
Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Technical Aspects of Ultrasound Imaging in Skeletal Muscle Examination
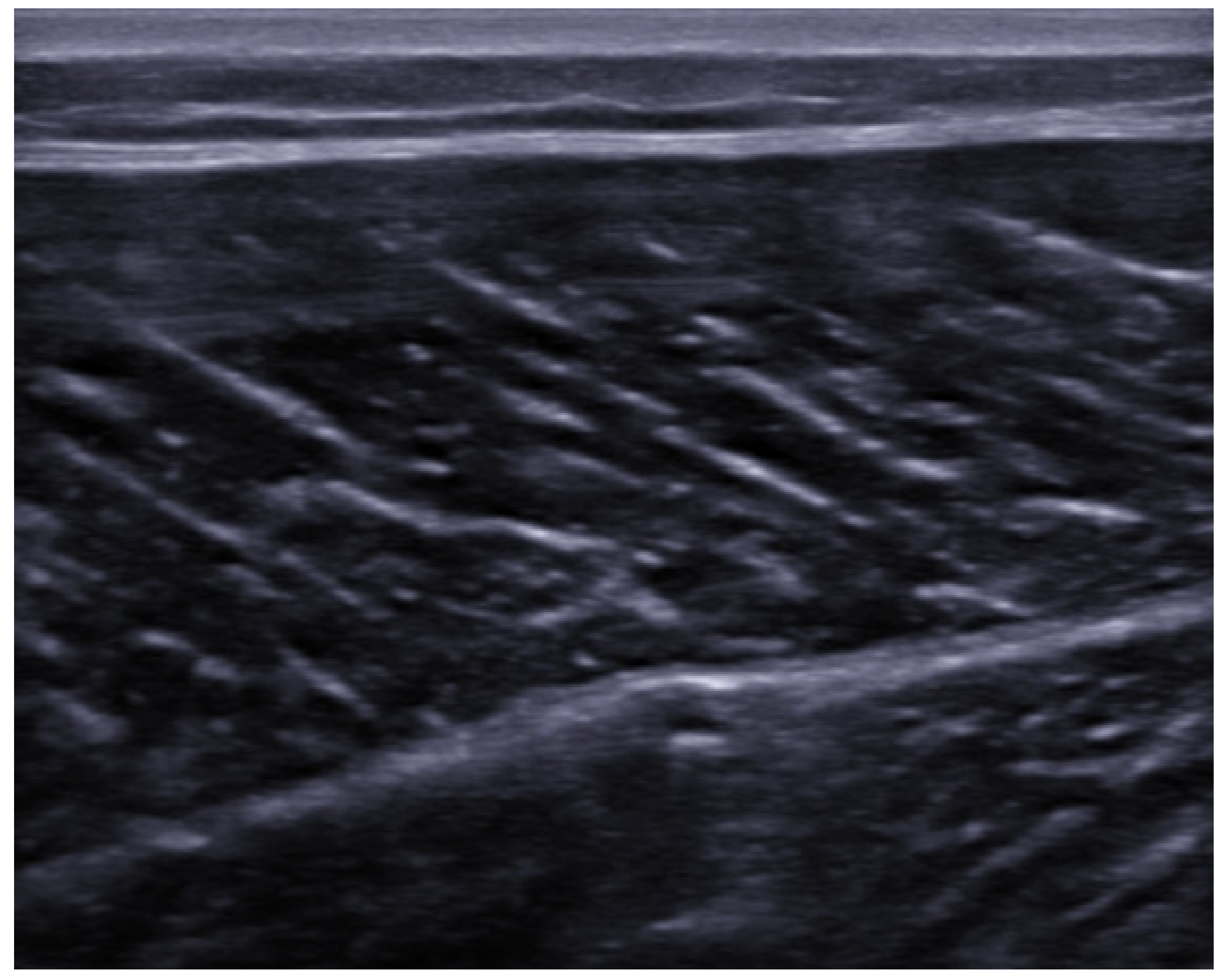
3. Ultrasound Anatomy of Skeletal Muscle
4. Muscle Injuries: Types and Mechanisms
- -
- mild form (loss of range of movement (ROM) less than one-third with short recovery time);
- -
- moderate form (loss of ROM between one- and two-thirds with moderate recovery time);
- -
- severe form (with loss of ROM larger than two-thirds with long recovery time).
