
A Review of Exoskeletons Considering Nurses

Abstract
:1. Introduction
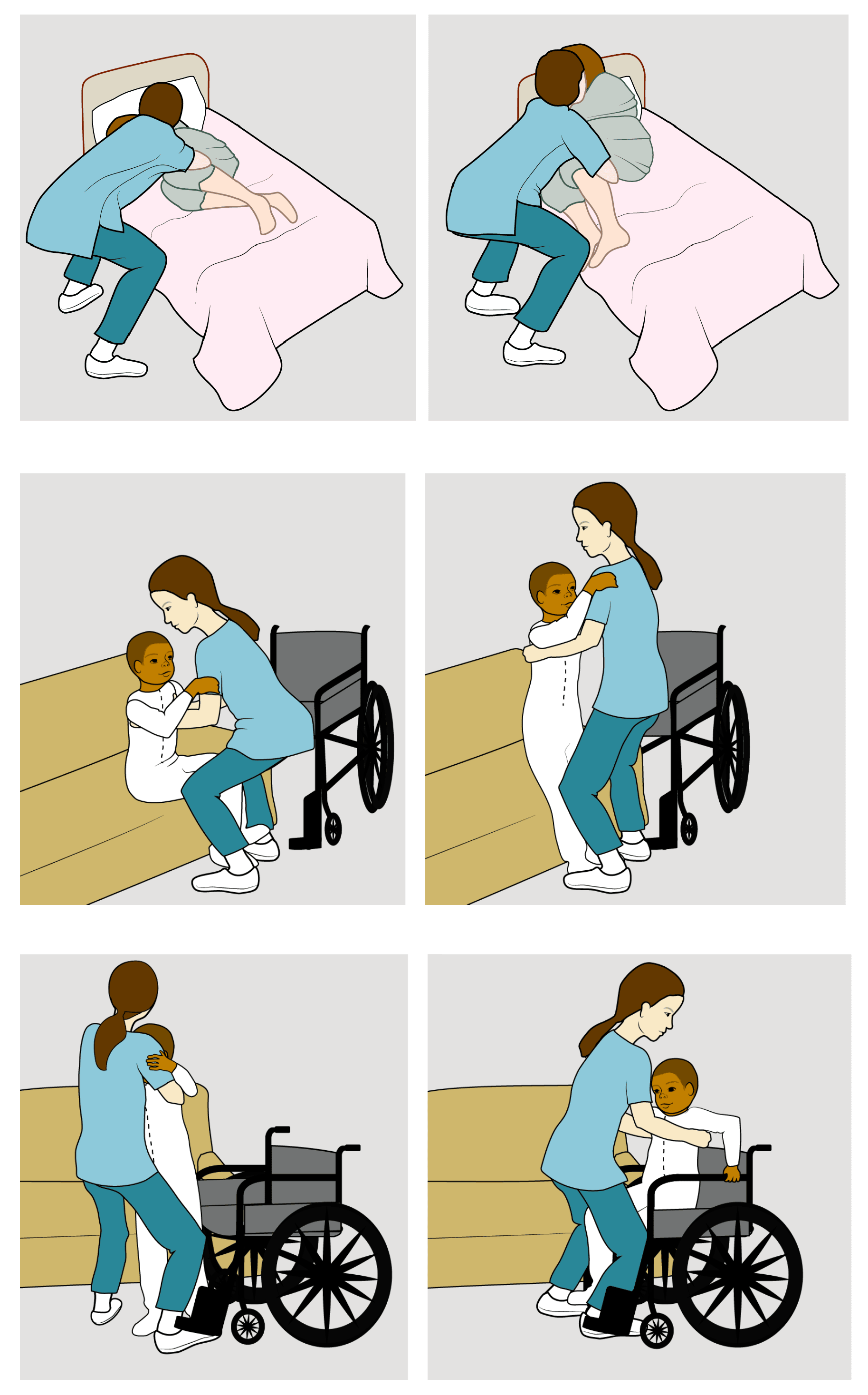
2. Nurses’ Activities and Injuries Due to Specific Movements during Manual Handling of Patients
Why Are Good Handling Techniques Not Sufficient to Avoid Injuries?
- Distance: It is much easier to lift something if it is very close to the body. However, the environment (bed, chair) can get in the way. Thus, nurses cannot get close to patients.
- Bending: The majority of the force goes from bones along the spine directly to disks in the back, straining them.
- Repetition: Each time a nurse lifts and moves a patient, there’s a risk of developing small tears inside disks in the back.
