Personalized Rehabilitation Recognition for Ubiquitous Healthcare Measurements


Abstract
:1. Introduction
2. Methods and Modeling
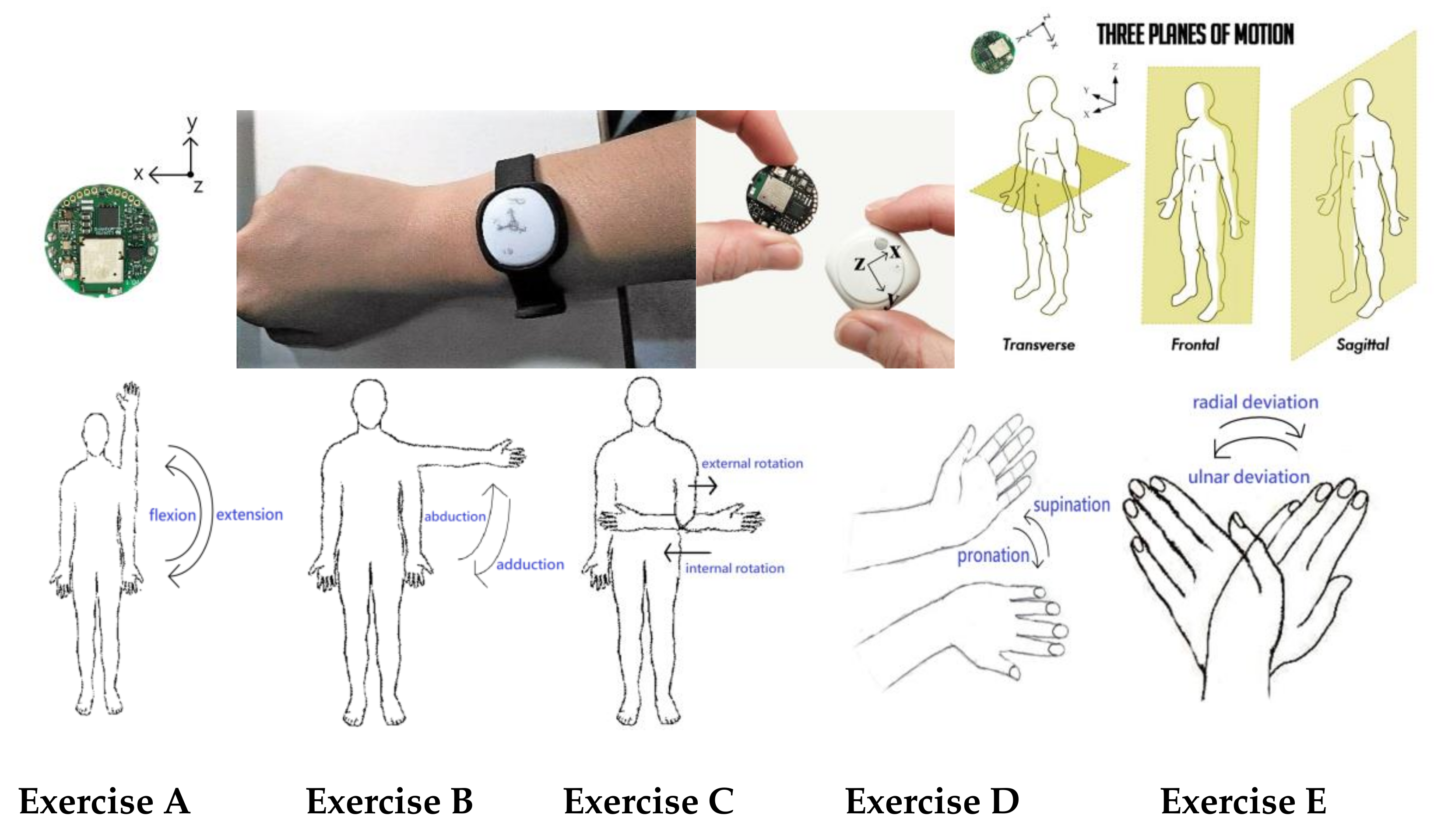
2.1. Rehabilitation Motion Design
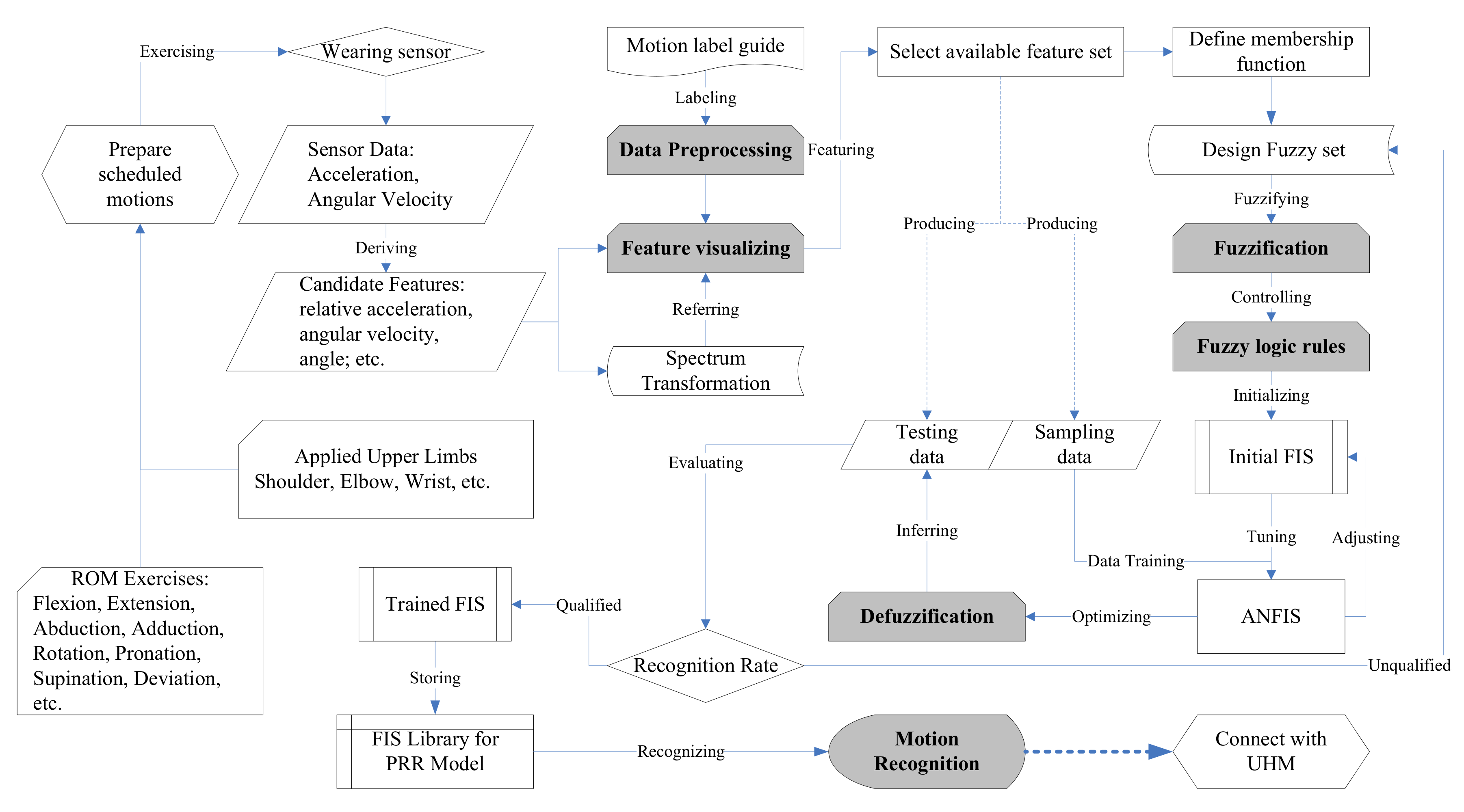
2.2. Modeling
2.2.1. Data Preprocessing and Sampling
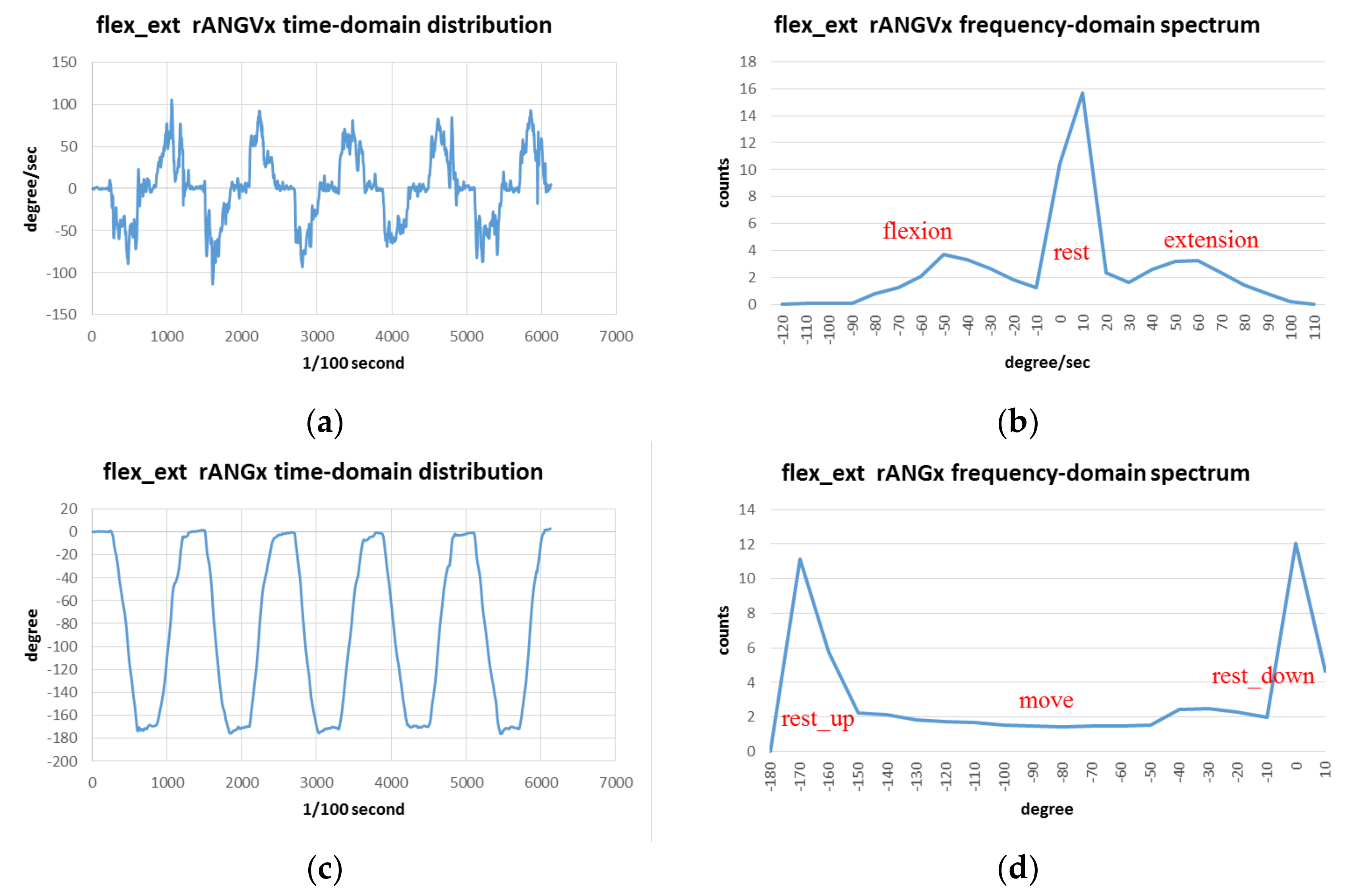
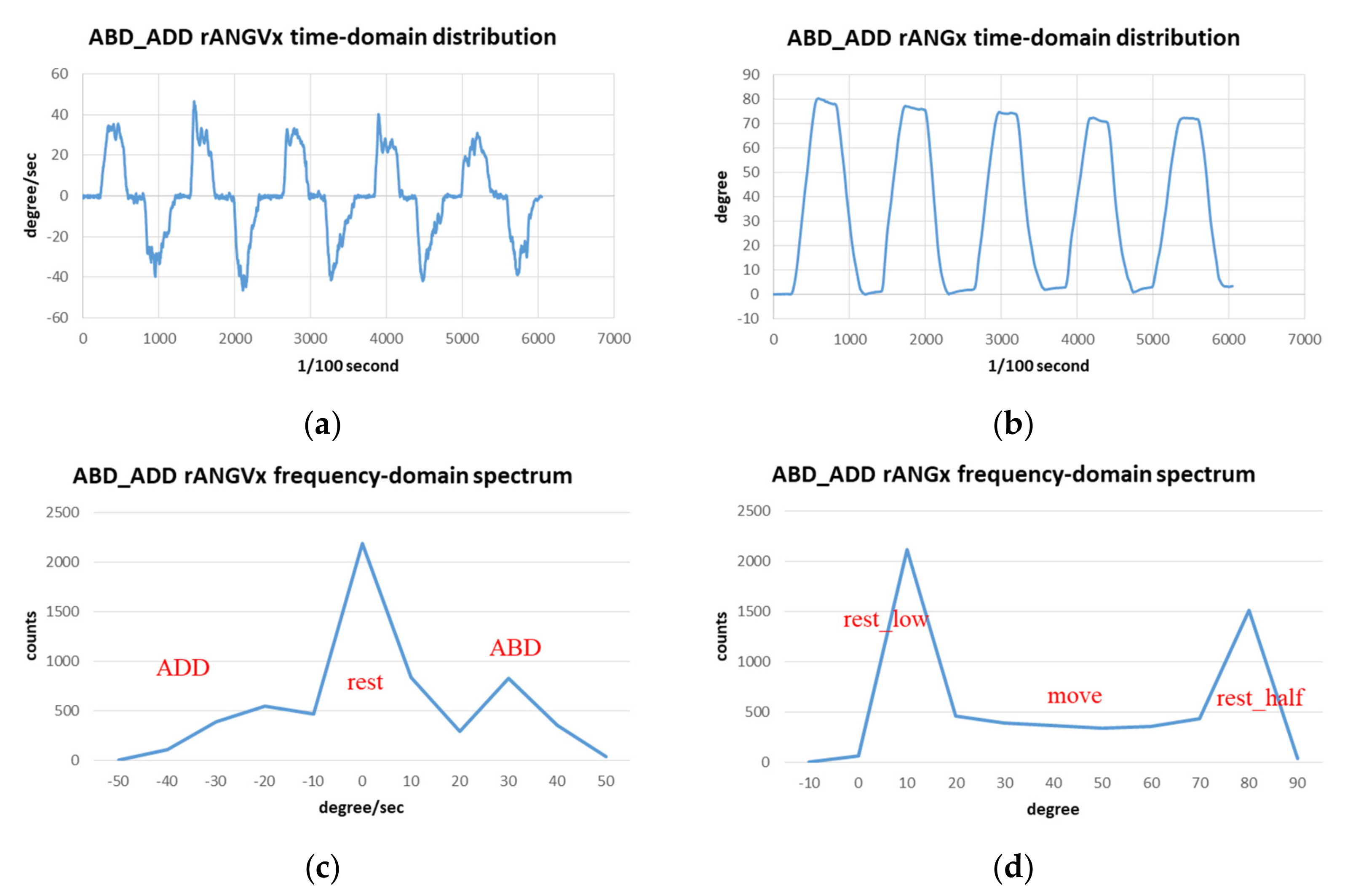
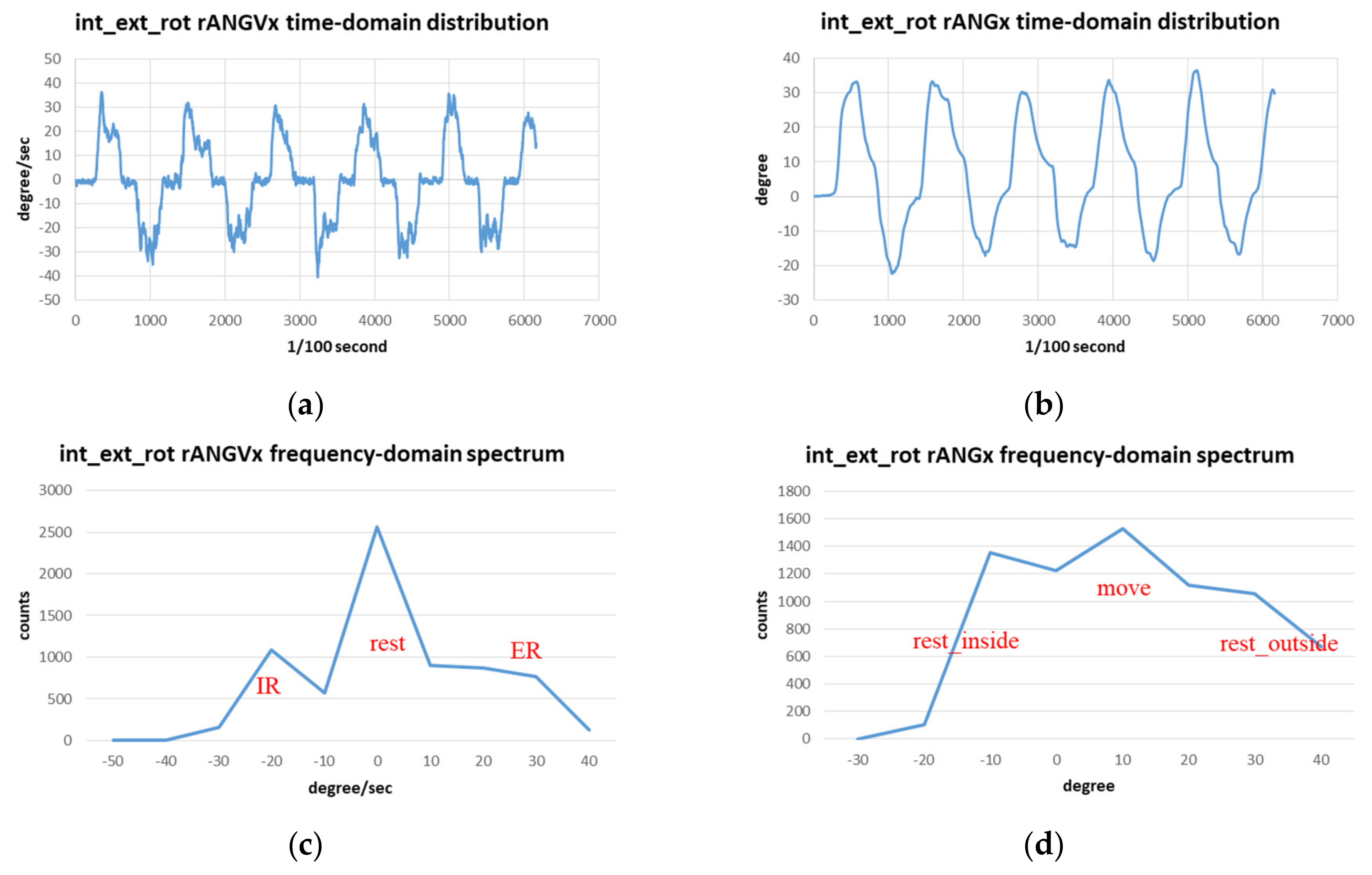
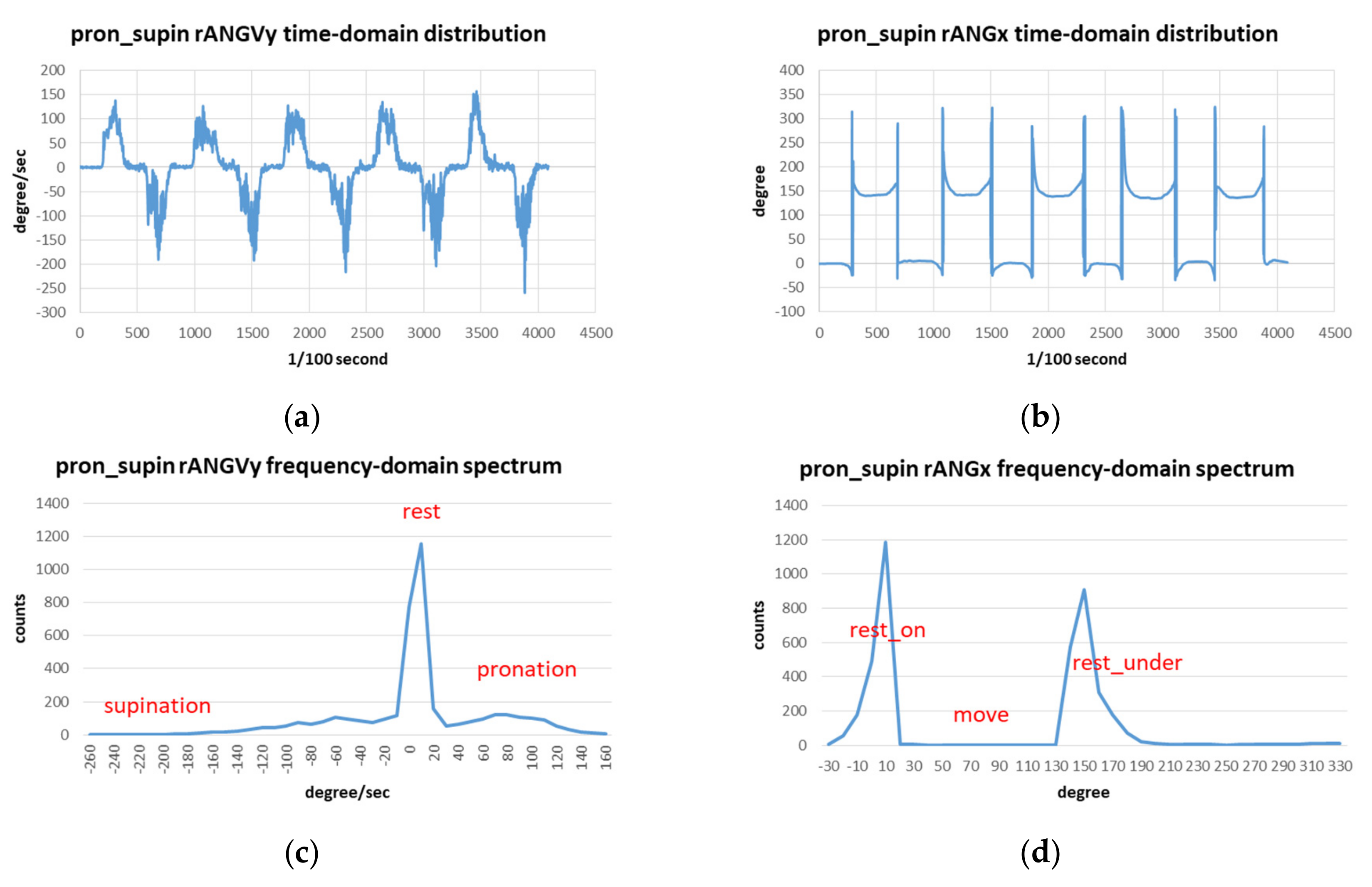
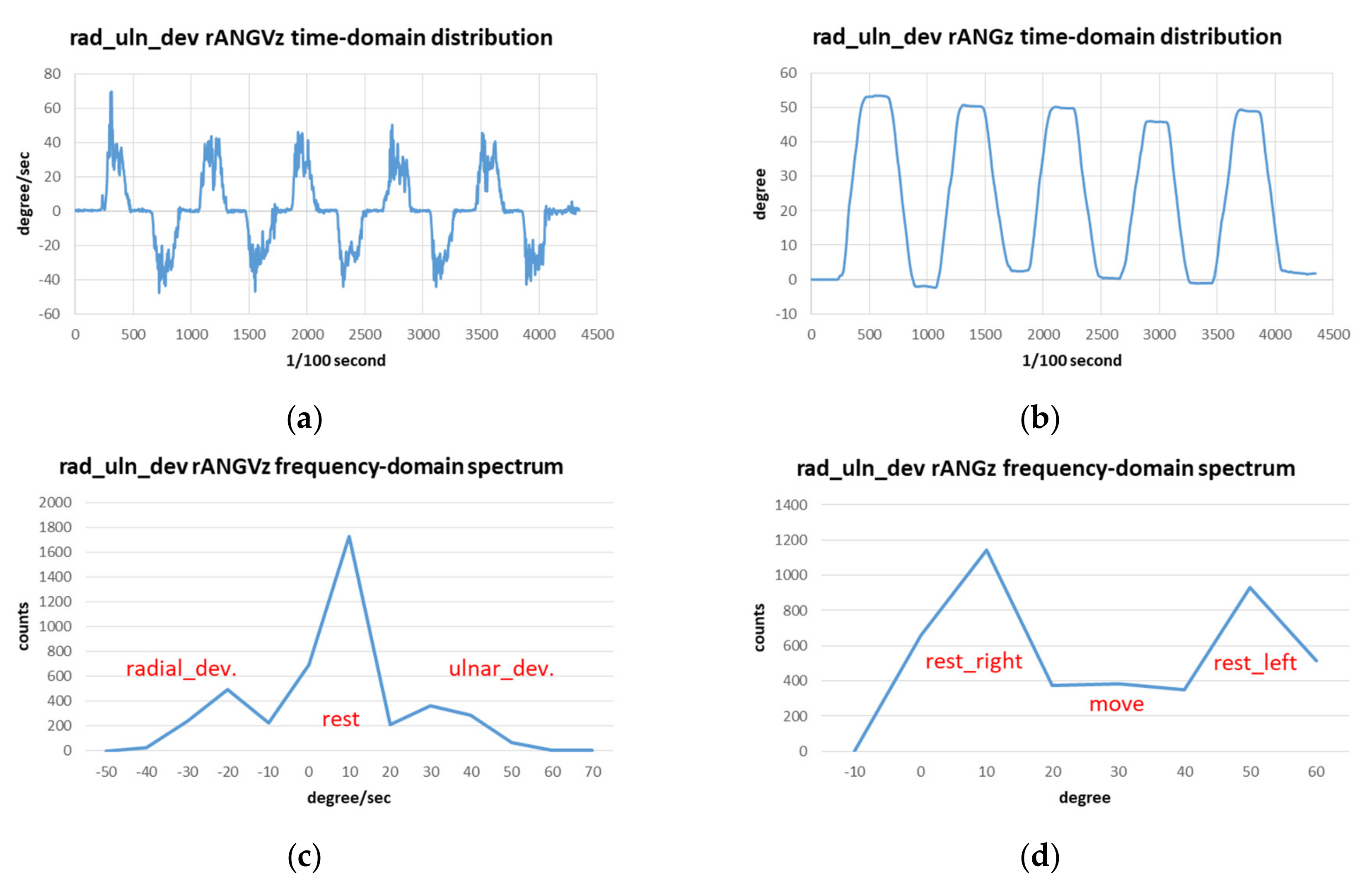
2.2.2. Feature Visualizing
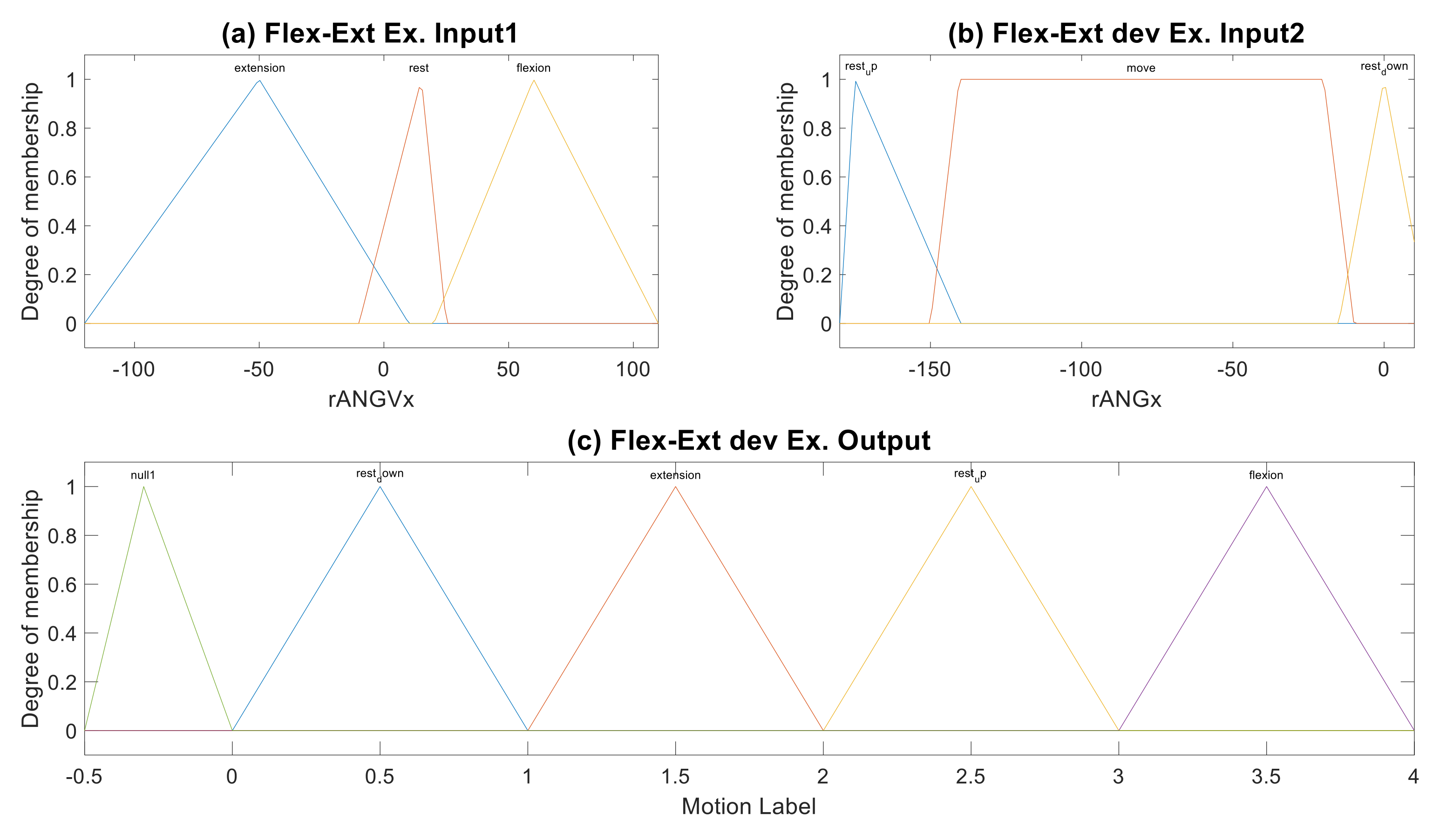
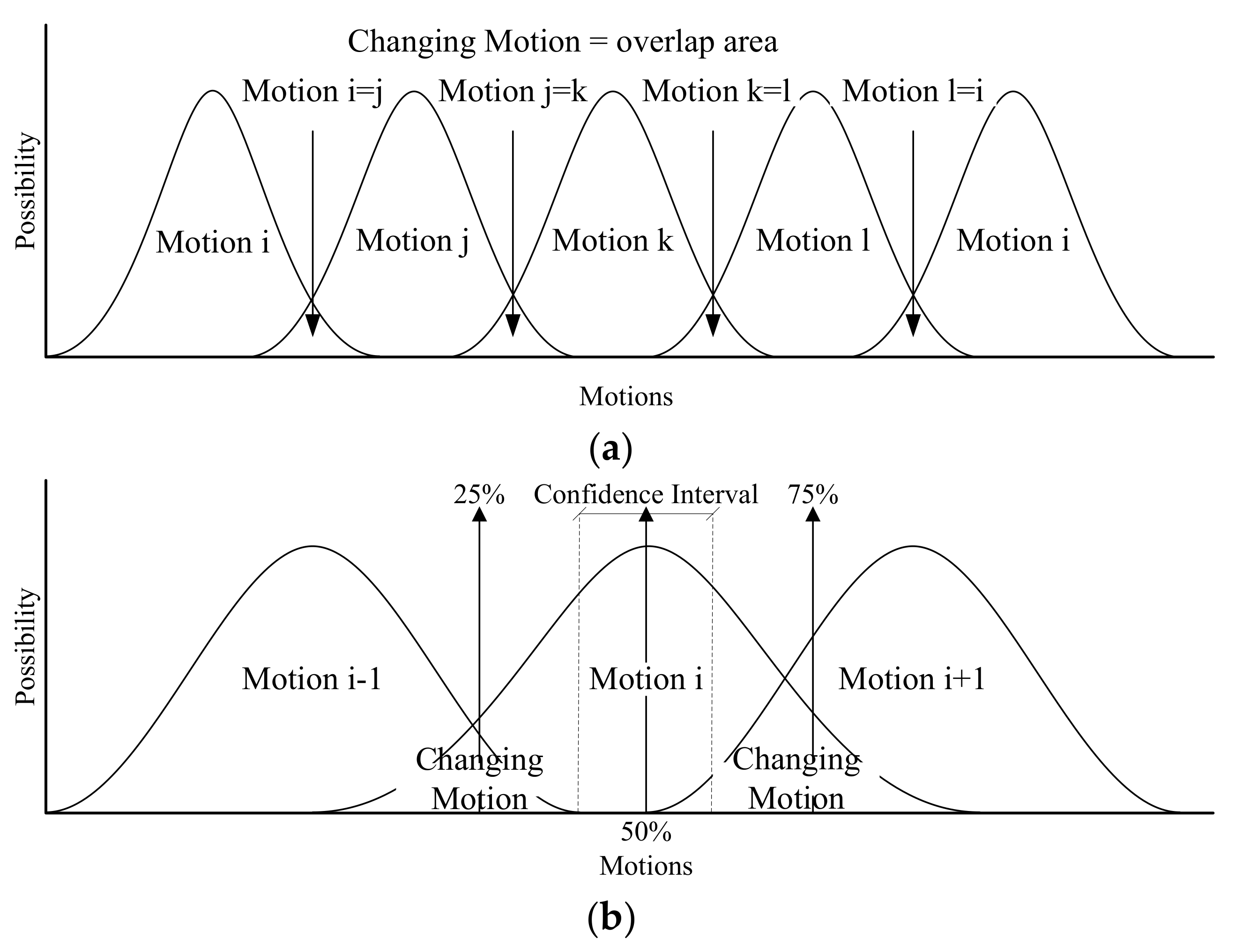
2.2.3. Fuzzification and Featuring
2.2.4. Fuzzy Logic Rule and Data Training
2.2.5. Defuzzification and Recognition
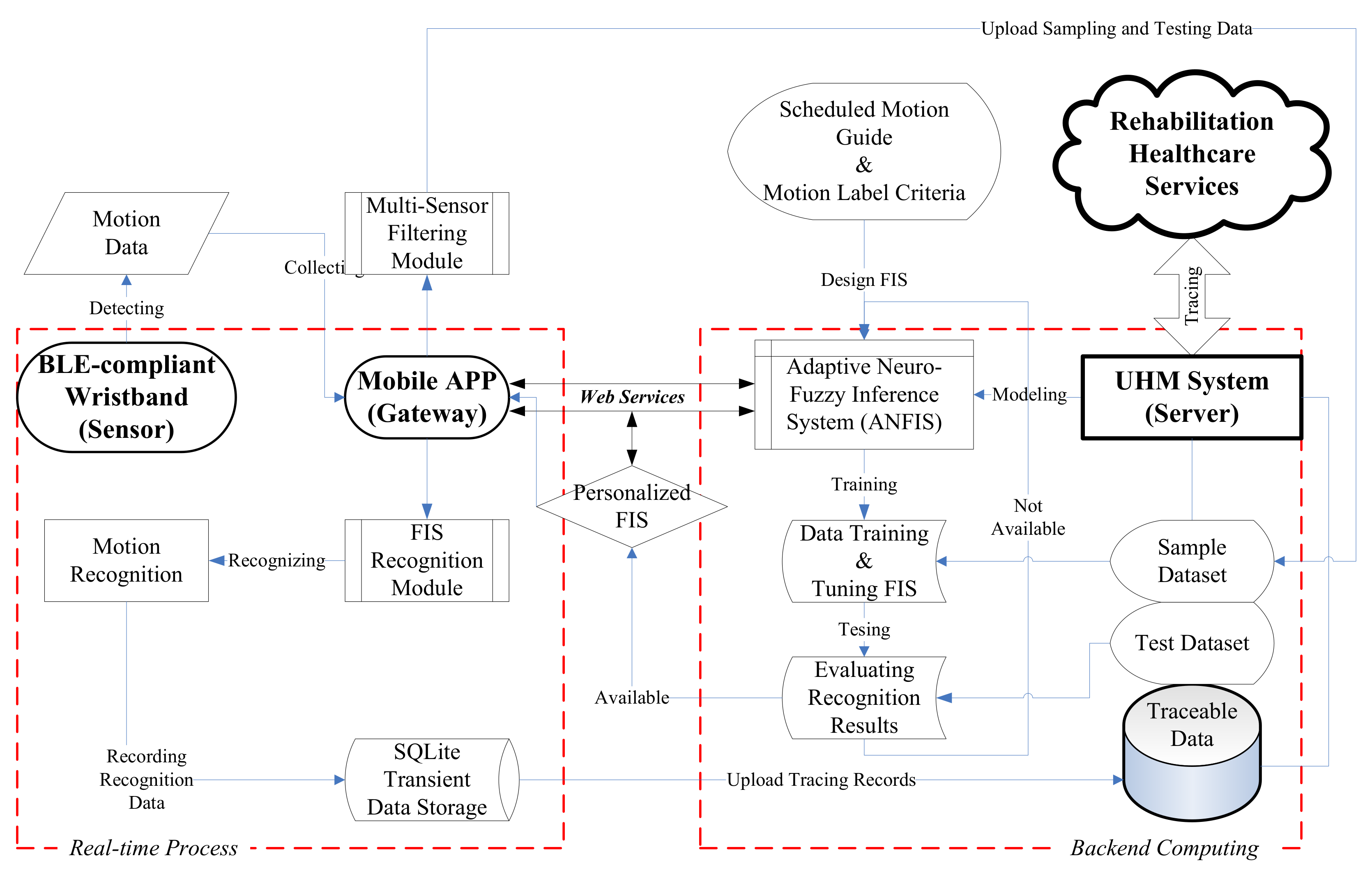
2.3. Ubiquitous Healthcare Measurement System
3. Results and Evaluation
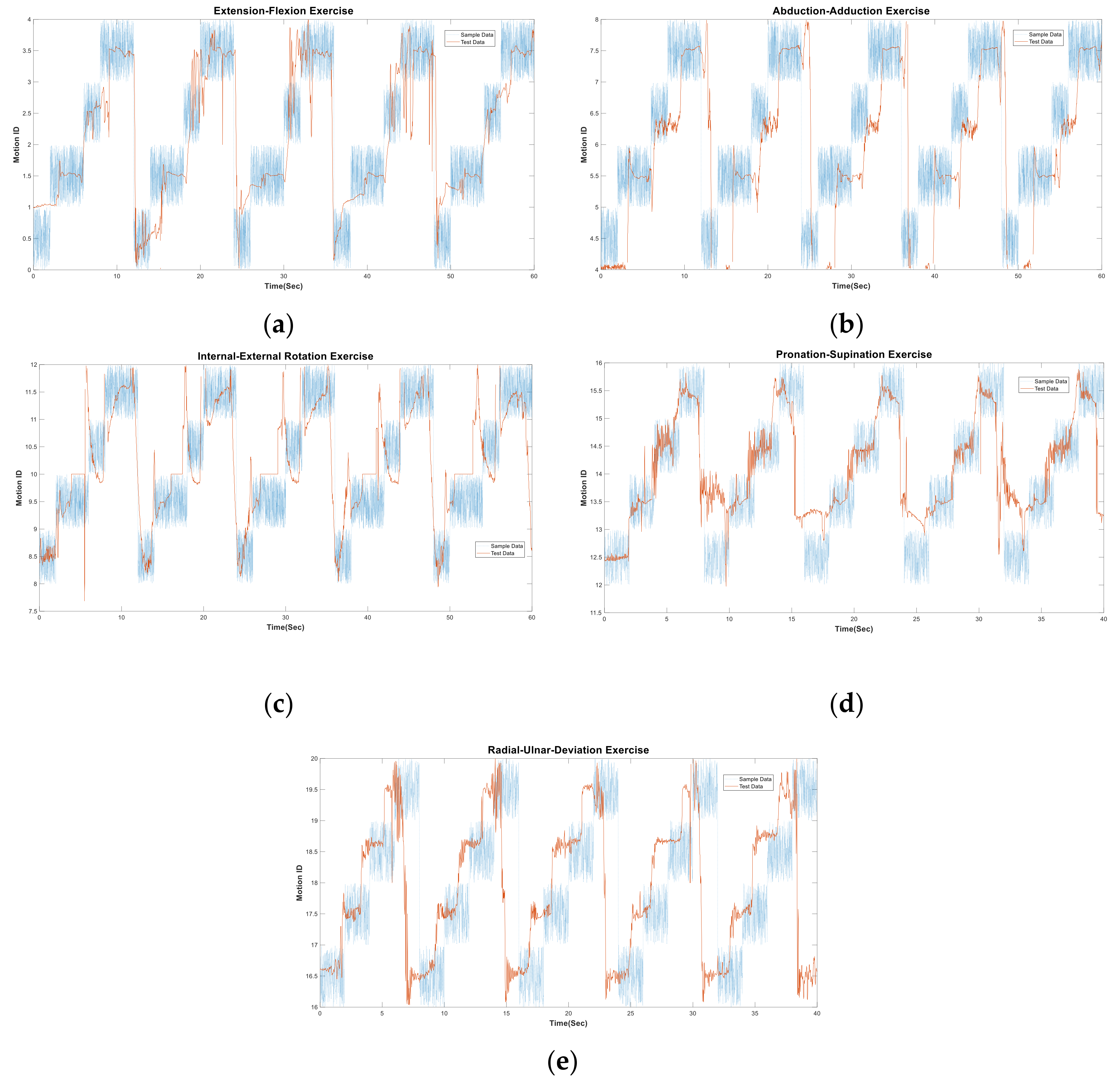
3.1. Inference Result
3.2. Recognition Evaluation
4. Implementation and Discussion
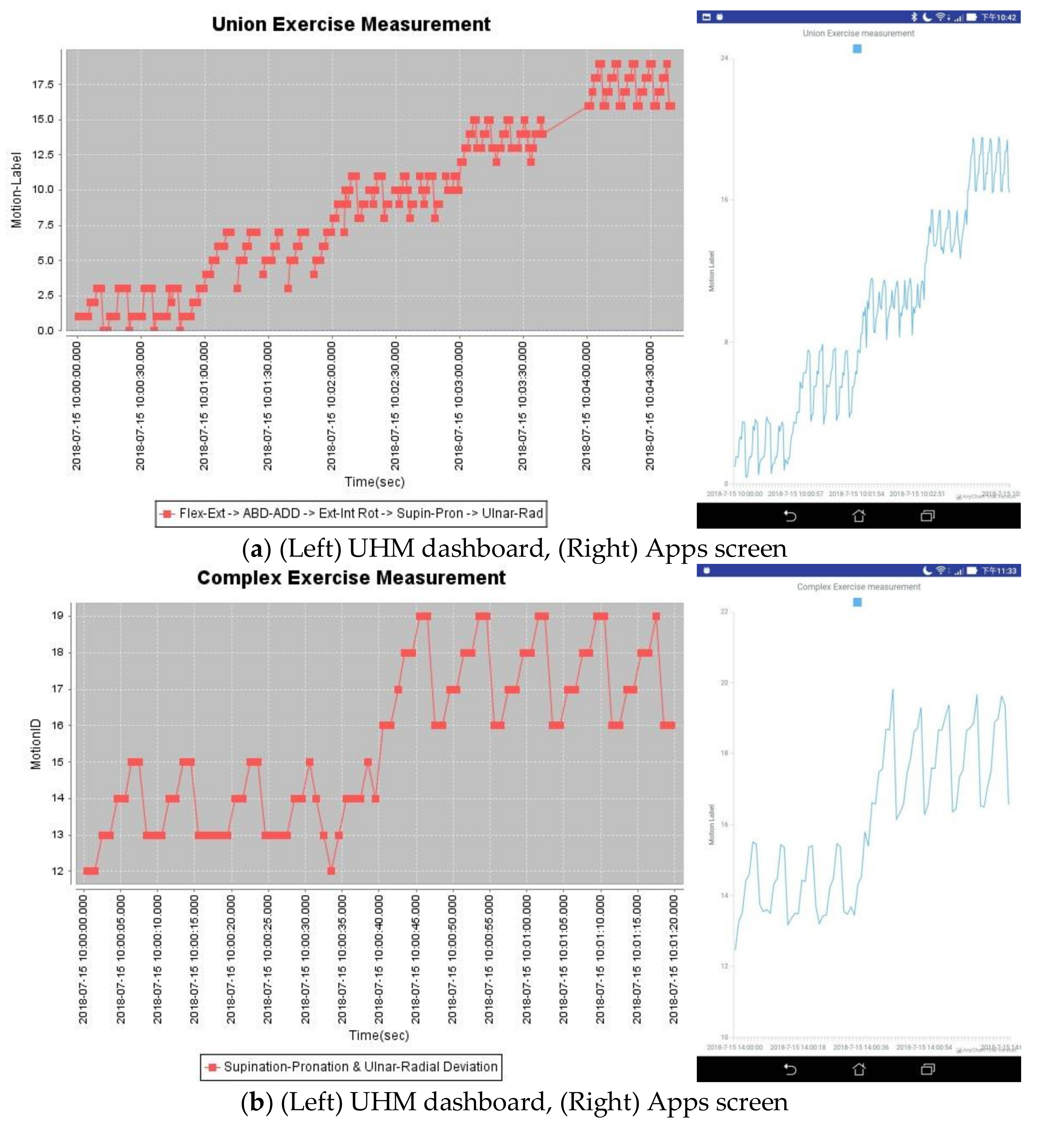
4.1. UHM Implementation
4.2. Discussion
4.2.1. Advantages
4.2.2. Limitations
5. Conclusions Remarks
Author Contributions
Funding
Conflicts of Interest
Appendix A




Appendix B




References
- Hume, M.C.; Gellman, H.; McKellop, H.; Brumfield, R.H. Functional range of motion of the joints of the hand. J. Hand Surg. 1990, 15, 240–243. [Google Scholar] [CrossRef]
