
Prescribed Drugs and Self-Directed Violence: A Descriptive Study in the Spanish Pharmacovigilance Database
 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Background
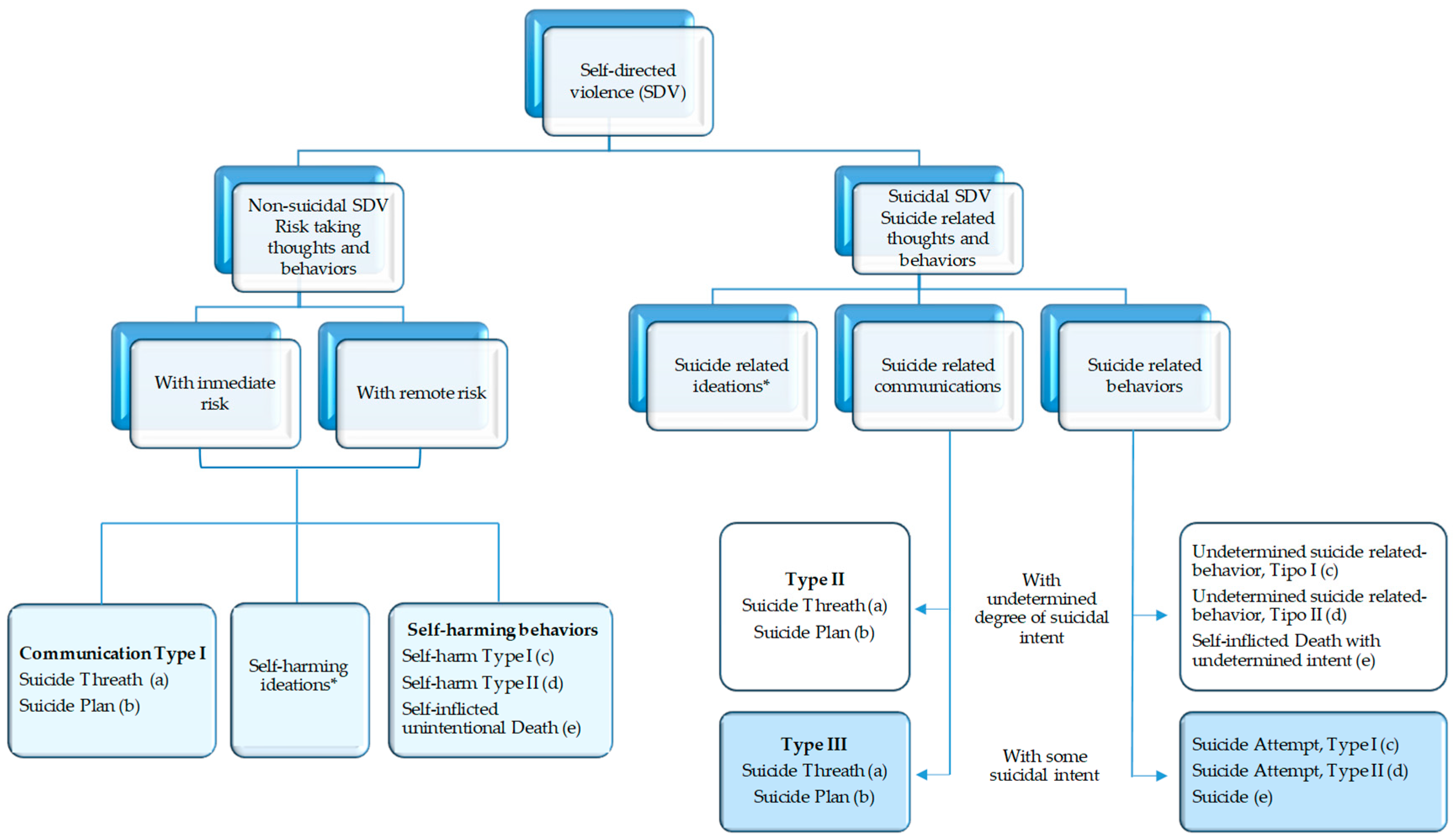
1.2. Self-Directed Violence: A Public Health Problem
1.3. Risks Factors
1.4. Aim