3. The Needs of Nurses to Be Addressed to Overcome the Challenges of Manual Handling
3.1. Comfort, Size, Body Shape, Cleanliness
3.2. Mechanical Aspects: Kinematics, Power, Simple Design
4. Review of Exoskeletons
4.1. Comfort, Size, Body Shape, Cleanliness
4.2. Mechanical Aspects: Kinematics, Power, Simple Design
4.3. Comparison of Available Exoskeletons
4.4. Recap
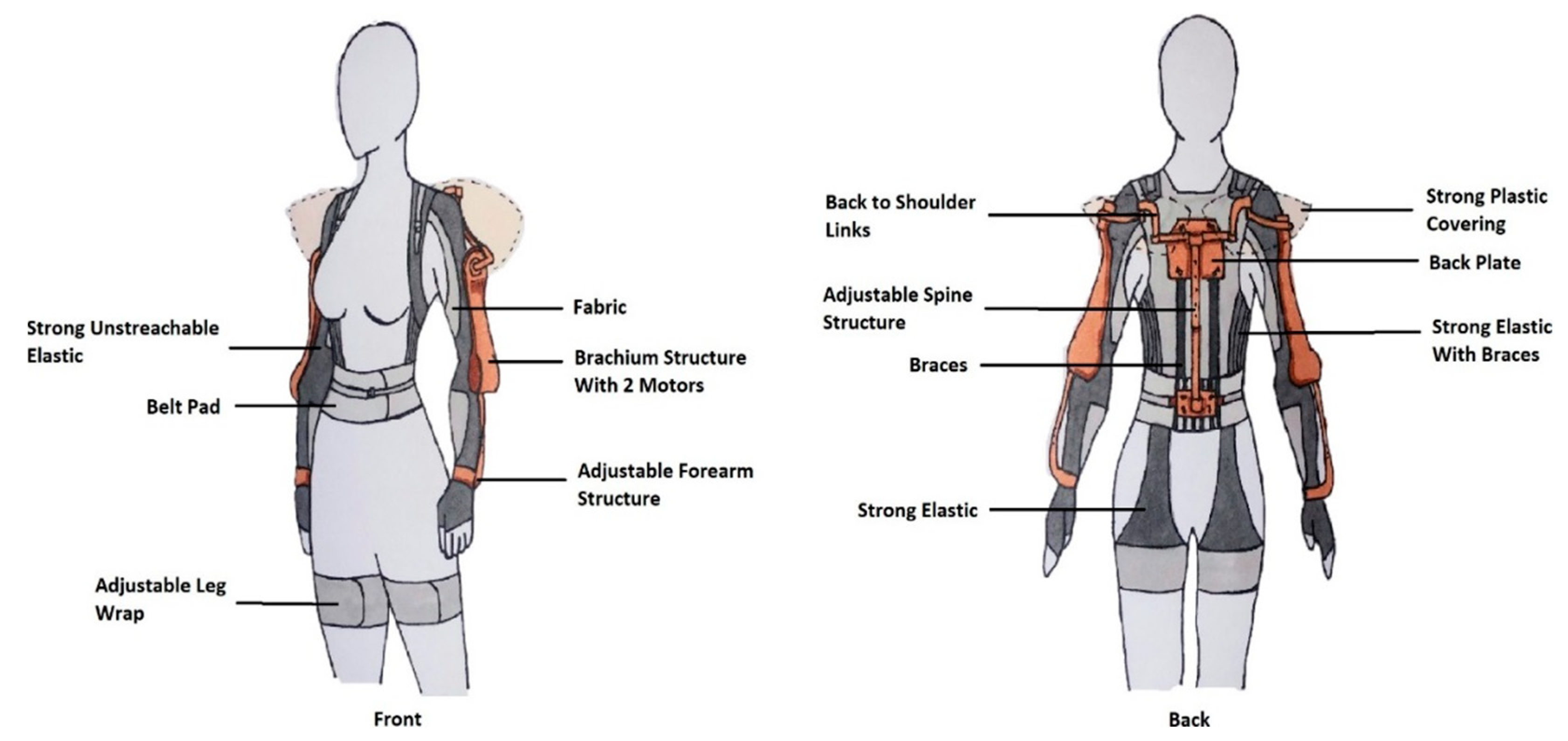
5. Most Important Characteristics and Preliminary Conceptual Design of an Exoskeleton for Nurses
- Design with a focus on women’s body shape,
- Pressure redistribution considering women’ sensitive areas,
- Patient friendly,
- Adjustable level of assistance,
- Allow twisting and bending motions,
- Lightweight and portable,
- Easy to wash and disinfect,
- Compact and intuitive system.
- Design with a focus on women
- Adjustable level of assistance to the arms with the actuators
- Patient friendly as the electric components are hidden and as there is no bulky structure on the front side of the user
- Lightweight and portable as a great part of it is made of light elastic material
- Allows twisting and bending motions
- Easy to wash and disinfect
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Smedley, J.; I Kryger, A.; Andersen, J.H.; Lassen, C.F.; A Brandt, L.P.; Vilstrup, I.; Overgaard, E.; Thomsen, J.F.; Mikkelsen, S. Risk factors for incident neck and shoulder pain in hospital nurses. Occup. Environ. Med. 2002, 60, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Ruiter, H.P.; Liaschenko, J. Patient-handling practices: To lift or not to lift. AAOHN J. 2011, 59, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Spine Research Institute. Even ‘Proper’ Technique Exposes Nurses’ Spines to Dangerous Forces. 2015. Available online: https://www.npr.org/2015/02/11/383564180/even-proper-technique-exposes-nurses-spines-to-dangerous-forces (accessed on 13 August 2020).