- -
- grade 1: no significant loss of function and strength, and minimal tissue tearing (less than 5%);
- -
- grade 2: myotendinous junction injury with evident reduction in strength and function;
- -
- grade 3: complete injury to the myotendinous unit and total loss of strength and function [9].
5. Ultrasound Findings of the Muscle Lesions
6. Classification and Grading of Muscle Injury
- -
- Grade I: muscle injury with low disability, localized pain, small hemorrhage and swelling with mild ROM limitation (<10°);
- -
- Grade II: moderate disability, pain and swelling, loss of function between 5% and 50% and moderate ROM limitation (10–25°);
- -
- Grade III: muscle rupture with severe disability and pain, loss of function more than 50% and severe ROM limitation (up to 25°) [29].
- -
- Type 1A—Fatigue-induced muscle disorder, mostly caused by change in playing surface, is characterized by focal increased “muscle tightness” and dull pain;
- -
- Type 1B—Delayed Onset Muscle Soreness (DOMS), that is a more generalized dull pain caused by decelerations during eccentric contractions. It peaks within 24–72 h after activity.
- -
- Type 2A—Spine-related neuromuscular muscle disorder, that is a focal increase of muscle tone caused by structural or functional spinal disorder;
- -
- Type 2B—Muscle-related neuromuscular muscle disorder, characterized by increased muscle firmness and cramp-like sensation, due to neuromuscular disorder.
- -
- Type 3A—Minor partial muscle tear involves less than a muscle fascicle and is characterized by localized pain and absence of visible hematoma;
- -
- Type 3B—Moderate partial muscle tear involves more than a muscle fascicle but not all muscle belly, with palpable defect painful to touch, and visible hematoma;
- -
7. Healing Process and Prognosis of Muscle Injury
- -
- Destructive phase: it occurs immediately after the trauma and is characterized by the necrosis of the muscle fibers, the development of an inflammatory process and the formation of a local hematoma;
- -
- Reparative phase: usually starts from the second day, it is characterized by the removal of cellular debris and necrotic tissue by macrophage cells; the local production of growth factors will promote the formation of a fibrous scar and the revascularization of the area. During this phase, the satellite cells may differentiate into myoblasts and can partly drive the regeneration of muscle tissue;
- -
- Remodeling phase: with the reorganization of the fibrous scar and the maturation of regenerated myofibrils, a progressive recovery of the functional capacity of the muscle can be observed [15].
8. Complications of Muscle Injuries and Atypical Lesions
8.1. Myositis Ossificans
8.2. Muscle Hernia
8.3. Compartment Syndrome
8.4. Muscle Atrophy
9. Rehabilitation and Interventional Therapy
10. Strengths and Limitations of US Imaging in Sport-Related Muscle Injury
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Woodhouse, J.B.; McNally, E.G. Ultrasound of skeletal muscle injury: An update. Semin. Ultrasound CT MR. 2011, 32, 91–100. [Google Scholar] [CrossRef]
- Kirkendall, D.T.; Garrett, W.E., Jr. Clinical perspectives regarding eccentric muscle injury. Clin. Orthop. Relat. Res. 2002, 403, S81–S89. [Google Scholar] [CrossRef]
- Bisciotti, G.N.; Volpi, P.; Alberti, G.; Aprato, A.; Artina, M.; Auci, A.; Bait, C.; Belli, A.; Bellistri, G.; Bettinsoli, P.; et al. Italian consensus statement (2020) on return to play after lower limb muscle injury in football (soccer). BMJ Open Sport Exerc. Med. 2019, 15, e000505. [Google Scholar] [CrossRef]
