1. Introduction
Deaths and serious injuries caused by traffic accidents represent a serious public health problem with broad social and economic consequences. However, contrary to what many people believe, accidents are preventable. Protection provided by vehicles through an Assistance and Driving Aid System (ADAS) can help reduce this problem. Among these systems, the Autonomous Emergency Braking (AEB) system stands out. This system identifies imminent collisions based on the recognition of objects placed in front of the vehicle by means of a camera and reacts automatically by activating the brakes. In this way, AEB can avoid certain types of collisions. Considering the obligations established by the regulations to install AEB in all new vehicles, these emergency braking and, in some cases, non-impact situations are expected to become more and more frequent. This implies new patterns of injury. The fact that an impact does not happen does not involve no injuries in the occupants [
1,
2,
3,
4,
5]. Sudden braking would be enough to be a potential risk for cervical spine damage, since neck is particularly sensitive to sudden changes in acceleration. The role of muscles is fundamental in cervical injury. Indeed, there are several studies [
6,
7,
8] that affirm that muscles are the main location of neck injury, especially in low-speed cases.
During dynamic loads, muscles fibres of the neck contract to stiffen the head–neck complex in order to reduce spinal column motion. The period during which the muscle is contracted varies depending on the passenger awareness [
9]. Those people who are warned previously about the event and know when this event will occur contract their muscles prior to impact. By contrast, unaware occupants contract cervical muscles as a reflex act during impact. There are researchers who affirm that in the event of a possible accident, there are no awareness-related differences [
7], and then being relaxed could be better; while others, on the contrary, suggest that it is better to contract the muscles before the accident [
