

Individual Treatment Trials—Do Experts Know and Use This Option to Improve the Treatability of Mucopolysaccharidosis?

Abstract
:1. Introduction
2. Results
2.1. Sociodemographic Data
2.2. Contentment with Available Therapy Options
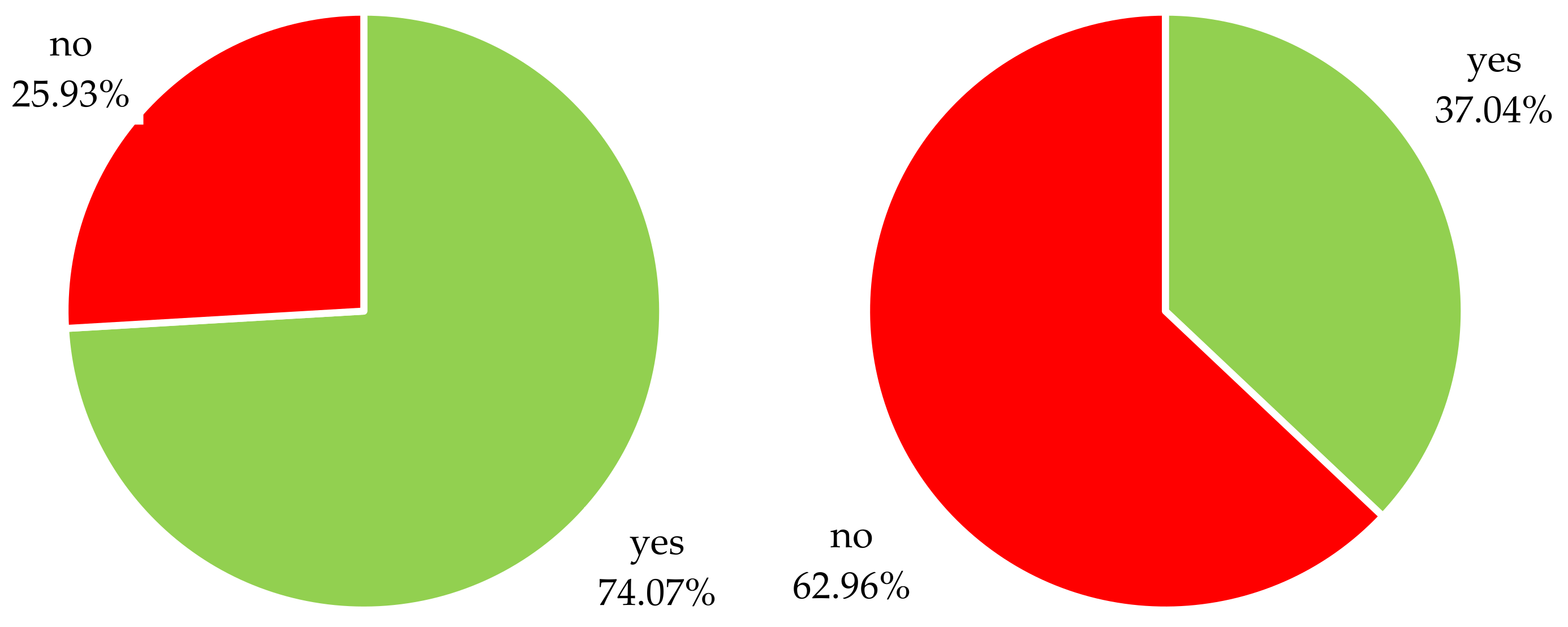
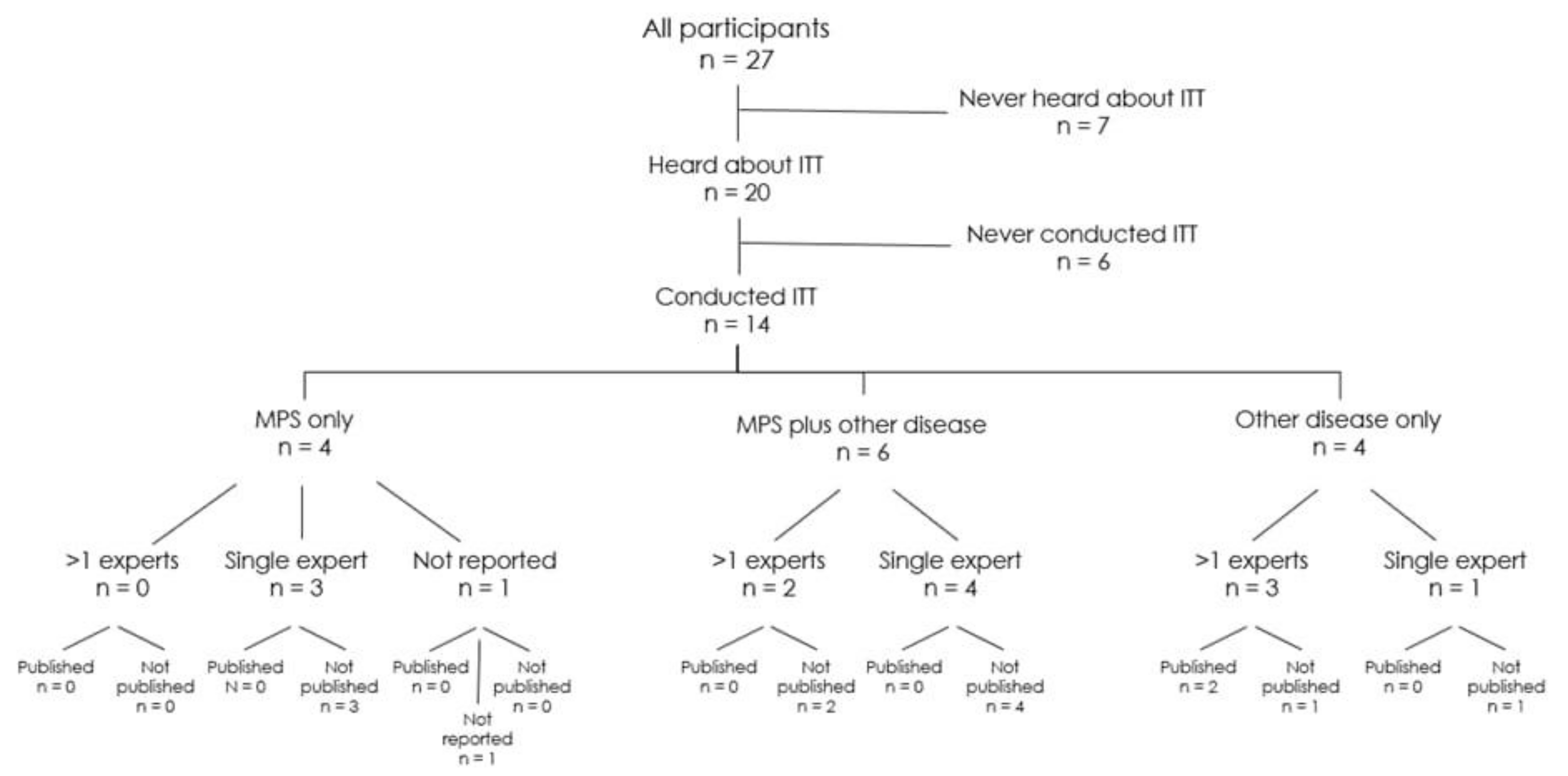
2.3. Familiarity and Utilization of ITTs
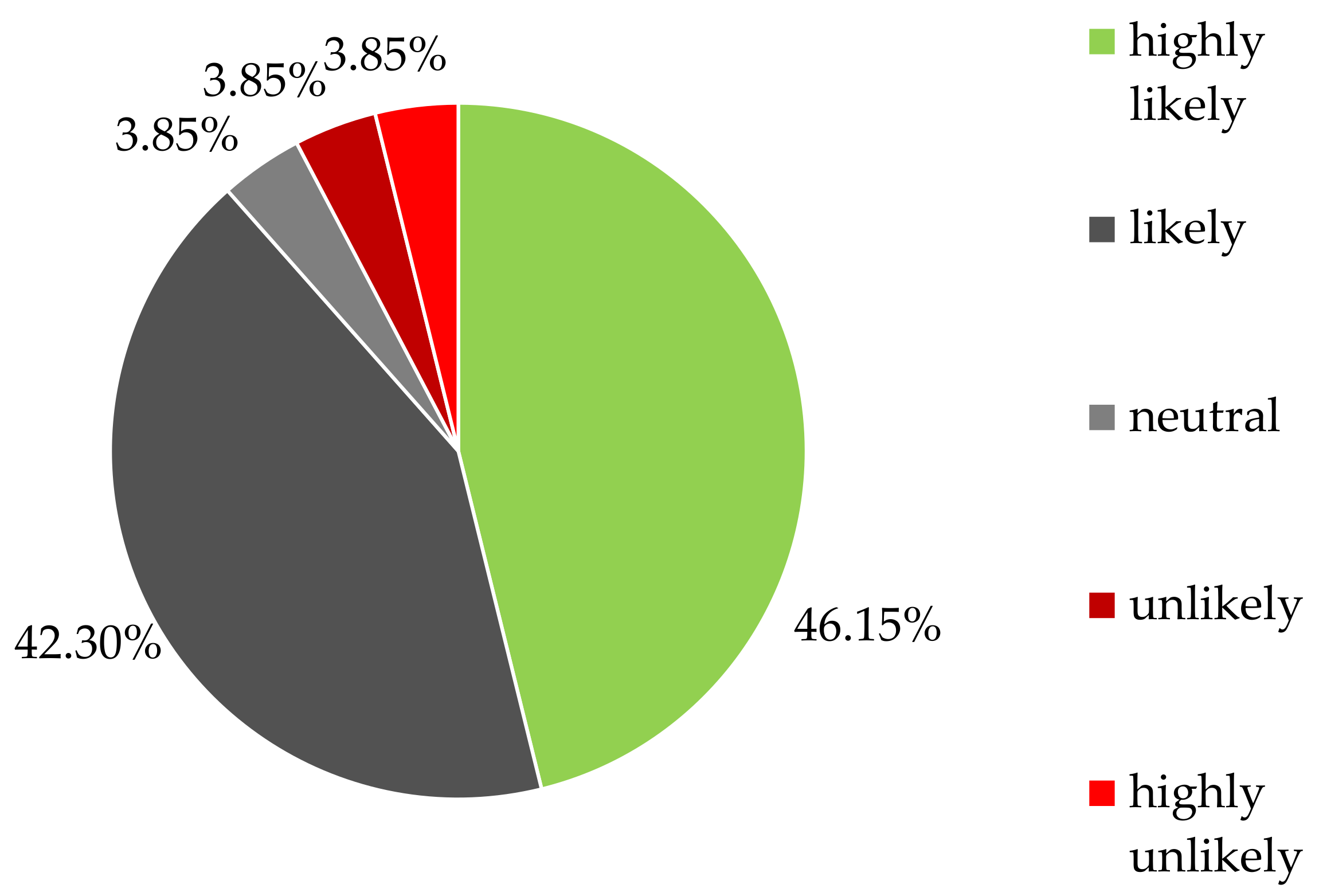
2.4. Willingness to Use a Decision Analysis Framework (DAF) Tool for ITTs in MPS
3. Discussion
4. Methods
4.1. Sampling and Eligibility Criteria
4.2. Data Sources and Instruments
4.2.1. Sociodemographic Data
4.2.2. Satisfaction with Currently Approved MPS Therapies
4.2.3. Knowledge, Awareness, Utilization, and Concerns Regarding ITTs
4.2.4. Necessity of a DAF Tool for ITTs in MPS
4.3. Data Analysis and Synthesis
4.4. Ethics Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, S.A.; Peracha, H.; Ballhausen, D.; Wiesbauer, A.; Rohrbach, M.; Gautschi, M.; Mason, R.W.; Giugliani, R.; Suzuki, Y.; Orii, K.E.; et al. Epidemiology of mucopolysaccharidoses. Mol. Genet. Metab. 2017, 121, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Sawamoto, K.; Álvarez González, J.V.; Piechnik, M.; Otero, F.J.; Couce, M.L.; Suzuki, Y.; Tomatsu, S. Mucopolysaccharidosis IVA: Diagnosis, Treatment, and Management. Int. J. Mol. Sci. 2020, 21, 1517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suarez-Guerrero, J.L.; Gómez Higuera, P.J.; Arias Flórez, J.S.; Contreras-García, G.A. Mucopolysaccharidosis: Clinical features, diagnosis and management. Rev. Chil. Pediatr. 2016, 87, 295–304. [Google Scholar] [CrossRef]
- Neufeld, E.F.; Muenzer, J. The mucopolysaccharidoses. In The Metabolic and Molecular Bases of Inherited Disease, 8th ed.; David Valle, M., Ed.; OMMBID, McGrawHill Medical: New York, NY, USA, 2001; pp. 3421–3451. [Google Scholar]
- Sun, A. Lysosomal storage disease overview. Ann. Transl. Med. 2018, 6, 476. [Google Scholar] [CrossRef]
- Yıldız, Y.; Sivri, H.S. Difficulties Associated with Enzyme Replacement Therapy for Mucopolysaccharidoses. Turk. Arch. Pediatr. 2021, 56, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Lagler, F.B. Innovative Treatments for Mucopolysaccharidoses. J. Child Sci. 2018, 8, e163–e171. [Google Scholar] [CrossRef] [Green Version]