- Lee, J.C.; Mitchell, A.W.; Healy, J.C. Imaging of muscle injury in the elite athlete. Br. J. Radiol. 2012, 85, 1173–1185. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J.; Healy, J.C.; Waldén, M.; Lee, J.C.; English, B.; Hägglund, M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br. J. Sports Med. 2012, 46, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Valle, X.; Alentorn-Geli, E.; Tol, J.L.; Hamilton, B.; Garrett, W.E., Jr.; Pruna, R.; Til, L.; Gutierrez, J.A.; Alomar, X.; Balius, R.; et al. Muscle injuries in sports: A new evidence-informed and expert consensus-based classification with clinical application. Sports Med. 2017, 47, 1241–1253. [Google Scholar] [CrossRef] [Green Version]
- Capannelli, D.; Miceli, M.; Piolanti, M.; Monetti, F.; Galletti, S.; Barozzi, L. The role of ultrasound in sports muscular injuries. Eur. Soc. Radiol. 2014. [Google Scholar] [CrossRef]
- Guermazi, A.; Roemer, F.W.; Robinson, P.; Tol, J.L.; Regatte, R.R.; Crema, M.D. Imaging of Muscle Injuries in Sports Medicine: Sports Imaging Series. Radiology 2017, 282, 646–663. [Google Scholar] [CrossRef]
- Van Holsbeeck, M.; Introcaso, J. Sonography of muscle. In Musculoskeletal Ultrasound, 2nd ed.; Van Holsbeeck, M., Introcaso, J., Eds.; Mosby: St Louis, MO, USA, 2001; pp. 23–75. [Google Scholar]
- Tok, F. Ultrasound imaging in Sports Medicine. In Musculoskeletal Ultrasound in Physical and Rehabilitation Medicine, 1st ed.; Özçakar, L., De Muynck, M., Eds.; Edi-ermes: Milano, Italy, 2014; pp. 125–140. [Google Scholar]
- O’Brien, W.D., Jr. Ultrasound-biophysics mechanisms. Prog. Biophys. Mol. Biol. 2007, 93, 212–255. [Google Scholar] [CrossRef] [Green Version]
- Entrekin, R.R.; Porter, B.A.; Sillesen, H.H.; Wong, A.D.; Cooperberg, P.L.; Fix, C.H. Real-time spatial compound imaging: Application to breast, vascular, and musculoskeletal ultrasound. Semin. Ultrasound CT MR 2001, 22, 50–64. [Google Scholar] [CrossRef]
- Huard, J.; Li, Y.; Fu, F.H. Muscle injuries and repair: Current trends in research. J. Bone Jt. Surg. Am. 2002, 84, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, T.A.; Järvinen, T.L.; Kääriäinen, M.; Aärimaa, V.; Vaittinen, S.; Kalimo, H.; Järvinen, M. Muscle injuries: Optimising recovery. Best Pract. Res. Clin. Rheumatol. 2007, 21, 317–331. [Google Scholar] [CrossRef]
- Järvinen, T.A.; Järvinen, T.L.; Kääriäinen, M.; Kalimo, H.; Järvinen, M. Muscle injuries: Biology and treatment. Am. J. Sports Med. 2005, 33, 745–764. [Google Scholar] [CrossRef]
- Slavotinek, J.P.; Verrall, G.M.; Fon, G.T. Hamstring injury in athletes: Using MR imaging measurements to compare extent of muscle injury with amount of time lost from competition. AJR Am. J. Roentgenol. 2002, 179, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- Beiner, J.M.; Jokl, P. Muscle contusion injury and myositis ossificans traumatica. Clin. Orthop. Relat. Res. 2002, 403, S110–S119. [Google Scholar] [CrossRef]
- Kary, J.M. Diagnosis and management of quadriceps strains and contusions. Curr. Rev. Musculoskelet Med. 2010, 30, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Croisier, J.L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef]
- Garrett, W.E., Jr. Muscle strain injuries. Am. J. Sports Med. 1996, 24, S2–S8. [Google Scholar] [CrossRef]
- El-Khoury, G.Y.; Daniel, W.W.; Kathol, M.H. Acute and chronic avulsive injuries. Radiol. Clin. North Am. 1997, 35, 747–766. [Google Scholar]