2. Results
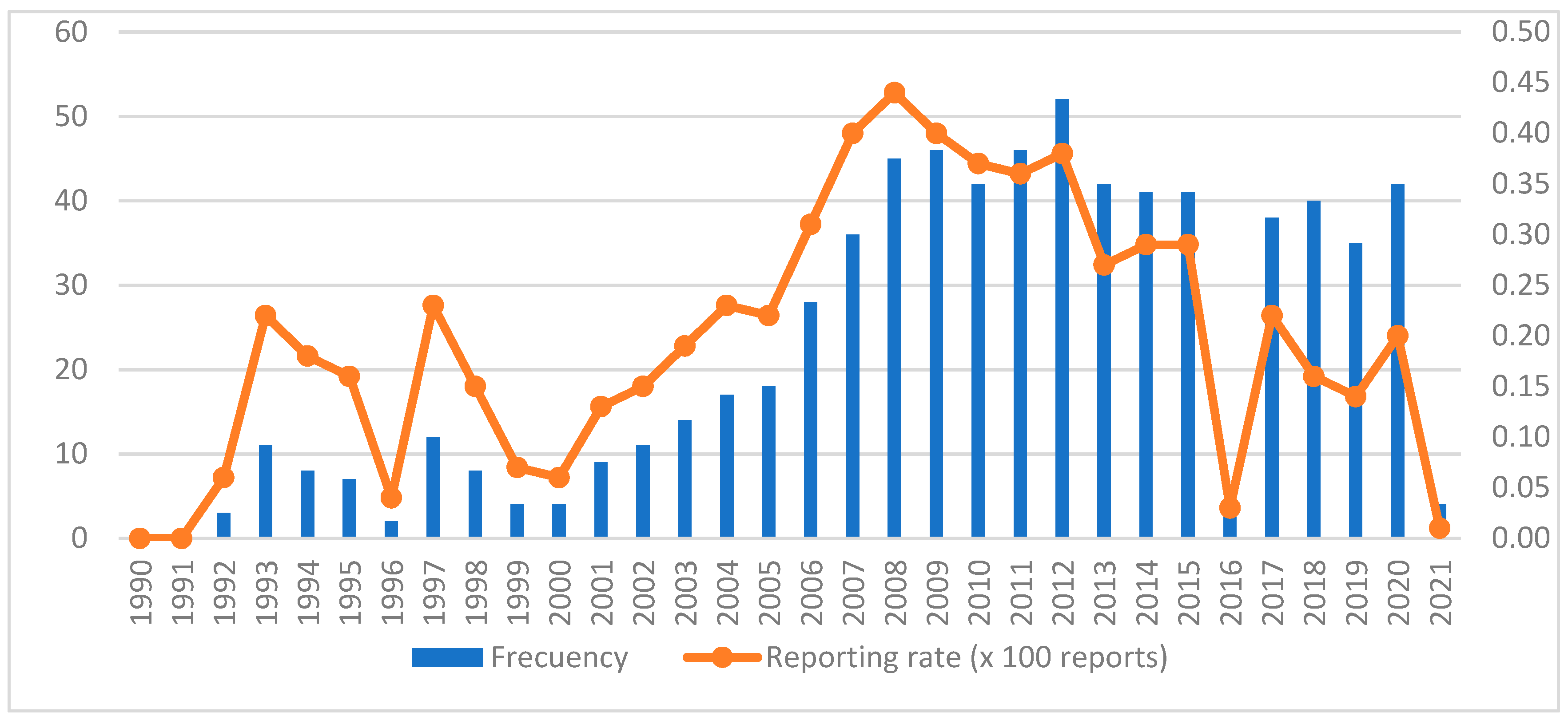
2.1. General Data on Reports
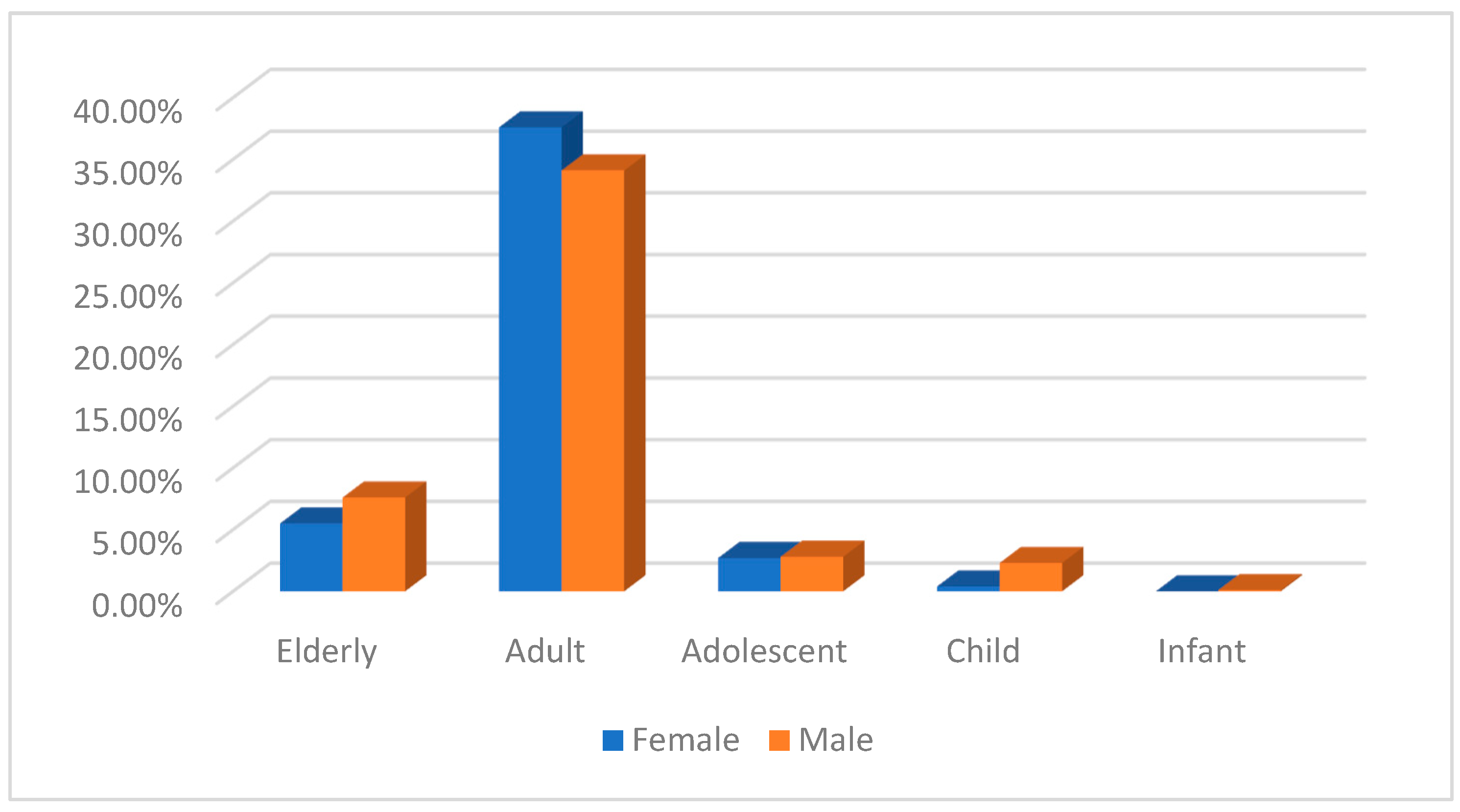
2.2. Patient Data (Study Population)
2.3. Self-Directed Adverse Drug Reactions
2.4. Drugs Involved
3. Discussion
4. Materials and Methods
4.1. Selection of Cases
