Risk of Falling in a Timed Up and Go Test Using an UWB Radar and an Instrumented Insole



Abstract
:1. Introduction
2. Materials and Methods
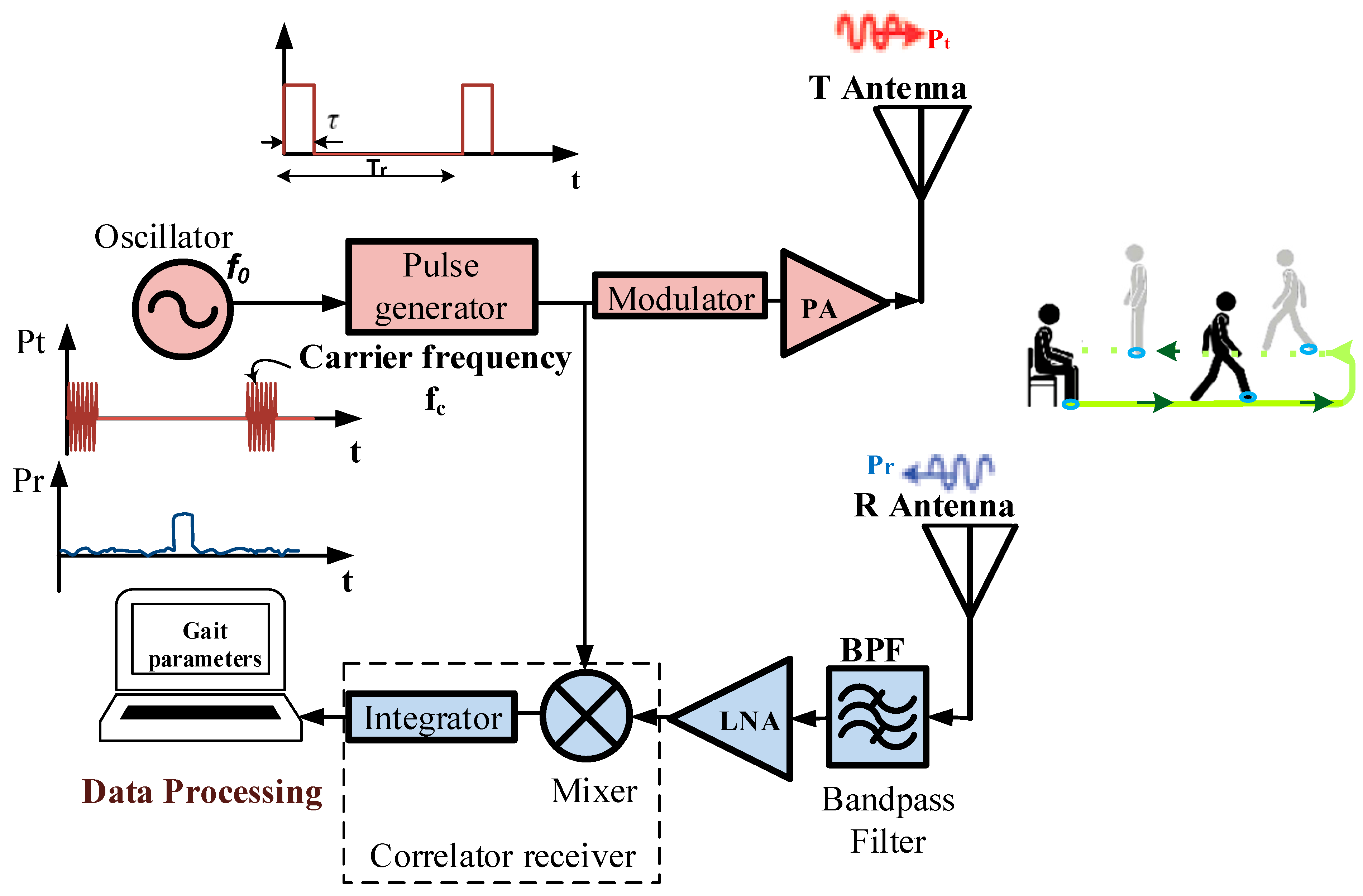
2.1. Contactless Sensor
2.2. Wearable Sensor
2.3. Experimental Procedure
2.4. TUG Data Analysis
2.4.1. Position-Based Activities Segmentation
- 1.
- Gait velocity estimation
- 2.