- Gunal, I.; Kose, N.; Erdogan, O.; Gokturk, E.; Seber, S. Normal Range of Motion of the Joints of the Upper Extremity in Male Subjects, with Special Reference to Side. J. Bone Joint Surg. 1996, 78, 1401–1404. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; van der Helm, F.C.T.; Veeger, H.E.J.; Makhsous, M.; van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; Werner, F.W.; Buchholz, B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion - Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Jackson, M.; Michaud, B.; Tetreault, P.; Begona, M. Improvements in measuring shoulder joint kinematics. J. Biomech. 2012, 45, 2180–2183. [Google Scholar] [CrossRef]
- Duprey, S.; Naaim, A.; Moissenet, F.; Begon, M.; Cheze, L. Kinematic models of the upper limb joints for multibody kinematics optimisation: An overview. J. Biomech. 2017, 62, 87–94. [Google Scholar] [CrossRef]
- Glueckauf, R.L.; Whitton, J.D.; Nickelson, D.W. Telehealth: The new frontier in rehabilitation and health care. In Assistive Technology: Matching Device and Consumer for Successful Rehabilitation; Scherer, M.J., Ed.; American Psychological Association: Washington, DC, USA, 2002; pp. 197–213. [Google Scholar]
- Van der Loos, H.M.; Reinkensmeyer, D.J.; Guglielmelli, E. Rehabilitation and Health Care Robotics. In Springer Handbook of Robotics; Siciliano, B., Khatib, O., Eds.; Springer-Verlag: Berlin/Heidelberg, Germany, 2008; pp. 1223–1251. [Google Scholar]