4.2. Statistical Analysis
- -
- General data on reports: date and seriousness of the report.
- -
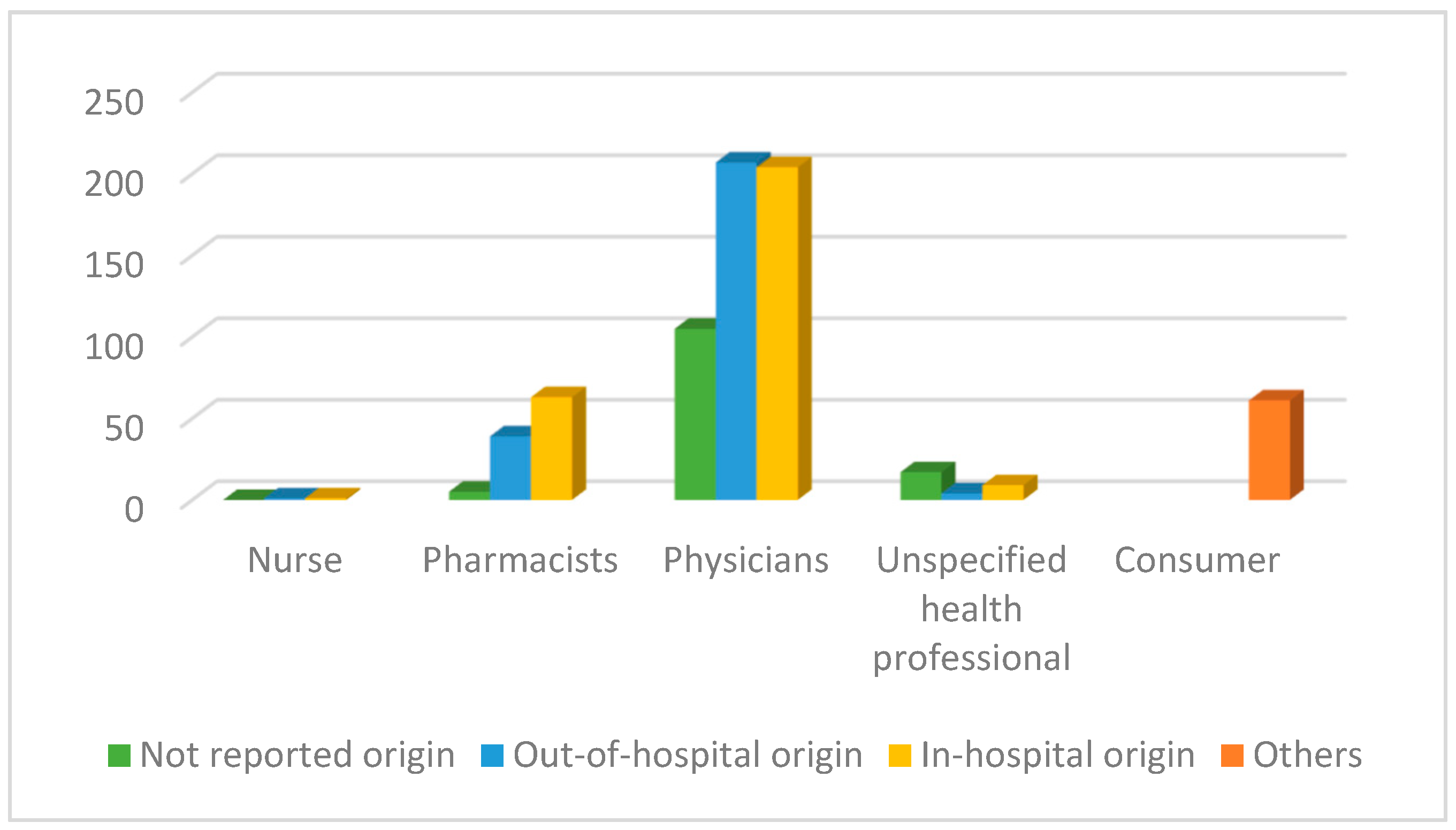
- Primary sources: physicians, pharmacists, nurses, other health professionals and consumers, as well as whether patients were in-hospital or out-of-hospital.