- Concolino, D.; Deodato, F.; Parini, R. Enzyme replacement therapy: Efficacy and limitations. Ital. J. Pediatr. 2018, 44, 120. [Google Scholar] [CrossRef]
- Sonoda, H.; Morimoto, H.; Yoden, E.; Koshimura, Y.; Kinoshita, M.; Golovina, G.; Takagi, H.; Yamamoto, R.; Minami, K.; Mizoguchi, A.; et al. A Blood-Brain-Barrier-Penetrating Anti-human Transferrin Receptor Antibody Fusion Protein for Neuronopathic Mucopolysaccharidosis II. Mol. Ther. 2018, 26, 1366–1374. [Google Scholar] [CrossRef]
- de Castro, M.J.; Del Toro, M.; Giugliani, R.; Couce, M.L. Gene Therapy for Neuronopathic Mucopolysaccharidoses: State of the Art. Int. J. Mol. Sci. 2021, 22, 9200. [Google Scholar] [CrossRef]
- Tomatsu, S.; Alméciga-Díaz, C.J.; Montaño, A.M.; Yabe, H.; Tanaka, A.; Dung, V.C.; Giugliani, R.; Kubaski, F.; Mason, R.W.; Yasuda, E.; et al. Therapies for the bone in mucopolysaccharidoses. Mol. Genet. Metab. 2015, 114, 94–109. [Google Scholar] [CrossRef] [Green Version]
- Taylor, M.; Khan, S.; Stapleton, M.; Wang, J.; Chen, J.; Wynn, R.; Yabe, H.; Chinen, Y.; Boelens, J.J.; Mason, R.W.; et al. Hematopoietic Stem Cell Transplantation for Mucopolysaccharidoses: Past, Present, and Future. Biol. Blood Marrow Transplant. 2019, 25, e226–e246. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Luan, Z.; Jiang, H.; Fang, J.; Qin, M.; Lee, V.; Chen, J. Allogeneic Hematopoietic Stem Cell Transplantation in Thirty-Four Pediatric Cases of Mucopolysaccharidosis-A Ten-Year Report from the China Children Transplant Group. Biol. Blood Marrow Transplant. 2016, 22, 2104–2108. [Google Scholar] [CrossRef] [PubMed]
- Fung, A.; Yue, X.; Wigle, P.R.; Guo, J.J. Off-label medication use in rare pediatric diseases in the United States. Intractable Rare Dis. Res. 2021, 10, 238–245. [Google Scholar] [CrossRef]
- Diel, J.; Heineck, I.; Santos, D.B.D.; Pizzol, T. Off-label use of drugs by age in Brazilian children: A population study. Rev. Bras. Epidemiol. 2020, 23, e200030. [Google Scholar] [CrossRef]
- De Zen, L.; Marchetti, F.; Barbi, E.; Benini, F. Off-label drugs use in pediatric palliative care. Ital. J. Pediatr. 2018, 44, 144. [Google Scholar] [CrossRef] [PubMed]