10], because the relative movement between the different parts of the body is smaller. The question then arises as to which situation implies less risk of cervical injury in an emergency braking case. Be relaxed? Or contract the muscles before the braking? Therefore, considering the design characteristics of a vehicle safety system such as AEB, which situation implies a lower risk related to cervical injury? Should the vehicle warn that an imminent braking is going to happen, making it possible to contract muscles beforehand? Or, on the contrary, would it be better if the system does not warn about it and the muscles of the passenger were relaxed before sudden braking?
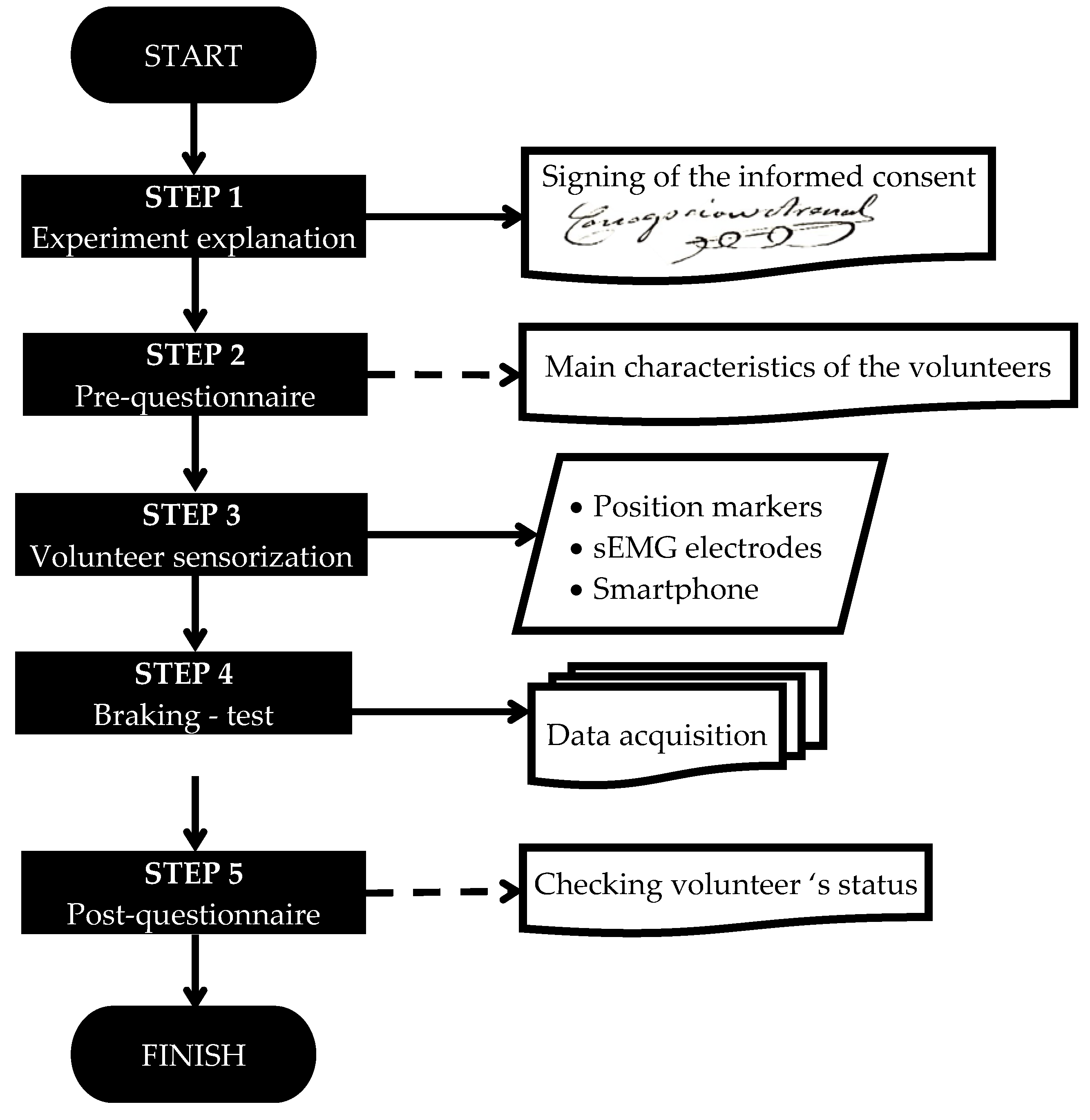
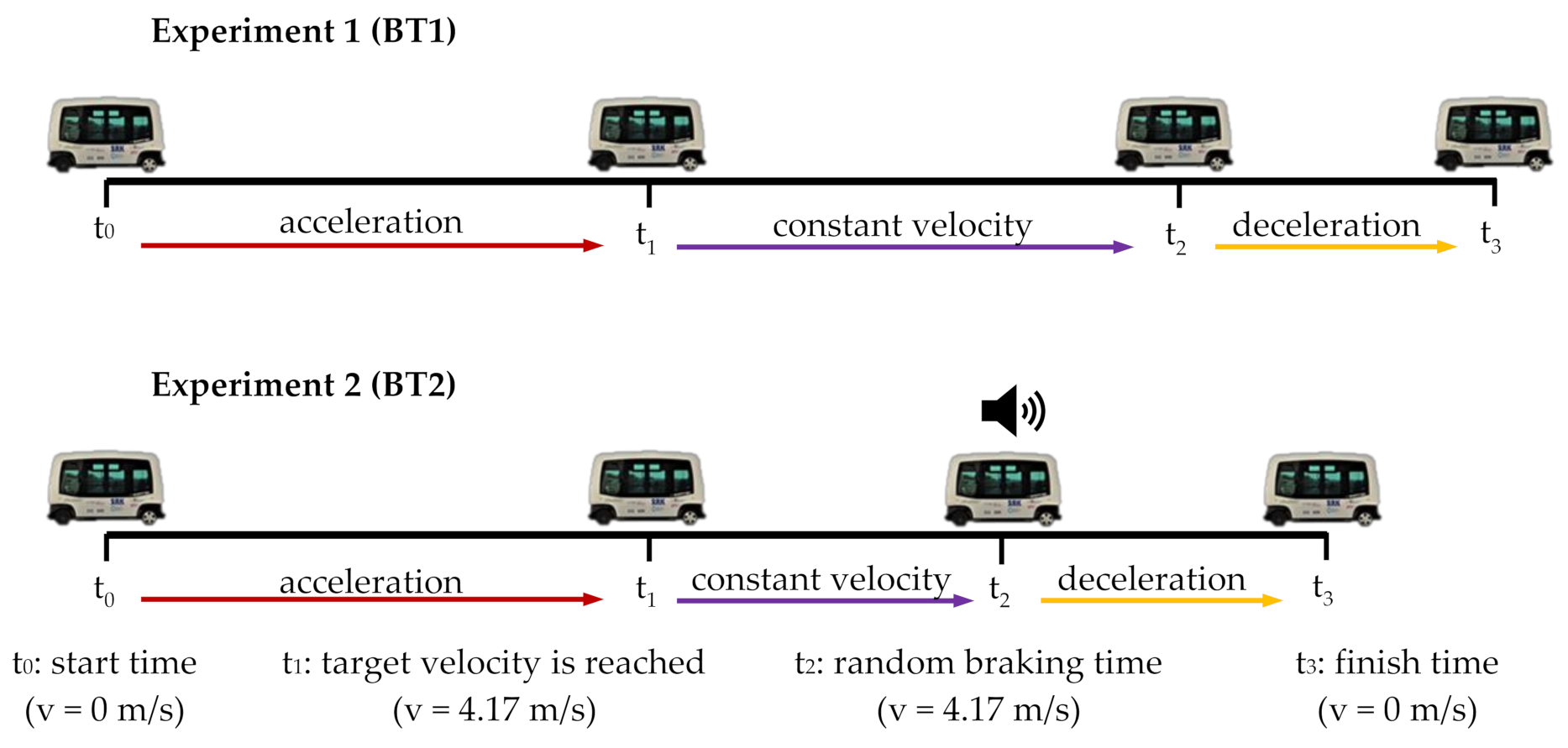
Finding whether there are differences in cervical muscle behaviour depending on whether the muscles are relaxed or contract before emergency braking is our main objective. For this, two different emergency braking tests will be carried out. In the first place, a test will be performed in which passengers will not be notified of the exact moment in which the emergency braking will take place, thus ensuring that they keep their muscles relaxed. Next, a second test will be carried out where passengers will be alerted to the moment at which the emergency braking is going to take place, so that they contract the muscles previously. On the other hand, there are research areas focused on the customised design of road safety based on gender and age [
11,
12]. Women have a 47% higher risk of serious injury in a car crash than men and five times higher risk of whiplash injury [
13]. However, most biomechanical models used in laboratories do not consider the anthropometric differences between women and men. Therefore, simulated crashes do not predict well female injuries. The overall effectiveness of occupant safety devices is biased toward male occupants. To the above, it should be added that older people are considered vulnerable users in road safety, since their body offers less resistance to impacts, so the probability of suffering a serious injury is higher as age increases. For this reason, analysing possible gender and age differences in cervical muscle behaviour is the other main aim of our work.