- -
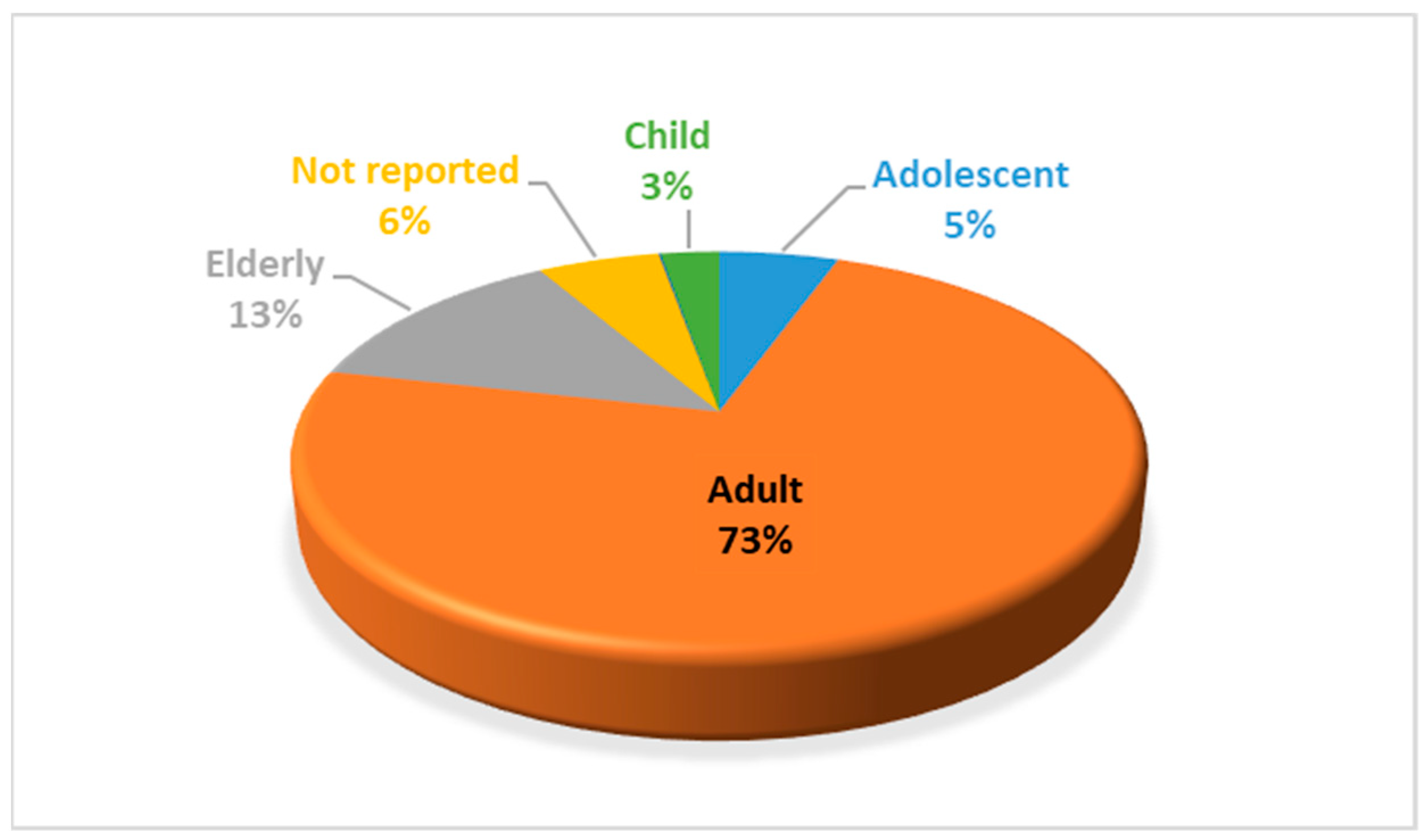
- Patient data: gender, age, age group. The age groups were infant (0–1.9 years old), child (2–11 years), adolescent (12–17 years), adult (8–65 years) and elderly (over 65 years).
- -
- ADRs: reactions of self-directed violence (several ADRs can be reported in one report), which were analyzed according to PT, High-Level Term (HLT), High-Level Group Term (HLGT) and System Organ Class (SOC), as well as severity and outcome of ADRs.