- Holtermann, A.; Clausen, T.; Jorgensen, M.B.; Burdorf, A.; Andersen, L. Patient handling and risk for developing persistent low-back pain among female healthcare workers. Natl. Libr. Med. 2013, 39, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Winkelmolen, G.H.; Landeweerd, J.A.; Drost, M.R. An evaluation of patient lifting techniques. Natl. Libr. Med. 1994, 37, 921–932. [Google Scholar] [CrossRef]
- Ulin, S.S.; Chaffin, D.B.; Patellos, C.L.; Blitz, S.G.; Emerick, C.A.; Lundy, F.; Misher, L.A. biomechanical analysis of methods used for transferring totally dependent patients. Natl. Libr. Med. 1997, 14, 19–27. [Google Scholar]
- National Health Service. Musculoskeletal Injuries in Healthcare Staff; Library Knowledge Services (North): Bristol, UK, 2018; Available online: https://www.lksnorth.nhs.uk/search-strategies-repository/musculoskeletal-injuries-in-healthcare-staff/ (accessed on 28 October 2020).
- Gov UK; Department of Health and Social Care. Tackling Obesity: Empowering Adults and Children to Live Healthier Lives; Gov UK; Department of Health and Social Care: London, UK, 2020.
- Great Britain National Audit Office. Tackling Obesity in England; The Stationery Office Books: London, UK, 2001; ISBN 9780102814019/0102814015.
- Scottish Government. The Scottish Health Survey 2008; Scottish Government: Edinburgh, UK, 2009; ISBN 9780755981076. Available online: https://www.gov.scot/publications/scottish-health-survey-2008/pages/77/ (accessed on 30 September 2020).
- Baker, C. Adult Obesity in England. 2017. Available online: https://commonslibrary.parliament.uk/research-briefings/sn03336/ (accessed on 29 August 2020).
- Doncaster, R.; Humber, S. Bariatric Policy. 2020. Available online: https://www.rdash.nhs.uk/wp-content/uploads/2014/04/Bariatric-Policy-v4.2.pdf (accessed on 3 October 2020).
- Menzel, N.; Brooks, S.; Bernard, E. Manual Handling Workload and Musculoskeletal Discomfort in Nursing Personnel. Ph.D. Thesis, University of South Florida, Tampa, FL, USA, 2001. Available online: https://digitalcommons.usf.edu/etd/1540/ (accessed on 19 August 2020).
- Health and Safety Executive. Moving and Handling Equipment. 2011. Available online: https://www.hse.gov.uk/healthservices/moving-handling-equipment.htm (accessed on 19 August 2020).
- Wilson, T.P.; Davis, K.G.; Kotowski, S.E.; Daraiseh, N. Quantification of patient and equipment handling for nurses through direct observation and subjective perceptions. Adv. Nurs. 2015, 2015, 928538. [Google Scholar] [CrossRef]
- Freiberg, A.; Euler, U.; Girbig, M.; Nienhaus, A.; Freitag, S.; Seidler, A. Does the use of small aids during patient handling activities lead to a decreased occurrence of musculoskeletal complaints and diseases? a systematic review. Natl. Libr. Med. 2016, 89, 547–559. [Google Scholar] [CrossRef]
- Toyama, S.; Yonetake, J. Development of the Ultrasonic Motor-Powered Assisted Suit System. In Proceedings of the 2007 IEEE/ICME International Conference on Complex Medical Engineering, Beijing, China, 23–27 May 2007. [Google Scholar] [CrossRef]
- Zhang, T.; Huang, H.H. A Lower-Back Robotic Exoskeleton: Industrial Handling Augmentation Used to Provide Spinal Support. IEEE Robot. Autom. Mag. 2018, 25, 95–106. [Google Scholar] [CrossRef]
- Royal College of Nursing. The UK Nursing Labour Market Review 2018; Royal College of Nursing: London, UK, 2018. [Google Scholar]
- Krupenevich, R.; Rider, P.; Domire, Z.; DeVita, P. Males and Females Respond Similarly to Walking with a Standardized, Heavy Load. Mil. Med. 2015, 180, 994–1000. [Google Scholar] [CrossRef]
- O’Connor, S. Exoskeletons in Nursing and Healthcare: A Bionic Future; SAGE: Newcastle upon Tyne, UK, 2021. [Google Scholar]
- National Health Service. How to Move, Lift and Handle Someone Else. 2018. Available online: https://www.nhs.uk/conditions/social-care-and-support-guide/practical-tips-if-you-care-for-someone/how-to-move-lift-and-handle-someone-else/ (accessed on 26 September 2020).
- Knibbe, J.J.; Friele, R.D. The use of logs to assess exposure to manual handling of patients, illustrated in an intervention study in home care nursing. Int. J. Ind. Ergon. 1999, 24, 445–454. [Google Scholar] [CrossRef] [Green Version]
- National Health Service. Moving and Handling Policy. Available online: https://www.nhft.nhs.uk/download.cfm?doc=docm93jijm4n825 (accessed on 2 November 2020).