- Chang, Y.-J.; Han, W.-Y.; Tsai, Y.-C. A Kinect-based upper limb rehabilitation system to assist people with cerebral palsy. Res. Dev. Disabili. 2013, 34, 3654–3659. [Google Scholar] [CrossRef] [PubMed]
- Lum, P.S.; Burgar, C.G.; Shor, P.C.; Majmundar, M.; van der Loos, M. Robot-assisted movement training compared with conventional therapy techniques for the rehabilitation of upper-limb motor function after stroke. Arch. Phys. Med. Rehabil. 2002, 83, 952–959. [Google Scholar] [CrossRef]
- Maund, E.; Craig, D.; Suekarran, S.; Neilson, A.R.; Wright, K.; Brealey, S.; Dennis, L.; Goodchild, L.; Hanchard, N.; Rangan, A.; et al. Management of frozen shoulder: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2012, 16, 1–264. [Google Scholar] [CrossRef]
- Lin., H.-C.; Chiang, S.-Y.; Lee, K.; Kan, Y.-C. An Activity Recognition Model Using Inertial Sensor Nodes in a Wireless Sensor Network for Frozen Shoulder Rehabilitation Exercises. Sensors 2015, 15, 2181–2204. [Google Scholar] [CrossRef] [PubMed]
- Lymberis, A. Smart wearable systems for personalised health management: Current R&D and future challenges. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Socociety (IEEE Cat. No.03CH37439), Cancun, Mexico, 17–21 September 2003. [Google Scholar]
- Koch, S. Home telehealth—Current state and future trends. Int. J. Med. Inform. 2006, 75, 565–576. [Google Scholar] [CrossRef]