- -
- Drugs: drug name, suspected or concomitant drug. Suspected drugs were analyzed according to the Anatomical Chemical Therapeutic Classification System and a qualitative analysis was carried out, including time sequence, prior knowledge, re-exposure and alternative causes.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on Violence and Health. 2022. Available online: http://apps.who.int/iris/bitstream/10665/112670/1/9275315884_spa.pdf?ua=1 (accessed on 28 February 2023).
- World Health Organization. Global Consultation on Violence and Health. Violence: A Public Health Priority. 1996. Available online: https://apps.who.int/iris/bitstream/handle/10665/179463/WHA49_R25_eng.pdf?sequence=1&isAllowed=y (accessed on 28 February 2023).
- Centers for Disease Control and Prevention. Definitions: Self-Directed Violence. 2014. Available online: https://www.cdc.gov/violenceprevention/suicide/definitions.html (accessed on 28 February 2023).
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 1: Background, rationale, and methodology. Suicide Life Threat. Behav. 2007, 37, 248–263. [Google Scholar] [CrossRef]
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life Threat. Behav. 2007, 37, 264–277. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D.; Bertolote, J.M.L.D.D. Self-directed violence. In World Report on Violence and Health; Krug, E.G., Dahlberg, L.L., Mercy, J.A., Zwi, A.B., Lozano, R., Eds.; World Health Organization: Geneva, Switzerland, 2002; pp. 183–212. [Google Scholar]
- Posner, K.; Oquendo, M.A.; Gould, M.; Stanley, B.; Davies, M. (C-CASA): Classification of Suicidal Events in the FDA’ s Pediatric Suicidal Risk Analysis of Antidepressants. Psychiatry Interpers. Biol. Process. 2007, 164, 1035–1043. [Google Scholar] [CrossRef]
- World Health Organization. Preventing Suicide: A Global Imperative. 2014. Available online: https://www.who.int/publications/i/item/9789241564779 (accessed on 28 February 2023).
- Bachmann, S. Epidemiology of suicide and the psychiatric perspective. Int. J. Environ. Res. Public. Health 2018, 15, 1425. [Google Scholar] [CrossRef] [PubMed]
- Suicide Worldwide in 2019. Available online: https://www.who.int/publications/i/item/9789240026643 (accessed on 28 February 2023).
- Eurostat. Causes of Death Statistics—Statistics Explained. 2022. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Causes_of_death_statistics&oldid=563103 (accessed on 28 February 2023).
- Deaths by Cause (Chapters) by Sex (14,511). Available online: https://www.ine.es/jaxiT3/Datos.htm?t=14511 (accessed on 28 February 2023).
- Suicide Observatory in Spain 2020—Suicide Prevention. Available online: https://www.fsme.es/observatorio-del-suicidio-2020/ (accessed on 28 February 2023).
- UNESCO. School Violence and Bullying: Global Status Report. 2017. Available online: http://unesdoc.unesco.org/images/0024/002469/246970e.pdf (accessed on 28 February 2023).
- Prendes Espinosa, M.P. Bullying and Cyberbullying: Two Forms of Violence in Schools. J. New Approaches Educ. Res. 2018, 7, 1–2. [Google Scholar] [CrossRef]
- Rouve, N.; Bagheri, H.; Telmon, N.; Pathak, A.; Franchitto, N.; Schmitt, L.; Rougé, D.; Lapeyre-Mestre, M.; Montastruc, J.L.; French Association of Regional PharmacoVigilance Centres. Prescribed drugs and violence: A case/noncase study in the French PharmacoVigilance Database. Eur. J. Clin. Pharmacol. 2011, 67, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.J.; Glenmullen, J.; Furberg, C.D. Prescription Drugs Associated with Reports of Violence Towards Others. PLoS ONE 2010, 5, e15337. [Google Scholar] [CrossRef]
- Anderson, P.D.; Bokor, G. Forensic Aspects of Drug-Induced Violence. J. Pharm. Pract. 2012, 25, 41–49. [Google Scholar] [CrossRef]
- Breggin, P.R. Suicidality, violence and mania caused by selective serotonin reuptake inhibitors (SSRIs): A review and analysis. Int. J. Risk Saf. 2004, 16, 31–49. [Google Scholar]
- Fergusson, D.; Doucette, S.; Glass, K.C.; Shapiro, S.; Healy, D.; Hebert, P.; Hutton, B. Association between suicide attempts and selective serotonin reuptake inhibitors: Systematic review of randomised controlled trials. BMJ 2005, 330, 396–399. [Google Scholar] [CrossRef]