- Schrier, L.; Hadjipanayis, A.; Stiris, T.; Ross-Russell, R.I.; Valiulis, A.; Turner, M.A.; Zhao, W.; De Cock, P.; de Wildt, S.N.; Allegaert, K.; et al. Off-label use of medicines in neonates, infants, children, and adolescents: A joint policy statement by the European Academy of Paediatrics and the European society for Developmental Perinatal and Pediatric Pharmacology. Eur. J. Pediatr. 2020, 179, 839–847. [Google Scholar] [CrossRef]
- Weda, M.; Hoebert, J.M.; Vervloet, M.; Puigmarti, C.M.; Damen, N.L.; Marchange, S.; Langedijk, J.; Lisman, J.A.; Dijk, L.v. Study on Off-Label Use of Medicinal Products in the European Union; European Comission: Brussels, Belgium, 2017. [Google Scholar]
- Gore, R.; Chugh, P.K.; Tripathi, C.D.; Lhamo, Y.; Gautam, S. Pediatric Off-Label and Unlicensed Drug Use and Its Implications. Curr. Clin. Pharmacol. 2017, 12, 18–25. [Google Scholar] [CrossRef]
- Langhof, H.; Strech, D. Off-Label Use, Compassionate Use und Individuelle Heilversuche: Ethische Implikationen Zulassungsüberschreitender Arzneimittelanwendungen; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Guyatt, G.H.; Heyting, A.; Jaeschke, R.; Keller, J.; Adachi, J.D.; Roberts, R.S. N of 1 randomized trials for investigating new drugs. Control. Clin. Trials 1990, 11, 88–100. [Google Scholar] [CrossRef]
- Kaplan, H.C.; Opipari-Arrigan, L.; Schmid, C.H.; Schuler, C.L.; Saeed, S.; Braly, K.L.; Burgis, J.C.; Nguyen, K.; Pilley, S.; Stone, J.; et al. Evaluating the Comparative Effectiveness of Two Diets in Pediatric Inflammatory Bowel Disease: A Study Protocol for a Series of N-of-1 Trials. Healthcare 2019, 7, 129. [Google Scholar] [CrossRef] [Green Version]
- Samuel, J.; Holder, T.; Molony, D. N-of-1 Trials as a Decision Support Tool in Clinical Practice: A Protocol for a Systematic Literature Review and Narrative Synthesis. Healthcare 2019, 7, 136. [Google Scholar] [CrossRef] [Green Version]