- Darwish, A.; Hassanien, A.E. Wearable and implantable wireless sensor network solutions for healthcare monitoring. Sensors 2011, 11, 5561–5595. [Google Scholar] [CrossRef]
- Chen, M.; Gonzalez, S.; Vasilakos, A.; Cao, H.; Leung, V. Body Area Networks: A Survey. Mobile Netw. Appl. 2010, 16, 1–23. [Google Scholar] [CrossRef]
- Ullah, S.; Higgins, H.; Braem, B.; Latre, B.; Blondia, C.; Moerman, I.; Saleem, S.; Rahman, Z.; Kwak, S. A Comprehensive Survey of Wireless Body Area Networks: On PHY, MAC, and Network Layers Solutions. J. Med. Syst. 2010, 36, 1065–1094. [Google Scholar] [CrossRef]
- Movassaghi, S.; Abolhasan, M.; Lipman, J.; Smith, D.; Jamalipour, A. Wireless Body Area Networks: A Survey. IEEE Commun. Surv. Tut. 2014, 16, 1658–1686. [Google Scholar] [CrossRef]
- Poslad, S. Ubiquitous Computing Smart Devices, Smart Environments and Smart Interaction; John Wiley & Sons: Chippenham, UK, 2009; pp. 75–113. [Google Scholar]
- Wu, M.-F.; Huang, W.-C.; Juang, C.-F.; Chang, K.-M.; Wen, C.-Y.; Chen, Y.-H.; Lin, C.-Y.; Chen, Y.-C.; Lin, C.-C. A New Method for Self-Estimation of the Severity of Obstructive Sleep Apnea Using Easily Available Measurements and Neural Fuzzy Evaluation System. IEEE J. Biomed. Health Inform. 2017, 21, 1524–1532. [Google Scholar] [CrossRef]
- Pärkkä, J.; Ermes, M.; Korpipää, P.; Mäntyjärvi, J.; Peltola, J.; Korhonen, I. Activity classification using realistic data from wearable sensors. IEEE T. Inf. Technol. Biomed. 2006, 10, 119–128. [Google Scholar] [CrossRef]