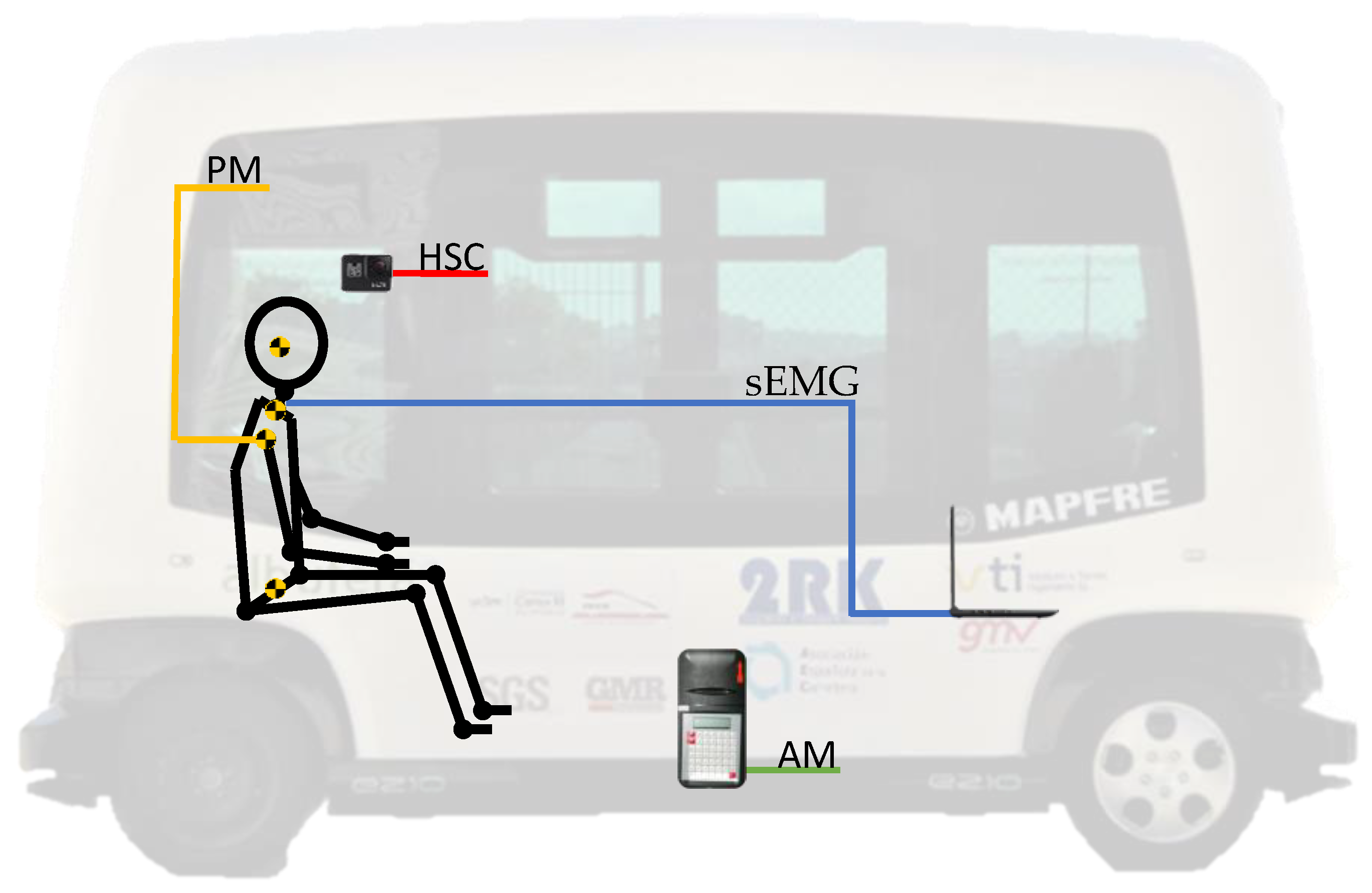
In order to analyse muscle behaviour, it is essential to have the maximum muscle biofidelity as possible. There are some biomechanical models such as cadavers, dummies, or computational models that do not have sufficient fidelity in the muscular response. This absence of biofidelity of these models can be solved by collecting data from human subjects. This factor is precisely one of the strengths of this study, where 18 volunteers participated.