- Clough, A.J.; Hilmer, S.N.; Naismith, S.L.; Gnjidic, D. The Feasibility of Using N-Of-1 Trials to Investigate Deprescribing in Older Adults with Dementia: A Pilot Study. Healthcare 2019, 7, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griggs, R.C.; Batshaw, M.; Dunkle, M.; Gopal-Srivastava, R.; Kaye, E.; Krischer, J.; Nguyen, T.; Paulus, K.; Merkel, P.A. Clinical research for rare disease: Opportunities, challenges, and solutions. Mol. Genet. Metab. 2009, 96, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldevila-Domenech, N.; Boronat, A.; Langohr, K.; de la Torre, R. N-of-1 Clinical Trials in Nutritional Interventions Directed at Improving Cognitive Function. Front. Nutr. 2019, 6, 110. [Google Scholar] [CrossRef]
- Vohra, S.; Shamseer, L.; Sampson, M.; Bukutu, C.; Schmid, C.H.; Tate, R.; Nikles, J.; Zucker, D.R.; Kravitz, R.; Guyatt, G.; et al. CONSORT extension for reporting N-of-1 trials (CENT) 2015 Statement. J. Clin. Epidemiol. 2016, 76, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Margolis, A.; Giuliano, C. Making the switch: From case studies to N-of-1 trials. Epilepsy Behav. Rep. 2019, 12, 100336. [Google Scholar] [CrossRef]
- Bobe, J.R.; De Freitas, J.K.; Glicksberg, B.S. Exploring the Potential for Collaborative Use of an App-Based Platform for n-of-1 Trials Among Healthcare Professionals That Treat Patients With Insomnia. Front. Psychiatry 2020, 11, 530995. [Google Scholar] [CrossRef] [PubMed]
- Scuffham, P.A.; Nikles, J.; Mitchell, G.K.; Yelland, M.J.; Vine, N.; Poulos, C.J.; Pillans, P.I.; Bashford, G.; del Mar, C.; Schluter, P.J.; et al. Using N-of-1 trials to improve patient management and save costs. J. Gen. Intern. Med. 2010, 25, 906–913. [Google Scholar] [CrossRef] [Green Version]
- Kane, P.B.; Bittlinger, M.; Kimmelman, J. Individualized therapy trials: Navigating patient care, research goals and ethics. Nat. Med. 2021, 27, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Wiesinger, A.-M.; Bigger, B.; Giugliani, R.; Scarpa, M.; Moser, T.; Lampe, C.; Kampmann, C.; Lagler, F.B. The Inflammation in the Cytopathology of Patients With Mucopolysaccharidoses- Immunomodulatory Drugs as an Approach to Therapy. Front. Pharmacol. 2022, 13, 863667. [Google Scholar] [CrossRef]
- Clough, A.J.; Hilmer, S.N.; Naismith, S.L.; Kardell, L.D.; Gnjidic, D. N-of-1 trials for assessing the effects of deprescribing medications on short-term clinical outcomes in older adults: A systematic review. J. Clin. Epidemiol. 2018, 93, 112–119. [Google Scholar] [CrossRef]