- Choi, S.; Brings, K. Work-related musculoskeletal risks associated with nurses and nursing assistants handling overweight and obese patients: A literature review. Work 2016, 53, 439–448. [Google Scholar] [CrossRef]
- Marras, W.; Granata, K. Spine loading during trunk lateral bending motions. J. Biomech. 1997, 30, 697–703. [Google Scholar] [CrossRef]
- Cambridge Dictionary. Musculoskeletal; Cambridge University Press: Cambridge, UK, 2021; Available online: https://dictionary.cambridge.org/dictionary/english/musculoskeletal (accessed on 15 September 2020).
- Smedley, J.; Egger, P.; Cooper, C.; Coggon, D. Manual handling activities and risk of low back pain in nurses. Occup. Environ. Med. 1995, 52, 160–163. [Google Scholar] [CrossRef]
- Daynard, D.; Yassi, A.; Cooper, J.; Tate, R.; Norman, R.; Wells, R. Biomechanical analysis of peak and cumulative spinal loads during simulated patient-handling activities: A substudy of a randomized controlled trial to prevent lift and transfer injury of health care workers. Appl. Ergon. 2001, 32, 199–214. [Google Scholar] [CrossRef]
- Warming, S.; Precht, D.; Suadicani, P.; Ebbehøj, N. Musculoskeletal complaints among nurses related to patient handling tasks and psychosocial factors—Based on logbook registrations. Appl. Ergon. 2009, 40, 569–576. [Google Scholar] [CrossRef]
- Retsas, A.; Pinikahana, J. Manual handling activities and injuries among nurses: An Australian hospital study. J. Adv. Nurs. 2000, 31, 875–883. [Google Scholar] [CrossRef]
- Herbison, G.P.; DMcBride Derrett, S.; Harcombe, H. Musculoskeletal disorders among nurses compared with two other occupational groups. Occup. Med. 2014, 64, 601–607. [Google Scholar] [CrossRef]
- Richardson, A.; McNoe, B.; Derrett, S.; Harcombe, H. Interventions to prevent and reduce the impact of musculoskeletal injuries among nurses: A systematic review. Int. J. Nurs. Stud. 2018, 82, 58–67. [Google Scholar] [CrossRef]
- Trinkoff, A.M.; Lipscomb, J.A.; Geiger-Brown, J.; Brady, B. Musculoskeletal problems of the neck, shoulder, and back and functional consequences in nurses. Am. J. Ind. Med. 2002, 41, 170–178. [Google Scholar] [CrossRef]
- Marras, W.S.; Davis, K.G.; Kirking, B.C.; Bertsche, P.K. A comprehensive analysis of low-back disorder risk and spinal loading during the transferring and repositioning of patients using different techniques. Ergonomics 2001, 42, 904–926. [Google Scholar] [CrossRef]
- Trinkoff, A.M.; Geiger-Brown, J.M.; Caruso, C.C.; Lipscomb, J.A.; Johantgen, M.; Nelson, A.L.; Sattler, B.A.; Selby, V.L. Patient Safety and Quality: An Evidence-Based Handbook for Nurses; AHRQ Publication: Rockville, MD, USA, 2008. [Google Scholar]
- University North Dakota State. Safe Patient Handling. Available online: https://www.ndsu.edu/pubweb/bismarcknursing/basic/skill/D004.html (accessed on 5 July 2022).
- Accident Compensation Corporation New Zealand. Moving and Handling People Guidelines, Section 04—Techniques. 2012. Available online: https://www.acc.co.nz/assets/provider/6ab7b70c43/acc6075-moving-guide-technique.pdf (accessed on 5 July 2022).
- Daniel, K.P.; Stuart, J.F. Lifting Techniques for Home Caregivers, American Company of Orthopaedic Surgeons. 2020. Available online: https://orthoinfo.aaos.org/en/staying-healthy/lifting-techniques-for-home-caregivers (accessed on 5 July 2022).
- Barr, A.E.; Barbe, M.F.; Clark, B.D. Work-Related Musculoskeletal Disorders of the Hand and Wrist: Epidemiology, Pathophysiology, and Sensorimotor Changes. J. Orthop. Sports Phys. Ther. 2006, 34, 610–627. [Google Scholar] [CrossRef] [PubMed]
- Coates, S.; Tanna, P.; Scott-Allen, E. Overview of the UK Population: August 2019. 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/overviewoftheukpopulation/august2019 (accessed on 1 December 2020).
- Jung, J. Obesity—the new majority. Case Manag. 2004, 15, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Galinsky, T.; Hudock, S.; Streit, J. Addressing the Need for Research on Bariatric Patient. Rehabil. Nurs. 2010, 35, 242–247. [Google Scholar] [CrossRef]
- Hignett, S.; Chipchase, S.; Tetley, A.; Griffiths, P. Risk Assessment and Process Planning for Bariatric Patient Handling Pathways; UK Health and Safety Executive. 2007. Available online: https://www.hse.gov.uk/research/rrhtm/rr573.htm (accessed on 5 July 2022).