In this work, the technique used to assess the cervical muscle response is surface electromyography (sEMG). During an emergency braking, the neck injury mechanism implies a sudden forward motion of the head, followed by another abrupt rearward movement. Considering this and similar studies in the literature [
14,
15,
16,
17], the trapezius (TRP) and sternocleidomastoid (SCM) were selected as target neck muscles. The SCM supports most of the dynamic load of the cervical area during rear impacts, while the TRP muscle bears most of the load in frontal impacts. There are other cervical muscles, such as the Scalenus muscle or Rectus Capitis Lateralis muscle, but they are deep muscles. If we wanted to properly assess the response of these deep muscles, the best option would be through intramuscular or needle electrodes. This would involve the need of researchers specialised in medicine, to which it should be added that this technique causes a greater probability of infection in the subject. It must be emphasised that neck injuries caused by non-collision accidents remain a meaningful health problem with a significant social cost [
18,
19]. Although these types of traffic accidents do not culminate in a final impact with another vehicle or obstacle on the road, they can involve significant levels of deceleration, translated into high loads that must be resisted by different anatomical regions. Among them, the cervical area stands out for being a very sensitive area to sudden changes in acceleration.
Furthermore, these musculoskeletal disorders (such as the controversial whiplash injury) are expected to continue growing due to the increase of the AEB systems in vehicles as well as the autonomous vehicles where these systems are also installed. Therefore, there is a need for performing new injury pattern studies where the traffic scenario can be different since the emergency braking system would avoid the impact.
Bearing in mind all the above, the hypotheses considered for the present work are the following:
First hypothesis: the passenger awareness of an emergency braking involves differences in the cervical muscle response.
Second hypothesis: there are differences in cervical muscle response during an emergency braking due to gender and age.
Answering these assumptions is the main aim of this study.
3. Results
Turning now to the experimental results, the next section explains the main results. Moreover, the amplitude and maximum values of the sEMG signals, once they had been normalised, were analysed for each volunteer in both autonomous emergency braking tests (without and with warning passengers). These values are represented by means of their average value (µ).