- Evans, G.F.; Haller, R.G.; Wyrick, P.S.; Parkey, R.W.; Fleckenstein, J.L. Submaximal delayed-onset muscle soreness: Correlations between MR imaging findings and clinical measures. Radiology 1998, 208, 815–820. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T.; Özçakar, L. Ultrasound imaging and rehabilitation of muscle disorders: Part 1. Traumatic injuries. Am. J. Phys. Med. Rehabil. 2019, 98, 1133–1141. [Google Scholar] [CrossRef]
- O’ Connor, P.J. Ecografia delle lesioni muscolari. In Ecografia Muscoloscheletrica, 2nd ed.; McNally, E.G., Ed.; Edra s.p.a.: Milano, Italy, 2015; pp. 431–442. [Google Scholar]
- Bianchi, S.; Abdelwahab, I.F.; Mazzola, C.G.; Ricci, G.; Damiani, S. Sonographic examination of muscle herniation. J. Ultrasound Med. 1995, 14, 357–360. [Google Scholar] [CrossRef]
- Teng, V.S.Y.; Sia, S.Y.; Zhang, J.; Gartner, L.E.; Unnikrishnan, K.; Puhaindran, M.E.; Hallinan, J.T.P.D. Morel-lavallee lesion of the right thigh mimicking sarcoma. Am. J. Phys. Med. Rehabil. 2019, 98, e52–e53. [Google Scholar] [CrossRef]
- Peetrons, P. Ultrasound of muscles. Eur. Radiol. 2002, 12, 35–43. [Google Scholar] [CrossRef]
- Grassi, A.; Quaglia, A.; Canata, G.L.; Zaffagnini, S. An update on the grading of muscle injuries: A narrative review from clinical to comprehensive systems. Joints 2016, 4, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Rachun, A. Standard Nomenclature of Athletic Injuries; American Medical Association: Chicago, IL, USA, 1966. [Google Scholar]
- Wise, D.D. Physiotherapeutic treatment of athletic injuries to the muscle-tendon complex of the leg. Can. Med. Assoc. J. 1977, 117, 635–639. [Google Scholar]
- Hamilton, B.; Valle, X.; Rodas, G.; Til, L.; Grive, R.P.; Rincon, J.A.; Tol, J.L. Classification and grading of muscle injuries: A narrative review. Br. J. Sports Med. 2015, 49, 306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.C.; Healy, J. Sonography of lower limb muscle injury. AJR Am. J. Roentgenol. 2004, 182, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Schneider-Kolsky, M.E.; Hoving, J.L.; Warren, P.; Connell, D.A. A comparison between clinical assessment and magnetic resonance imaging of acute hamstring injuries. Am. J. Sports Med. 2006, 34, 1008–1015. [Google Scholar] [CrossRef]
- Takebayashi, S.; Takasawa, H.; Banzai, Y.; Miki, H.; Sasaki, R.; Itoh, Y.; Matsubara, S. Sonographic findings in muscle strain injury: Clinical and MR imaging correlation. J. Ultrasound Med. 1995, 14, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Chan, O.; Del Buono, A.; Best, T.M.; Maffulli, N. Acute muscle strain injuries: A proposed new classification system. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2356–2362. [Google Scholar] [CrossRef]
- Mueller-Wohlfahrt, H.W.; Haensel, L.; Mithoefer, K.; Ekstrand, J.; English, B.; McNally, S.; Orchard, J.; van Dijk, C.N.; Kerkhoffs, G.M.; Schamasch, P.; et al. Terminology and classification of muscle injuries in sport: The Munich consensus statement. Br. J. Sports Med. 2013, 47, 342–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Askling, C.; Magnusson, H.; Mithoefer, K. Return to play after thigh muscle injury in elite football players: Implementation and validation of the Munich muscle injury classification. Br. J. Sports Med. 2013, 47, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Oliva, F.; Frizziero, A.; Nanni, G.; Barazzuol, M.; Via, A.G.; Ramponi, C.; Brancaccio, P.; Lisitano, G.; Rizzo, D.; et al. ISMuLT Guidelines for muscle injuries. Muscles Ligaments Tendons J. 2014, 24, 241–249. [Google Scholar]
- Koulouris, G.; Connell, D. Hamstring muscle complex: An imaging review. RadioGraphics 2005, 25, 571–586. [Google Scholar] [CrossRef]
- Park, G.Y.; Kwon, D.R. Application of real-time sonoelastography in musculoskeletal diseases related to physical medicine and rehabilitation. Am. J. Phys. Med. Rehabil. 2011, 90, 875–886. [Google Scholar] [CrossRef]
