Emerging Wireless Sensor Networks and Internet of Things Technologies—Foundations of Smart Healthcare





Abstract
:1. Introduction
Contributions
- An extensive survey on emerging communication standards and technologies suitable for smart healthcare applications is presented. A particular emphasis has been given to the latest IoT standards and technologies. The specific requirements in terms of data rates, latency, and energy efficiency are discussed.
- An overview of security and privacy issues, as the major challenge for future smart healthcare systems, is presented.
- Emerging trends and applications for healthcare are presented. Particular attention is devoted to crowdsourcing/crowdsensing, envisaged as tools for the rapid collection of massive quantities of medical data.
- Finally, open research and technical challenges in designing an IoT system for smart healthcare are discussed.
2. Communication Technologies for WSN-Based Healthcare
2.1. LR-WPAN Standards and Technologies
Advances in LR-WPAN Networking
- Defining a protocol by which adjacent nodes in the network can arrange the addition or removal of cells from the scheduling matrix;
- Defining a 6top function to create a communication schedule; establishing logical links, including procedures to support distributed dynamic scheduling, as well as mechanisms for maintaining communication schedules;
- Mapping the communication schedule to multi-hop routes created by RPL;
- Resource management, that is, adjusting the resources allocated to adjacent nodes;
- Forcing the differentiation, that is, different treatment of data flows generated by the application layer and signal messages used by 6LoWPAN and RPL to detect adjacent nodes, respond to topology changes, and self-configure IP addresses.
2.2. LP-WAN Standards and Technologies
2.2.1. LP-WAN Technologies in Licensed Bands
2.2.2. LP-WAN Technologies in Unlicensed Bands
2.3. Security and Privacy for Smart Healthcare
3. Emerging Trends and Applications in Smart Healthcare
3.1. Application Domains and System Architectures
- Healthcare IoT for Patients provides patients with personalized healthcare utilizing different wearable devices such as activity trackers [79], inertial sensors [80] heart-rate and blood pressure monitoring sensors [81], glucose-level meters [82]. These devices are used to track patient’s healthcare parameters in real-time and even perform local data analysis in addition to storing the historical data in the cloud. Based on these measurements, the patients are given personalized suggestions on how to improve their medical condition, while at the same time potentially life-threatening conditions can be detected on time. This is expected to have a strong impact on people’s lives, especially for those living alone and improve their sense of health security.
- Healthcare IoT for Doctors provides them with timely information about the health conditions of the patient in the hospital. Besides, it also enables them to keep track of the health condition of the patients in the home environment, which was not possible until the advent of healthcare IoT. In addition to the aforementioned benefits, the large amount of collected data regarding the patient’s health condition enables the use of advanced machine learning techniques. These can be used to identify the effectiveness of the treatment, learn more about the illness itself, and monitor its progress.
- Healthcare IoT for Hospitals is expected to propel the further use of IoT in the healthcare field. In particular, by tagging different hospital assets such as defibrillators, respirators, and monitoring equipment, their location can be tracked in real-time. Besides, if the medical staff location is also being tracked, there also exists a possibility to optimize their engagement and easily locate them in the case of an emergency. Finally, the analysis of such data could provide the hospitals with new insights on how to improve the overall organization and use of resources.
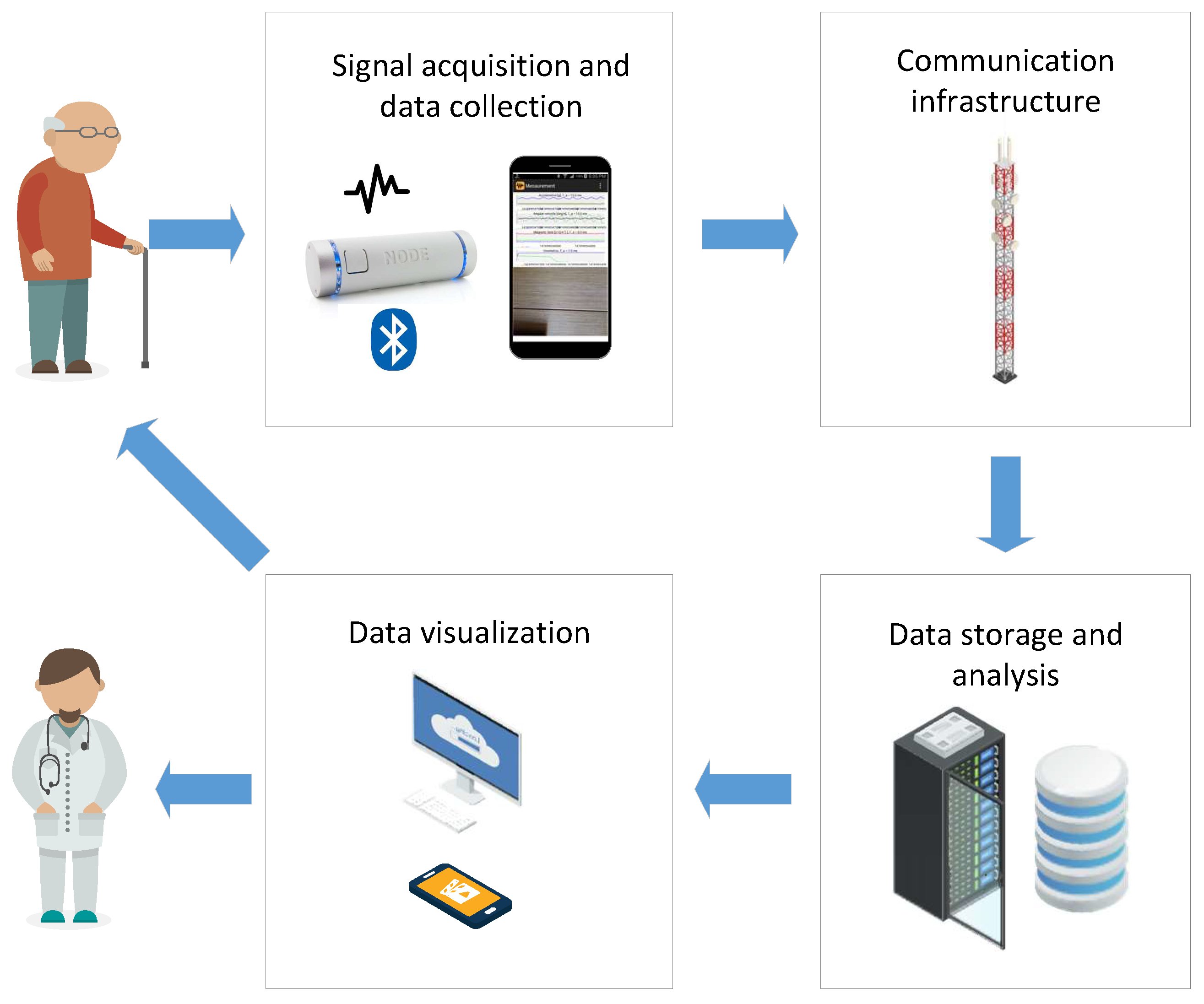
- Signal acquisition and data collection: the goal is to sense and transmit different measurements of patient vital signs, as well as environmental data that may be relevant for the analysis. It usually consists of one or more biomedical sensors such as heart-rate sensors, blood pressure, temperature, and so forth, which send the measurements via a wireless connection to the subsequent data collection unit. The signal acquisition components shall be designed to be portable, non-intrusive, and energy-efficient in order not to interfere much with the patient’s activities and at the same time provide high-quality data about the patient’s health condition. Besides, this block can also perform local pre-processing before sending the data to the main data storage and analysis block. Depending on the availability of internet connection at the given location, this module is usually equipped with mobile, Wi-Fi, or Ethernet connectivity unit.
