
Clinical Impact of Functional CYP2C19 and CYP2D6 Gene Variants on Treatment with Antidepressants in Young People with Depression: A Danish Cohort Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Population
2.2. Associations between the CYP2C19 and CYP2D6 Phenotypes and Clinical Outcomes
2.3. Potential Clinical Validity and Population Impact of PGx Testing
3. Discussion
3.1. Potential Clinical Validity and Population Impact of PGx Testing
3.2. Strengths and Limitations
4. Methods
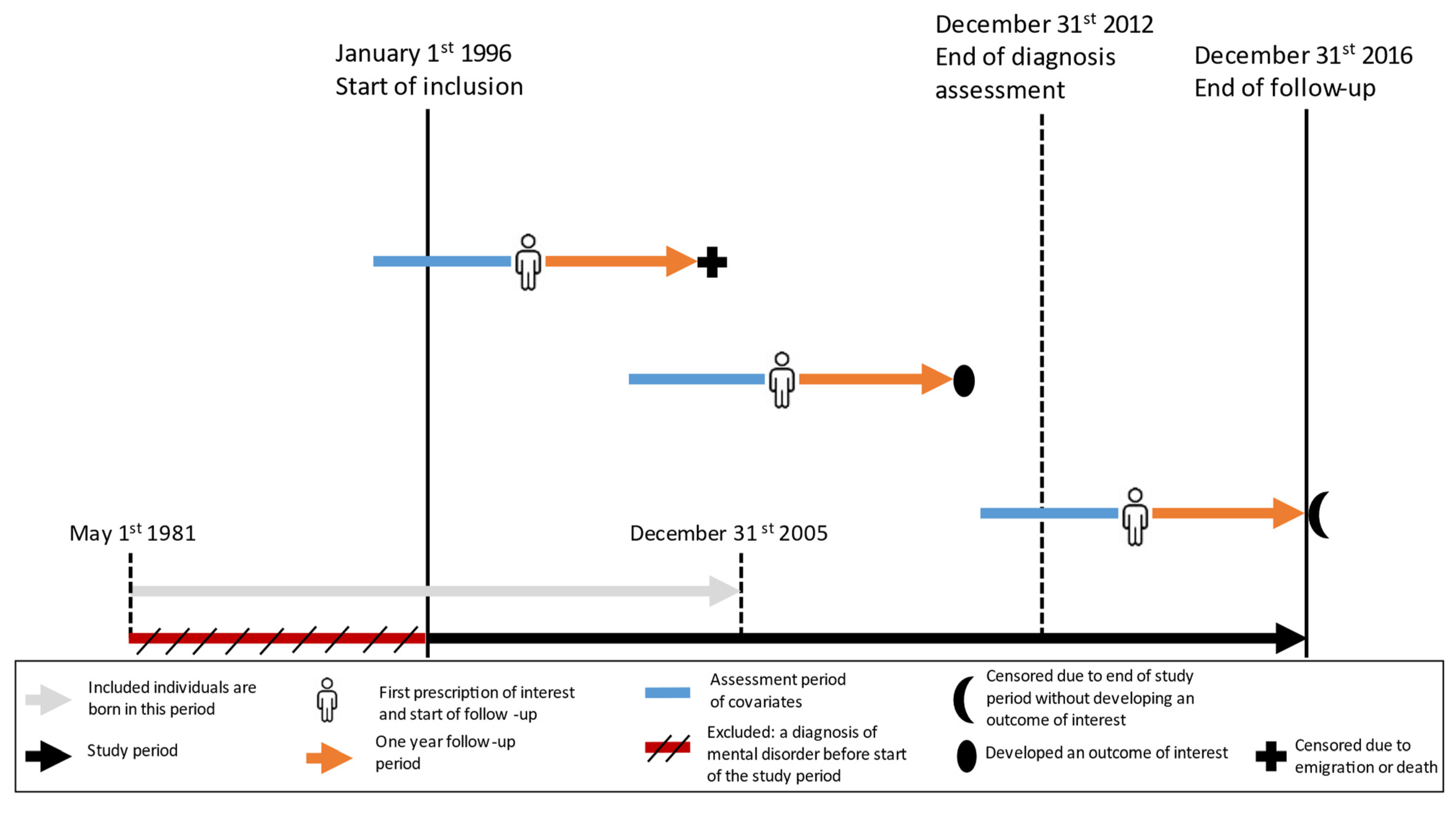
4.1. Study Design and Setting
4.2. Data Sources
4.3. Genotyping and Phenotyping
4.4. Study Population and Study Period
4.5. CYP2C19 and CYP2D6 Genotyping and Phenotyping
4.6. Outcomes
4.7. Covariates
4.8. Statistical Analyses
4.9. Data Protection
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- McAllister-Williams, R.H.; Arango, C.; Blier, P.; Demyttenaere, K.; Falkai, P.; Gorwood, P.; Hopwood, M.; Javed, A.; Kasper, S.; Malhi, G.S.; et al. The identification, assessment and management of difficult-to-treat depression: An international consensus statement. J. Affect Disord. 2020, 267, 264–282. [Google Scholar] [CrossRef] [PubMed]
- Bousman, C.A.; Bengesser, S.A.; Aitchison, K.J.; Amare, A.T.; Aschauer, H.; Baune, B.T.; Behroozi Asl, B.; Bishop, J.R.; Burmeister, M.; Chaumette, B.; et al. Review and consensus on pharmacogenomic testing in psychiatry. Pharmacopsychiatry 2021, 54, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Jukić, M.M.; Haslemo, T.; Molden, E.; Ingelman-Sundberg, M. Impact of CYP2C19 genotype on escitalopram exposure and therapeutic failure: A retrospective study based on 2087 Patients. Am. J. Psychiatry 2018, 175, 463–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milosavljevic, F.; Bukvic, N.; Pavlovic, Z.; Miljevic, C.; Pešic, V.; Molden, E.; Ingelman-Sundberg, M.; Leucht, S.; Jukic, M.M. Association of CYP2C19 and CYP2D6 poor and intermediate metabolizer status with antidepressant and antipsychotic exposure: A systematic review and meta-analysis. JAMA Psychiatry 2021, 78, 270–280. [Google Scholar] [CrossRef]