- Menzel, N.N.; Brooks, S.M.; Bernard, T.E.; Nelson, A. The physical workload of nursing personnel: Association with musculoskeletal discomfort. Int. J. Nurs. Stud. 2004, 41, 859–867. [Google Scholar] [CrossRef]
- Wilson, A.B. Limb Prosthetics; R.E. Krieger Pub. Co.: Huntington, NY, USA, 1972. [Google Scholar]
- Baltrusch, S.J.; Houdijk, H.; van Dieen, J.; Van Bennekom, C.A.M.; Kruif, D.A. Perspectives of End Users on the Potential Use of Trunk Exoskeletons for People with Low-Back Pain: A Focus Group Study. Hum. Factors J. Hum. Factors Ergon. Soc. 2020, 62, 365–376. [Google Scholar] [CrossRef]
- Ulrey, B.L.; Fathallah, F.A. Subject-specific, whole-body models of the stooped posture with a personal weight transfer device. J. Electromyogr. Kinesiol. 2012, 23, 206–215. [Google Scholar] [CrossRef]
- Hill, D.; Holloway, C.S.; Ramirez, D.Z.M.; Smitham, P.; Pappas, Y. What are user perspectives of exoskeleton technology? a literature review. Int. J. Technol. Assess. Health Care 2017, 33, 160–167. [Google Scholar] [CrossRef]
- De Rossi, S.M.M.; Vitiello, N.; Lenzi, T.; Ronsse, R.; Koopman, B.; Persichetti, A.; Vecchi, F.; Ijspeert, A.J.; Van der Kooij, H.; Carrozza, M.C. Sensing Pressure Distribution on a Lower-Limb Exoskeleton Physical Human-Machine Interface. Sensors 2011, 11, 207–227. [Google Scholar] [CrossRef]
- Kristen, H.; Michiel, L.; Tim, B.; Toxiri, S.; O′Sullivan, L.W. Assessment of an active industrial exoskeleton to aid dynamic lifting and lowering manual handling tasks. Appl. Ergon. 2018, 68, 125–131. [Google Scholar]
- Bosch, T.; van Eck, J.; Knitel, K.; de Looze, M. The effects of a passive exoskeleton on muscle activity, discomfort and endurance time in forward bending work. Appl. Ergon. 2016, 54, 212–217. [Google Scholar] [CrossRef]
- Hyundai. Hyundai Develops Wearable Vest Exoskeleton for Overhead Work. 2019. Available online: https://www.hyundai.news/eu/brand/hyundai-develops-wearable-vest-exoskeleton-for-overhead-work/ (accessed on 10 September 2020).
- Tashiro, T.; Aoki, K.; Lee, Y.; Sakaki, T. Research and development of wearable auxiliary tool for behavior assistance of elderly who requires nursing care. In Proceedings of the 2017 17th International Conference on Control, Automation and Systems (ICCAS), Jeju, Korea, 18–21 October 2017. [Google Scholar] [CrossRef]
- Nathanael, J.; Guillaume, M. Connecting a Human limb to an exoskeleton. IEEE Trans. Robot. 2011, 28, 697–709. [Google Scholar]
- Mark, T.; David, W.; Felix, M.G.; Christophe, M.; Urs, S.; Thomas, B. Biomechanical Model-Based Development of an Active Occupational Upper-Limb Exoskeleton to Support Healthcare Workers in the Surgery Waiting Room. Int. J. Environ. Res. Public Health 2020, 17, 5140. [Google Scholar]
- Lamers, E.P.; Yang, A.J.; Zelik, K.E. Feasibility of a Biomechanically-Assistive Garment to Reduce Low Back Loading During Leaning and Lifting. IEEE Trans. Biomed. Eng. 2018, 65, 1674–1680. [Google Scholar] [CrossRef]
- Hara, H.; Sankai, Y. Development of HAL for lumbar support. In Proceedings of the SCIS and ISIS 2010-Joint 5th International Conference on Soft Computing and Intelligent Systems and 11th International Symposium on Advanced Intelligent Systems, Okayama, Japan, 8–12 December 2010. [Google Scholar] [CrossRef]
- Lotz, C.A.; Agnew, M.J.; Godwin, A.A.; Stevenson, J.M. The effect of an on-body personal lift assist device (PLAD) on fatigue during a repetitive lifting task. J. Electromyogr. Kinesiol. 2009, 19, 331–340. [Google Scholar] [CrossRef]
- Baltrusch, S.J.; Van Dieen, J.H.; Van Bennekom, C.A.; Houdijk, H. Testing an Exoskeleton That Helps Workers With Low-Back Pain: Less Discomfort With the Passive SPEXOR Trunk Device. IEEE Robot. Autom. Mag. 2020, 27, 66–76. [Google Scholar] [CrossRef]