- Communication infrastructure: aims to transfer the data from the signal acquisition and data collection block to the subsequent data storage and analysis. Depending on the availability of communication networks and the requirements of the underlying data (bit-rate, latency), this block could use cable Internet, Wi-Fi, 4G, and so forth.
- Data storage and analysis: is usually implemented as a cloud server, due to cost-effectiveness, ease of configuration and scalability. Its main purpose is to collect and store data from different data collection units deployed in the patient’s home, perform data analysis by using different signal processing and ML algorithms, and enable access to such data by different users. In addition, strong security mechanisms (data encryption, secure communication, access control) shall be enforced. This is to ensure data privacy protection and prevent any possible misuse of highly sensitive healthcare data.
- Data visualization: represents the final block which is in charge of communication of the results of the analysis towards the end-user. This block is usually implemented as a web, desktop or mobile application, which may be aimed at either healthcare practitioners or the patient itself. In such a way, the patient is informed about its healthcare condition in a timely manner. This component shall be implemented having in mind best practices in user interface design and usability, to ease adoption by the end-users.
3.2. Crowdsourcing/Crowdsensing for Healthcare Applications
4. Technical Challenges in Smart Healthcare
4.1. Designing IoT for Smart Healthcare
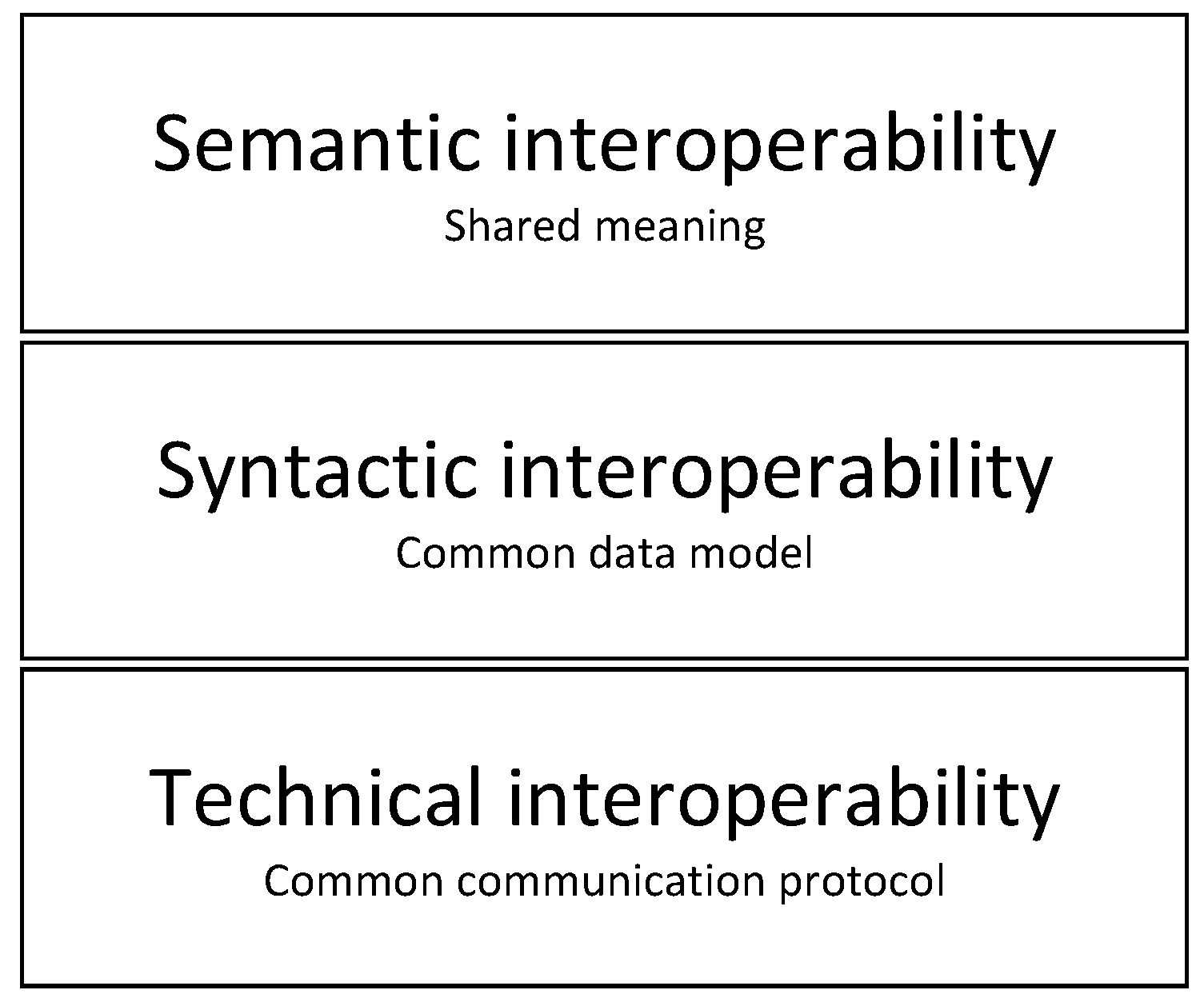
- Technical interoperability layer ensures that systems use common communications channels and protocols (e.g., ZigBee, NB-IoT, LoRaWAN, etc.). This layer represents the lowest level of interoperability which is required to facilitate minimal interoperability conditions. Usually, TCP/IP is used as a common solution for technical interoperability. However, in constrained applications where energy consumption has to be reduced, other more energy-efficient protocols are used.
- Syntactic interoperability layer further builds on the previous layer by ensuring that a common data format is used for the exchange of messages between different systems. At this interoperability layer, two or more systems can interpret the content of exchanged messages.
- Semantic interoperability layer ensures that the meaning of the data is represented semantically, categorized and linked to other semantic data. This layer ensures that systems can combine received information with other information sources.
4.2. Crowdsensing/Crowdsourcing Challenges
5. Conclusions
- Interconnection: The ability to enable the efficient and reliable interconnection of network devices, sensors, and people within a single communication infrastructure. Interconnection provides the collection of data from all parts of the healthcare system, thus offering the required functionality and identification of possible system improvements and innovations.
- Information transparency: Transparency should provide operators with access to relevant information needed to make timely and reliable decisions.
- Technical assistance: The system should have the ability to aggregate and visualize information in order to solve problems in a short time.
- Intelligent decision-making: A real-time and interactive decision-making IoMT system should provide accurate diagnosis and treatment services, data fusion from multiple sources, and multimodal ML-based decision-making engines.
- Safety and Security: The ability to deliver highly secure networks that will ensure the safety and privacy of the patients. This will require to employ new design paradigms based on well-founded security practices to build trustworthy systems. Designers must consider security at the very early stages of the design of smart healthcare systems.
- Development of advanced API models, such as REpresentational State Transfer (REST) scalable architecture.
- Innovative cloud platforms that provide efficient extraction of data context and decision making.