- Winn, N.; Lalam, R.; Cassar-Pullicino, V. Sonoelastography in the musculoskeletal system: Current role and future directions. World J. Radiol. 2016, 8, 868–879. [Google Scholar] [CrossRef]
- Drakonaki, E.E.; Allen, G.M.; Wilson, D.J. Ultrasound elastography for musculoskeletal applications. Br. J. Radiol. 2012, 85, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Botar Jid, C.; Vasilescu, D.; Damian, L.; Dumitriu, D.; Ciurea, A.; Dudea, S.M. Musculoskeletal sonoelastography. Pictorial essay. Med. Ultrason. 2012, 14, 239–245. [Google Scholar] [PubMed]
- Koçyiğit, F.; Kuyucu, E.; Koçyiğit, A. Real-time sonoelastography findings in a patient with tennis leg: A promising technique in the assessment of muscle rupture. Eur. J. Phys. Rehabil. Med. 2016, 52, 754–755. [Google Scholar]
- Drakonaki, E.E.; Sudoł-Szopińska, I.; Sinopidis, C.; Givissis, P. High resolution ultrasound for imaging complications of muscle injury: Is there an additional role for elastography? J. Ultrason. 2019, 19, 137–144. [Google Scholar] [CrossRef]
- Connell, D.A.; Schneider-Kolsky, M.E.; Hoving, J.L.; Malara, F.; Buchbinder, R.; Koulouris, G.; Burke, F.; Bass, C. Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries. AJR Am. J. Roentgenol. 2004, 183, 975–984. [Google Scholar] [CrossRef]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Skjødt, T.; Bolvig, L.; Bang, N.; Hölmich, P. The diagnostic and prognostic value of ultrasonography in soccer players with acute hamstring injuries. Am. J. Sports Med. 2014, 42, 399–404. [Google Scholar] [CrossRef]
- Renoux, J.; Brasseur, J.L.; Wagner, M.; Frey, A.; Folinais, D.; Dibie, C.; Maiza, D.; Crema, M.D. Ultrasound-detected connective tissue involvement in acute muscle injuries in elite athletes and return to play: The French National Institute of Sports (INSEP) study. J. Sci Med. Sport. 2019, 22, 641–646. [Google Scholar] [CrossRef]
- King, J.B. Post-traumatic ectopic calcification in the muscles of athletes: A review. Br. J. Sports Med. 1998, 32, 287–290. [Google Scholar] [CrossRef] [Green Version]
- Devilbiss, Z.; Hess, M.; Ho, G.W.K. Myositis Ossificans in Sport: A Review. Curr. Sports Med. Rep. 2018, 17, 290–295. [Google Scholar] [CrossRef]
- Tyler, P.; Saifuddin, A. The imaging of myositis ossificans. Semin. Musculoskelet Radiol. 2010, 14, 201–216. [Google Scholar] [CrossRef]
- Zeiss, J.; Ebraheim, N.A.; Woldenberg, L.S. Magnetic resonance imaging in the diagnosis of anterior tibialis muscle herniation. Clin. Orthop Relat Res. 1989, 244, 249–253. [Google Scholar] [CrossRef]
- Blankenbaker, D.G.; Tuite, M.J. Temporal changes of muscle injury. Semin. Musculoskelet Radiol. 2010, 14, 176–193. [Google Scholar] [CrossRef]
- Stiegler, H.; Brandl, R.; Krettek, C. Das chronische rezidivierende Kompartmentsyndrom [Chronic relapsing compartment syndrome]. Unfallchirurg 2009, 112, 373–380. [Google Scholar] [CrossRef]
- McDonald, S.; Bearcroft, P. Compartment syndromes. Semin. Musculoskelet Radiol. 2010, 14, 236–244. [Google Scholar] [CrossRef]
- Broski, S.M.; Tiegs Heiden, C.A.; Ringler, M.D. Muscle: Ischemia, infarction, and compartment syndrome. Semin. Musculoskelet Radiol. 2017, 21, 443–458. [Google Scholar] [CrossRef]
- Steeds, R.P.; Alexander, P.J.; Muthusamy, R.; Bradley, M. Sonography in the diagnosis of rhabdomyolysis. J. Clin. Ultrasound. 1999, 27, 531–533. [Google Scholar] [CrossRef]