- Imamura, Y.; Tanaka, T.; Ayusawa, K.; Yoshida, E. Verification of Assistive Effect Generated by Passive Power-Assist Device Using Humanoid Robot. In Proceedings of the 2014 IEEE/SICE International Symposium on System Integration, Tokyo, Japan, 13–15 December 2014. [Google Scholar] [CrossRef]
- Naruse, K.; Kawai, S.; Kukichi, T. Three-dimensional lifting-up motion analysis for wearable power assist device of lower back support. In Proceedings of the 2005 IEEE/RSJ International Conference on Intelligent Robots and Systems, Edmonton, AB, Canada, 2–6 August 2005. [Google Scholar] [CrossRef]
- Rosales, I.; Lopez, R.; Aguilar, H.; Cordero, A.; Salazar, S.; Lozano, R. Design and modelling of a backbone pneumatic exoskeleton. In Proceedings of the 2014 18th International Conference on System Theory, Control and Computing (ICSTCC), Sinaia, Romania, 17–19 October 2014. [Google Scholar]
- Pauline, M.; Jernej, C.; Dasa, G.; Benjamin, S.; Jonas, B.; Luca, T. Objective and Subjective Effects of a Passive Exoskeleton on Overhead Work. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 28, 152–164. [Google Scholar]
- Yu, S.; Huang, T.-H.; Wang, D.; Lynn, B.P.; Sayd, D.; Silivanov, V.; Park, Y.S.; Tian, Y.; Su, H. Design and Control of a High-Torque and Highly Backdrivable Hybrid Soft Exoskeleton for Knee Injury Prevention During Squatting. IEEE Robot. Autom. Lett. 2019, 4, 4579–4586. [Google Scholar] [CrossRef]
- Be’har, Y.; Superflex. Aura Powered Suit. 2017. Available online: https://www.designboom.com/technology/yves-behar-aura-powered-suit-superflex-01-11-2017/ (accessed on 21 January 2021).
- Didelot, A.; Barde, S.; Malikov, S.; Sellal, J.M.; Aubet-Cuvelier, A.; Wiolande, L. The use of exoskeletons to help with prone positioning in the intensive care unit during COVID-19. Sci. Direct Phys. Rehabil. Med. 2020, 63, 379–382. [Google Scholar] [CrossRef]
- Corfor. 2016. Available online: https://www.corfor.fr/ (accessed on 27 November 2020).
- Suit, X. An Effective and Affordable Exoskeleton That Reduces the Risk of Work-Related Back Injuries. 2019. Available online: https://www.suitx.com/backx (accessed on 16 December 2020).
- Toxiri, S.; Verstraten, T.; Calanca, A.; Caldwell, D.G.; Ortiz, J. Using parallel elasticity in back-support exoskeletons: A study on energy consumption during industrial lifting tasks. In Proceedings of the 2019 Wearable Robotics Association Conference (WearRAcon), Scottsdale, AZ, USA, 25–27 March 2019. [Google Scholar]
- Zhang, J.; Fiers, P.; Witte, K.A.; Jackson, R.W.; Poggensee, K.L.; Atkeson, C.G.; Collins, S. Human-in-the-loop optimization of exoskeleton assistance during walking. Science 2017, 356, 1280–1284. [Google Scholar] [CrossRef]
- Herowear: Technology for All. 2020. Available online: https://herowearexo.com/ (accessed on 17 November 2020).
- Han, M.; Li, T.; Wang, S.; Ma, T.; Ai, N. Design of a booster exoskeleton for lumbar spine protection of physical workers. In Proceedings of the IEEE International Conference on Mechatronics and Automation, Tianjin, China, 4–7 August 2019. [Google Scholar] [CrossRef]
- Haning, S.L.; Schwerha, D.J. Women and Exoskeletons: Design and Its Effect on Fit and Comfort. Masters’ Thesis, The Russ College of Engineering and Technology of Ohio University, Athens, OH, USA, 2019. [Google Scholar]
- Yang, X.; Huang, T.H.; Hu, H.; Yu, S.; Zhang, S.; Zhou, X.; Carriero, A.; Yue, G.; Su, H. Spine-Inspired Continuum Soft Exoskeleton for Stoop Lifting Assistance. IEEE Robot. Autom. Lett. 2019, 4, 4547–4554. [Google Scholar] [CrossRef]
- Taal, S.R.; Sankai, Y. Practical design of full body exoskeletons. In Proceedings of the International Conference on Biomedical Electronics and Devices, Valencia, Spain, 20–23 January 2010. [Google Scholar]
- Full Body Powered Exoskeleton. 2019. Available online: https://www.sarcos.com/products/guardian-xo-powered-exoskeleton/ (accessed on 18 September 2020).
- German Bionics. Crayx. Available online: https://www.germanbionic.com/en/crayx/ (accessed on 22 October 2020).