- Fabbri, C.; Tansey, K.E.; Perlis, R.H.; Hauser, J.; Henigsberg, N.; Maier, W.; Mors, O.; Placentino, A.; Rietschel, M.; Souery, D.; et al. Effect of cytochrome CYP2C19 metabolizing activity on antidepressant response and side effects: Meta-analysis of data from genome-wide association studies. Eur. Neuropsychopharmacol. 2018, 28, 945–954. [Google Scholar] [CrossRef]
- Lunenburg, C.A.; Gasse, C. Pharmacogenetics in psychiatric care, a call for uptake of available applications. Psychiatry Res. 2020, 292, 113336. [Google Scholar] [CrossRef]
- Schmidt, M.; Hallas, J.; Laursen, M.; Friis, S. Data Resource Profile: Danish online drug use statistics (MEDSTAT). Int. J. Epidemiol. 2016, 45, 1401–1402g. [Google Scholar] [CrossRef] [Green Version]
- Mars, B.; Heron, J.; Kessler, D.; Davies, N.M.; Martin, R.M.; Thomas, K.H.; Gunnell, D. Influences on antidepressant prescribing trends in the UK: 1995–2011. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Milani, S.A.; Raji, M.A.; Chen, L.; Kuo, Y.-F. Trends in the Use of Benzodiazepines, Z-Hypnotics, and Serotonergic Drugs Among US Women and Men Before and During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2131012. [Google Scholar] [CrossRef]
- Whirl-Carrillo, M.; Huddart, R.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Whaley, R.; Klein, T.E. An Evidence-Based Framework for Evaluating Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2021, 110, 563–572. [Google Scholar] [CrossRef]
- Dutch Pharmacogenetics Working Group. Dutch Pharmacogenetics Working Group Guidelines 2018. Available online: https://api.pharmgkb.org/v1/download/file/attachment/DPWG_November_2018.pdf (accessed on 10 July 2022).