- Segmenting the TUG signal from a radar
2.4.2. Acceleration-Based Activities Segmentation
2.5. Comparing Radar and Instrumented Insole
2.5.1. Stride Length Computation
- 1.
- First approach
- 2.
- Second approach
- 3.
- Third approach
2.5.2. Risk of Falling Analysis
- 100 indicates the total absence of gait pathology. It means that the gait of the participant is close to the average gait parameters from the control subjects.
- Every 10 points that the falls below 100 corresponds one standard deviation away from or away from the average computed in the control subjects.
- 0 to 24 indicates a very high fall risk;
- 25 to 49 indicates a high fall risk;
- 50 to 74 indicates a medium fall risk;
- 75 to 99 indicates a low fall risk;
- 100 indicates a very low fall risk.
2.5.3. Statistical Analysis
3. Results and Discussion
3.1. Sensors Reduction Process
3.2. TUG’s Activities Segmentation for Enhancing Gait and Balance Disorders Detection
3.3. Contactless TUG Testing
3.4. Effect of the Turning Task
3.5. Discussion on the Stride Length Computation
3.6. Clinical Implications
3.7. Limitations of This Study
4. Conclusions and Future Works
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, C.; Un, K.; Mak, P.; Chen, Y.; Muñoz-Ferreras, J.; Yang, Z.; Gómez-García, R. Overview of Recent Development on Wireless Sensing Circuits and Systems for Healthcare and Biomedical Applications. IEEE J. Emerg. Sel. Top. Circuits Syst. 2018, 8, 165–177. [Google Scholar] [CrossRef]
- Hamad, R.A.; Hidalgo, A.S.; Bouguelia, M.; Estevez, M.E.; Quero, J.M. Efficient Activity Recognition in Smart Homes Using Delayed Fuzzy Temporal Windows on Binary Sensors. IEEE J. Biomed. Health Inform. 2020, 24, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Lach, J.; Lo, B.; Yang, G. Toward Pervasive Gait Analysis with Wearable Sensors: A Systematic Review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef] [PubMed]
- Muro-de-la-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharghan, S.K.; Mohammed, S.L.; Al-Naji, A.; Abu-AlShaeer, M.J.; Jawad, H.M.; Jawad, A.M.; Chahl, J. Accurate Fall Detection and Localization for Elderly People Based on Neural Network and Energy-Efficient Wireless Sensor Network. Energies 2018, 11, 2866. [Google Scholar] [CrossRef] [Green Version]
- Torres, R.L.S.; Visvanathan, R.; Hoskins, S.; van den Hengel, A.; Ranasinghe, D.C. Effectiveness of a Batteryless and Wireless Wearable Sensor System for Identifying Bed and Chair Exits in Healthy Older People. Sensors 2016, 16, 546. [Google Scholar] [CrossRef] [Green Version]
- Wahid, F.; Begg, R.K.; Hass, C.J.; Halgamuge, S.; Ackland, D.C. Classification of Parkinson’s Disease Gait Using Spatial-Temporal Gait Features. IEEE J. Biomed. Health Inf. 2015, 19, 1794–1802. [Google Scholar] [CrossRef]
- Ren, L.; Peng, Y. Research of fall detection and fall prevention technologies: A systematic review. IEEE Access 2019, 7, 77702–77722. [Google Scholar] [CrossRef]
- Lin, C.-L.; Chiu, W.-C.; Chu, T.-C.; Ho, Y.-H.; Chen, F.-H.; Hsu, C.-C.; Hsieh, P.-H.; Chen, C.-H.; Lin, C.-C.K.; Sung, P.-S.; et al. Innovative Head-Mounted System Based on Inertial Sensors and Magnetometer for Detecting Falling Movements. Sensors 2020, 20, 5774. [Google Scholar] [CrossRef]
- Jarchi, D.; Pope, J.; Lee, T.K.M.; Tamjidi, L.; Mirzaei, A.; Sanei, S. A Review on Accelerometry-Based Gait Analysis and Emerging Clinical Applications. IEEE Rev. Biomed. Eng. 2018, 11, 177–194. [Google Scholar] [CrossRef]
- Greene, B.R.; O’Donovan, A.; Romero-Ortuno, R.; Cogan, L.; Scanaill, C.N.; Kenny, R.A. Quantitative falls risk assessment using the Timed Up and Go test. IEEE Trans. Biomed. Eng. 2010, 57, 2918–2926. [Google Scholar] [CrossRef]
- Liu, Y.; Hu, Y.H.; Pan, Q. Distributed, Robust Acoustic Source Localization in a Wireless Sensor Network. IEEE Trans. Signal. Process. 2012, 60, 4350–4359. [Google Scholar] [CrossRef]
