
Umbilical Cord Knots: Is the Number Related to Fetal Risk?

 ,
, 
 ,
, 
Abstract
:1. Introduction
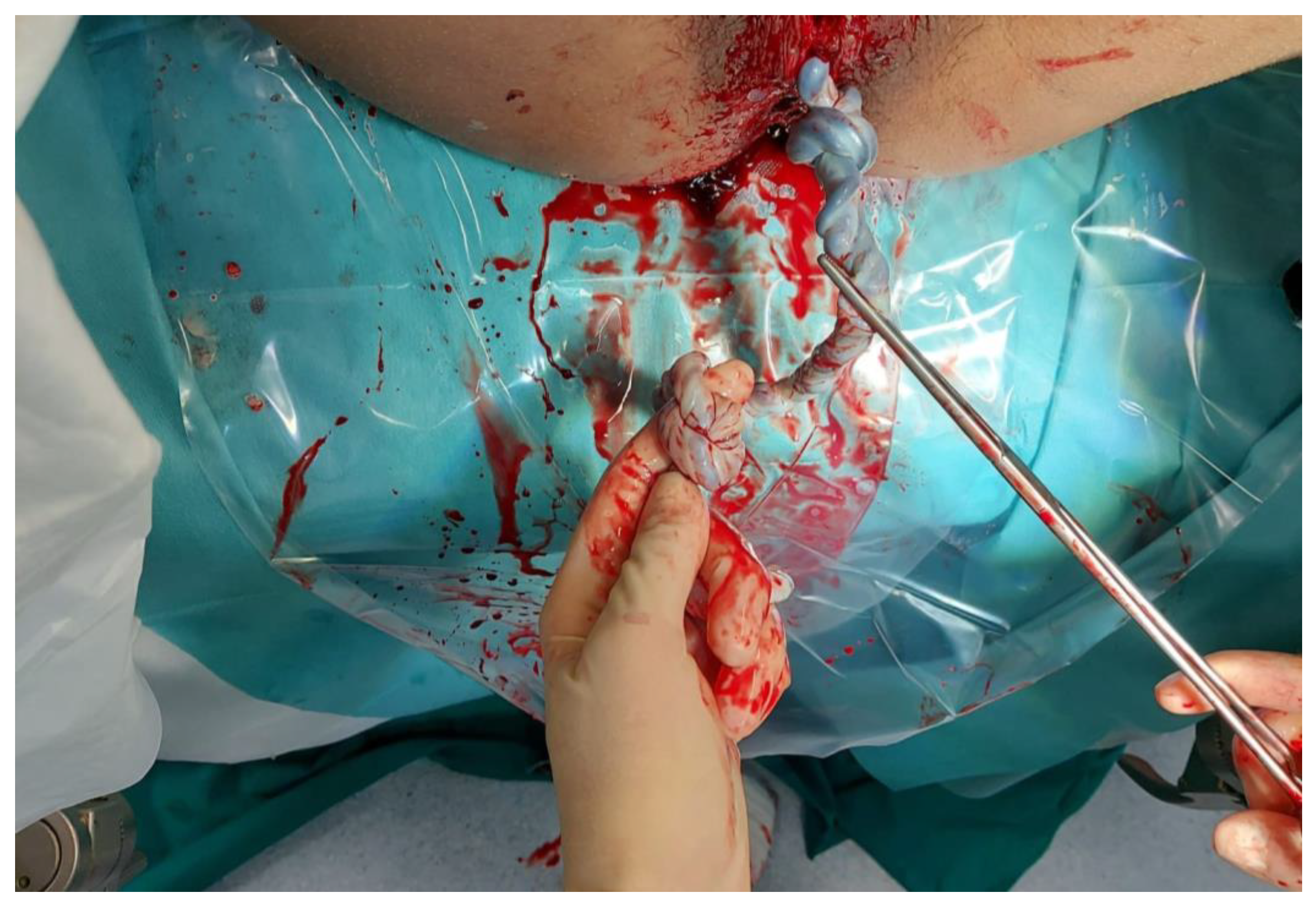
2. Case
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hershkovitz, R.; Silberstein, T.; Sheiner, E.; Shoham-Vardi, I.; Holcberg, G.; Katz, M.; Mazor, M. Risk factors associated with true knots of the umbilical cord. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 98, 36–39. [Google Scholar] [CrossRef]
- Guzikowski, W.; Kowalczyk, D.; Więcek, J. Diagnosis of true umbilical cord knot. Arch. Med Sci. 2014, 10, 91–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, R.N. Combined simple and complex cord knots. Eur. J. Obstet. Gynecol. Reprod. Biol. 1995, 62, 131–133. [Google Scholar] [CrossRef]
- Maher, J.T.; Conti, J.A. A comparison of umbilical cord blood gas values between newborns with and without true knots. Obstet. Gynecol. 1996, 88, 863–866. [Google Scholar] [CrossRef]
- Linde, L.E.; Rasmussen, S.; Kessler, J.; Ebbing, C. Extreme umbilical cord lengths, cord knot and entanglement: Risk factors and risk of adverse outcomes, a population-based study. PLoS ONE 2018, 13, e0194814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zbeidy, R.; Souki, F.G. One long umbilical cord, four nuchal cord loops and a true knot. BMJ Case Rep. 2017, 2017, bcr2017223241. [Google Scholar] [CrossRef] [Green Version]
- Carlucci, S.; Stabile, G.; Sorrentino, F.; Nappi, L.; Botta, G.; Menato, G.; Masturzo, B. The singular case of multiple chorangioma syndrome in an IVF pregnancy. Analysis of the case and review of literature. Placenta 2020, 103, 120–123. [Google Scholar] [CrossRef]
- Carlucci, S.; Stabile, G.; Catagini, S.; Borghi, C.; Scutiero, G.; Morano, D.; Greco, P. Fetal disseminated intravascular coagulopathy, hydrops and massive umbilical vein thrombosis consequence of a rare placental condition: Multifocal chorangiomatosis. J. Matern. Neonatal Med. 2020, 1–5. [Google Scholar] [CrossRef]
- Nappi, L.; Trezza, F.; Bufo, P.; Riezzo, I.; Turillazzi, E.; Borghi, C.; Bonaccorsi, G.; Scutiero, G.; Fineschi, V.; Greco, P. Classification of stillbirths is an ongoing dilemma. J. Périnat. Med. 2016, 44, 837–843. [Google Scholar] [CrossRef] [Green Version]