- Pfeifer, P.; Greusing, S.; Kupferschmidt, H.; Bartsch, C.; Reisch, T. A comprehensive analysis of attempted and fatal suicide cases involving frequently used psychotropic medications. Gen. Hosp. Psychiatry 2020, 63, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.K. Pharmacovigilance analysis of adverse psychiatric events and suicidality reported for roflumilast, an add-on COPD therapy. Br. J. Pharm. 2013, 3, 972–982. [Google Scholar] [CrossRef]
- Ye, X.; Blais, J.E.; Ng, V.W.S.; Castle, D.; Hayes, J.F.; Wei, Y.; Kang, W.; Gao, L.; Yan, V.K.C.; Wong, I.C.K.; et al. Association between statins and the risk of suicide attempt, depression, anxiety, and seizure: A population-based, self-controlled case series study. J. Affect. Disord. 2023, 320, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Tuccori, M.; Lapi, F.; Testi, A.; Coli, D.; Moretti, U.; Vannacci, A.; Motola, D.; Salvo, F.; Rivolta, A.L.; Blandizzi, C.; et al. Statin-associated psychiatric adverse events: A case/non-case evaluation of an Italian database of spontaneous adverse drug reaction reporting. Drug. Saf. 2008, 31, 1115–1123. [Google Scholar] [CrossRef]
- Samyde, J.; Petit, P.; Hillaire-Buys, D.; Faillie, J.L. Quinolone antibiotics and suicidal behavior: Analysis of the World Health Organization’s adverse drug reactions database and discussion of potential mechanisms. Psychopharmacology 2016, 233, 2503–2511. [Google Scholar] [CrossRef]
- Thomas, K.H.; Martin, R.M.; Potokar, J.; Pirmohamed, M.; Gunnell, D. Reporting of drug induced depression and fatal and non-fatal suicidal behaviour in the UK from 1998 to 2011. BMC Pharmacol. Toxicol. 2014, 15, 54. [Google Scholar] [CrossRef]
- Reith, D.M.; Edmonds, L. Assessing the role of drugs in suicidal ideation and suicidality. CNS Drugs 2007, 21, 463–472. [Google Scholar] [CrossRef]
- Sheard, M.H. Clinical pharmacology of aggressive behavior. Clin. Neuropharmacol. 1988, 11, 483–492. [Google Scholar] [CrossRef]
- Jones, K.A.; Nielsen, S.; Bruno, R.; Frei, M.; Lubman, D.I. Benzodiazepines their role in aggression and why GPs should prescribe with caution. Aust. Fam. Physician 2011, 40, 862–865. [Google Scholar]
- Saïas, T.; Gallarda, T. Paradoxical aggressive reactions to benzodiazepine use: A review. Encephale 2008, 34, 330–336. [Google Scholar] [CrossRef]
- Bielefeldt, A.O.; Danborg, P.B.; Gotzsche, P.C. Precursors to suicidality and violence on antidepressants: Systematic review of trials in adult healthy volunteers. J. R. Soc. Med. 2016, 109, 381–392. [Google Scholar] [CrossRef]
- Olesen, J.B.; Hansen, P.R.; Erdal, J.; Abildstrøm, S.Z.; Weeke, P.; Fosbøl, E.L.; Poulsen, H.E.; Gislason, G.H. Antiepileptic drugs and risk of suicide: A nationwide study. Pharmacoepidemiol. Drug Saf. 2010, 19, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Wallerstedt, S.M.; Brunlöf, G.; Sundström, A.; Eriksson, A.L. Montelukast and psychiatric disorders in children. Pharmacoepidemiol. Drug Saf. 2009, 18, 858–864. [Google Scholar] [CrossRef]
- Philip, G.; Hustad, C.; Noonan, G.; Malice, M.P.; Ezekowitz, A.; Reiss, T.F.; Knorr, B. Reports of suicidality in clinical trials of montelukast. J. Allergy Clin. Immunol. 2009, 124, 691–696. [Google Scholar] [CrossRef]
- Aldea Perona, A.; García-Sáiz, M.; Sanz Álvarez, E. Psychiatric Disorders and Montelukast in Children: A Disproportionality Analysis of the VigiBase(®). Drug Saf. 2016, 39, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Garnock-Jones, K.P. Roflumilast: A Review in COPD. Drugs 2015, 75, 1645–1656. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.; Furberg, C. Varenicline and suicide. Risk of psychiatric side effects with varenicline. BMJ 2009, 339, b4964. [Google Scholar] [CrossRef]
- Pollock, M.; Mosholder, A.; Governale, L. Suicidality: Varenicline; Bupropion, Nicotine Transdermal Patch; US Food and Drug Administration Center for Drug Evaluation and Research: Silver Spring, MD, USA, 2008.