- Huber, A.M.; Tomlinson, G.A.; Koren, G.; Feldman, B.M. Amitriptyline to relieve pain in juvenile idiopathic arthritis: A pilot study using Bayesian metaanalysis of multiple N-of-1 clinical trials. J. Rheumatol. 2007, 34, 1125–1132. [Google Scholar] [PubMed]
- Yelland, M.J.; Poulos, C.J.; Pillans, P.I.; Bashford, G.M.; Nikles, C.J.; Sturtevant, J.M.; Vine, N.; Del Mar, C.B.; Schluter, P.J.; Tan, M.; et al. N-of-1 randomized trials to assess the efficacy of gabapentin for chronic neuropathic pain. Pain Med. 2009, 10, 754–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yelland, M.J.; Nikles, C.J.; McNairn, N.; Del Mar, C.B.; Schluter, P.J.; Brown, R.M. Celecoxib compared with sustained-release paracetamol for osteoarthritis: A series of n-of-1 trials. Rheumatology 2007, 46, 135–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nixdorf, D.R.; Sobieh, R.; Gierthmühlen, J. Using an n-of-1 trial to assist in clinical decision making for patients with orofacial pain. J. Am. Dent. Assoc. 2012, 143, 259–261. [Google Scholar] [CrossRef]
- Germini, F.; Coerezza, A.; Andreinetti, L.; Nobili, A.; Rossi, P.D.; Mari, D.; Guyatt, G.; Marcucci, M. N-of-1 Randomized Trials of Ultra-Micronized Palmitoylethanolamide in Older Patients with Chronic Pain. Drugs Aging 2017, 34, 941–952. [Google Scholar] [CrossRef] [PubMed]
- Odineal, D.D.; Marois, M.T.; Ward, D.; Schmid, C.H.; Cabrera, R.; Sim, I.; Wang, Y.; Wilsey, B.; Duan, N.; Henry, S.G.; et al. Effect of Mobile Device-Assisted N-of-1 Trial Participation on Analgesic Prescribing for Chronic Pain: Randomized Controlled Trial. J. Gen. Intern. Med. 2020, 35, 102–111. [Google Scholar] [CrossRef]
- Lee, R.R.; Shoop-Worrall, S.; Rashid, A.; Thomson, W.; Cordingley, L. “Asking Too Much?”: Randomized N-of-1 Trial Exploring Patient Preferences and Measurement Reactivity to Frequent Use of Remote Multidimensional Pain Assessments in Children and Young People With Juvenile Idiopathic Arthritis. J. Med. Internet Res. 2020, 22, e14503. [Google Scholar] [CrossRef]