- Di Massa, G.; Stabile, G.; Romano, F.; Balduit, A.; Mangogna, A.; Belmonte, B.; Canu, P.; Bertucci, E.; Ricci, G.; Salviato, T. CD133 Expression in Placenta Chorioangioma Presenting as a Giant Asymptomatic Mass. Medicina 2021, 57, 162. [Google Scholar] [CrossRef]
- Kong, C.W.; Chan, L.W.; To, W.W. Neonatal outcome and mode of delivery in the presence of nuchal cord loops: Implications on patient counselling and the mode of delivery. Arch. Gynecol. Obstet. 2015, 292, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Weiner, E.; Fainstein, N.; Schreiber, L.; Sagiv, R.; Bar, J.; Kovo, M. The association between umbilical cord abnormalities and the development of non-reassuring fetal heart rate leading to emergent cesarean deliveries. J. Perinatol. 2015, 35, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.J.L.; Warland, J.; Parast, M.M.; Bendon, R.W.; Hasegawa, J.; Banks, J.; Clapham, L.; Heazell, A.E.P. Umbilical cord characteristics and their association with adverse pregnancy outcomes: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0239630. [Google Scholar] [CrossRef] [PubMed]
- Carter, E.B.; Chu, C.S.; Thompson, Z.; Tuuli, M.G.; Macones, G.A.; Cahill, A.G. True knot at the time of delivery: Electronic fetal monitoring characteristics and neonatal outcomes. J. Perinatol. 2018, 38, 1620–1624. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, Y.; Wainstock, T.; Walfisch, A.; Sheiner, E. The Significance of True Knot of the Umbilical Cord in Long-Term Offspring Neurological Health. J. Clin. Med. 2020, 10, 123. [Google Scholar] [CrossRef] [PubMed]
- Bohiltea, R.E.; Varlas, V.N.; Dima, V.; Iordache, A.M.; Salmen, T.; Mihai, B.M.; Bohiltea, A.T.; Vladareanu, E.M.; Ducu, I.; Grigoriu, C. The Strategy against Iatrogenic Prematurity Due to True Umbilical Knot: From Prenatal Diagnosis Challenges to the Favorable Fetal Outcome. J. Clin. Med. 2022, 11, 818. [Google Scholar] [CrossRef] [PubMed]
- López, R.; Cajal, C.; Ocampo, M. Prenatal diagnosis of true knot of the umbilical cord. Ultrasound Obstet. Gynecol. 2004, 23, 99–100. [Google Scholar] [CrossRef]
- Sherer, D.M.; Amoabeng, O.; Dryer, A.M.; Dalloul, M. Current Perspectives of Prenatal Sonographic Diagnosis and Clinical Management Challenges of True Knot of the Umbilical Cord. Int. J. Women Health 2020, 12, 221–233. [Google Scholar] [CrossRef] [Green Version]