- Jiangpeng, D.; Xiaole, B.; Zhimin, Y.; Zhaohui, S.; Dong, X.; PerFall, D. A pervasive fall detection system using mobile phones. In Proceedings of the 2010 8th IEEE International Conference on Pervasive Computing and Communications Workshops (PERCOM Workshops), Mannheim, Germany, 29 March–2 April 2010; pp. 292–297. [Google Scholar]
- Milosevic, M.; Jovanov, E.; Milenkovic, A. Quantifying Timed-Up-and-Go test: A smartphone implementation. In Proceedings of the Body Sensor Networks (BSN), 2013 IEEE International Conference, Cambridge, MA, USA, 6–9 May 2013; pp. 1–6. [Google Scholar]
- Hegde, N.; Bries, M.; Sazonov, E. A comparative review of footwear-based wearable systems. Electronics 2016, 5, 48. [Google Scholar] [CrossRef]
- Liu, T.; Guo, X.; Wang, G. Elderly-falling detection using distributed direction-sensitive pyroelectric infrared sensor arrays. Multidimens. Syst. Signal Process. 2012, 23, 451–467. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, M.; Yuan, Y.; Chan, K.Y. Fall Detection and Personnel Tracking System Using Infrared Array Sensors. IEEE Sens. J. 2020, 20, 9558–9566. [Google Scholar] [CrossRef]
- Han, C.; Wu, K.; Wang, Y.; Ni, L.M. WiFall: Device-free fall detection by wireless networks. In Proceedings of the IEEE INFOCOM 2014-IEEE Conference on Computer Communications, Toronto, ON, Canada, 27 April–2 May 2014; pp. 271–279. [Google Scholar]
- Ding, J.; Wang, Y. A WiFi-Based Smart Home Fall Detection System Using Recurrent Neural Network. IEEE Trans. Consum. Electron. 2020, 66, 308–317. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, D.; Wang, Y.; Ma, J.; Wang, Y.; Li, S. RT-Fall: A Real-Time and Contactless Fall Detection System with Commodity WiFi Devices. IEEE Trans. Mob. Comput. 2017, 16, 511–526. [Google Scholar] [CrossRef]
- Sun, S.; Zhao, X.; Tan, M. Fast and Robust RGB-D Multiple Human Tracking Based on Part Model for Mobile Robots. In Proceedings of the 2019 Chinese Control Conference (CCC), Guangzhou, China, 27–30 July 2019; pp. 4525–4530. [Google Scholar]
- Cippitelli, E.; Fioranelli, F.; Gambi, E.; Spinsante, S. Radar and RGB-Depth Sensors for Fall Detection: A Review. IEEE Sens. J. 2017, 17, 3585–3604. [Google Scholar] [CrossRef] [Green Version]
- Panahi, L.; Ghods, V. Human fall detection using machine vision techniques on RGB–D images. Biomed. Signal Process. Control 2018, 44, 146–153. [Google Scholar] [CrossRef]
- Han, T.; Kang, W.; Choi, G. IR-UWB Sensor Based Fall Detection Method Using CNN Algorithm. Sensors 2020, 20, 5948. [Google Scholar] [CrossRef]
- Ma, L.; Liu, M.; Wang, N.; Wang, L.; Yang, Y.; Wang, H. Room-Level Fall Detection Based on Ultra-Wideband (UWB) Monostatic Radar and Convolutional Long Short-Term Memory (LSTM). Sensors 2020, 20, 1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diraco, G.; Leone, A.; Siciliano, P. A Radar-Based Smart Sensor for Unobtrusive Elderly Monitoring in Ambient Assisted Living Applications. Biosensors 2017, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, P.P.; Rocha, A.S.; Shaker, G.; Lee, D.; Wei, J.; Fong, B.; Thatte, A.; Karimi, A.; Xu, L.; Ma, A.; et al. Comparative Analysis of Gait Speed Estimation Using Wideband and Narrowband Radars, Thermal Camera, and Motion Tracking Suit Technologies. J. Healthc. Inform. Res. 2020, 4, 215–237. [Google Scholar] [CrossRef]
- Camplani, M.; Paiement, A.; Mirmehdi, M.; Damen, D.; Hannuna, S.; Burghardt, T.; Tao, L. Multiple human tracking in RGB-depth data: A survey. IET Comput. Vis. 2017, 11, 265–285. [Google Scholar] [CrossRef] [Green Version]
- Aminzadeh, F.; Edwards, N.; Lockett, D.; Nair, R.C. Utilization of bathroom safety devices, patterns of bathing and toileting, and bathroom falls in a sample of community living older adults. Technol. Disabil. 2001, 13, 95–103. [Google Scholar] [CrossRef]