- Retsinformation. Vejledning om Medikamentel Behandling af Børn og Unge Med Psykiske Lidelse. 2019. Available online: https://www.retsinformation.dk/eli/retsinfo/2019/9733 (accessed on 10 July 2022).
- Ramsey, L.B.; Bishop, J.R.; Strawn, J.R. Pharmacogenetics of treating pediatric anxiety and depression. Pharmacogenomics 2019, 20, 867–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jürgens, G.; Jacobsen, C.B.; Rasmussen, H.B.; Werge, T.; Nordentoft, M.; Andersen, S.E. Utility and adoption of CYP2D6 and CYP2C19 genotyping and its translation into psychiatric clinical practice. Acta Psychiatr. Scand. 2012, 125, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Tonk, E.C.M.; Gurwitz, D.; Der Zee, A.-H.M.-V.; Janssens, A.C.J.W. Assessment of pharmacogenetic tests: Presenting measures of clinical validity and potential population impact in association studies. Pharmacogenomics 2017, 17, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.E.; Rigter, T.; Rodenburg, W.; Fleur, T.M.C.; Houwink, E.J.F.; Weda, M.; Cornel, M.C. Review of the reported measures of clinical validity and clinical utility as arguments for the implementation of pharmacogenetic testing: A case study of statin-induced muscle toxicity. Front. Pharmacol. 2017, 8, 555. [Google Scholar] [CrossRef] [Green Version]
- Poweleit, E.A.; Aldrich, S.L.; Martin, L.J.; Hahn, D.; Strawn, J.R.; Ramsey, L.B. Pharmacogenetics of sertraline tolerability and response in pediatric anxiety and depressive disorders. J. Child Adolesc. Psychopharmacol. 2019, 29, 348–361. [Google Scholar] [CrossRef]
- Jessel, C.D.; Mostafa, S.; Potiriadis, M.; Everall, I.P.; Gunn, J.M.; Bousman, C.A. Use of antidepressants with pharmacogenetic prescribing guidelines in a 10-year depression cohort of adult primary care patients. Pharm. Genom. 2020, 30, 145–152. [Google Scholar] [CrossRef]
- Aldrich, S.L.; Poweleit, E.A.; Prows, C.A.; Martin, L.J.; Strawn, J.R.; Ramsey, L.B. Influence of CYP2C19 Metabolizer status on escitalopram/citalopram tolerability and response in youth with anxiety and depressive disorders. Front. Pharmacol. 2019, 10, 99. [Google Scholar] [CrossRef]
- Campos, A.I.; Byrne, E.M.; Mitchell, B.L.; Wray, N.R.; Lind, P.A.; Licinio, J.; Medland, S.E.; Martin, N.G.; Hickie, I.B.; Rentería, M.E. Impact of CYP2C19 metaboliser status on SSRI response: A retrospective study of 9500 participants of the Australian Genetics of Depression Study. Pharm. J. 2022, 22, 130–135. [Google Scholar] [CrossRef]
- Chen, Q.-H.; Li, Y.-L.; Hu, Y.-R.; Liang, W.-Y.; Zhang, B. Observing time effect of SSRIs on suicide risk and suicide-related behaviour: A network meta-analysis protocol. BMJ Open 2021, 11, e054479. [Google Scholar] [CrossRef]
- Van der Wouden, C.H.; Cambon-Thomsen, A.; Cecchin, E.; Cheung, K.C.; Dávila-Fajardo, C.L.; Deneer, V.H.; Dolžan, M.; Ingelman-Sundberg, M.; Jönsson, S.; Karlsson, M.O.; et al. Implementing pharmacogenomics in Europe: Design and implementation strategy of the ubiquitous pharmacogenomics consortium. Clin. Pharmacol. Ther. 2017, 101, 341–358. [Google Scholar] [CrossRef] [PubMed]
- Höfer, P.; Schosser, A.; Calati, R.; Serretti, A.; Massat, I.; Kocabas, N.A.; Konstantinidis, A.; Linotte, S.; Mendlewicz, J.; Souery, D.; et al. The impact of Cytochrome P450 CYP1A2, CYP2C9, CYP2C19 and CYP2D6 genes on suicide attempt and suicide risk—A European multicentre study on treatment-resistant major depressive disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Rahikainen, A.L.; Vauhkonen, P.; Pett, H.; Palo, J.U.; Haukka, J.; Ojanperä, I.; Niemi, M.; Sajantila, A. Completed suicides of citalopram users-the role of CYP genotypes and adverse drug interactions. Int. J. Legal Med. 2019, 133, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://medstat.dk/ (accessed on 8 June 2022).