- Hegde, N.; Bries, M.; Swibas, T.; Melanson, E.; Sazonov, E. Automatic Recognition of Activities of Daily Living Utilizing Insole-Based and Wrist-Worn Wearable Sensors. IEEE J. Biomed. Health Inform. 2018, 22, 979–988. [Google Scholar] [CrossRef]
- Fletcher, R.R.; Poh, M.-Z.; Eydgahi, H. Wearable sensors: Opportunities and challenges for low-cost health care. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010. [Google Scholar]
- Singh, G.; Nelson, A.; Robucci, R.; Patel, C.; Banerjee, N. Inviz: Low-power personalized gesture recognition using wearable textile capacitive sensor arrays. In Proceedings of the IEEE International Conference on Pervasive Computing and Communications (PerCom), St. Louis, MO, USA, 23–27 March 2015. [Google Scholar]
- Rault, T.; Bouabdallah, A.; Challal, Y.; Marin, F. A survey of energy-efficient context recognition systems using wearable sensors for healthcare applications. Pervasive Mob. Comput. 2017, 37, 23–44. [Google Scholar] [CrossRef]
- Chang, Y.-J.; Chen, S.-F.; Huang, J.-D. A Kinect-based system for physical rehabilitation: A pilot study for young adults with motor disabilities. Res. Dev. Disabil. 2011, 32, 2566–2570. [Google Scholar] [CrossRef]
- Bose, B.K. Expert system, fuzzy logic, and neural network applications in power electronics and motion control. Proc. IEEE 1994, 82, 1303–1323. [Google Scholar] [CrossRef]