The results have been divided into two different phases within the emergency braking test. First, the braking phase is presented. This stage corresponds to the braking itself, that is, the period from when the vehicle begins to brake until it finally stops. Then, the post-braking phase takes place. This other stage corresponds to the period after braking, that is, from when the vehicle has stopped until the passenger stops moving. It must be considered that the subject will continue to move after the vehicle stops, due to their different inertia and the movement caused by the sudden deceleration. This would cause the passenger to continue moving until something stops the excursion, such as an obstacle or the resistance offered by muscles.
sEMG Signals
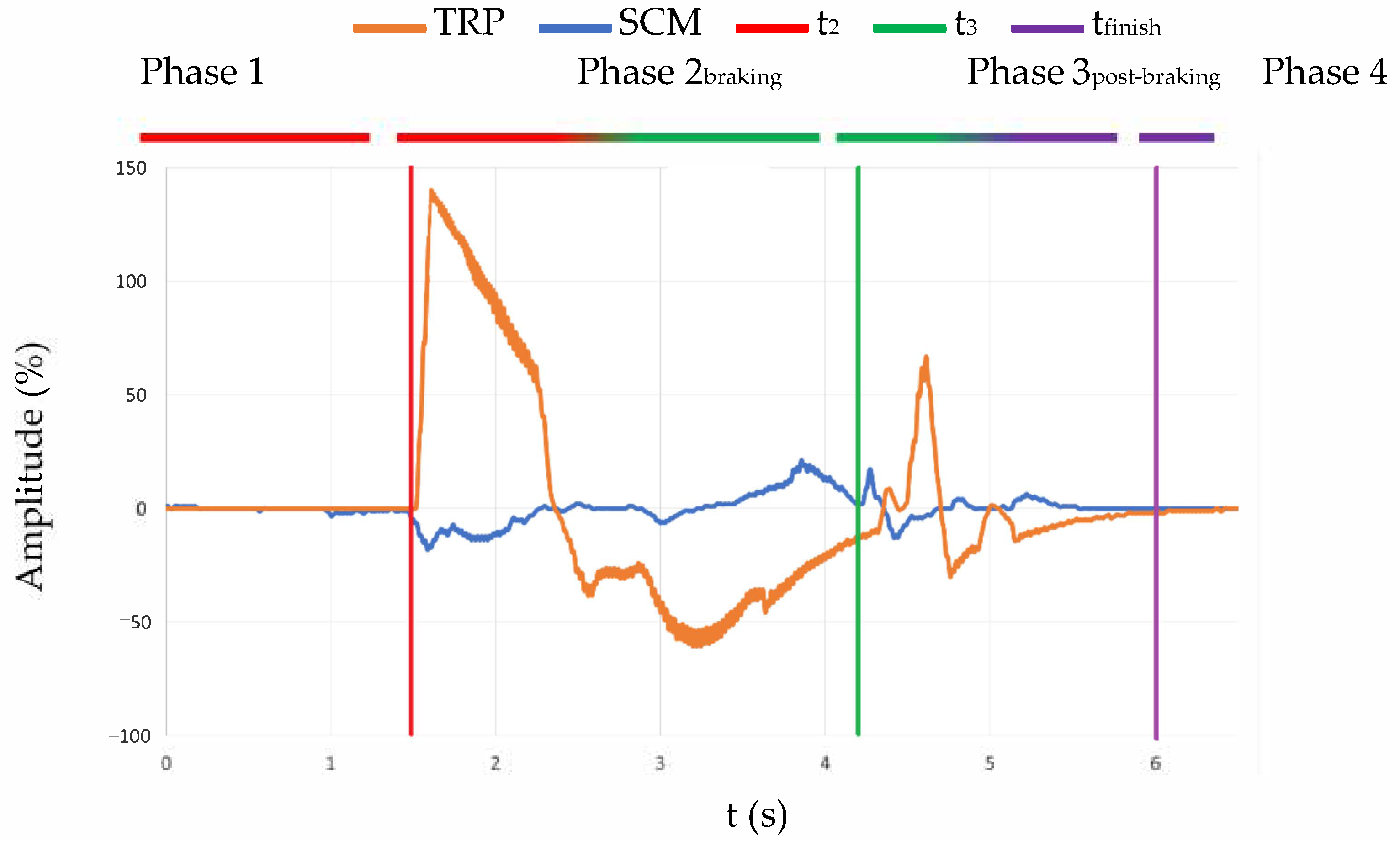
The sEMG signals acquired were from two different muscles, an agonist and an antagonist regarding the movement. In this section, all the graphics related to the EMG signal are going to show the signal from both muscles at the same time. Therefore, it is possible to point out the contraction in every step of the experiment. An example can be seen in
Figure 5. This figure shows the contraction of the muscles in the whole experiment, in which we observed different phases defined by time. The first one is what is happening before t
2 (red line) when the volunteer is relaxed. After that comes the second phase, which is enveloped between t
2 (red line) and t
3 (green line) and is when we observed the contraction due to the emergency braking. Once the bus is completely stopped, that signals the third phase (between t
3 (green line) and t
finish (purple line)), which the authors have decided to name post-braking, and where the bounces caused by emergency braking can be seen.
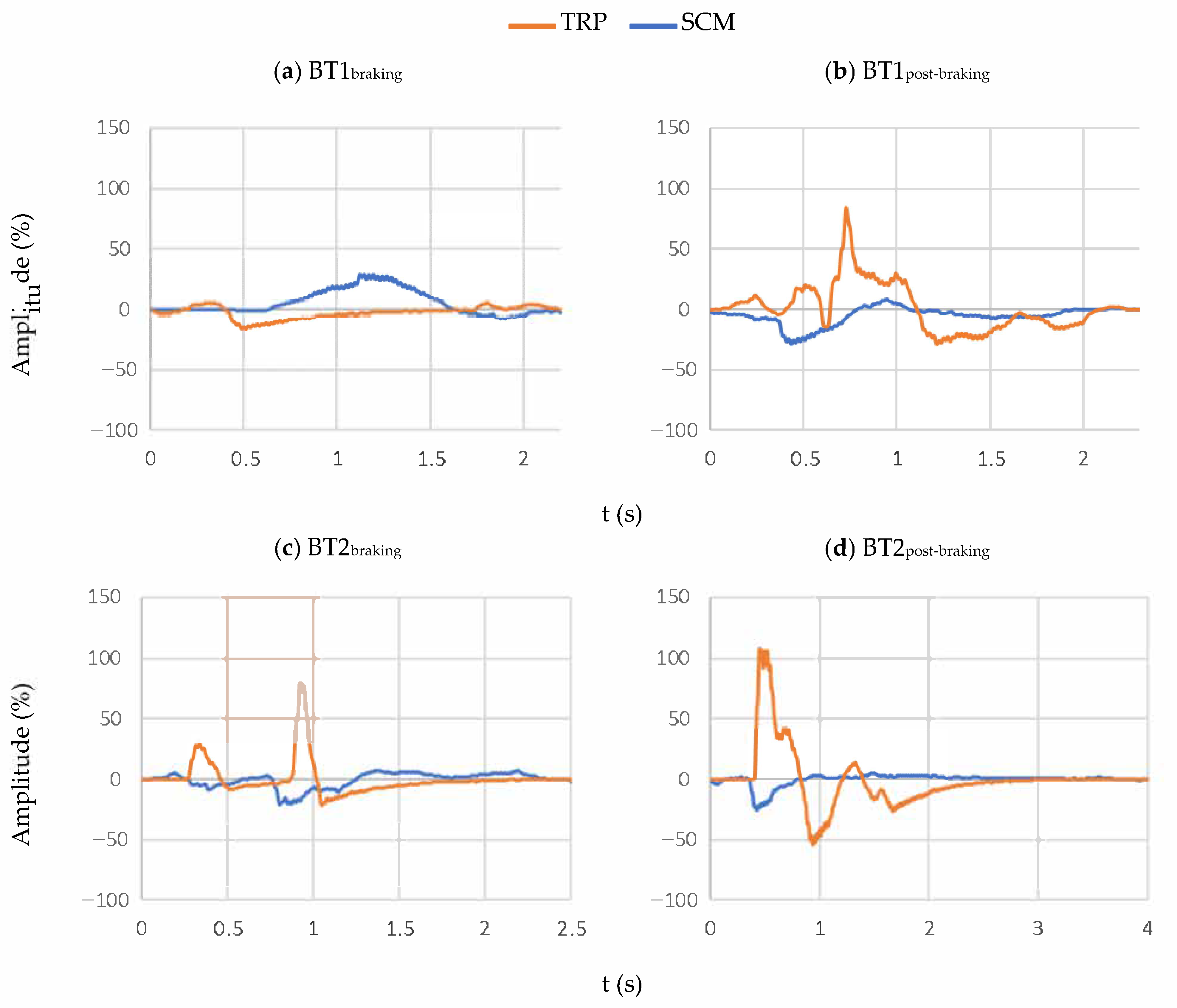
For a better understanding of the results, the signals that are shown in the following lines (
Figure 6) have been triggered. This provides a better definition of the different distinctive points of each experiment.
The example that is shown in
Figure 6 represents, in the left column, the muscle contractions during the emergency braking (from t
2 to t
3), and in the right column, the muscle contractions once the bus has completely stopped (from t
3). The signal of each muscle is represented in different colours, blue for the SCM and orange for the TRP response.