- Seifert, A.; Grimmer, M.; Zoubir, A.M. Doppler Radar for the Extraction of Biomechanical Parameters in Gait Analysis. IEEE J. Biomed. Health Inform. 2020, 1. [Google Scholar] [CrossRef]
- Hernangómez, R.; Santra, A.; Stańczak, S. Human Activity Classification with Frequency Modulated Continuous Wave Radar Using Deep Convolutional Neural Networks. In Proceedings of the 2019 International Radar Conference (RADAR), Guangzhou, China, 23–27 September 2019; pp. 1–6. [Google Scholar]
- Saho, K.; Uemura, K.; Sugano, K.; Matsumoto, M. Using Micro-Doppler Radar to Measure Gait Features Associated with Cognitive Functions in Elderly Adults. IEEE Access 2019, 7, 24122–24131. [Google Scholar] [CrossRef]
- Mokhtari, G.; Aminikhanghahi, S.; Zhang, Q.; Cook, D.J. Fall detection in smart home environments using UWB sensors and unsupervised change detection. J. Reliab. Intell. Environ. 2018, 4, 131–139. [Google Scholar] [CrossRef]
- Koo, Y.S.; Ren, L.; Wang, Y.; Fathy, A.E. UWB MicroDoppler Radar for human Gait analysis, tracking more than one person, and vital sign detection of moving persons. In Proceedings of the 2013 IEEE MTT-S International Microwave Symposium Digest (MTT), Seattle, WA, USA, 2–7 June 2013; pp. 1–4. [Google Scholar]
- Wang, F.; Skubic, M.; Rantz, M.; Cuddihy, P.E. Quantitative gait measurement with pulse-Doppler radar for passive in-home gait assessment. IEEE Trans. Biomed. Eng. 2014, 61, 2434–2443. [Google Scholar] [CrossRef] [Green Version]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: The Get Up and Go Test. Arch Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar]
- Han, Y.; Lauteslager, T.; Lande, T.S.; Constandinou, T.G. UWB Radar for Non-contact Heart Rate Variability Monitoring and Mental State Classification. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6578–6582. [Google Scholar]
- Xethru by Novelda. X4m200 Datasheets. Available online: https://www.codico.com/shop/media/datasheets/Novelda_X4M200_respiration_sensor_rev_c_preliminary.pdf (accessed on 14 May 2020).
- Gunasekara, A. Contactless Estimation of Breathing Rate Using UWB Radar; University of Ottawa: Ottawa, ON, Canada, 2017. [Google Scholar]
- Zampieri, C.; Arash, S.; Patricia, C.-K.; John, G.; Fay, B.H. Assessing mobility at home in people with early Parkinson’s disease using an instrumented Timed Up and Go test. Parkinsonism Relat. Disord. 2011, 17, 277–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zampieri, C.; Salarian, A.; Carlson-Kuhta, P.; Aminian, K.; Nutt, J.G.; Horak, F.B. The instrumented Timed Up and Go test: Potential outcome measure for disease modifying therapies in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2010, 81, 171–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otis, M.J.D.; Ayena, J.C.; Tremblay, L.E.; Fortin, P.E.; Ménélas, B.-A.J. Use of an enactive insole for reducing the risk of falling on different types of soil using vibrotactile cueing for the elderly. PLoS ONE 2016, 11, e0162107. [Google Scholar] [CrossRef] [PubMed]
- Ayena, J.C.; Tremblay, L.E.; Otis, M.J.D.; Ménélas, B.-A.J. Comparing auditory, visual and vibrotactile cues in individuals with Parkinson’s disease for reducing risk of falling over different types of soil. Somatosens. Mot. Res. 2017, 34, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Noshadi, H.; Dabiri, F.; Ahmadian, S.; Amini, N.; Sarrafzadeh, M. Hermes: Mobile system for instability analysis and balance assessment. ACM Trans. Embed. Comput. Syst. 2013, 12, 1–24. [Google Scholar] [CrossRef]
- Lin, F.; Wang, A.; Zhuang, Y.; Tomita, M.R.; Xu, W. Smart insole: A wearable sensor device for unobtrusive gait monitoring in daily life. IEEE Trans. Ind. Inf. 2016, 12, 2281–2291. [Google Scholar] [CrossRef]