- Baltrusch, S.; van Dieën, J.; van Bennekom, C.; Houdijk, H. The effect of a passive trunk exoskeleton on functional performance in healthy individuals. Appl. Ergon. 2018, 72, 94–106. [Google Scholar] [CrossRef]
- Souza, R.S.; Sanfilippo, F.; Silva, J.R.; Cordero, A.F. Modular exoskeleton design: Requirement engineering with kaos. In Proceedings of the 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 June 2016. [Google Scholar] [CrossRef]
- Ekso Bionics. Ekso Evo. 2019. Available online: https://eksobionics.com/ekso-evo/ (accessed on 18 December 2020).
- Levitate Technologie. Airframe. 2019. Available online: https://www.levitatetech.com/airframe/ (accessed on 30 September 2020).
- Yu, Z.; Zhuo, W.; Chunjie, C.; Tao, F.; Ruimei, S.; Yanjie, L. A lightweight soft exoskeleton in lower LIMB assistance 2020. In Proceedings of the Chinese Automation Congress (CAC), Shanghai, China, 6–8 November 2020. [Google Scholar]
- Domenico, C.; Luca, T.; Michele, X.; Massimiliano, S.; Lorenzo, M.; Antonio, F. An assistive Soft Wrist Exosuit for flexion Movements with an Ergonomic Reinforced Glove. Front. Robot. AI 2020, 7, 595862. [Google Scholar]
- Hongyue, H.; Kai, F.; Huanyi, G.; Xinyu, W.; Chunjie, C. A Novel Control Method of a Soft Exosuit with Plantar Pressure Sensors. In Proceedings of the IEEE 4th International Conference on Advanced Robotics and Mechatronics (ICARM), Toyonaka, Japan, 3–5 July 2019. [Google Scholar]
- Park, E.J.; Akbas, T.; Eckert-Erdheim, A.; Sloot, L.H.; Nuckols, R.W.; Orzel, D.; Schumm, L.; Ellis, T.D.; Awad, L.N.; Walsh, C.J. A Hinge-Free, Non-Restrictive, Lightweight Tethered Exosuit for Knee Extension Assistance During Walking. IEEE Trans. Med. Robot. Bionics 2020, 2, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Hee, D.L.; Heejin, P.; Bak, S.; Tae, H.K. Development of a Soft Exosuit System for Walking Assistance During Stair Ascent and Descent. Int. J. Control. Autom. Syst. 2020, 18, 2678–2686. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bedroom | Bathroom | Elsewhere |
|---|---|---|
| - Sitting up or moving up in bed | - Bathing | - Sitting in a chair |
| - Transfer from a bed to chair or vice versa | - Showering | - Standing |
| - Getting in or out of bed | - Using the toilet | - Walking |
| - Turning over in bed | - Getting up from the floor after a fall | |
| - Getting in and out of a vehicle |
| Height (cm) | Back | Waist | Brachium | Forearm | Thigh | Shoulder | |
|---|---|---|---|---|---|---|---|
| Women | 161.5 | 48 | 35 | 31 | 24 | 17 | 39 |
| Nurses | 163.9 | 49 | 36 | 32 | 25 | 18 | 40 |
| Advantages | Disadvantages | |
|---|---|---|
| Powered-Rigid Exoskeletons [17,18,57,58,62,63,70,77] |
|
|
| Passive Exoskeletons [48,50,54,69,81,82] |
|
|
| Soft Exoskeletons[57,61,66,68,83,84] |
|
|
| Reference | Targeted Users | Body Area Supported | Results Found from Experiments or Simulations | Suggested Solution by the Study |
|---|---|---|---|---|
| Naruse et al. [62] | Physical Workers | Lower-Back | Reduces upper body weight and muscle activity while bending and lifting weight. | Powered exoskeleton (exo) with cable and drum actuator. |
| PAS [17] | Nurses | Shoulders, Lower-Back, Knees | For transfer tasks. | Motor Powered exo made out of plastic for twisting motions. |
| HAL [58] | Nurses | Shoulders, Lower-Back, Hip, Knees | Reduces loads on spine during lifting of heavy weight. Increases user’s strength. | Motor Powered exo that supports hip flexion/extension and reduces trunk flexion. |
| Rosales et al. [63] | Physical Workers | Lower-Back | Reduces loads on spine during lifting of heavy weight. Increases user’s strength. | Powered exo using Pneumatic Artificial Muscles. Uses force sensors for adequate assistance. |
| Tashiro et al. [54] | Nurses | Lower-Back, Elbow joint | Reduces loads on nurses during bath-caring, involving standing and transfer assistance (titling, twisting, and lifting) | Powered exo using Hydraulic Actuators. Focus on patient for the design of the device (bars to grab for patient). |
| Zhang et al. [18] | Physical Workers | Lower-Back, Hip, Knees | Reduces lumbar spine compression during lifting of heavy objects. | Powered exo with motors and series-elastic actuators. |
| Mk2 [70] | Physical Workers | Lower-Back, Hip | Assist lower-back during lifting of heavy objects. | Powered exo with parallel-elastic actuator and unactuated joints. |
| Yu et al. [65] | Physical Workers | Knees | Assists squat and stoop lifting to avoid knee pain. | Powered exo using cable, high-torque motor, and large arm moment. |
| Yang et al. [75] | Physical Workers | Lower-Back | Assists squat and stoop lifting to reduce shear and compression forces on spine by 37% and 40% respectively. | Spine shaped soft powered exo using cable and motor. |