- Díaz de la Noval, B.; Porcel Llaneza, I.; Rueda Sepúlveda, M.; Ferrer Barriendos, F.J.; Fernández Blanco, C. True umbilical cord knot, an emergency during labor. Clin. Case Rep. 2019, 7, 2242–2244. [Google Scholar] [CrossRef] [Green Version]
- Clerici, G.; Koutras, I.; Luzietti, R.; Di Renzo, G.C. Multiple true umbilical knots: A silent risk for intrauterine growth restriction with anomalous hemodynamic pattern. Fetal Diagn. Ther. 2007, 22, 440–443. [Google Scholar] [CrossRef]
- Srinivasan, A.; Graves, L. Four true umbilical cord knots. J. Obstet. Gynaecol. Can. 2006, 28, 32–35. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factors | Major risk factors: umbilical length Minor risk factors: polyhydramnios parity fetal sex |
| Diagnosis | There are no specific prenatal indications. Some authors assume that 3D power sonography may be useful: “Hanging noose” sign |
| Management | There are no clinical management guidelines. The presence of a true knot is not associated with electronic fetal monitoring, repetitive late decelerations or neonatal morbidity but there is a statistically significant higher rate of fetal distress and meconium-stained amniotic fluid and a four-fold higher rate of antepartum fetal death. Unknown risk in case of multiple knots. The caesarean section rate in these cases was significantly higher: OR for emergency caesarean deliveries due to non-reassuring fetal heart rate was 2.7 for the true knot and 2.9 for multiple UC loops. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stabile, G.; Carlucci, S.; De Bonis, L.; Sorrentino, F.; Nappi, L.; Ricci, G. Umbilical Cord Knots: Is the Number Related to Fetal Risk? Medicina 2022, 58, 703. https://doi.org/10.3390/medicina58060703
Stabile G, Carlucci S, De Bonis L, Sorrentino F, Nappi L, Ricci G. Umbilical Cord Knots: Is the Number Related to Fetal Risk? Medicina. 2022; 58(6):703. https://doi.org/10.3390/medicina58060703
Chicago/Turabian StyleStabile, Guglielmo, Stefania Carlucci, Lucia De Bonis, Felice Sorrentino, Luigi Nappi, and Giuseppe Ricci. 2022. "Umbilical Cord Knots: Is the Number Related to Fetal Risk?" Medicina 58, no. 6: 703. https://doi.org/10.3390/medicina58060703
APA StyleStabile, G., Carlucci, S., De Bonis, L., Sorrentino, F., Nappi, L., & Ricci, G. (2022). Umbilical Cord Knots: Is the Number Related to Fetal Risk? Medicina, 58(6), 703. https://doi.org/10.3390/medicina58060703