- Gassó, P.; Rodríguez, N.; Mas, S.; Pagerols, M.; Blázquez, A.; Plana, M.T.; Torra, M.; Lázaro, L.; Lafuente, A. Effect of CYP2D6, CYP2C9 and ABCB1 genotypes on fluoxetine plasma concentrations and clinical improvement in children and adolescent patients. Pharm. J. 2014, 14, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.L.; Mulder, R.T.; Joyce, P.R.; Luty, S.E.; Kennedy, M.A. No evidence of increased adverse drug reactions in cytochrome P450CYP2D6 poor metabolizers treated with fluoxetine or nortriptyline. Hum. Psychopharmacol. Clin. Exp. 2004, 19, 17–23. [Google Scholar] [CrossRef]
- Hicks, J.B.; Sangkuhl, K.; Muller, D.J.; Ji, Y.; Leckband, S.G.; Leeder, J.S.; Graham, R.L.; Chiulli, D.L.; LLerena, A.; Skaar, T.C.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. 2015. Available online: https://files.cpicpgx.org/data/guideline/publication/SSRI/2015/25974703.pdf (accessed on 10 July 2022).
- Petrović, J.; Pešić, V.; Lauschke, V.M. Frequencies of clinically important CYP2C19 and CYP2D6 alleles are graded across Europe. Eur. J. Hum. Genet. 2020, 28, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelton, R.C.; Parikh, S.V.; Law, R.A.; Rothschild, A.J.; Thase, M.E.; Dunlop, B.W.; DeBattista, C.; Conway, C.R.; Forester, B.P.; Macaluso, M.; et al. Combinatorial pharmacogenomic algorithm is predictive of citalopram and escitalopram metabolism in patients with major depressive disorder. Psychiatry Res. 2020, 290, 113017. [Google Scholar] [CrossRef]
- Montgomery, S.; Hansen, T.; Kasper, S. Efficacy of escitalopram compared to citalopram: A meta-analysis. Int. J. Neuropsychopharmacol. 2011, 14, 261–268. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, C.B.; Bybjerg-Grauholm, J.; Pedersen, M.G.; Grove, J.; Agerbo, E.; Bækvad-Hansen, M.; Poulsen, J.B.; Hansen, C.S.; McGrath, J.J.; Als, T.D.; et al. The iPSYCH2012 case–cohort sample: New directions for unravelling genetic and environmental architectures of severe mental disorders. Mol. Psychiatr. 2018, 23, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, C.B.; Gøtzsche, H.; Møller, J.O.; Mortensen, P.B. The Danish Civil Registration System. A cohort of eight million persons. Dan. Med. Bull. 2006, 53, 441–449. [Google Scholar] [CrossRef]
- Mors, O.; Perto, G.P.; Mortensen, P.B. The Danish Psychiatric Central Research Register. Scand. J. Public Health 2011, 39, 54–57. [Google Scholar]
- Kildemoes, H.W.; Sørensen, H.T.; Hallas, J. The Danish national prescription registry. Scand. J. Public Health 2011, 39 (Suppl. 7), 38–41. [Google Scholar] [CrossRef] [PubMed]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish national patient register. Scand. J. Public Health 2011, 39 (Suppl. 7), 30–33. [Google Scholar] [CrossRef] [PubMed]
- Helweg-Larsen, K. The Danish Register of Causes of Death. Scand. J. Public Health 2011, 39 (Suppl. 7), 26–29. [Google Scholar]
- Statistics Denmark. Data for Research. Available online: https://www.dst.dk/en/TilSalg/Forskningsservice] (accessed on 10 July 2022).