- Kravitz, R.L.; Schmid, C.H.; Marois, M.; Wilsey, B.; Ward, D.; Hays, R.D.; Duan, N.; Wang, Y.; MacDonald, S.; Jerant, A.; et al. Effect of Mobile Device-Supported Single-Patient Multi-crossover Trials on Treatment of Chronic Musculoskeletal Pain: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1368–1377. [Google Scholar] [CrossRef]
- Whitney, R.L.; Ward, D.H.; Marois, M.T.; Schmid, C.H.; Sim, I.; Kravitz, R.L. Patient Perceptions of Their Own Data in mHealth Technology-Enabled N-of-1 Trials for Chronic Pain: Qualitative Study. JMIR Mhealth Uhealth 2018, 6, e10291. [Google Scholar] [CrossRef]
- Notcutt, W.; Price, M.; Miller, R.; Newport, S.; Phillips, C.; Simmons, S.; Sansom, C. Initial experiences with medicinal extracts of cannabis for chronic pain: Results from 34 ‘N of 1’ studies. Anaesthesia 2004, 59, 440–452. [Google Scholar] [CrossRef]
- Fountzilas, E.; Tsimberidou, A.M. Overview of precision oncology trials: Challenges and opportunities. Expert Rev. Clin. Pharmacol. 2018, 11, 797–804. [Google Scholar] [CrossRef]
- Kyr, M.; Svobodnik, A.; Stepanova, R.; Hejnova, R. N-of-1 Trials in Pediatric Oncology: From a Population-Based Approach to Personalized Medicine-A Review. Cancers 2021, 13, 5428. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, R.; Duan, N.; Eslick, I.; Gabler, N.; Kaplan, H.; Larson, E. Design and implementation of N-of-1 trials: A user’s guide. In Agency for Healthcare Research and Quality; Effective Health Care Program, Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [Google Scholar]
- Kravitz, R.L.; Paterniti, D.A.; Hay, M.C.; Subramanian, S.; Dean, D.E.; Weisner, T.; Vohra, S.; Duan, N. Marketing therapeutic precision: Potential facilitators and barriers to adoption of n-of-1 trials. Contemp. Clin. Trials 2009, 30, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Alemayehu, C.; Mitchell, G.; Nikles, J.; Aseffa, A.; Clavarino, A. Acceptability and barriers to implementation of N-of-1 tests in Ethiopia—A qualitative study. BMC Med. Res. Methodol. 2019, 19, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, P.; Safford, M.M.; Hilmer, S.N.; Steinman, M.A.; Matlock, D.D.; Maurer, M.S.; Lachs, M.S.; Kronish, I.M. N-of-1 trials to facilitate evidence-based deprescribing: Rationale and case study. Br. J. Clin. Pharmacol. 2022, 88, 4460–4473. [Google Scholar] [CrossRef]