- Ayena, J.C.; Otis, M.J.D. Validation of Minimal Number of Force Sensitive Resistors to Predict Risk of Falling During a Timed Up and Go Test. J. Med. Biol. Eng. 2020, 40, 348–355. [Google Scholar] [CrossRef]
- Rana, M.M.; Halim, N.; Rahamna, M.M.; Abdelhadi, A. Position and Velocity Estimations of 2D-Moving Object Using Kalman Filter: Literature Review. In Proceedings of the 2020 22nd International Conference on Advanced Communication Technology (ICACT), Pyeongchang, Korea, 16–19 February 2020; pp. 541–544. [Google Scholar]
- Shakhakarmi, N.; Vaman, D.R. Real Time Position Location & Tracking (PL&T) using Prediction Filter and Integrated Zone Finding in OFDM Channel. WSEAS Trans. Commun. 2012, 11, 1190–2742. [Google Scholar]
- Van Lummel, R.C.; Walgaard, S.; Maier, A.B.; Ainsworth, E.; Beek, P.J.; van Dieën, J.H. The Instrumented Sit-to-Stand Test (iSTS) Has Greater Clinical Relevance than the Manually Recorded Sit-to-Stand Test in Older Adults. PLoS ONE 2016, 11, e0157968. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Zheng, H.; Wang, H.; McClean, S.; Newell, D. iGAIT: An interactive accelerometer based gait analysis system. Comput. Methods Programs Biomed. 2012, 108, 715–723. [Google Scholar] [CrossRef]
- Ayub, S.; Zhou, X.; Honary, S.; Bahraminasab, A.; Honary, B. Sensor Placement Modes for Smartphone Based Pedestrian Dead Reckoning. In Computer, Informatics, Cybernetics and Applications; He, X., Hua, E., Lin, Y., Liu, X., Eds.; Springer: Amsterdam, The Netherlands, 2012; Volume 107, pp. 123–132. [Google Scholar]
- Ben Brahem, M.; Ménélas, B.-A.J.; Otis, M.J.D. Use of a 3DOF accelerometer for foot tracking and gesture recognition in mobile HCI. Procedia Comput. Sci. 2013, 19, 453–460. [Google Scholar] [CrossRef] [Green Version]
- Capela, N.A.; Lemaire, E.D.; Baddour, N. Novel algorithm for a smartphone-based 6-minute walk test application: Algorithm, application development, and evaluation. J. Neuroeng. Rehabil. 2015, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salarian, A.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. iTUG, a sensitive and reliable measure of mobility. IEEE Trans. Neural. Syst. Rehabil. Eng. 2010, 18, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, M.; Mongeon, D.; Prince, F. Biomechanical parameters for gait analysis: A systematic review of healthy human gait. Phys. Ther. Rehabil. 2017, 4, 6. [Google Scholar] [CrossRef]
- Hamacher, D.; Singh, N.B.; Van Dieën, J.H.; Heller, M.O.; Taylor, W.R. Kinematic measures for assessing gait stability in elderly individuals: A systematic review. J. R. Soc. Interface. 2011, 8, 1682–1698. [Google Scholar] [CrossRef]
- Huijben, B.; van Schooten, K.S.; van Dieën, J.H.; Pijnappels, M. The effect of walking speed on quality of gait in older adults. Gait Posture 2018, 65, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Díez, L.E.; Bahillo, A.; Otegui, J.; Otim, T. Step Length Estimation Methods Based on Inertial Sensors: A Review. IEEE Sens. J. 2018, 18, 6908–6926. [Google Scholar] [CrossRef]
- Hannink, J.; Kautz, T.; Pasluosta, C.F.; Barth, J.; Schülein, S.; Gaßmann, K.G.; Klucken, J.; Eskofier, B.M. Mobile Stride Length Estimation With Deep Convolutional Neural Networks. IEEE J. Biomed. Health Inform. 2018, 22, 354–362. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Jang, H.; Hwang, D.; Park, C. A Step, Stride and Heading Determination for the Pedestrian Navigation System. J. Glob. Position. Syst. 2004, 3, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, H. Using the ADXL202 in Pedometer and Personal Navigation Applications. In Application Notes American Devices; Analog Devices: Cambridge, MA, USA, 2002. [Google Scholar]
- Scarlett, J. Enhancing the Performance of Pedometers Using a Single Accelerometer. Available online: http://www.sgbotic.com/products/appnotes/sensors/47076299220991AN_900.pdf (accessed on 21 January 2021).