- Bayer, M.L.; Magnusson, S.P.; Kjaer, M. Tendon research group bispebjerg. Early versus delayed rehabilitation after acute muscle injury. N. Engl. J. Med. 2017, 377, 1300–1301. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.; Hamilton, B. Medical interventions in the management of hamstring muscle injury. Eur. J. Sport Sci. 2014, 14, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, D.; Corazza, A.; Arcidiacono, A.; Messina, C.; Serafini, G.; Sconfienza, L.M.; Silvestri, E. Ultrasound-guided procedures to treat sport-related muscle injuries. Br. J. Radiol. 2016, 89, 20150484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alessandrino, F.; Balconi, G. Complications of muscle injuries. J. Ultrasound. 2013, 16, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Morvan, G.; Vuillemin, V.; Guerini, H. Interventional musculoskeletal ultrasonography of the lower limb. Diagn. Interv. Imaging. 2012, 93, 652–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamada, M.; Shimizu, Y.; Aramaki-Hattori, N.; Kato, T.; Takada, K.; Aoki, M.; Kishi, K.; Nagasao, T. Management of chronic expanding haematoma using triamcinolone after latissimus dorsi flap harvesting. Arch. Plast. Surg. 2015, 42, 218–222. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, M.; Anitua, E.; Delgado, D.; Sánchez, P.; Orive, G.; Padilla, S. Muscle repair: Platelet-rich plasma derivates as a bridge from spontaneity to intervention. Injury 2014, 45, S7–S14. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Creaney, L.; Hamilton, B. Growth factor delivery methods in the management of sports injuries: The state of play. Br. J. Sports Med. 2008, 42, 314–320. [Google Scholar] [CrossRef] [Green Version]
- Beitzel, K.; McCarthy, M.B.; Russell, R.P.; Apostolakos, J.; Cote, M.P.; Mazzocca, A.D. Learning about PRP using cell-based models. Muscles Ligaments Tendons J. 2014, 4, 38–45. [Google Scholar] [CrossRef]
- Borrione, P.; Ruiz, M.T.P.; Giannini, S.; Gianfrancesco, A.D.; Pigozzi, F. Effect of plateletreleased growth factors on muscle strains: A case control report. Med. Sport 2011, 64, 317–322. [Google Scholar]
- Hamilton, B.; Knez, W.; Eirale, C.; Chalabi, H. Platelet enriched plasma for acute muscle injury. Acta Orthop. Belg. 2010, 76, 443–448. [Google Scholar]
- Hamid, M.S.A.; Mohamed Ali, M.R.; Yusof, A.; George, J.; Lee, L.P. Platelet-rich plasma injections for the treatment of hamstring injuries: A randomized controlled trial. Am. J. Sports Med. 2014, 42, 2410–2418. [Google Scholar] [CrossRef] [PubMed]
- Hamid, M.S.A.; Hussein, K.H.; Helmi Salim, A.M.; Puji, A.; Mat Yatim, R.; Yong, C.C.; Sheng, T.W.Y. Study protocol for a double-blind, randomised placebo-controlled trial evaluating clinical effects of platelet-rich plasma injection for acute grade-2 hamstring tear among high performance athletes. BMJ Open 2020, 10, e039105. [Google Scholar] [CrossRef]
- Reurink, G.; Goudswaard, G.J.; Moen, M.H.; Weir, A.; Verhaar, J.A.; Bierma-Zeinstra, S.M.; Maas, M.; Tol, J.L. Dutch Hamstring Injection Therapy (HIT) Study Investigators. Platelet-rich plasma injections in acute muscle injury. N. Engl. J. Med. 2014, 370, 2546–2547. [Google Scholar] [CrossRef]
- Setayesh, K.; Villarreal, A.; Gottschalk, A.; Tokish, J.M.; Choate, W.S. Treatment of muscle injuries with platelet-rich plasma: A Review of the literature. Curr. Rev. Musculoskelet Med. 2018, 11, 635–642. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rachun 1966 [30] | Wise 1977 [31] | Lee et al. 2004 [33] | Schneider-Kolsky et al. 2006 [34] | Grassi et al. 2016 [29] | |
|---|---|---|---|---|---|
| Grade I | Localized pain, aggravated by movement, minor disability, mild swelling, ecchymosis, local tenderness, minimal haemorrhage. | Minimal pain to palpation, well localized. | Small tear, <5% loss of function | <10° ROM loss. | Minimal and localized pain, minimal hemorrage and swelling, mild ROM loss (<10°). |