- Nørgaard-Pedersen, B.; Hougaard, D.M. Storage policies and use of the Danish Newborn Screening Biobank. J. Inherit Metab. Dis. 2007, 30, 530–536. [Google Scholar] [CrossRef]
- 1000 Genome Project. Available online: https://www.internationalgenome.org/category/phase-3/ (accessed on 10 July 2022).
- Broad Institute. Ricopili. Available online: https://data.broadinstitute.org/mpg/ricopili/ (accessed on 10 July 2022).
- Schork, A.J.; Won, H.; Appadurai, V.; Nudel, R.; Gandal, M.; Delaneau, O.; Revsbech Christiansen, M.; Hougaard, D.M.; Bækved-Hansen, M.; Bybjerg-Grauholm, J.; et al. A genome-wide association study of shared risk across psychiatric disorders implicates gene regulation during fetal neurodevelopment. Nat. Neurosci. 2019, 22, 353–361. [Google Scholar] [CrossRef]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerdland, 2004.
- Suissa, S.; Moodie, E.E.M.; Dell’Aniello, S. Prevalent new-user cohort designs for comparative drug effect studies by time-conditional propensity scores. Pharmacoepidemiol. Drug Saf. 2017, 26, 459–468. [Google Scholar] [CrossRef]
- Lunenburg, C.A.T.C.; Thirstrup, J.P.; Bybjerg-Grauholm, J.; Bækvad-Hansen, M.; Hougaard, D.M.; Nordentoft, M.; Werge, T.; Børglum, A.D.; Mors, O.; Mortensen, P.B.; et al. Pharmacogenetic genotype and phenotype frequencies in a large Danish population-based case-cohort sample. Transl. Psychiatry 2021, 11, 294. [Google Scholar] [CrossRef]
- Caudle, K.E.; Dunnenberger, H.M.; Freimuth, R.R.; Peterson, J.F.; Burlison, J.D.; Whirl-Carrillo, M.; Scott, S.A.; Rehm, H.L.; Williams, M.S.; Klein, T.E.; et al. Standardizing terms for clinical pharmacogenetic test results: Consensus terms from the Clinical Pharmacogenetics Implementation Consortium (CPIC). Genet. Med. 2017, 19, 215–223. [Google Scholar] [CrossRef]
- Robarge, J.D.; Li, L.; Desta, Z.; Nguyen, A.; A Flockhart, D. The star-allele nomenclature: Retooling for translational genomics. Clin. Pharmacol. Ther. 2007, 82, 244–248. [Google Scholar] [CrossRef]
- Botton, M.R.; Whirl-Carrillo, M.; Del Tredici, A.L.; Sangkuhl, K.; Cavallari, L.H.; Agúndez, J.A.G.; Duconge, J.; Lee, M.T.M.; Woodahl, E.L.; Claudio-Campos, K.; et al. PharmVar GeneFocus: CYP2C19. Clin. Pharmacol. Ther. 2021, 109, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Nofziger, C.; Turner, A.J.; Sangkuhl, K.; Whirl-Carrillo, M.; Agúndez, J.A.G.; Black, J.L.; Dunnenberger, H.M.; Ruano, G.; Kennedy, M.A.; Phillips, M.S.; et al. PharmVar GeneFocus: CYP2D6. Clin. Pharmacol. Ther. 2020, 107, 154–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasse, C.; Danielsen, A.A.; Pedersen, M.G.; Pedersen, C.B.; Mors, O.; Christensen, J. Positive predictive value of a register-based algorithm using the Danish National Registries to identify suicidal events. Pharmacoepidemiol. Drug Saf. 2018, 27, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Sundhedsstyrelsen. Den Nationale Rekommandationsliste (NRL): Unipolar Depression. 2019. Available online: https://sst.dk/da/viden/laegemidler/anbefalinger/den-nationale-rekommandationsliste-_nrl_/unipolar-depression (accessed on 14 June 2022).