- Yu, H.; Sun, G.-M.; Song, W.-X.; Li, X. Human motion recognition based on neural network. In Proceedings of the 2005 International Conference on Communications, Circuits and Systems, Hong Kong, China, 27–30 May 2005. [Google Scholar]
- Du, Y.; Wang, W.; Wang, L. Hierarchical Recurrent Neural Network for Skeleton Based Action Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 8–10 June 2015; pp. 1110–1118. [Google Scholar]
- Lee, C.C. Fuzzy logic in control systems: Fuzzy logic controller Part II. IEEE T. Syst. Man Cyb. 1990, 20, 419–435. [Google Scholar] [CrossRef]
- Bardossy, A.; Duckstein, L. Fuzzy rule-based modeling with applications to geophysical, biological and engineering systems. CRC Press: Boca Raton, FL, USA, 1995. [Google Scholar]
- Herrero, D.; Martinez, H. Fuzzy mobile-robot positioning in intelligent spaces using wireless sensor networks. Sensors 2011, 11, 10820–10839. [Google Scholar] [CrossRef]
- Zadeh, L.A. Outline of a new approach to the analysis of complex systems and decision processes. IEEE T. Syst. Man Cyb. 1973, 3, 28–44. [Google Scholar] [CrossRef]
- Mamdani, E.H.; Assilian, S. An experiment in linguistic synthesis with a fuzzy logic controller. Int. J. Man-Mach. Stud. 1975, 7, 1–13. [Google Scholar] [CrossRef]
- Takagi, T.; Sugeno, M. Derivation of fuzzy control rules from human operator’s control actions. IFAC Proc. Volumes 1983, 16, 55–60. [Google Scholar] [CrossRef]