- Chalmers, I.; Smeeth, L.; Goldacre, B. Personalised Medicine Using N-of-1 Trials: Overcoming Barriers to Delivery. Healthcare 2019, 7, 134. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age (n = 25) | |
| Mean age (standard deviation) Median age Minimum, Maximum | = 54.36 (10.04) = 53 Min = 36, Max = 70 |
| Sex (n = 27) | |
| Female (n, %) | 17 (62.96) |
| Male (n, %) | 10 (37.04) |
| Years of clinical practice (n = 27) | |
| 0–10 years (n, %) | 2 (7.41) |
| 11–20 years (n, %) | 6 (22.21) |
| 21–30 years (n, %) | 11 (40.74) |
| 31–40 years (n, %) | 6 (22.22) |
| >40 years (n, %) | 2 (7.41) |
| Number of patients treated (n = 27) | |
| <10 (n, %) | 7 (25.93) |
| 11–20 (n, %) | 7 (25.93) |
| 21–50 (n, %) | 8 (29.63) |
| 51–100 (n, %) | 3 (11.11) |
| >100 (n, %) | 2 (7.41) |
| I Am Satisfied with the Available Treatment Options for My Patients with MPS. (n = 27) | |
| Strongly agree (n, %) | 0 (0) |
| Agree (n, %) | 3 (11.11) |
| Neutral (n, %) | 5 (18.52) |
| Disagree (n, %) | 12 (44.44) |
| Strongly disagree (n, %) | 7 (25.93) |
| My patients are satisfied with the available treatment options for MPS. (n = 27) | |
| Strongly agree (n, %) | 0 (0) |
| Agree (n, %) | 4 (14.81) |
| Neutral (n, %) | 8 (29.63) |
| Disagree (n, %) | 12 (44.44) |
| Strongly disagree (n, %) | 3 (11.11) |
| Have you Ever Heard of n-of-1 Trials? (n = 27) | |
| Yes (n, %) | 20 (74.07) |
| No (n, %) | 7 (25.93) |
| Have you ever used an n-of-1 trial in the treatment of your MPS patients? (n = 27) | |
| Yes (n, %) | 10 (37.04) |
| No (n, %) | 17 (62.96) |
| Have you conducted n-of 1 trials with patients suffering from other diseases? (n = 27) | |
| Yes (n, %) | 10 (37.04) |
| No (n, %) | 17 (62.96) |
| With which type of MPS do you ran the n-of-1 trial? (n = 8) | |
| MPS I Hurler (n, %) | 2 (25.00) |
| MPS II (n, %) | 3 (37.50) |
| MPS III B (n, %) | 1 (12.50) |
| MPS VI (n, %) | 1 (12.50) |
| MPS VII (n, %) | 1 (12.50) |
| How many n-of-1 trials have you ever ran with MPS patients? (n = 9) | |
| 1 (n, %) | 7 (77.8) |
| 2 (n, %) | 1 (11.11) |
| 3 (n, %) | 1 (11.11) |
| 4 (n, %) | 0 (0) |
| 5 (n, %) | 0 (0) |
| > 5 (n, %) | 0 (0) |
| Have you ran systematic evaluated n-of-1 trials with an advanced monitoring plan? (n = 12) | |
