. Cancer Sci. 2018, 109, 1811–1824. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Liou, Y.L.; Wan, Z.R.; Tang, J.; Zhou, Y.; Zhuang, W.; Wang, G. Aberrant DNA methylation of PAX1, SOX1 and ZNF582 genes as potential biomarkers for oesophageal squamous cell carcinoma. Biomed. Pharmacother. 2019, 120, 109488. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, S.; Xie, L.; Liu, P.; Xie, F.; Wu, J.; Cao, J.; Ding, W.Q. Overexpression of DNA polymerase iota (Polι) in oesophageal squamous cell carcinoma. Cancer Sci. 2012, 103, 1574–1579. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. Off J. Eur. Soc. Med. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Chen, X.; Gole, J.; Gore, A.; He, Q.; Lu, M.; Min, J.; Yuan, Z.; Yang, X.; Jiang, Y.; Zhang, T.; et al. Non-invasive early detection of cancer four years before conventional diagnosis using a blood test. Nat. Commun. 2020, 11, 3475. [Google Scholar] [CrossRef]
- Chu, L.Y.; Peng, Y.H.; Weng, X.F.; Xie, J.J.; Xu, Y.W. Blood-based biomarkers for early detection of esophageal squamous cell carcinoma. World J. Gastroenterol. 2020, 26, 1708–1725. [Google Scholar] [CrossRef]
- Payne, K.; Pugh, M.; Brooks, J.; Batis, N.; Taylor, G.; Nankivell, P.; Mehanna, H. Circulating tumour cell expression of immune markers as prognostic and therapeutic biomarkers in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Int. J. Mol. Sci. 2020, 21, 8229. [Google Scholar] [CrossRef]
- Iacob, R.; Mandea, M.; Iacob, S.; Pietrosanu, C.; Paul, D.; Hainarosie, R.; Gheorghe, C. Liquid Biopsy in Squamous Cell Carcinoma of the Esophagus and of the Head and Neck. Front. Med. 2022, 9, 827297. [Google Scholar] [CrossRef]
- Anastasiadou, E.; Jacob, L.S.; Slack, F.J. Non-coding RNA networks in cancer. Nat. Rev. Cancer 2018, 18, 5–18. [Google Scholar] [CrossRef]
- Bhan, A.; Soleimani, M.; Mandal, S.S. Long noncoding RNA and cancer: A new paradigm. Cancer Res. 2017, 77, 3965–3981. [Google Scholar] [CrossRef]
- Li, Y.; Li, J.; Luo, M.; Zhou, C.; Shi, X.; Yang, W.; Lu, Z.; Chen, Z.; Sun, N.; He, J. Novel long noncoding RNA NMR promotes tumor progression via NSUN2 and BPTF in oesophageal squamous cell carcinoma. Cancer Lett. 2018, 430, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Lin, Y.; Luo, Y.; Xiong, X.; Wang, L.; Durante, K.; Li, J.; Zhou, F.; Guo, Y.; Chen, S.; et al. A signature of saliva-derived exosomal small RNAs as predicting biomarker for oesophageal carcinoma: A multicenter prospective study. Mol. Cancer 2022, 21, 21. [Google Scholar] [CrossRef] [PubMed]
- Farazi, T.A.; Hoell, J.I.; Morozov, P.; Tuschl, T. microRNAs in human cancer. Adv. Exp. Med. Biol. 2013, 774, 1. [Google Scholar]
- Zhao, J.; Li, L.; Wang, Z.; Li, L.; He, M.; Han, S.; Dong, Y.; Liu, X.; Zhao, W.; Ke, Y.; et al. Luteolin attenuates cancer cell stemness in PTX-resistant ooesophageal cancer cells through mediating SOX2 protein stability. Pharmacol. Res. 2021, 174, 105939. [Google Scholar] [CrossRef] [PubMed]
- Xue, S.T.; Zheng, B.; Cao, S.Q.; Ding, J.C.; Hu, G.S.; Liu, W.; Chen, C. Long non-coding RNA LINC00680 functions as a ceRNA to promote oesophageal squamous cell carcinoma progression through the miR-423-5p/PAK6 axis. Mol. Cancer 2022, 21, 69. [Google Scholar] [CrossRef] [PubMed]
- Zong, M.; Feng, W.; Wan, L.; Yu, X.; Yu, W. LncRNA TUG1 promotes oesophageal cancer development through regulating PLK1 expression by sponging miR-1294. Biotechnol. Lett. 2022, 42, 2537–2549. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Qi, Y.; Qu, J.; Gai, L.; Shi, Y.; Yuan, C. Pathophysiological Functions of the lncRNA TUG1. Curr. Pharm. Des. 2020, 26, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.M.; Zang, H.L.; Geng, Y.X.; Li, Y.H. LncRNA FAM83A-AS1 aggravates the malignant development of oesophageal cancer by binding to miR-495-3p. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9408–9415. [Google Scholar] [PubMed]
- Yao, W.; Jia, X.; Xu, L.; Li, S.; Wei, L. MicroRNA-2053 involves in the progression of oesophageal cancer by targeting KIF3C. Cell Cycle 2021, 20, 1163–1172. [Google Scholar] [CrossRef]