- Ying, H.; Ding, Y.; Li, S.; Shao, S. Comparison of necessary conditions for typical Takagi-Sugeno and Mamdani fuzzy systems as universal approximators. IEEE T. Syst. Man Cy. A. 1999, 29, 508–514. [Google Scholar] [CrossRef]
- Jang, J.S-R. “ANFIS: Adaptive-network-based fuzzy inference system,”. IEEE T. Syst. Man Cyb. 1993, 23, 665–685. [Google Scholar]
- Toosi, A.N.; Kahani, M. A new approach to intrusion detection based on an evolutionary soft computing model using neuro-fuzzy classifiers. Comput. Commun. 2007, 30, 2201–2212. [Google Scholar] [CrossRef]
- Chan, C.S.; Liu, H. Fuzzy qualitative human motion recognition. IEEE T. Fuzzy Syst. 2009, 17, 851–862. [Google Scholar] [CrossRef]
- Chiang, S.-Y.; Kan, Y.-C.; Chen, Y.-S.; Tu, Y.-C.; Lin, H.-C. Fuzzy Computing Model of Activity Recognition on WSN Movement Data for Ubiquitous Healthcare Measurement. Sensors 2016, 16, 2053. [Google Scholar] [CrossRef]
- Mbientlab, Wearable Technology for Healthcare. Available online: https://mbientlab.com/ (accessed on 15 July 2018).
- Rada-Vilela, J. The FuzzyLite Libraries for Fuzzy Logic Control. Available online: https://www.fuzzylite.com/ (accessed on 20 June 2017).
- Sensortec, Bosch BMI160, Inertial Measurement Units. Available online: https://www.bosch-sensortec.com/bst/products/all_products/bmi160 (accessed on 10 January 2019).