Moreover, it was evaluated whether there were differences in the cervical behaviour of the passengers according to their gender (♀ women and ♂ men) and age (younger than or equal to 35, and older than 35). This age threshold to disaggregate our sample data in two age groups was decided considering the physical and physiological changes associated with the age of 35 (the beginning of the so-called “early–middle-aged”). From this age on, people start to lose muscle mass and flexibility is reduced. We must pay special attention to the sEMG signal of the trapezius, as this muscle is essential in trying to retain the movement of the head concerning the torso when passengers travel in the direction of travel.
It was also included the µ and the P.P.O.M parameter. µ is the mean value and P.P.O.M is a variable defined by the percentage of people (♀ or ♂) whose amplitude or maximum value was higher than the mean value. In addition, P.P.O.M was calculated considering the value according to the genre of the volunteer.
It should also be noted that two different phases are analysed within the emergency braking test. On the one hand, results of the first phase of the test (Phase 2braking) are presented. This stage corresponds to the braking itself, that is, the period from when the vehicle begins to brake until it finally stops. On the other hand, the results of the second phase of the test (Phase 3post-braking) are shown. This stage corresponds to the period after braking, that is, from when the vehicle has stopped until the passenger stops moving. It must be taken into account that the subject will continue to move after the vehicle stops, due to its different inertia and the movement caused by the sudden deceleration. It will cause the passenger to continue moving until there is something that stops said excursions, such as an obstacle or the resistance offered by muscles to try not to get thrown out of the seat.
After analysing the results, we observed that there are differences in cervical behaviour based on gender. In the case of the BT1 (without warning) (see
Table 4), men experienced higher sEMG signal intensity of trapezius in both phases (braking and post-braking); while women showed a greater cervical response of SCM particularly in the post-braking stage. In any case, greater values of the sEMG signal are registered in the phase after braking for both women and men.
In the BT2 (with a warning) (see
Table 5), women suffered greater sEMG values of both cervical muscles in the braking phase, while men experienced a higher cervical response of TRP and SCM in the post-braking stage. These differences due to gender are more significant in the post-braking stage. On the other hand, when passengers are warned of the braking, it was also observed that men experienced greater values of the sEMG signal in the post-braking phase. In fact, these differences concerning the braking stage in men were more significant in BT2 than in BT1. On the contrary, women showed lower sEMG values in the post-braking phase.