- Carstensen, B.; Dickman, P. Lexis Macro for Splitting Follow-Up 2003. Available online: http://bendixcarstensen/Lexis/ (accessed on 10 July 2022).



{kind=link}
{kind=link}
| Antidepressants | ||||||||
|---|---|---|---|---|---|---|---|---|
| Citalopram, n = 8281 | Escitalopram, n = 2632 | Sertraline, n = 4583 | Fluoxetine, n = 1801 | |||||
| n | (%) | n | (%) | n | (%) | n | (%) | |
| Sex | ||||||||
| Female | 5896 | (71.2) | 1783 | (67.7) | 3164 | (69.0) | 1377 | (76.5) |
| Male | 2385 | (28.8) | 849 | (32.3) | 1419 | (31.0) | 424 | (23.5) |
| Age in groups | ||||||||
| Children/adolescents (≤18 years) | 3111 | (37.6) | 928 | (35.3) | 2513 | (54.8) | 1338 | (74.3) |
| Young adults (19–25 years) | 4263 | (51.5) | 1428 | (54.3) | 1567 | (34.2) | 403 | (22.4) |
| Adults (26+ years) | 907 | (11.0) | 276 | (10.5) | 503 | (11.0) | 60 | (3.3) |
| Mean age in years, (SD) | 20.3 (3.6) | 20.5 (3.4) | 19.2 (4.3) | 17.5 (3.3) | ||||
| Region at index prescription | ||||||||
| Capital Region | 2296 | (27.7) | 787 | (29.9) | 1068 | (23.3) | 514 | (28.5) |
| Middle Jutland | 2029 | (24.5) | 676 | (25.7) | 1161 | (25.3) | 323 | (17.9) |
| North Jutland | 887 | (10.7) | 227 | (8.6) | 574 | (12.5) | 148 | (8.2) |
| Southern Denmark | 1592 | (19.2) | 595 | (22.6) | 1073 | (23.4) | 374 | (20.8) |
| Zealand | 1477 | (17.8) | 347 | (13.2) | 707 | (15.4) | 442 | (24.5) |
| Parents/adults SES * | ||||||||
| Missing | 152 | (1.8) | 23 | (0.9) | 126 | (2.7) | 25 | (1.4) |
| Employed | 3670 | (44.3) | 1256 | (47.7) | 2292 | (50.0) | 1094 | (60.7) |
| On social benefits | 1839 | (22.2) | 465 | (17.7) | 1064 | (23.2) | 309 | (17.2) |
| On study | 1947 | (23.5) | 673 | (25.6) | 782 | (17.1) | 273 | (15.2) |
| Others | 673 | (8.1) | 215 | (8.2) | 319 | (7.0) | 100 | (5.6) |
| Within last year: No. of psychiatric hospital contacts | ||||||||
| 0 | 4965 | (60.0) | 1450 | (55.1) | 2078 | (45.3) | 590 | (32.8) |
| 1 | 1220 | (14.7) | 408 | (15.5) | 844 | (18.4) | 371 | (20.6) |
| 2 | 445 | (5.4) | 143 | (5.4) | 311 | (6.8) | 193 | (10.7) |
| 3 | 213 | (2.6) | 80 | (3.0) | 143 | (3.1) | 68 | (3.8) |
| 4 | 107 | (1.3) | 36 | (1.4) | 100 | (2.2) | 42 | (2.3) |
| >4 | 1331 | (16.1) | 515 | (19.6) | 1107 | (24.2) | 537 | (29.8) |
| Past: No. of past mental diagnoses | ||||||||
| 0 | 2757 | (33.3) | 798 | (30.3) | 952 | (20.8) | 241 | (13.4) |
| 1 | 2511 | (30.3) | 880 | (33.4) | 1217 | (26.6) | 566 | (31.4) |