- Artificial intelligence, big data, and cognitive systems in the processing of large amounts of data.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| API | Application Programming Interface |
| BAN | Body Area Network |
| CoAP | Constrained Application Protocol |
| COTS | Commercial Off-The-Shelf |
| CP-ABE | Ciphertext-Policy Attribute-Based Encryption |
| CSMA/CA | Carrier Sense Multiple Access/Collision Avoidance |
| DBPSK | Differential Binary Phase-Shift Keying |
| DL | Downlink |
| DSSS | Direct Sequence Spread Spectrum |
| EC-GSM-IoT | Extended Coverage – GSM – Internet of Things |
| ECG | Electrocardiogram |
| EEG | Electroencephalogram |
| EGPRS | Enhanced General Packet Radio Service |
| EHR | Electronic Health Records |
| EMG | Electromyogram |
| FDA | Food and Drug Administration |
| FDMA | Frequency Division Multiple Access |
| FHSS | Frequency Hopping Spread Spectrum |
| FSK | Frequency Shift Keying |
| GFSK | Gaussian Frequency Shift Keying |
| HBC | Human Body Communications |
| IoT | Internet of Things |
| IoMT | Internet of Medical Things |
| IMD | Implantable Medical Devices |
| ISM | Industrial, Scientific and Medical |
| LECIM | Low-Energy Critical Infrastructure Monitoring |
| LLN | Low-power and Lossy Networks |
| LDPC | Low Density Parity Check |
| LoRaWAN | Long Range Wider Area Network |
| LP-WAN | Low Power Wide Area Network |
| LR-WPAN | Low Rate - Wireless Personal Area Network |
| LTE CAT-N | Long Term Evolution Category N |
| LTE-M | Long Term Evolution - Machine Type Communications |
| MAC | Medium Access Control |
| MITM | Man-In-The-Middle |
| MCS | Mobile Crowdsensing |
| MTC | Machine Type Communications |
| NB-IoT | Narrow Band Internet of Things |
| NFC | Near Field Communication |
| OFDM | Orthogonal Frequency Division Multiplexing |
| OTA | Over-the-Air |
| PER | Packet Error Rate |
| PSK | Phase Shift Keying |
| RAW | Restricted Access Window |
| QC | Quantum Computing |
| QKD | Quantum Key Distribution |
| QoI | Quality of Information |
| QoS | Quality of Service |
| QPSK | Quadrature Phase shift Keying |
| QRNG | Quantum Random Number Generator |
| REST | REpresentational State Transfer |
| RFD | Radio Frequency |
| RFD | Radio Frequency Identification |
| PASH | Privacy-Aware Smart Health |
| RHM | Remote Health Monitoring |
| RPMA | Random Phase Multiple Access |
| RPL | Routing Protocol for Low-Power and Lossy Networks |
| SDN | Software-Defined Networking |
| SHR | Smart Health Record |
| SpO2 | Oxygen Saturation |
| SRD | Short Range Device |
| TDMA | Time Division Multiple Access |
| TSCH | Time-Slotted Channel Hopping |
| UL | Uplink |
| UWB | Ultra-WideBand |
| WBAN | Wireless Body Area Network |
| WMDs | Wearable Medical Devices |
| WSN | Wireless Sensor Network |
| 6LoWPAN | IPv6 over Low - Power Wireless Personal Area Networks |
| 6TiSCH | IPv6 over the TSCH |
References
- World Population Prospects 2019. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf (accessed on 22 April 2020).
- Wolff, J.L.; Jacobs, B.J. Chapter 7—Chronic Illness Trends and the Challenges to Family Caregivers: Organizational and Health System Barriers. In Family Caregiving in the New Normal; Gaugler, J.E., Kane, R.L., Eds.; Academic Press: San Diego, CA, USA, 2015; pp. 79–103. [Google Scholar] [CrossRef]
- Muhammed, T.; Mehmood, R.; Albeshri, A.; Katib, I. UbeHealth: A Personalized Ubiquitous Cloud and Edge-Enabled Networked Healthcare System for Smart Cities. IEEE Access 2018, 6, 32258–32285. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, L.; Song, H.; Cao, X. Ubiquitous WSN for Healthcare: Recent Advances and Future Prospects. IEEE Internet Things J. 2014, 1, 311–318. [Google Scholar] [CrossRef]
- Alam, M.M.; Malik, H.; Khan, M.I.; Pardy, T.; Kuusik, A.; Le Moullec, Y. A Survey on the Roles of Communication Technologies in IoT-Based Personalized Healthcare Applications. IEEE Access 2018, 6, 36611–36631. [Google Scholar] [CrossRef]
- Habibzadeh, H.; Dinesh, K.; Rajabi Shishvan, O.; Boggio-Dandry, A.; Sharma, G.; Soyata, T. A Survey of Healthcare Internet of Things (HIoT): A Clinical Perspective. IEEE Internet Things J. 2020, 7, 53–71. [Google Scholar] [CrossRef]
- Baker, S.B.; Xiang, W.; Atkinson, I. Internet of Things for Smart Healthcare: Technologies, Challenges, and Opportunities. IEEE Access 2017, 5, 26521–26544. [Google Scholar] [CrossRef]
- Wu, T.; Wu, F.; Redouté, J.; Yuce, M.R. An Autonomous Wireless Body Area Network Implementation Towards IoT Connected Healthcare Applications. IEEE Access 2017, 5, 11413–11422. [Google Scholar] [CrossRef]
- IEEE Standard for Local and Metropolitan Area Networks—Part 15.6: Wireless Body Area Networks; IEEE Std 802.15.6-2012; IEEE: Piscataway, NJ, USA, 2012; pp. 1–271.