| Yes (n, %) | 4 (33.33) |
| No (n, %) | 8 (66.67) |
| Have you included further experts in your n-of-1 trial? (n = 13) | |
| Yes (n, %) | 5 (38.46) |
| No (n, %) | 8 (61.54) |
| Have you ever published your n-of-trials in a journal? (n = 13) | |
| Yes (n, %) | 2 (15.38) |
| No (n, %) | 11 (84.62) |
| What is the primary reason why you do not use n-of-1 trials in your practice? (n = 21) | |
| Impractical to implement (n, %) | 5 (23.81) |
| Not sufficiently trained in n-of-1 trial design (n, %) | 4 (19.05) |
| Too time consuming (n, %) | 4 (19.05) |
| Not relevant to most patients in my practice (n, %) | 5 (23.81) |
| My patients are unlikely to be interested in my practice (n, %) | 0 (0) |
| Some other reason (n, %) | 3 (14.29) |
| Assume There Is a Service That Made it Easy for You to Offer n-of-1 Trials to Select Patients in Your Practice with MPS. How Likely Are You to Use a Service Like This to Make Data Driven Treatment Choices at Least One in the Next Year? (n = 26) | |
| Highly likely (n, %) | 12 (46.15) |
| Likely (n, %) | 11 (42.30) |
| Neutral (n, %) | 1 (3.85) |
| Unlikely (n, %) | 1 (3.85) |
| Highly unlikely (n, %) | 1 (3.85) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiesinger, A.-M.; Strobl, H.; Lagler, F.B. Individual Treatment Trials—Do Experts Know and Use This Option to Improve the Treatability of Mucopolysaccharidosis? Pharmaceuticals 2023, 16, 416. https://doi.org/10.3390/ph16030416
Wiesinger A-M, Strobl H, Lagler FB. Individual Treatment Trials—Do Experts Know and Use This Option to Improve the Treatability of Mucopolysaccharidosis? Pharmaceuticals. 2023; 16(3):416. https://doi.org/10.3390/ph16030416
Chicago/Turabian StyleWiesinger, Anna-Maria, Hannah Strobl, and Florian B. Lagler. 2023. "Individual Treatment Trials—Do Experts Know and Use This Option to Improve the Treatability of Mucopolysaccharidosis?" Pharmaceuticals 16, no. 3: 416. https://doi.org/10.3390/ph16030416
APA StyleWiesinger, A. -M., Strobl, H., & Lagler, F. B. (2023). Individual Treatment Trials—Do Experts Know and Use This Option to Improve the Treatability of Mucopolysaccharidosis? Pharmaceuticals, 16(3), 416. https://doi.org/10.3390/ph16030416