Next, results are shown taking into account the age of the volunteers. The sample was divided into two age groups: less than or equal to 35 years and older than 35 years.
When passengers have not been warned in advance of the emergency braking (BT1 test) (see
Table 6), increases in the intensity of the sEMG signal of TRP muscle are observed in subjects older than 35 years of age, regardless of gender, in the post-braking phase. However, these increments are more significant in women, reaching 226% higher values for this age group.
In the case of the braking stage, women over 35 years of age continue to experience higher sEMG signal values. However, men do not seem to experience large changes in the electromyographic signal depending on their age in the emergency braking phase.
By including age in the analysis, it continues to be maintained that greater sEMG values are registered after stopping the vehicle (post-braking stage), independently of gender and age group. On the other hand, women suffered more activity in SCM muscle than men in both tests and for all age groups. For their part, men under or equal to 35 years experienced more TRP sEMG signal in both phases. Nevertheless, when men are older than 35, they registered lower sEMG values of TRP muscle than women.
If we analyse the results when passengers are previously warned about emergency braking (BT2) (see
Table 7), we can observe differences. Subjects younger than or equal to 35 experienced significant increases in the intensity of the sEMG signals of both cervical muscles, regardless of gender, in braking and post-braking phases. In this case (BT2), it is remarkable that women experience lower values of the sEMG signal in the post-braking phase with respect to the braking stage. While, on the contrary, men show higher values in the post-braking phase, also showing more notable differences between both stages.
In the case of the braking phase, women older than 35 continue to experience higher sEMG signal values. However, men do not seem to experience large changes in the electromyographic signal depending on their age in the emergency braking phase.
4. Discussion
Deaths and serious injuries caused by traffic accidents continue to be a concerning public health problem. This can be significantly mitigated by certain Assistance and Driving Aid Systems such as the Autonomous Emergency Braking (AEB) system, which can avoid the impact. This non-impact situation implies new injury patterns. In particular, the neck is very sensitive to sudden changes in acceleration, such as those caused by emergency braking. This is the reason why, in this study, the response of two superficial cervical muscles (trapezius (TRP) and sternocleidomastoid (SCM)) from 18 volunteers was assessed by sEMG.
Two different emergency braking tests were designed for this study, where their main difference is the awareness of the passenger about the time of emergency braking. This was decided considering controversies of previous studies where some authors did not find notable differences between warned or relaxed occupants, while other researchers suggested that it is better to contract the muscle before the accident. It should be noted that all tests were carried out at low speed to avoid any type of damage to the volunteer. Results were split according to gender and age because previous studies found important anthropometric differences that should be considered in the possible different injury patterns in traffic accidents. In fact, after analysing the results, we appreciated differences in cervical muscle behaviour based on gender and age, and depending on the braking phase.
If we focus on the results observed when passengers have not been warned of the emergency braking (BT1 test), men experienced higher sEMG signal intensity of trapezius in both phases (braking and post-braking), while women showed a greater cervical response of SCM particularly in the post-braking stage. In any case, this last phase seems to imply a greater risk of cervical injury, since higher values of the sEMG signal are reached in both men and women. This may be due to the fact that after the vehicle stops, the passenger continues to move, experiencing a series of rebounds, moving the head several times back and forth until it finally stabilises. This situation causes an overload on the neck, alternating between the performance of both cervical muscles TRP and SCM, until they manage to stop the movement of the head with respect to the torso. If we now approach the issue from the perspective of those passengers who were warned about braking (BT2 test), women suffered greater sEMG values of both cervical muscles in the braking phase, while men experienced higher cervical response of TRP and SCM in the post-braking stage. Gender differences are more significant in this last phase. The post-braking phase continues to be more harmful, since higher sEMG values are also obtained in this stage with respect to the braking phase, but now this only occurs in the case of men. On the contrary, women showed lower sEMG values in the post-braking phase in BT2. In addition, these differences with respect to the braking stage in men were more significant in BT2 than in BT1. Therefore, the post-braking phase affects the cervical behaviour more when the passenger is warned about the sudden braking. This seems to indicate that during the post-braking phase (once the first forward movement of the head has already taken place as a result of the braking itself), despite having been previously warned (and, therefore, tensing our muscles), it is much more difficult to maintain conscious control of the tension of our muscles to stabilise our movement. Men are more sensitive to these differences in the post-braking phase, while women are more sensitive in the initial braking phase.