- Movassaghi, S.; Abolhasan, M.; Lipman, J.; Smith, D.; Jamalipour, A. Wireless Body Area Networks: A Survey. IEEE Commun. Surv. Tutor. 2014, 16, 1658–1686. [Google Scholar] [CrossRef]
- Darroudi, S.M.; Gomez, C.; Crowcroft, J. Bluetooth Low Energy Mesh Networks: A Standards Perspective. IEEE Commun. Mag. 2020, 58, 95–101. [Google Scholar] [CrossRef]
- Liu, X.; Yin, J.; Liu, Y.; Zhang, S.; Guo, S.; Wang, K. Vital Signs Monitoring with RFID: Opportunities and Challenges. IEEE Netw. 2019, 33, 126–132. [Google Scholar] [CrossRef]
- Jara, A.J.; Lopez, P.; Fernandez, D.; Zamora, M.A.; Ubeda, B.; Skarmeta, A.F. Communication Protocol for Enabling Continuous Monitoring of Elderly People through Near Field Communications. Interact. Comput. 2014, 26, 145–168. [Google Scholar] [CrossRef]
- Elsts, A.; Fafoutis, X.; Woznowski, P.; Tonkin, E.; Oikonomou, G.; Piechocki, R.; Craddock, I. Enabling Healthcare in Smart Homes: The SPHERE IoT Network Infrastructure. IEEE Commun. Mag. 2018, 56, 164–170. [Google Scholar] [CrossRef]
- Ugrenovic, D.; Gardasevic, G. CoAP protocol for Web-based monitoring in IoT healthcare applications. In Proceedings of the 2015 23rd Telecommunications Forum Telfor (TELFOR), Belgrade, Serbia, 25 November 2015; pp. 79–82. [Google Scholar]
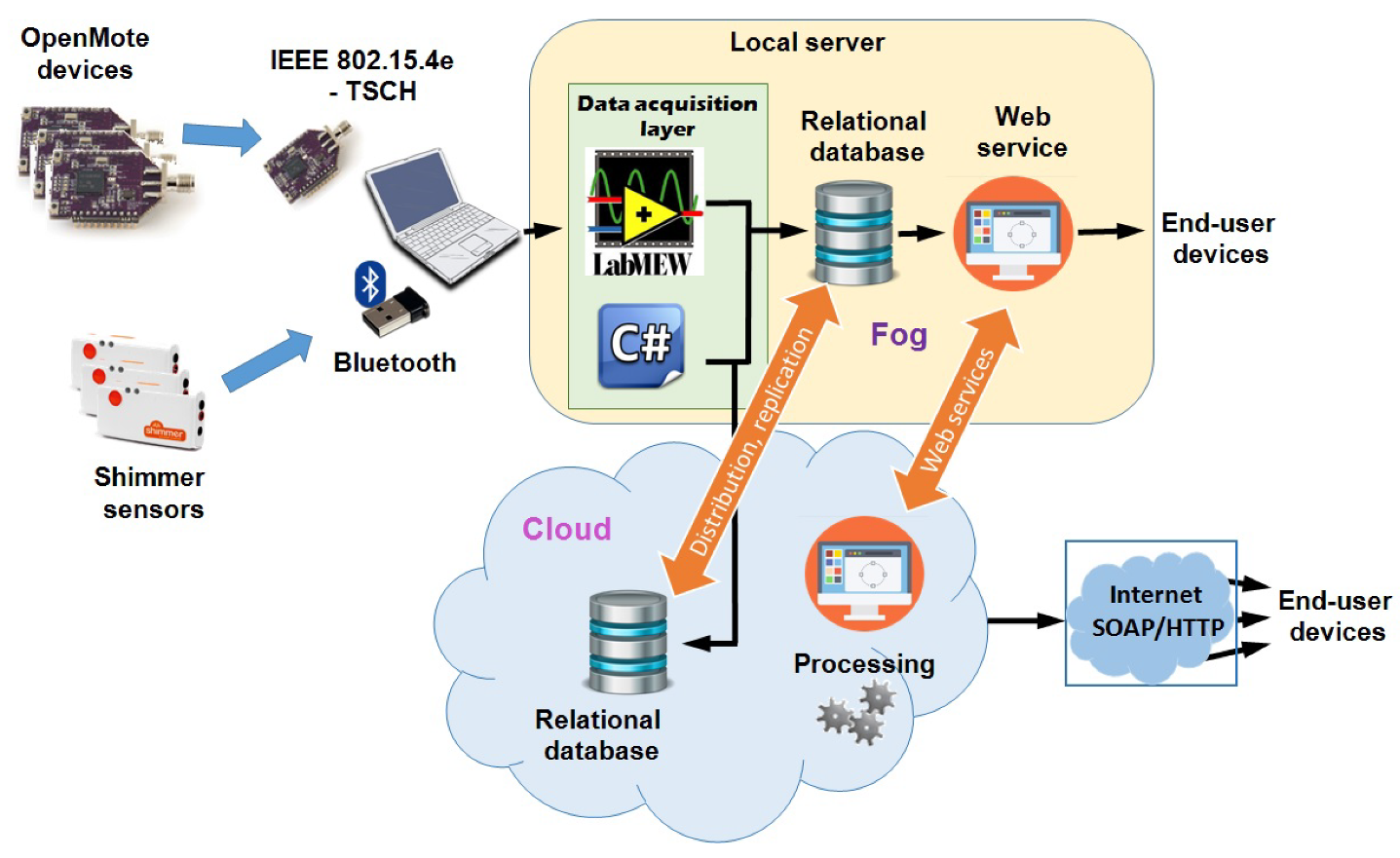
- Gardašević, G.; Fotouhi, H.; Tomasic, I.; Vahabi, M.; Björkman, M.; Lindén, M. A Heterogeneous IoT-Based Architecture for Remote Monitoring of Physiological and Environmental Parameters. In Internet of Things (IoT) Technologies for HealthCare; Ahmed, M.U., Begum, S., Fasquel, J.B., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 48–53. [Google Scholar]
- IEEE Standard for Information Technology—Telecommunications and Information Exchange between Systems—Local and Metropolitan Area Networks—Specific Requirements—Part 11: Wireless LAN Medium Access Control (MAC) and Physical Layer (PHY) Specifications Amendment 2: Sub 1 GHz License Exempt Operation; IEEE Std 802.11ah-2016; IEEE: Piscataway, NJ, USA, 2017; pp. 1–594.
- Raza, U.; Kulkarni, P.; Sooriyabandara, M. Low Power Wide Area Networks: An Overview. IEEE Commun. Surv. Tutor. 2017, 19, 855–873. [Google Scholar] [CrossRef] [Green Version]
- Hadi, M.S.; Lawey, A.Q.; El-Gorashi, T.E.H.; Elmirghani, J.M.H. Patient-Centric Cellular Networks Optimization Using Big Data Analytics. IEEE Access 2019, 7, 49279–49296. [Google Scholar] [CrossRef]
- IEEE Standard for Low-Rate Wireless Networks; IEEE Std 802.15.4-2015; IEEE: Piscataway, NJ, USA, 2016; pp. 1–709.
- García Algora, C.M.; Alfonso Reguera, V.; Deligiannis, N.; Steenhaut, K. Review and Classification of Multichannel MAC Protocols for Low-Power and Lossy Networks. IEEE Access 2017, 5, 19536–19561. [Google Scholar] [CrossRef]
- Gardasevic, G.; Mijovic, S.; Stajkic, A.; Buratti, C. On the performance of 6LoWPAN through experimentation. In Proceedings of the 2015 International Wireless Communications and Mobile Computing Conference (IWCMC), Dubrovnik, Croatia, 24 August 2015; pp. 696–701. [Google Scholar]
- Gardasevic, G.; Plavsic, P.; Vasilievic, D. Experimental IoT Testbed for Testing the 6TiSCH and RPL Coexistence. In Proceedings of the IEEE INFOCOM 2019—IEEE Conference on Computer Communications Workshops (INFOCOM WKSHPS), Paris, France, 2 May 2019; pp. 917–918. [Google Scholar]
- Torabi, N.; Rostamzadeh, K.; Leung, V.C.M. IEEE 802.15.4 Beaconing Strategy and the Coexistence Problem in ISM Band. IEEE Trans. Smart Grid 2015, 6, 1463–1472. [Google Scholar] [CrossRef]
- ZigBee Specifications. Available online: https://zigbeealliance.org/solution/zigbee/ (accessed on 12 April 2012).
- Bluetooth Core Specification, Version 4.0, SIG. Available online: https://www.bluetooth.com/specifications/archived-specifications/ (accessed on 26 April 2020).
- Bluetoth 5.0 Specifications. Available online: https://www.bluetooth.com/wp-content/uploads/2019/03/Bluetooth_5-FINAL.pdf (accessed on 9 April 2020).