- Bian, W.; Li, Y.; Zhu, H.; Gao, S.; Niu, R.; Wang, C.; Zhang, H.; Qin, X.; Li, S. miR-493 by regulating of c-Jun targets Wnt5a/PD-L1-inducing oesophageal cancer cell development. Thorac. Cancer 2021, 12, 1579–1588. [Google Scholar] [CrossRef]
- Gong, Z.; Li, J.; Cang, P.; Jiang, H.; Liang, J.; Hou, Y. RPL34-AS1 functions as tumor suppressive lncRNA in oesophageal cancer. Biomed. Pharmacother. 2019, 120, 109440. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Pan, E.; Zhang, Y.; Zhao, C.; Liu, Q.; Pu, Y.; Yin, L. LncRNA RPL34-AS1 suppresses the proliferation, migration and invasion of oesophageal squamous cell carcinoma via targeting miR-575/ACAA2 axis. BMC Cancer 2022, 26, 1017. [Google Scholar]


{kind=link}
| Clinical Significance | Protein | References |
|---|---|---|
| The correlation between protein levels and tumor stage | CXCL12, CXCR4, CXCL8/CXCR2, CRP, M-CSF, SCF, MMP-2, MMP-9, ADAM17, ADAM9, ADAMTS-6, CLDN7 | [17,25,26,27,28,29,30,31,32,33,34,35,36,37,38] |
| The correlation between protein levels and the presence of lymph node metastases | CXCL12, CXCR4, CXCL8/CXCR2, CRP, IL-6, M-CSF, MMP-2, MMP-9, ADAM17, ADAMTS-6, CLDN7 | [25,26,27,28,29,32,33,38,39] |
| The correlation between protein levels and the presence of distant metastases | IL-6, CRP, M-CSF | [17,30,32,40] |
| The correlation between protein levels and survival of OC patients | CXCL12, CXCL8/CXCR2, IL-6, TIMP-2, ADAM9, ADAMTS-6 | [25,29,35,36,37,41] |
| Diagnosis of OC patients | CXCR4, CXCL8, IL-6, MMP-9 | [17,42,43,44] |
| Novel targeted therapies for OC patients | CLDN18.2 | [45] |
| Genes | Functions | Methylation Status and References |
|---|---|---|
| EYA4 | Engaged in the regulation of apoptosis, innate immunity, DNA damage repair, and angiogenesis | Hypermethylation status [110,111] |
| PAX1 | Engaged in the control of transcription, DNA-dependent processes, and promoter development | Hypermethylation status [112] |
| SOX1 | Engaged in the establishment and upkeep of chromatin structure, regulation of transcription, and is DNA-dependent | Hypermethylation status [112] |
| ZNF582 | Engaged in transcriptional regulation | Hypermethylation status [112] |
| Polι | Engaged in the translation process and synthesis of DNA | Hypomethylation state [113] |
| Biomarkers of ncRNAs | Mechanism | References |
|---|---|---|
| LncRNA TUG 1 | Control of the miR-1294/PLK1 pathway, a pivotal oncogenic mechanism in oesophageal cancer. | [126,127] |
| LncRNA FAM83A-AS1 | Intensification of malignant advancement by suppressing the activity of miR-495-3p. | [128] |
| miR-2053 | Elevation of kinesin family member 3C (KIF3C) expression and initiation of the PI3K/AKT signaling pathway are implicated in cell proliferation, apoptosis, migration, and invasion. | [129] |
| miR-493 | Suppresses transcription factor Jun (c-JUN) and p-PI3K/p-AKT activity, enhances p21 | [130] |
| LncRNA RPL34-AS1 | Upregulation of RPL34-AS1, suppressed cell proliferation, colony formation, invasion, and migration in vitro, overexpression of RPL34-AS1, and inhibited tumor growth in vivo | [131,132] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romanowicz, A.; Lukaszewicz-Zajac, M.; Mroczko, B. Exploring Potential Biomarkers in Oesophageal Cancer: A Comprehensive Analysis. Int. J. Mol. Sci. 2024, 25, 4253. https://doi.org/10.3390/ijms25084253
Romanowicz A, Lukaszewicz-Zajac M, Mroczko B. Exploring Potential Biomarkers in Oesophageal Cancer: A Comprehensive Analysis. International Journal of Molecular Sciences. 2024; 25(8):4253. https://doi.org/10.3390/ijms25084253
Chicago/Turabian StyleRomanowicz, Adrianna, Marta Lukaszewicz-Zajac, and Barbara Mroczko. 2024. "Exploring Potential Biomarkers in Oesophageal Cancer: A Comprehensive Analysis" International Journal of Molecular Sciences 25, no. 8: 4253. https://doi.org/10.3390/ijms25084253
APA StyleRomanowicz, A., Lukaszewicz-Zajac, M., & Mroczko, B. (2024). Exploring Potential Biomarkers in Oesophageal Cancer: A Comprehensive Analysis. International Journal of Molecular Sciences, 25(8), 4253. https://doi.org/10.3390/ijms25084253