- Lin, H.-C.; Kan, Y.-C.; Hong, Y.-M. The Comprehensive Gateway Model for Diverse Environmental Monitoring upon Wireless Sensor Network. IEEE Sensors J. 2011, 11, 1293–1303. [Google Scholar] [CrossRef]
- Hu, W.; Xie, D.; Tan, T.; Maybank, S. Learning activity patterns using fuzzy self-organizing neural network. IEEE T. Syst. Man Cy. B. 2004, 34, 1618–1626. [Google Scholar] [CrossRef]
- Attal, F.; Mohammed, S.; Dedabrishvili, M.; Chamroukhi, F.; Oukhellou, L.; Amirat, Y. Physical Human Activity Recognition Using Wearable Sensors. Sensors 2015, 15, 31314–31338. [Google Scholar] [CrossRef]
- Cancela, J.; Villanueva Mascato, S.; Gatsios, D.; Rigas, G.; Marcante, A.; Gentile, G.; Biundo, R.; Giglio, M.; Chondrogiorgi, M.; Vilzmann, R.; et al. Monitoring of motor and non-motor symptoms of Parkinson’s disease through a mHealth platform. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 663–666. [Google Scholar]
- Zhao, W.; Lun, R.; Espy, D.D.; Ann Reinthal, M. Realtime Motion Assessment for Rehabilitation Exercises: Integration Of Kinematic Modeling With Fuzzy Inference. J. Artif. Intell. Soft Comput. Res. 2014, 4, 267–285. [Google Scholar] [CrossRef]
- Martin, P.; Reza Emami, M. A neuro-fuzzy approach to real-time trajectory generation for robotic rehabilitation. Robot. and Auton. Syst. 2014, 62, 568–578. [Google Scholar] [CrossRef]
- Pancardo, P.; Hernández-Nolasco, J.A.; Acosta-Escalante, F. A Fuzzy Logic-Based Personalized Method to Classify Perceived Exertion in Workplaces Using a Wearable Heart Rate Sensor. Mobile Inform. Syst. 2018, 2018, 4216172. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motion | Definition | Joints | Exercise |
|---|---|---|---|
| Flexion | move the limb along +Z axis on sagittal plane | shoulder, elbow, wrist | flexion-extension 1 |
| Extension | move the limb along –Z axis on sagittal plane | ||
| Abduction(ABD) | move the limb along +Z axis on frontal plane | shoulder | horizontal abduction-adduction 2 |
| Adduction(ADD) | move the limb along –Z axis on frontal plane | ||
| Rotation | rotate the limb or palm around Z axis on transverse plane | elbow, wrist | ext-int rotation 3, pronation-supination 4 |
| Deviation | swing the wrist between radial and ulnar sides orthogonal to frontal plane | wrist | ulnar-radial deviation 5 |
| Exercise | rANGVx | rANGVy | rANGVz | rANGx | rANGz |
|---|---|---|---|---|---|
| A. flex-ext Ex. | V | V | |||
| B. abd-add Ex. | V | V | |||
| C. ext-int rot. Ex. | V | V | |||
| D. pron-supin Ex. | V | V | |||
| E. ulnar-rad dev. Ex. | V | V |
| Input Features and Mamdani-Type MF (Vertex of Geometric Shape) 1 | ||||
| rANGVx Vertex Set Shape | MF1: i_rest [−120,−50,10] Triangle | MF2: i_flexion [−10,15,25] Triangle | MF3: i_extension [20,60,110] Triangle | |
| rANGx Vertex Set Shape | MF1: i_rest_down [−180,−175,−140] Triangle | MF2: i_move [−150,−140.5,−19.9994,−9.98] Trapezoid | MF3: i_rest_up [−14.999,0.00043,15] Triangle | |
| Output Feature and Sugeno-Type MF (Coefficients of Linear Equation) 2 | ||||
| Motion Coefficient | MF1: o_rest_down [0.0077,0.1022,0.913] | MF2: o_flexion [0.0008,0.0002,1.5907] | ||
| Motion Coefficient | MF3: o_rest_up [−0.1899,0.1779,33.5760] | MF4: o_extension [−0.0019,−0.0011,3.5074] | ||
| Virtual Motion 3 | null_1: [0.0181,−1.0772,−0.5743], null_2: [−0.0009,−0.0012,3.3421], null_3: [−0.0266,0.0076,4.2697], null_4: [−0.0118,0.0475,1.1785], null_5: [0.0011,−0.0427,−4.9702] | |||
| Feature | rANGVx | rANGx | Motion |
|---|---|---|---|
| Rule 1 | i_rest | i_rest_down | o_rest_down |
| Rule 2 | i_flexion | i_move | o_flexion |
| Rule 3 | i_rest | i_rest_up | o_rest_up |
| Rule 4 | i_extension | i_move | o_extension |
| Rule 5 | i_rest | i_move | null_1 |
| Rule 6 | i_flexion | i_rest_down | null_2 |
| Rule 7 | i_flexion | i_rest_up | null_3 |
| Rule 8 | i_extension | i_rest_down | null_4 |
| Rule 9 | i_extension | i_rest_up | null _5 |
| Exercise | Joint Motion | Adaptable Scheme | Quartile Scheme | ||
|---|---|---|---|---|---|
| 25% | 50% | 75% | |||
| A. flexion-extension | rest_down | 0.9 | 1 | 1 | 1 |
| ext | 0.765 | 0.225 | 1 | 1 | |
| rest_up | 0.51 | 0.4 | 0.55 | 0.283 | |
| flex | 0.96 | 0.941 | 0.966 | 0.975 | |
| average | 0.809 | 0.642 | 0.879 | 0.815 | |
| B. abduction-adduction | rest_low | 0.97 | 1 | 0.967 | 1 |
| ABD | 0.905 | 1 | 1 | 0.8 | |
| rest_half | 0.995 | 1 | 1 | 1 | |
| ADD | 0.863 | 0.866 | 1 | 1 | |
| average | 0.927 | 0.967 | 0.992 | 0.95 | |
| C. external-internal rotation | rest_inside | 1 | 1 | 1 | 1 |
| ER | 0.48 | 1 | 0.408 | 0.025 | |
| rest_outside | 0.52 | 1 | 0.383 | 0.033 | |
| IR | 0.723 | 0.714 | 1 | 0.874 | |
| average | 0.654 | 0.929 | 0.698 | 0.483 | |
| D. pronation-supination | rest_on | 1 | 1 | 1 | 1 |
| pronation | 0.975 | 1 | 0.933 | 0.95 | |
| rest_under | 0.905 | 1 | 1 | 0.7 | |
| supination | 0.78 | 1 | 1 | 0.627 | |
| average | 0.915 | 1 | 0.983 | 0.819 | |
| E. ulnar-radial deviation | rest_right | 0.965 | 1 | 1 | 0.917 |
| ulnar_dev. | 0.7 | 0.833 | 0.767 | 0.433 | |
| rest_left | 0.95 | 1 | 1 | 0.85 | |
| radial_dev. | 0.405 | 0.475 | 0.339 | 0.441 | |
| average | 0.755 | 0.827 | 0.777 | 0.660 | |
| Exercise No. | TP | FN | FP | TN | TPR | FPR | TNR | ACC |
|---|---|---|---|---|---|---|---|---|
| A | 15 | 4 | 0 | 1 | 0.79 | 0 | 1 | 0.8 |
| B | 15 | 1 | 0 | 4 | 0.94 | 0 | 1 | 0.95 |
| C | 5 | 0 | 6 | 9 | 1 | 0.4 | 0.6 | 0.7 |
| D | 15 | 4 | 1 | 0 | 0.79 | 1 | 0 | 0.75 |
| E | 7 | 6 | 0 | 7 | 0.54 | 0 | 1 | 0.7 |
| Average | 0.81 | 0.28 | 0.72 | 0.78 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kan, Y.-C.; Kuo, Y.-C.; Lin, H.-C. Personalized Rehabilitation Recognition for Ubiquitous Healthcare Measurements. Sensors 2019, 19, 1679. https://doi.org/10.3390/s19071679
Kan Y-C, Kuo Y-C, Lin H-C. Personalized Rehabilitation Recognition for Ubiquitous Healthcare Measurements. Sensors. 2019; 19(7):1679. https://doi.org/10.3390/s19071679
Chicago/Turabian StyleKan, Yao-Chiang, Yu-Chieh Kuo, and Hsueh-Chun Lin. 2019. "Personalized Rehabilitation Recognition for Ubiquitous Healthcare Measurements" Sensors 19, no. 7: 1679. https://doi.org/10.3390/s19071679
APA StyleKan, Y. -C., Kuo, Y. -C., & Lin, H. -C. (2019). Personalized Rehabilitation Recognition for Ubiquitous Healthcare Measurements. Sensors, 19(7), 1679. https://doi.org/10.3390/s19071679