- Cai, G.; Fang, Y.; Wen, J.; Han, G.; Yang, X. QoS-Aware Buffer-Aided Relaying Implant WBAN for Healthcare IoT: Opportunities and Challenges. IEEE Netw. 2019, 33, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Viegas, V.; Postolache, O.; Dias Pereira, J. Transducer Electronic Data Sheets: Anywhere, Anytime, Anyway. Electronics 2019, 8, 1345. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.Y.; Wang, Y.; Barrett, M.; Dobkin, B.; Pottie, G.J.; Kaiser, W.J. Personalized Multilayer Daily Life Profiling Through Context Enabled Activity Classification and Motion Reconstruction: An Integrated System Approach. IEEE J. Biomed. Health Inform. 2016, 20, 177–188. [Google Scholar] [CrossRef]
- Khanafer, M.; Guennoun, M.; Mouftah, H.T. A Survey of Beacon-Enabled IEEE 802.15.4 MAC Protocols in Wireless Sensor Networks. IEEE Commun. Surv. Tutor. 2014, 16, 856–876. [Google Scholar] [CrossRef]
- Quintero, V.L.; Estevez, C.; Orchard, M.E.; Pérez, A. Improvements of Energy-Efficient Techniques in WSNs: A MAC-Protocol Approach. IEEE Commun. Surv. Tutor. 2019, 21, 1188–1208. [Google Scholar] [CrossRef]
- Guntupalli, L.; Ghose, D.; Li, F.Y.; Gidlund, M. Energy Efficient Consecutive Packet Transmissions in Receiver-Initiated Wake-Up Radio Enabled WSNs. IEEE Sens. J. 2018, 18, 4733–4745. [Google Scholar] [CrossRef]
- Peng, M.; Liu, W.; Wang, T.; Zeng, Z. Relay Selection Joint Consecutive Packet Routing Scheme to Improve Performance for Wake-Up Radio-Enabled WSNs. Wirel. Commun. Mob. Comput. 2020, 2020, 1–32. [Google Scholar] [CrossRef]
- IEEE Standard for Local and Metropolitan Area Networks—Part 15.4: Low-Rate Wireless Personal Area Networks (LR-WPANs) Amendment 1: MAC Sublayer; IEEE Std 802.15.4e-2012; IEEE: Piscataway, NJ, USA, 2012; pp. 1–225.
- Elsts, A.; Fafoutis, X.; Oikonomou, G.; Piechocki, R.; Craddock, I. TSCH Networks for Health IoT: Design, Evaluation and Trials in the Wild. ACM Transactions on Internet of Things. ACM Trans. Internet Things 2020, 1. [Google Scholar] [CrossRef] [Green Version]
- Vilajosana, X.; Watteyne, T.; Chang, T.; Vučinić, M.; Duquennoy, S.; Thubert, P. IETF 6TiSCH: A Tutorial. IEEE Commun. Surv. Tutor. 2020, 22, 595–615. [Google Scholar] [CrossRef]
- Vucinic, M.; Pejanovic-Djurisic, M.; Watteyne, T. SODA: 6TiSCH Open Data Action. In Proceedings of the 2018 IEEE Workshop on Benchmarking Cyber-Physical Networks and Systems (CPSBench), Porto, Portugal, 13 April 2018; pp. 42–46. [Google Scholar]
- Vučinić, M.; Chang, T.; Škrbić, B.; Kočan, E.; Pejanović-Djurišić, M.; Watteyne, T. Key Performance Indicators of the Reference 6TiSCH Implementation in Internet-of-Things Scenarios. IEEE Access 2020, 8, 79147–79157. [Google Scholar] [CrossRef]
- IEEE Standard for Local and Metropolitan Area Networks—Part 15.4: Low-Rate Wireless Personal Area Networks (LR-WPANs) Amendment 3: Physical Layer (PHY) Specifications for Low-Data-Rate, Wireless, Smart Metering Utility Networks; IEEE Std 802.15.4g-2012; IEEE: Piscataway, NJ, USA, 2012; pp. 1–252.
- IEEE Standard for Local and Metropolitan Area Networks—Part 15.4: Low-Rate Wireless Personal Area Networks (LR-WPANs)—Amendment 5: Physical Layer Specifications for Low Energy, Critical Infrastructure Monitoring Networks; IEEE Std 802.15.4k-2013; IEEE: Piscataway, NJ, USA, 2013; pp. 1–149.
- Vilajosana, X.; Tuset, P.; Watteyne, T.; Pister, K. OpenMote: Open-Source Prototyping Platform for the Industrial IoT. In Ad Hoc Networks; Mitton, N., Kantarci, M.E., Gallais, A., Papavassiliou, S., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 211–222. [Google Scholar]
- Salahuddin, M.A.; Al-Fuqaha, A.; Guizani, M.; Shuaib, K.; Sallabi, F. Softwarization of Internet of Things Infrastructure for Secure and Smart Healthcare. Computer 2017, 50, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Meng, Y.; Huang, Z.; Shen, G.; Ke, C. SDN-Based Security Enforcement Framework for Data Sharing Systems of Smart Healthcare. IEEE Trans. Netw. Serv. Manag. 2020, 17, 308–318. [Google Scholar] [CrossRef]
- Tomovic, S.; Lekic, N.; Radusinovic, I.; Gardasevic, G. A new approach to dynamic routing in SDN networks. In Proceedings of the 2016 18th Mediterranean Electrotechnical Conference (MELECON), Limassol, Cyprus, 20 April 2016; pp. 1–6. [Google Scholar]
- Tsapardakis, E.; Ojo, M.; Chatzimisios, P.; Giordano, S. Performance Evaluation of SDN and RPL in Wireless Sensor Networks. In Proceedings of the 2018 Global Information Infrastructure and Networking Symposium (GIIS), Paris, France, 18 December 2018; pp. 1–5. [Google Scholar]
- Alnoman, A.; Sharma, S.K.; Ejaz, W.; Anpalagan, A. Emerging Edge Computing Technologies for Distributed IoT Systems. IEEE Netw. 2019, 33, 140–147. [Google Scholar] [CrossRef]
- Tang, W.; Zhang, K.; Zhang, D.; Ren, J.; Zhang, Y.; Shen, X. Fog-Enabled Smart Health: Toward Cooperative and Secure Healthcare Service Provision. IEEE Commun. Mag. 2019, 57, 42–48. [Google Scholar] [CrossRef]
- Shen, W.; Yin, B.; Liu, L.; Cao, X.; Cheng, Y.; Li, Q.; Wang, W. Secure In-Band Bootstrapping for Wireless Personal Area Networks. IEEE Internet Things J. 2016, 3, 1385–1394. [Google Scholar] [CrossRef]
- Sanchez-Iborra, R.; Cano, M.D. State of the Art in LP-WAN Solutions for Industrial IoT Services. Sensors 2016, 16, 708. [Google Scholar] [CrossRef] [PubMed]
- Elsaadany, M.; Ali, A.; Hamouda, W. Cellular LTE-A Technologies for the Future Internet-of-Things: Physical Layer Features and Challenges. IEEE Commun. Surv. Tutor. 2017, 19, 2544–2572. [Google Scholar] [CrossRef]
- Lavric, A.; Popa, V. Performance Evaluation of LoRaWAN Communication Scalability in Large-Scale Wireless Sensor Networks. Wirel. Commun. Mob. Comput. 2018, 2018, 6730719. [Google Scholar] [CrossRef] [Green Version]
- Petajajarvi, J.; Mikhaylov, K.; Roivainen, A.; Hanninen, T.; Pettissalo, M. On the coverage of LPWANs: Range evaluation and channel attenuation model for LoRa technology. In Proceedings of the 2015 14th International Conference on ITS Telecommunications (ITST), Copenhagen, Denmark, 2–4 December 2015; pp. 55–59. [Google Scholar]
- Haxhibeqiri, J.; De Poorter, E.; Moerman, I.; Hoebeke, J. A survey of LoRaWAN for IoT: From technology to application. Sensors 2018, 18, 3995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Iborra, R.; Sanchez-Gomez, J.; Santa, J.; Fernández, P.J.; Skarmeta, A. Integrating LP-WAN Communications within the Vehicular Ecosystem. In Proceedings of the 2017 International Symposium on Mobile Internet Security (MobiSec’17), Jeju Island, Korea, 19 October 2017. [Google Scholar]
- Olatinwo, D.D.; Abu-Mahfouz, A.; Hancke, G. A Survey on LPWAN Technologies in WBAN for Remote Health-Care Monitoring. Sensors 2019, 19, 5268. [Google Scholar] [CrossRef] [Green Version]
- WEIGHTLESS Website. Available online: http://www.weightless.org/ (accessed on 30 April 2020).