- Kriikku, P.; Ojanperä, I. The relationship between bupropion and suicide in post-mortem investigations. Forensic Sci. Int. 2016, 266, 343–348. [Google Scholar] [CrossRef]
- Ascher, J.; Stemhagen, A.; Stender, M.; Win, B.; Winter, C. Patient Understanding of the Neuropsychiatric Risks Associated with Branded Bupropion Hydrochloride Products Used for Smoking Cessation. Drugs Real. World Outcomes 2018, 5, 181–191. [Google Scholar] [CrossRef]
- Ghaeli, P.; Mahmoudi-Gharaei, J.; Kouti, L.; Shakiba, A.; Hazara, R.; Alimadadi, A. Risk of Suicidal Events in Youths Taking Atomoxetine Compared with Those on Methylphenidate; An Observational Cross-Sectional Study. J. Pharm. Care 2021, 9, 166–170. [Google Scholar] [CrossRef]
- Prevost, N.; English, J.C. Isotretinoin: Update on Controversial Issues. J. Pediatr. Adolesc. Gynecol. 2013, 26, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Sundström, A.; Alfredsson, L.; Sjölin-Forsberg, G.; Gerdén, B.; Bergman, U.; Jokinen, J. Association of suicide attempts with acne and treatment with isotretinoin: Retrospective Swedish cohort study. BMJ 2010, 341, c5812. [Google Scholar] [CrossRef]
- Garcia, P.; Revet, A.; Yrondi, A.; Rousseau, V.; Degboe, Y.; Montastruc, F. Psychiatric Disorders and Hydroxychloroquine for Coronavirus Disease 2019 (COVID-19): A VigiBase Study. Drug Saf. 2020, 43, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gonzalez, C.; Lopez-Gonzalez, E.; Herdeiro, M.T.; Figueiras, A. Strategies to improve adverse drug reaction reporting: A critical and systematic review. Drug Saf. 2013, 36, 317–328. [Google Scholar] [CrossRef]
- EMA Guideline on the Use of Statistical Signal Detection Methods in the EudraVigilance Data Analysis System (EV-DAS). Doc ref EMEA/106464/2006rev.1. Available online: http://eudravigilance.emea.europa.eu/human/docs/10646406en.pdf (accessed on 28 February 2023).
- Bate, A.; Evans, S.J.W. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol. Drug Saf. 2009, 18, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Moore, N.; Thiessard, F.; Begaud, B. The history of disproportionality measures (reporting odds ratio, proportional reporting rates) in spontaneous reporting of adverse drug reactions. Pharmacoepidemiol. Drug Saf. 2005, 14, 285–286. [Google Scholar] [CrossRef]
- Almenoff, J.; Tonning, J.M.; Gould, A.L.; Szarfman, A.; Hauben, M.; Ouellet-Hellstrom, R.; Ball, R.; Hornbuckle, K.; Walsh, L.; Yee, C.; et al. Perspectives on the Use of Data Mining in Pharmacovigilance. Drug Saf. 2005, 28, 981–1007. [Google Scholar] [CrossRef]
- Almenoff, J.S.; Pattishall, E.N.; Gibbs, T.G.; DuMouchel, W.; Evans, S.J.; Yuen, N. Novel Statistical Tools for Monitoring the Safety of Marketed Drugs. Clin. Pharmacol. Ther. 2007, 82, 157–166. [Google Scholar] [CrossRef]
- Alvarez, Y.; Hidalgo, A.; Maignen, F.; Slattery, J. Validation of Statistical Signal Detection Procedures in EudraVigilance Post-Authorization Data. Drug Saf. 2010, 33, 475–487. [Google Scholar] [CrossRef]
- Hauben, M.; Horn, S.; Reich, L. Potential Use of Data-Mining Algorithms for the Detection of ‘Surprise’ Adverse Drug Reactions. Drug Saf. 2007, 30, 143–155. [Google Scholar] [CrossRef]
- Hauben, M.; Madigan, D.; Gerrits, C.M.; Walsh, L.; Van Puijenbroek, E.P. The role of data mining in pharmacovigilance. Expert. Opin. Drug Saf. 2005, 4, 929–948. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, A.; Maciá, M.A.; del Pozo, J.G.; de Abajo, F. Small risk ratios may have strong public health impact. BMJ 2003, 327, 1050–1051. [Google Scholar] [CrossRef] [PubMed]
- Bonifazi, G.; Corradini, E.; Ursino, D.; Virgili, L. New Approaches to Extract Information from Posts on COVID-19 Published on Reddit. Int. J. Inf. Technol. Decis. Mak. 2022, 21, 1385–1431. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preferred Terms of the MedDRA Classification | N | Percentage |
|---|---|---|
| Suicide attempt | 319 | 41.2 |
| Suicidal ideation | 224 | 28.9 |
| Intentional overdose | 106 | 13.7 |
| Completed suicide | 54 | 7 |
| Self-harm ideation | 29 | 3.7 |
| Intentional self-harm | 18 | 2.3 |