Men show more cervical muscle activity during stabilisation (post-braking). It should be noted that there could be two explanations for these results (higher values of sEMG signals). Either their muscles suffer more (more possibility of damage), or they activate by tightening the muscles more, which translates into less relative movement of the head regarding the torso. The latter can translate into a lower risk of bone injury to the cervical vertebrae, since there is less relative movement of the head with respect to the torso. However, the fact of registering a greater electromyographic activity of the cervical muscles could also imply higher risk of muscular injury at the cervical spine. Therefore, the authors consider that more studies should be carried out to affirm which of the two situations would be more harmful globally (considering not only the risk of muscle damage but also the risk of damage to bone and other biological tissues). To do this, the authors propose repeating these tests recording acceleration values, in addition, to perform a detailed kinematic study of the different body regions.
By contrast, women, when they are warned of braking, register lower values of sEMG signal in the post-braking phase. This may be related to the greater relative movement between the head and torso that women experience. This lower electromyographic signal after the braking phase can indicate that women (after the initial muscle tensioning due to the warning) relax the muscles earlier and are less opposed to the inertial movement of their head with respect to the torso. This translated into injury risk, which could on the one hand imply a lower risk of muscle injury (by registering lower values of sEMG signal) but a greater risk of bone injury (by experiencing a greater relative movement of the head with respect to the torso). In any case, we can conclude that cervical behaviours, when passengers are warned, are completely opposite in women and men. These conclusions can be due to anthropometric differences. For example, women are smaller, have smaller vertebra, lower head mass, and less musculature. Consequently, women suffer a different combined response of head, neck, and torso to the emergency braking forces. Perhaps the strength of the musculature is an explanation for these differences.
Gender and awareness-related differences in cervical muscle response have also been reported by other studies [
6,
9,
10], while other authors considered the opposite [
7,
55]. Given these conflicting findings, it remains unclear if awareness of perturbation timing should be controlled.
Regarding the analysis based on the age of the volunteers, where results were divided into two age groups: less than or equal to 35 years and older than 35 years. When passengers have not been warned of the emergency braking (BT1 test), increases in the intensity of the sEMG signal of TRP muscle are observed in subjects older than 35 years of age, regardless of gender, in the post-braking phase. However, these increments are more significant in women. In the case of the braking stage, women over 35 years of age continue to experience higher sEMG signal values. However, men do not seem to experience large changes in the electromyographic signal depending on their age in the emergency braking phase. These results seem to indicate that as age increases, there is a greater risk of cervical injury, especially in the post-braking phase, when passengers are not warned about emergency braking. This may be due to the fact that as age increases, muscle mass is lost, and with it, muscle strength. This biological fact is more pronounced in women, hence the more significant increases in results.
By including age in the analysis, it continues to be maintained that greater sEMG values are registered after stopping the vehicle (post-braking stage), independently of gender and age group. On the other hand, women suffered more activity in SCM muscle than men in both tests and for all age groups. This may be due to the fact that women suffer a greater number of rebounds or these alternative neck movements are more abrupt after braking the vehicle until they manage to stabilise the neck. Therefore, they need to activate the SCM muscle more, as this is the main muscle to retain the movement of the head backwards. For their part, men under or equal to 35 years experienced more TRP sEMG signal in both phases. This could also be explained by the previous reason; since men suffer fewer rebounds in the neck, therefore, they experience less relative movement between the head and the torso during both braking phases. Thus, men seem to be mostly affected only by the first forward movement of the head, which would imply greater use of the TRP muscle.
Analysing the results when passengers are previously warned about emergency braking (BT2 test), we can also observe differences. Subjects younger than or equal to 35 experienced significant increases in the intensity of the sEMG signals of both cervical muscles, regardless of gender, in braking and post-braking phases. This could be because young people have greater muscle strength. Therefore, by being warned of braking, the youngest volunteers are able to activate the muscles more to try to stop their movement; hence, they register higher values of sEMG signal.
When women are warned (BT2 test), they experience lower values of the sEMG signal in the post-braking phase with respect to the braking stage. While, on the contrary, men show higher values in the post-braking phase, also showing more notable differences between both stages. In the case of the braking phase, women older than 35 continue to experience higher sEMG signal values. However, men do not seem to experience large changes in the electromyographic signal depending on their age in the emergency braking phase.
In conclusion, it is remarkable that the differences in cervical muscle behaviour due to gender and age are more appreciable and significant when subjects are warned about emergency braking. In any case, the main conclusions drawn from these differences in injury patterns should be taken into account when safety systems are designed to protect all type of users.
As the main limitation of the study, it must be considered that all tests were performed within the admitted physiological limits, so that the volunteer was not subjected to levels of deceleration that could cause injuries. Authors were always focused on the volunteer’s health and keeping them safe. Therefore, in order to extrapolate the conclusions drawn here to higher levels of deceleration that could cause injuries, these tests would have to be repeated with other types of subjects, such as postmortem human surrogates, dummies, or biomechanical models; because under no circumstance can research that could damage or injury use human beings as volunteers.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