- Goursaud, C.; Gorce, J.M. Dedicated networks for IoT: PHY / MAC state of the art and challenges. EAI Endorsed Trans. Internet Things 2015. [Google Scholar] [CrossRef]
- Standards News. IEEE Commun. Stand. Mag. 2018, 2, 12–17. [CrossRef]
- Patel, M.; Wang, J. Applications, challenges, and prospective in emerging body area networking technologies. IEEE Wirel. Commun. 2010, 17, 80–88. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Q. Body Area Communications: Channel Modeling, Communication Systems, and EMC; Wiley: Hoboken, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, J.; Zhao, G. Towards 5G Enabled Tactile Robotic Telesurgery. arXiv 2018, arXiv:1803.03586. [Google Scholar]
- Rezaei, F.; Pradhumna, L.S.; Hempel, M.; Sushanta, M.R.; Sharif, H. Covert Communication in Wireless Sensor Networks for E-Health Applications; Technological Breakthroughs in Modern Wireless Sensor Applications; IGI Global: Hershey, PA, USA, 2015; pp. 352–371. [Google Scholar] [CrossRef] [Green Version]
- Zeng, F.G.; Rebscher, S.; Harrison, W.; Sun, X.; Feng, H. Cochlear implants: System design, integration, and evaluation. IEEE Rev. Biomed. Eng. 2008, 1, 115–142. [Google Scholar] [CrossRef] [Green Version]
- ULLAH, S.; KHAN, P.; ULLAH, N.; SALEEM, S.; HIGGINS, H.; Sup KWAK, K. A Review of Wireless Body Area Networks for Medical Applications. Int. J. Commun. Netw. Syst. Sci. 2009. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Zhu, J.; Wang, X.; Hanzo, L. A Survey on Wireless Security: Technical Challenges, Recent Advances, and Future Trends. Proc. IEEE 2016, 104, 1727–1765. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Jin, H.; Nahrstedt, K. WritingHacker: Audio based eavesdropping of handwriting via mobile devices. In Proceedings of the UbiComp 2016—Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Heidelberg, Germany, 12 September 2016. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Jin, H.; Nahrstedt, K. Mobile Devices based Eavesdropping of Handwriting. IEEE Trans. Mob. Comput. 2019, 19, 1649–1663. [Google Scholar] [CrossRef]
- Solanas, A.; Patsakis, C.; Conti, M.; Vlachos, I.S.; Ramos, V.; Falcone, F.; Postolache, O.; Perez-martinez, P.A.; Pietro, R.D.; Perrea, D.N.; et al. Smart health: A context-aware health paradigm within smart cities. IEEE Commun. Mag. 2014, 52, 74–81. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, D.; Deng, R.H. Security and Privacy in Smart Health: Efficient Policy-Hiding Attribute-Based Access Control. IEEE Internet Things J. 2018, 5, 2130–2145. [Google Scholar] [CrossRef]
- Katzis, K.; Jones, R.; Despotou, G. The challenges of balancing safety and security in implantable medical devices. Stud. Health Technol. Inform. 2016, 226. [Google Scholar] [CrossRef]
- Sun, W.; Cai, Z.; Li, Y.; Liu, F.; Fang, S.; Wang, G. Security and Privacy in the Medical Internet of Things: A Review. Secur. Commun. Netw. 2018, 2018, 5978636. [Google Scholar] [CrossRef]
- Esposito, C.; Castiglione, A.; Tudorica, C.; Pop, F. Security and privacy for cloud-based data management in the health network service chain: A microservice approach. IEEE Commun. Mag. 2017, 55, 102–108. [Google Scholar] [CrossRef]
- Finkle, J. FDA warns of security flaw in Hospira infusion pumps. Technol. News Reuters. 2015. Available online: https://www.reuters.com/article/us-hospira-fda-cybersecurity/fda-warns-of-security-flaw-in-hospira-infusion-pumps-idUSKCN0Q52GJ20150731 (accessed on 20 April 2020).
- FDA. Firmware Update to Address Cybersecurity Vulnerabilities Identified in Abbott’s (Formerly St. Jude Medical’s) Implantable Cardiac Pacemakers: FDA Safety Communication. 2017. Available online: https://www.fda.gov/medical-devices/safety-communications/firmware-update-address-cybersecurity-vulnerabilities-identified-abbotts-formerly-st-jude-medicals (accessed on 20 April 2020).
- Camara, C.; Peris-Lopez, P.; Tapiador, J.E. Security and privacy issues in implantable medical devices: A comprehensive survey. J. Biomed. Inform. 2015, 55, 272–289. [Google Scholar] [CrossRef] [Green Version]
- Lewis, A.M.; Travagnin, M. A Secure Quantum Communications Infrastructure for Europe; JRC Technical Papers; JRC: Ispra, Italy, 2019. [Google Scholar]
- Cavaliere, F.; Prati, E.; Poti, L.; Muhammad, I.; Catuogno, T. Secure Quantum Communication Technologies and Systems: From Labs to Markets. Quantum Rep. 2020, 20, 7. [Google Scholar] [CrossRef] [Green Version]
- Salvi, E.; Bosoni, P.; Tibollo, V.; Kruijver, L.; Calcaterra, V.; Sacchi, L.; Bellazzi, R.; Larizza, C. Patient-Generated Health Data Integration and Advanced Analytics for Diabetes Management: The AID-GM Platform. Sensors 2020, 20, 128. [Google Scholar] [CrossRef] [Green Version]
- Berbakov, L.; Jovanović, C.; Svetel, M.; Vasiljević, J.; Dimić, G.; Radulović, N. Quantitative Assessment of Head Tremor in Patients with Essential Tremor and Cervical Dystonia by Using Inertial Sensors. Sensors 2019, 19, 4246. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.D.; Liu, J.K.; Wen, B.; He, Q.Y.; Li, Y.; Miao, F. Cuffless Blood Pressure Estimation Using Pressure Pulse Wave Signals. Sensors 2018, 18, 4227. [Google Scholar] [CrossRef] [Green Version]
- Bertachi, A.; Viñals, C.; Biagi, L.; Contreras, I.; Vehí, J.; Conget, I.; Giménez, M. Prediction of Nocturnal Hypoglycemia in Adults with Type 1 Diabetes under Multiple Daily Injections Using Continuous Glucose Monitoring and Physical Activity Monitor. Sensors 2020, 20, 1705. [Google Scholar] [CrossRef] [Green Version]