| Grade II | Localized pain, aggravated by movement, moderate disability, moderate swelling, ecchymosis, local tenderness, stretching and tearing of fibers, without complete disruption. | Substantial pain to palpation, poorly localized; 6–12 mmdifference in circumference, develops within 12–24 h; <50% loss of ROM; pain on contraction with loss of power and disturbed gait. | Larger tear, 5–50% loss of function. | 10–25° ROM loss. | Moderate pain, moderate swelling and disability, loss of function between 5% and 50% and moderate ROM loss (10–25°). |
| Grade III | Severe pain, and disability, severe swelling, ecchymosis, hematoma, palpable defect and loss of muscle function; muscle or tendon rupture. | Intractable pain to palpation, diffuse; >12 mm difference in circumference, develops rapidly within one hour; >50% loss of ROM; severe pain on contraction with almost total loss of power with flicker contractions and unable to bear weight. | Complete tear >50% loss of function. | >25° ROM loss. | Severe pain and disability, more of 50% of loss of function and severe ROM loss (up to 25°). |
| Takebayashi et al. 1995 | Peetrons 2002 | Lee et al. 2004 | Chan et al. 2012 | |
|---|---|---|---|---|
| Grade I | “<20% cross-sectional area.” | “Minimal elongations with less than 5% of muscle involved.” | “Normal, or focal/general areas of increased echogenicity +/− peri-fascial fluid.” | “Normal appearance; focal or general increased echogenicity with no architectural distortion.” |
| Grade II | “20–50% cross-sectional area.” | “5–50% muscle involvement, partial muscle rupture, demonstrable hypo or an echoic gap, with “bell clapper” sign.” | “Discontinuity of muscle fibers in echogenic perimyseal striae; hypervascularity around disrupted muscle fibers; intramuscular fluid collection; partial detachment of adjacent fascia or aponeurosis.” | “Discontinuous muscle fibers; disruption site is hypervascularized and altered in echogenicity; no perimyseal striation adjacent to the MTJ.” |
| Grade III | “>50% cross-sectional area.” | “Complete tear of muscle or fascia, with extravasation of collection away from injured part of muscle.” | “Complete myotendinous or osteotendinous avulsion; complete discontinuity of muscle fibers and associated hematoma; “bell clapper” sign.” | “Complete discontinuity of muscle fibers; hematoma and retraction of the muscle ends.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paoletta, M.; Moretti, A.; Liguori, S.; Snichelotto, F.; Menditto, I.; Toro, G.; Gimigliano, F.; Iolascon, G. Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities. Medicina 2021, 57, 1040. https://doi.org/10.3390/medicina57101040
Paoletta M, Moretti A, Liguori S, Snichelotto F, Menditto I, Toro G, Gimigliano F, Iolascon G. Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities. Medicina. 2021; 57(10):1040. https://doi.org/10.3390/medicina57101040
Chicago/Turabian StylePaoletta, Marco, Antimo Moretti, Sara Liguori, Francesco Snichelotto, Ilaria Menditto, Giuseppe Toro, Francesca Gimigliano, and Giovanni Iolascon. 2021. "Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities" Medicina 57, no. 10: 1040. https://doi.org/10.3390/medicina57101040
APA StylePaoletta, M., Moretti, A., Liguori, S., Snichelotto, F., Menditto, I., Toro, G., Gimigliano, F., & Iolascon, G. (2021). Ultrasound Imaging in Sport-Related Muscle Injuries: Pitfalls and Opportunities. Medicina, 57(10), 1040. https://doi.org/10.3390/medicina57101040