| Intentional poisoning | 10 | 1.3 |
| Self-injurious behavior | 7 | 0.9 |
| Suicidal behavior | 4 | 0.5 |
| Suicidal depression | 4 | 0.5 |
| Total | 775 | 100 |
| Outcome | N | Percentage |
|---|---|---|
| Not reported | 141 | 18.2 |
| Recovering | 60 | 7.7 |
| Fatal | 108 | 13.9 |
| Not recovered | 60 | 7.7 |
| Recovered | 395 | 51 |
| Recovered with sequelae | 11 | 1.5 |
| Total | 775 | 100 |
| ATC First Level/Therapeutic Group | N | Percentage | |
|---|---|---|---|
| A | Alimentary tract and metabolism | 44 | 4.2 |
| B | Blood and blood forming organs | 5 | 0.5 |
| C | Cardiovascular system | 21 | 1.9 |
| D | Dermatologicals | 10 | 1 |
| G | Genito urinary system and sex hormones | 2 | 0.2 |
| H | Systemic hormonal preparations, excluding sex hormones and insulins | 5 | 0.5 |
| J | Antiinfective for systemic use | 139 | 13.2 |
| L | Antineoplastic and immunomodulating agents | 54 | 5.3 |
| M | Musculo-skeletal system | 26 | 2.5 |
| N | Nervous system | 677 | 64.5 |
| P | Antiparasitic products, insecticides and repellents | 12 | 1.1 |
| R | Respiratory system | 57 | 5.5 |
| S | Sensory organs | 1 | 0.1 |
| Total | 1053 | 100 | |
| Nervous System | N | Percentage | |
|---|---|---|---|
| N01 | Anaesthetics | 4 | 0.4 |
| N02 | Analgesics | 32 | 3.1 |
| N03 | Antiepileptics | 113 | 10.7 |
| N04 | Antiparkinsonians | 17 | 1.6 |
| N05 | Psycholeptics | 231 | 21.9 |
| N06 | Psychoanaleptics | 204 | 19.5 |
| N07 | Other nervous system drugs | 76 | 7.3 |
| Total | 677 | 64.5 | |
| Antiinfective for Systemic Use | N | Percentage | |
|---|---|---|---|
| J01 | Antibacterials for systemic use | 16 | 1.5 |
| J02 | Antimycotics for systemic use | 1 | 0.1 |
| J04 | Antimycobacterials | 2 | 0.2 |
| J05 | Antivirals for systemic use | 116 | 11 |
| J07 | Vaccines | 4 | 0.4 |
| Total | 139 | 13.2 | |
| DRUG | N | % |
|---|---|---|
| Vareniclin | 44 | 4.2 |
| Fluoxetine | 33 | 3.1 |
| Lorazepam | 32 | 3 |
| Escitalopram | 28 | 2.7 |
| Venlafaxin | 23 | 2.2 |
| Veralipride | 22 | 2.1 |
| Pregabalin | 21 | 2 |
| Roflumilast | 21 | 2 |
| Bupropion | 19 | 1.8 |
| Aripiprazol | 18 | 1.7 |
| Paracetamol | 16 | 1.5 |
| Chlorazepate | 16 | 1.5 |
| Olanzapine | 16 | 1.5 |
| Lamivudine | 15 | 1.4 |
| Ribavirin | 15 | 1.4 |
| Alprazolam | 15 | 1.4 |
| Diazepam | 15 | 1.4 |
| Quetiapine | 15 | 1.4 |
| Abacavir | 14 | 1.3 |
| Risperidone | 14 | 1.3 |
| Dolutegravir | 13 | 1.2 |
| Topiramate | 13 | 1.2 |
| Amitriptilin | 13 | 1.2 |
| Levetiracetam | 12 | 1.1 |
| Atomoxetine | 12 | 1.1 |
| Efavirenz | 11 | 1 |
| Clonazepam | 11 | 1 |
| Duloxetine | 11 | 1 |
| Mirtazapine | 11 | 1 |
| Emtricytabin | 10 | 0.9 |
| Tenofovir | 10 | 0.9 |
| Sertraline | 10 | 0.9 |
| Montelukast | 10 | 0.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avedillo-Salas, A.; Pueyo-Val, J.; Fanlo-Villacampa, A.; Navarro-Pemán, C.; Lanuza-Giménez, F.J.; Ioakeim-Skoufa, I.; Vicente-Romero, J. Prescribed Drugs and Self-Directed Violence: A Descriptive Study in the Spanish Pharmacovigilance Database. Pharmaceuticals 2023, 16, 772. https://doi.org/10.3390/ph16050772
Avedillo-Salas A, Pueyo-Val J, Fanlo-Villacampa A, Navarro-Pemán C, Lanuza-Giménez FJ, Ioakeim-Skoufa I, Vicente-Romero J. Prescribed Drugs and Self-Directed Violence: A Descriptive Study in the Spanish Pharmacovigilance Database. Pharmaceuticals. 2023; 16(5):772. https://doi.org/10.3390/ph16050772
Chicago/Turabian StyleAvedillo-Salas, Ana, Javier Pueyo-Val, Ana Fanlo-Villacampa, Cristina Navarro-Pemán, Francisco Javier Lanuza-Giménez, Ignatios Ioakeim-Skoufa, and Jorge Vicente-Romero. 2023. "Prescribed Drugs and Self-Directed Violence: A Descriptive Study in the Spanish Pharmacovigilance Database" Pharmaceuticals 16, no. 5: 772. https://doi.org/10.3390/ph16050772
APA StyleAvedillo-Salas, A., Pueyo-Val, J., Fanlo-Villacampa, A., Navarro-Pemán, C., Lanuza-Giménez, F. J., Ioakeim-Skoufa, I., & Vicente-Romero, J. (2023). Prescribed Drugs and Self-Directed Violence: A Descriptive Study in the Spanish Pharmacovigilance Database. Pharmaceuticals, 16(5), 772. https://doi.org/10.3390/ph16050772