- Kitchin, R. Big Data, new epistemologies and paradigm shifts. Big Data Soc. 2014, 2014, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Pastorino, R.; De Vito, C.; Migliara, G.; Glocker, K.; Binenbaum, I.; Ricciardi, W.; Boccia, S. Benefits and challenges of Big Data in healthcare: An overview of the European initiatives. Eur. J. Public Health 2019, 29, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Dash, S.; Shakyawar, S.K.; Sharma, M.; Kaushik, S. Big data in healthcare: Management, analysis and future prospects. J. Big Data 2019, 6, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Howe, J. The Rise of Crowdsourcing. Wired Mag. 2006, 14, 1–4. [Google Scholar]
- Ranard, B.; Ha, Y.; Meisel, Z.F.; Asch, D.A.; Hill, S.S.; Becker, L.B.; Seymour, A.K.; Merchant, R.M. Crowdsourcing—Harnessing the Masses to Advance Health and Medicine, a Systematic Review. J. Gen. Intern. Med. 2014, 29, 187–203. [Google Scholar] [CrossRef]
- Wazny, K. “Crowdsourcing” ten years in: A review. J. Glob. Health 2017, 7, 1–19. [Google Scholar] [CrossRef]
- Wazny, K. Applications of crowdsourcing in health: An overview. J. Glob. Health 2018, 8, 1–20. [Google Scholar] [CrossRef]
- Créquit, P.; Mansouri, G.; Benchoufi, M.; Vivot, A.; Ravaud, P. Mapping of Crowdsourcing in Health: Systematic Review. J. Med. Internet Res. 2018, 20, e187:1–e187:23. [Google Scholar]
- Wang, J.; Wang, L.; Wang, Y.; Zhang, D.; Kong, L. Task Allocation in Mobile Crowd Sensing: State-of-the-Art and Future Opportunities. IEEE Internet Things J. 2018, 5, 3747–3757. [Google Scholar] [CrossRef] [Green Version]
- Skoric, T.; Mohamoud, O.; Milovanovic, B.; Japundzic-Zigon, N.; Bajic, D. Binarized cross-approximate entropy in crowdsensing environment. Comput. Biol. Med. 2017, 80, 137–147. [Google Scholar] [CrossRef]
- Tan, J.; Liu, W.; Wang, T.; Zhao, M.; Liu, A.; Zhang, S. A high-accurate content popularity prediction computational modeling for mobile edge computing using matrix completion technology. Trans. Emerg. Telecommun. Technol. 2020, 2020, e3871. [Google Scholar] [CrossRef]
- Ganti, R.; Ye, F.; Lei, H. Mobile crowdsensing: Current state and future challenges. IEEE Commun. Mag. 2011, 49, 32–39. [Google Scholar] [CrossRef]
- Jovanovic, S.; Jovanovic, M.; Skoric, T.; Jokic, S.; Milovanovic, B.; Katzis, K.; Bajic, D. A Mobile Crowd Sensing Application for Hypertensive Patients. Sensors 2019, 2019, 400. [Google Scholar] [CrossRef] [Green Version]
- Tokosi, T.O.; Scholtz, B.M. A Classification Framework of Mobile Health CrowdSensing Research: A Scoping Review. In Proceedings of the ACM SAICSIT Conference (SAICSIT’19), Skukuza, South Africa, 17–18 September 2019; Volume 2019, pp. 1–12. [Google Scholar] [CrossRef]
- Mehdi, M.; Mahlmeier, G.; Agrawal, K.; Pryss, R.; Reichert, M.; Hauck, F. Referenceable mobile crowdsensing architecture: A healthcare use case. Procedia Comput. Sci. 2018, 34, 445–451. [Google Scholar] [CrossRef]
- Jaimes, L.G.; Steele, R. Incentivization for health crowdsensing. In Proceedings of the IEEE 15th International Conference on Dependable, Autonomic and Secure Computing, Orlando, FL, USA, 6–10 November 2017; Volume 2017. [Google Scholar] [CrossRef]
- Jin, H.; Su, L.; Chen, D.; Nahrstedt, K.; Xu, J. Quality of information aware incentive mechanisms for mobile crowd sensing systems. In Proceedings of the 16th ACM International Symposium on Mobile Ad Hoc Networking and Computing, MobiHoc ’15, Hangzhou, China, 22–25 June 2015; Volume 2015, pp. 167–176. [Google Scholar] [CrossRef]
- Influxdata TICK Stack. Available online: https://www.influxdata.com/time-series-platform/ (accessed on 30 April 2012).
- Pryss, R.; Editors Baumeister, H.; Montag, C.E. Mobile Crowdsensing in Healthcare Scenarios: Taxonomy, Conceptual Pillars, Smart Mobile Crowdsensing Services, in: Digital Phenotyping and Mobile Sensing. In Digital Phenotyping and Mobile Sensing; Springer: Berlin, Germany, 2019; pp. 221–234. [Google Scholar] [CrossRef]
- McCartney, P. Crowdsourcing in Healthcare. MCN Am. J. Matern. Nurs. 2013, 38, 392. [Google Scholar] [CrossRef]
- Wang, W.; Huang, H.; Wu, Y.; Huang, Q. Cryptanalysis and Improvement of an Anonymous Batch Verification Scheme for Mobile Healthcare Crowd Sensing. IEEE Accessl 2019, 7, 165842–165851. [Google Scholar] [CrossRef]
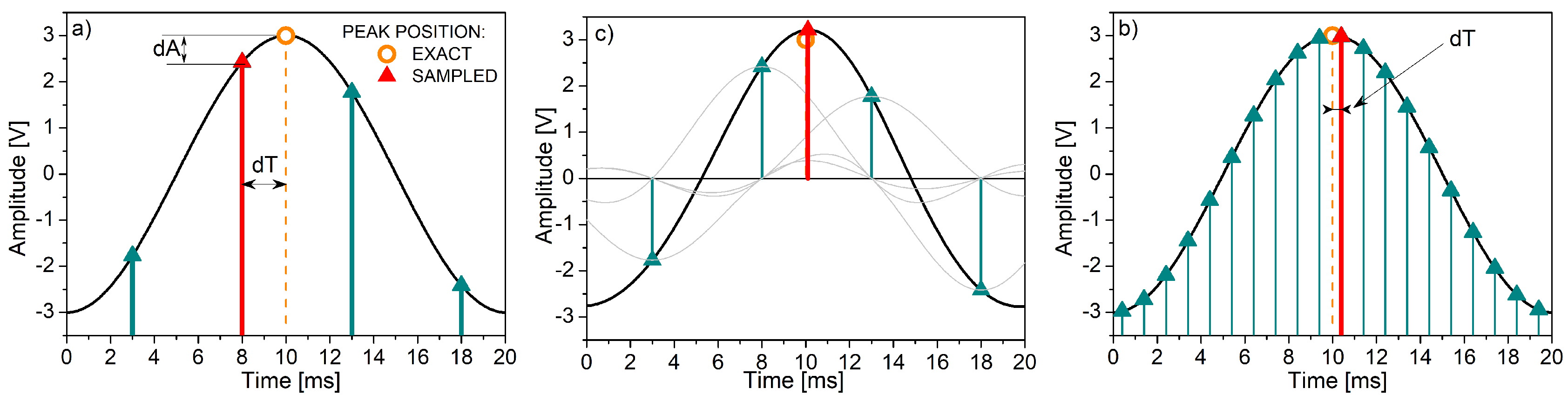
- Shannon, C. Communication in the presence of noise. Proc. Inst. Radio Eng. 1949, 37, 10–21. [Google Scholar] [CrossRef]
- Jelinek, H.F.; Cornforth, D.J.; Khandoker, A.H. ECG Time Series Variability Analysis - Engineering and Medicine; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2016. [Google Scholar] [CrossRef]
- Camm, J.; Marek, M. Heart rate variability. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Wessel, N.; Malberg, H.; Bauernschmitt, R.; Kurths, J. Nonlinear methods of cardiovascular physics and their clinical applicability. Int. J. Bifurc. Chaos 2007, 17, 3325–3371. [Google Scholar] [CrossRef] [Green Version]
- Tarvainen, M.; Ranta-aho, P.; Karjalainen, P. An advanced detrending approach with application to HRV analysis. IEEE Trans. Biomed. Eng. 2002, 49, 172–174. [Google Scholar] [CrossRef]
- Bajic, D.; Loncar, T.; Milovanovic, B. Biomedical Signals in BANs: Pre-Channel Issues. In Proceedings of the European Wireless 2011, Invited Paper, Vienna, Austria, 27–29 April 2011; pp. 89–92. [Google Scholar]
- Li, Q.; Li, Y.; Gao, J.; Zhao, B.; Fan, W.; Han, J. Resolving conflicts in heterogeneous data by truth discovery and source reliability estimation. In Proceedings of the SIGMOD ’14: 2014 ACM SIGMOD International Conference on Management of Data, Snowbird, UT, USA, 22–27 June 2014; pp. 1187–1198. [Google Scholar] [CrossRef]
- Ren, Y.; Zeng, Z.; Wang, T.; Zhang, S.; Zhi, G. A trust-based minimum cost and quality aware data collection scheme in P2P network. Peer Netw. Appl. 2020, 2020. [Google Scholar] [CrossRef]