- Xing, H.; Li, J.; Hou, B.; Zhang, Y.; Guo, M. Pedestrian Stride Length Estimation from IMU Measurements and ANN Based Algorithm. J. Sens. 2017, 2017, 6091261. [Google Scholar] [CrossRef] [Green Version]
- Truong, P.H.; Nguyen, N.D.; Ho, N.-H.; Jeong, G.-M. Nonparametric Regression-based Step-length Estimation for Arm-swing Walking using a Smartphone. Int. J. Comput. Commun. Control 2018, 13, 566–573. [Google Scholar] [CrossRef]
- Ho, N.-H.; Truong, P.H.; Jeong, G.-M. Step-Detection and Adaptive Step-Length Estimation for Pedestrian Dead-Reckoning at Various Walking Speeds Using a Smartphone. Sensors 2016, 16, 1423. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.H.; Rozumalski, A. The gait deviation index: A new comprehensive index of gait pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Galli, M. Gait Scores: Interpretations and Limitations. In Handbook of Human Motion; Springer International Publishing: Cham, Switzerland, 2018; pp. 673–687. [Google Scholar]
- Joanna, M.; Magdalena, S.; Katarzyna, B.-M.; Daniel, S.; Ewa, L.-D. The Utility of Gait Deviation Index (GDI) and Gait Variability Index (GVI) in Detecting Gait Changes in Spastic Hemiplegic Cerebral Palsy Children Using Ankle–Foot Orthoses (AFO). Children 2020, 7, 149. [Google Scholar] [CrossRef]
- Gagnon, D.; Menelas, B.A.J.; Otis, M.J.D. Qualitative risk of falling assessment based on gait abnormalities. In Proceedings of the 2013 IEEE International Conference on Systems, Man, and Cybernetics, Manchester, UK, 13–16 October 2013; pp. 3966–3971. [Google Scholar]
- Di Rosa, M.; Hausdorff, J.M.; Stara, V.; Rossi, L.; Glynn, L.; Casey, M.; Burkard, S.; Cherubini, A. Concurrent validation of an index to estimate fall risk in community dwelling seniors through a wireless sensor insole system: A pilot study. Gait Posture 2017, 55, 6–11. [Google Scholar] [CrossRef]
- Ayena, J.C.; Otis, M.J.D. Dimensional reduction of balance parameters in risk of falling evaluation using a minimal number of force-sensitive resistors. Int. J. Occup. Saf. Ergon. 2020, 10, 1–32. [Google Scholar] [CrossRef]
- Rosenlund, S.; Holsgaard-Larsen, A.; Overgaard, S.; Jensen, C. The Gait Deviation Index Is Associated with Hip Muscle Strength and Patient-Reported Outcome in Patients with Severe Hip Osteoarthritis—A Cross-Sectional Study. PLoS ONE 2016, 11, e0153177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Noritake, K.; Sugiura, H.; Kamiya, Y.; Tomita, H.; Ito, Y.; Sugiura, H.; Ochi, N.; Yoshihashi, Y. Association between Gait Deviation Index and Physical Function in Children with Bilateral Spastic Cerebral Palsy: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 28. [Google Scholar] [CrossRef] [Green Version]
- Brahem, M.B.; Ayena, J.C.; Otis, M.J.D.; Menelas, B.A.J. Risk of falling assessment on different types of ground using the instrumented TUG. In Proceedings of the 2015 IEEE International Conference on Systems, Man, and Cybernetics, Kowloon, China, 9–12 October 2015; pp. 2372–2377. [Google Scholar]
- Ma, L.; Tian, S.; Song, Y.; Wu, Z.; Yue, M. An Approach of ACARS Trajectory Reconstruction Based on Adaptive Cubic Spline Interpolation. In Proceedings of the Security, Privacy, and Anonymity in Computation, Communication, and Storage, Cham, Switzerland, 14–17 July 2019; pp. 245–252. [Google Scholar]
- Vibert, J.F. Neurophysiologie: De la Physiologie à L’exploration Fonctionnelle; Elsevier Masson ed.: Issy Les Moulineaux, France, 2011. [Google Scholar]