| CrayX [78] | Physical Workers | Lower-Back | Supports heavy lifting. | Motor Powered exo. |
| PLAD [59] | Physical Workers | Lower-Back | Supports user during bending. Lumbar muscle activity reduced by 14%. | Passive exo using Elastic springs system. Exchanges forces with the user at the spine, pelvis, and feet. |
| BNDR [48] | Physical Workers | Lower-Back | Reduces loads on spine during bending by 14%. | Passive exo using springs. Exchanges forces with the user at the chest, and thighs. Reduces torso flexion. |
| LAEVO [52] | Physical Workers, Nurses | Lower-Back | Reduces back muscles activity during bending by 35%. | Passive exo. Transfers loads from lower-back to chest and legs using tubes. |
| SPEXOR [60] | Nurses | Lower-Back | Reduces loads on spine. Assists bending. | Passive exo using springs. Clutch for level of assistance. |
| Han [73] | Physical Workers | Lower-Back | Assists during lifting and transfer tasks. Reduces loads on spine. | Passive exo using com- pression springs’ stored energy. |
| EVO [81] | Physical Workers | Neck, Lower-Back | Provides muscular assistance and prevent injuries. | Passive exo using springs. Different level of assistance. |
| Airframe [82] | Physical Workers | Shoulders, Neck, Upper-Back | Prevents musculoskeletal injuries. Reduces muscles activity. | Passive exo using springs. Different level of assistance. |
| VEX [50] | Physical Workers | Shoulders, Neck, Upper-Back | Assists during heavy lifting. Reduces muscle activity by 30%. | Passive exo using springs. Different level of assistance. |
| SSL [61] | Nurses | Lower-Back | Assists nurses during manual handling. | Soft exo using elastic belts. |
| Aura [64,66] | Elderly | Torso, Lower-Back, Hip, Legs | Assists during standing up and sitting down motions. | Soft exo using artificial muscles and sensors. |
| Lamers et al. [57] | Nurses | Lower-Back | Reduces loads on back. Reduces back muscles activity by 15% during lifting. | Soft exo using elastic bands. Redistributes forces. |
| Yu Z. et al. [83] | Healthy adults | Hip, Legs | Assists during walking. Decreases metabolic rate by 7.3% up to 14.6%. | Soft exo using Bowden cable, and elastics controlled by iterative learning control system. |
| Domenico C., et al. [84] | Physical Workers | Wrist, Hand | Assists during flexion of the hand. Reduces muscle fatigue and activity. | Soft exo using cable-driven actuator. |
| SIAT Soft Exosuit (SSEX) [85] | Healthy adults | Hip, Legs | Assists during walking by decreasing muscle activity. | Cable-driven soft exo with gait analysis. |
| Evelyn J.P, et al. [86] | Adults with difficulty walking | Knees | Assists knee extension when needed while walking. | Soft exo using some rigid components, straps, and Bowden cable. |
| Hee D.L., et al. [87] | Healthy adults, adults with knees difficulty | Knees | Supports knee joint to assist when ascending or descending stairs. Reduces muscles activity. | Soft exo with wire-driven actuator. |
| Type | Support Area for Manual Handling | Adjustable Size | Required Support Provided for Physical Tasks | Use of Sensors to Provide Effective Response | Portable | Washable/Disinfectable | All Day Use | Does Not Interfere | Easy to Put On | Weight | Adjustable Assistance | Easy Interface | Patient Friendly | Low Cost | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1: Soft Exo [57,61,66,68,83,84,85,86,87] | Soft | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Group 2: Commercialized Spring Actuated Passive Exo [50,81,82] | Passive | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Group 3: Passive Exoskeletons [48,54,69] | Passive | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Group 4: Commercialized Full-Body Powered Exoskeletons [58,77] | Powered | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| Group 5: Powered Exoskeletons for Lower-Back [51,63,78] | Powered | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Group 6: Full-Body Powered Exoskeletons [17,18,62,70] | Powered | ✓ | ✓ | ✓ | ✓ | ✓ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rayssiguie, E.; Erden, M.S. A Review of Exoskeletons Considering Nurses. Sensors 2022, 22, 7035. https://doi.org/10.3390/s22187035
Rayssiguie E, Erden MS. A Review of Exoskeletons Considering Nurses. Sensors. 2022; 22(18):7035. https://doi.org/10.3390/s22187035
Chicago/Turabian StyleRayssiguie, Esther, and Mustafa Suphi Erden. 2022. "A Review of Exoskeletons Considering Nurses" Sensors 22, no. 18: 7035. https://doi.org/10.3390/s22187035
APA StyleRayssiguie, E., & Erden, M. S. (2022). A Review of Exoskeletons Considering Nurses. Sensors, 22(18), 7035. https://doi.org/10.3390/s22187035