| 2 | 1648 | (19.9) | 550 | (20.9) | 1169 | (25.5) | 603 | (33.5) |
| 3 | 845 | (10.2) | 268 | (10.2) | 779 | (17.0) | 253 | (14.0) |
| 4 | 361 | (4.4) | 105 | (4.0) | 296 | (6.5) | 96 | (5.3) |
| >4 | 159 | (1.9) | 31 | (1.2) | 170 | (3.7) | 42 | (2.3) |
| Past ever: history of self-harm/suicide attempt | ||||||||
| Yes | 1312 | (15.8) | 431 | (16.4) | 651 | (14.2) | 321 | (17.8) |
| Within last year: history of self-harm/suicide attempt | ||||||||
| Yes | 586 | (7.1) | 206 | (7.8) | 346 | (7.5) | 197 | (10.9) |
| Within last 90ds: strong CYP2D6 inhibitor use | ||||||||
| Yes | 67 | (0.8) | 32 | (1.2) | 66 | (1.4) | 10 | (0.6) |
| Within last 90ds: moderate CYP2D6 inhibitor use | ||||||||
| Yes | 142 | (1.7) | 42 | (1.6) | 77 | (1.7) | 14 | (0.8) |
| Within last 90ds: weak CYP2D6 inhibitor use | ||||||||
| Yes | One of the categories had <5 observations | |||||||
| Within last 90ds: strong CYP2C19 inhibitor use | ||||||||
| Yes | 216 | (2.6) | 73 | (2.8) | 109 | (2.4) | 39 | (2.2) |
| Within last 90ds: moderate CYP2C19 inhibitor use | ||||||||
| No | 8281 | (100.0) | 2632 | (100.0) | 4583 | (100.0) | 1801 | (100.0) |
| Within last 90ds: weak CYP2C19 inhibitor use | ||||||||
| Yes | 189 | (2.3) | 59 | (2.2) | 122 | (2.7) | 41 | (2.3) |
| Within last 90ds: CYP2C19 inducer use | ||||||||
| Yes | All categories had <5 | |||||||
| Within last 90ds: Antiepileptic drug use | ||||||||
| Yes | 80 | (1.0) | 35 | (1.3) | 69 | (1.5) | 13 | (0.7) |
| Year as category of first prescription | ||||||||
| 1995–2001 | 237 | (2.9) | 0 | 0 | 185 | (4.0) | 44 | (2.4) |
| 2001–2005 | 2201 | (26.6) | 524 | (19.9) | 988 | (21.6) | 264 | (14.7) |
| 2006–2010 | 4447 | (53.7) | 1890 | (71.8) | 1931 | (42.1) | 828 | (46.0) |
| 2011–2016 | 1396 | (16.9) | 218 | (8.3) | 1479 | (32.3) | 665 | (36.9) |
| Antidepressants | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total, n = 17,297 | Escitalopram, n = 2632 | Citalopram, n = 8281 | Sertraline, n = 4583 | Fluoxetine, n = 1801 | ||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | |
| CYP2D6 phenotype | ||||||||||
| CYP2D6_NM | 10,770 | (62.3) | 1629 | (61.9) | 5159 | (62.3) | 2855 | (62.3) | 1127 | (62.6) |
| CYP2D6_IM | 5781 | (33.4) | 873 | (33.2) | 2778 | (33.5) | 1533 | (33.4) | 597 | (33.1) |
| CYP2D6_PM | 746 | (4.3) | 130 | (4.9) | 344 | (4.2) | 195 | (4.3) | 77 | (4.3) |
| CYP2C19 phenotype | ||||||||||
| CYP2C19_UM | 678 | (3.9) | 118 | (4.5) | 304 | (3.7) | 194 | (4.2) | 62 | (3.4) |