- Vandewynckel, J.; Otis, M.J.-D.; Bouchard, B.; Ménélas, B.A.J.; Bouzouane, A. Towards a Real-time Error Detection within a Smart Home by Using Activity Recognition with a Shoe-mounted Accelerometer. Procedia Comput. Sci. 2013, 19, 516–523. [Google Scholar] [CrossRef] [Green Version]
- Son, M.; Youm, C.; Cheon, S.; Kim, J.; Lee, M.; Kim, Y.; Kim, J.; Sung, H. Evaluation of the turning characteristics according to the severity of Parkinson disease during the timed up and go test. Aging Clin. Exp. Res. 2017, 29, 1191–1199. [Google Scholar] [CrossRef]
- Gulley, E.; Ayers, E.; Verghese, J. A comparison of turn and straight walking phases as predictors of incident falls. Gait Posture 2020, 79, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Yardibi, T.; Cuddihy, P.; Genc, S.; Bufi, C.; Skubic, M.; Rantz, M.; Liang, L.; Phillips, C. Gait characterization via pulse-Doppler radar. In Proceedings of the 2011 IEEE International Conference on Pervasive Computing and Communications Workshops (PERCOM Workshops), Seattle, WA, USA, 21–25 March 2011; pp. 662–667. [Google Scholar]
- Alshamaa, D.; Chkeir, A.; Soubra, R.; Dauriac, B. A Smart Radar System for Automatic Functional Capacity Tests. In Proceedings of the 2019 3rd International Conference on Bio-engineering for Smart Technologies (BioSMART), Paris, France, 24–26 April 2019; pp. 1–4. [Google Scholar]
- Sheikh, M.; Hosseini, H.A. Investigating the relationship between spatiotemporal gait variability and falls self-efficacy in individuals with chronic stroke. Physiother. Theory Pr. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Bouça-Machado, R.; Jalles, C.; Guerreiro, D.; Pona-Ferreira, F.; Branco, D.; Guerreiro, T.; Matias, R.; Ferreira, J.J. Gait Kinematic Parameters in Parkinson’s Disease: A Systematic Review. J. Parkinson Dis. 2020, 1–11. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| System | Parameters Measured by the System |
|---|---|
| Insole | Cadence—Stride time—Stride speed—Stride length |
| Radar | Stride length—Stride speed |
| Methods | Radar Estimation vs. Approach Estimation | WF vs. WB (p-Value) | Walk and Turn | |||
|---|---|---|---|---|---|---|
| WF (p-Value) | WB (p-Value) | B and A Turn (p-Value) | p-Value | RMSE | ||
| 1st approach | 0.0215 | 0.0061 | <0.001 | 0.0803 | <0.001 | 0.4099 |
| 2nd approach | <0.001 | <0.001 | <0.001 | 0.1677 | <0.001 | 0.5761 |
| 3rd approach | 0.0171 | 0.0024 | 0.2477 | 0.6848 | 0.2083 | 0.3675 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayena, J.C.; Chioukh, L.; Otis, M.J.-D.; Deslandes, D. Risk of Falling in a Timed Up and Go Test Using an UWB Radar and an Instrumented Insole. Sensors 2021, 21, 722. https://doi.org/10.3390/s21030722
Ayena JC, Chioukh L, Otis MJ-D, Deslandes D. Risk of Falling in a Timed Up and Go Test Using an UWB Radar and an Instrumented Insole. Sensors. 2021; 21(3):722. https://doi.org/10.3390/s21030722
Chicago/Turabian StyleAyena, Johannes C., Lydia Chioukh, Martin J.-D. Otis, and Dominic Deslandes. 2021. "Risk of Falling in a Timed Up and Go Test Using an UWB Radar and an Instrumented Insole" Sensors 21, no. 3: 722. https://doi.org/10.3390/s21030722
APA StyleAyena, J. C., Chioukh, L., Otis, M. J. -D., & Deslandes, D. (2021). Risk of Falling in a Timed Up and Go Test Using an UWB Radar and an Instrumented Insole. Sensors, 21(3), 722. https://doi.org/10.3390/s21030722