- Lehrach, H.; Ionescu, A.M. The Future of Health Care: Deep data, smart sensors, virtual patients and the Internet-of-Humans. White Paper, 11 May 2016. Available online: https://ec.europa.eu/futurium/en/system/files/ged/futurehealth_white_paper.pdf (accessed on 29 April 2020).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technology | RFID | Bluetooth/BLE | ZigBee | TSCH | Wi-Fi HaLow |
|---|---|---|---|---|---|
| Standard | ISO/IEC 15, 693 | IEEE 802.15.1 | IEEE 802.15.4 | IEEE 802.15.4e | IEEE 802.11ah |
| Frequency band | 860–960 MHz, 2.4 GHz | 2.4/5 GHz | 868/915 MHz, 2.4 GHz | 2.4 GHz | Sub-1 GHz |
| Data Rate | 106–640 kbps | 1–24 Mbps/BLE: 2 Mbps | 20–250 kbps | Up to 250 kbps | 150 kbps to 78 Mbps |
| Energy efficiency | High | Medium; BLE: Very high | High | Very high | High |
| Transmission range | Up to 50 m | 10–100 m/Bluetooth 5.0: up to 250 m | 10–150 m | 10–150 m | Up to 1 km |
| Reliability | Medium | Medium/High | Medium | Very high | High |
| Mesh networking | Yes | No/Bluetooth Mesh: yes | Yes | Yes | No |
| Typical applications | Patient and medical equipment localization | Wearable healthcare monitoring, data acquisition | Home health monitoring, data aggregation | Healthcare in residential environment, data aggregation | Remote patient monitoring, backhaul aggregation, video streaming |
| Sensor Node | Data Rate | Sampling | Nodes | ADC | Power Consumption | Privacy Required | Latency |
|---|---|---|---|---|---|---|---|
| Glucose sensor | <1 kbps | <50 Hz | - | 16-bit | Extremely Low | High | <150 ms |
| [10,56] | |||||||
| Pacemaker | <1 kbps | <500 Hz | - | 12-bit | Low | High | <150 ms |
| [10,56] | |||||||
| Endoscope capsule | 1 Mbps | - | 2 | - | High | Medium | <150 ms |
| [10,56,60] | |||||||
| Cochlear implant | <1 Mbps | 5, 12, 49 MHz | - | - | Low | - | <150 ms |
| [56] | |||||||
| ECG (12-channel) | 72 kbps | <500 Hz | <6 | 12-bit | High | High | <250 ms |
| [10,56,60,65] | |||||||
| SpO2 | 32 kbps | - | - | - | Low | High | <250 ms |
| [10,65] | |||||||
| Respiration | <10 kbps | - | <12 | - | High | Medium | <250 ms |
| [60] | |||||||
| Blood pressure | <10 kbps | <100 Hz | <12 | 12-bit | High | High | <150 ms |
| [10,56,60,65] | |||||||
| EMG (12-channel) | 1.536 Mbps | 8 kHz | <6 | 16-bit | Low | - | <250 ms |
| [60] | |||||||
| Temperature | <10 kbps | - | <12 | - | Low | - | <250 ms |
| [56,60,62] | |||||||
| Blood flow rate | 480 kbps | <40 Hz | - | 12-bit | Low | - | <150 ms |
| [56] |
| Type of Threats, Attacks | Requirements | Description | Possible Actions |
|---|---|---|---|
| Eavesdropping, Evil-twin access point, Man in the Middle | Confidentiality | Intended users (patients, medical staff or even devices) may only access confidential data. Confidentiality aims to secure this access. Smart Healthcare devices must be able to safely transfer their sensitive data. | Privacy is at risk when confidentiality is bridged. Early detection of such threats is crucial. To mitigate these threats, it is necessary to employ cryptographic techniques for preventing eavesdroppers from intercepting data transmissions between legitimate users. |
| Insider attack, Replay attack, Frame injection attack | Integrity | Any type of attack that can alter medical data can be catastrophic for a Smart Healthcare system such as a Hospital Information System. Integrity aims to guarantee the accuracy of the transmitted information without any falsification [66]. | Detect such attacks as early as possible. All data values must satisfy semantic standards while unauthorized tampering is eliminated [72]. Employ techniques such as digest, digital signatures or watermarking in the case of multi-media data [73]. |
| DoS, Beacon flood, Authentication flood | Availability | In a complex Smart Healthcare system, only authorized users and perhaps other systems should be able to access wireless network resources anytime and anywhere upon request. | Techniques such as spread spectrum techniques, direct-sequence spread spectrum, frequency-hopping spread spectrum can be employed [66] to mitigate such threats for IoT medical devices. |
| Impersonation, Password, Dictionary, Brute-force, Sniffer, Spoofing, Access aggregation | Authenticity | Specified to differentiate authorized users from unauthorized users. In Smart Healthcare systems authentication is crucial for all participating entities (patients, medical staff point, devices, etc.) | Use medium access control (MAC) address for authentication purposes. Also use network-layer authentication, transport-layer authentication and application layer authentication [66]. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gardašević, G.; Katzis, K.; Bajić, D.; Berbakov, L. Emerging Wireless Sensor Networks and Internet of Things Technologies—Foundations of Smart Healthcare. Sensors 2020, 20, 3619. https://doi.org/10.3390/s20133619
Gardašević G, Katzis K, Bajić D, Berbakov L. Emerging Wireless Sensor Networks and Internet of Things Technologies—Foundations of Smart Healthcare. Sensors. 2020; 20(13):3619. https://doi.org/10.3390/s20133619
Chicago/Turabian StyleGardašević, Gordana, Konstantinos Katzis, Dragana Bajić, and Lazar Berbakov. 2020. "Emerging Wireless Sensor Networks and Internet of Things Technologies—Foundations of Smart Healthcare" Sensors 20, no. 13: 3619. https://doi.org/10.3390/s20133619
APA StyleGardašević, G., Katzis, K., Bajić, D., & Berbakov, L. (2020). Emerging Wireless Sensor Networks and Internet of Things Technologies—Foundations of Smart Healthcare. Sensors, 20(13), 3619. https://doi.org/10.3390/s20133619