| CYP2C19_RM | 4483 | (25.9) | 687 | (26.1) | 2168 | (26.2) | 1143 | (24.9) | 485 | (26.9) |
| CYP2C19_NM | 7553 | (43.7) | 1122 | (42.6) | 3600 | (43.5) | 2042 | (44.6) | 789 | (43.8) |
| CYP2C19_IM | 4215 | (24.4) | 652 | (24.8) | 2024 | (24.4) | 1111 | (24.2) | 428 | (23.8) |
| CYP2C19_PM | 368 | (2.1) | 53 | (2) | 185 | (2.2) | 93 | (2) | 37 | (2.1) |
| Age Group | Children and Adolescents | Children and Adolescents | Young Adults | Young Adults | |
| Drug | (Es)citalopram | (Es)citalopram | Sertraline | Fluoxetine | |
| Phenotype | CYP2C19 PM | CYP2C19 PM | CYP2C19 PM | CYP2D6 PM | |
| Risk geno-/phenotype freq. | 2.18% | 2.18% | 2.00% | 4.30% | |
| Outcome | Switching | Suicide Attempt/Self-Harm | Switching | ER Contact | |
| IRR * | 1.64 | 2.67 | 2.06 | 3.28 | |
| RR | 1.46 | 2.15 | 1.57 | ** | |
| RD | 0.09 | 0.1 | 0.11 | ** | |
| Population impact of PGx | PAF | 1.00% | 2.4% | 1.12% | ** |
| NNT | 11 | 11 | 10 | ** | |
| NNG | 503 | 464 | 460 | ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thiele, L.S.; Ishtiak-Ahmed, K.; Thirstrup, J.P.; Agerbo, E.; Lunenburg, C.A.T.C.; Müller, D.J.; Gasse, C. Clinical Impact of Functional CYP2C19 and CYP2D6 Gene Variants on Treatment with Antidepressants in Young People with Depression: A Danish Cohort Study. Pharmaceuticals 2022, 15, 870. https://doi.org/10.3390/ph15070870
Thiele LS, Ishtiak-Ahmed K, Thirstrup JP, Agerbo E, Lunenburg CATC, Müller DJ, Gasse C. Clinical Impact of Functional CYP2C19 and CYP2D6 Gene Variants on Treatment with Antidepressants in Young People with Depression: A Danish Cohort Study. Pharmaceuticals. 2022; 15(7):870. https://doi.org/10.3390/ph15070870
Chicago/Turabian StyleThiele, Liv S., Kazi Ishtiak-Ahmed, Janne P. Thirstrup, Esben Agerbo, Carin A. T. C. Lunenburg, Daniel J. Müller, and Christiane Gasse. 2022. "Clinical Impact of Functional CYP2C19 and CYP2D6 Gene Variants on Treatment with Antidepressants in Young People with Depression: A Danish Cohort Study" Pharmaceuticals 15, no. 7: 870. https://doi.org/10.3390/ph15070870
APA StyleThiele, L. S., Ishtiak-Ahmed, K., Thirstrup, J. P., Agerbo, E., Lunenburg, C. A. T. C., Müller, D. J., & Gasse, C. (2022). Clinical Impact of Functional CYP2C19 and CYP2D6 Gene Variants on Treatment with Antidepressants in Young People with Depression: A Danish Cohort Study. Pharmaceuticals, 15(7), 870. https://doi.org/10.3390/ph15070870