

Substantial Improvements in Facial Morphology through Surgical-Orthodontic Treatment: A Case Report and Literature Review
 , ,
, , 
 and
and
Abstract
:1. Introduction
2. Case Description
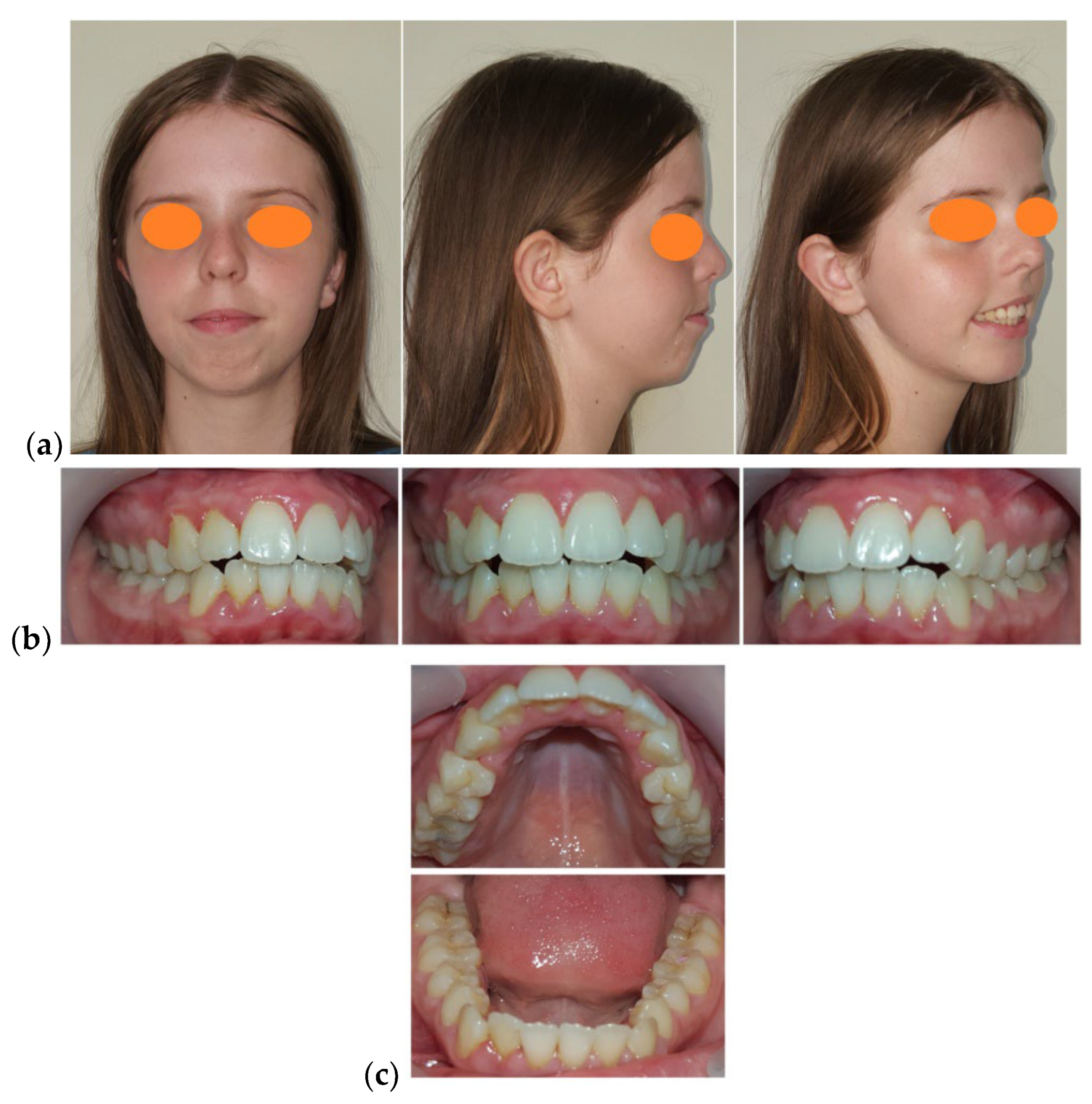
2.1. Patient Data
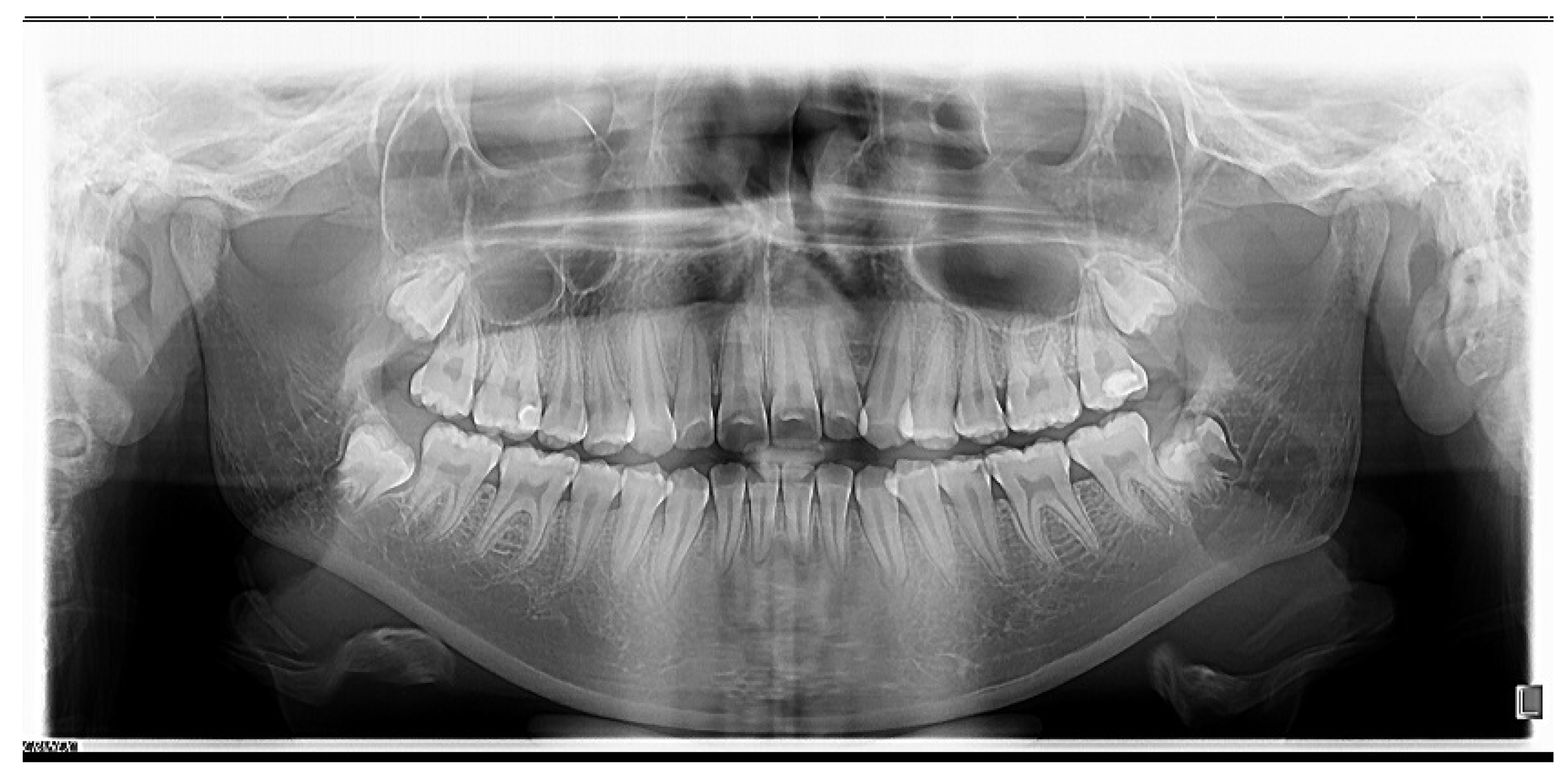
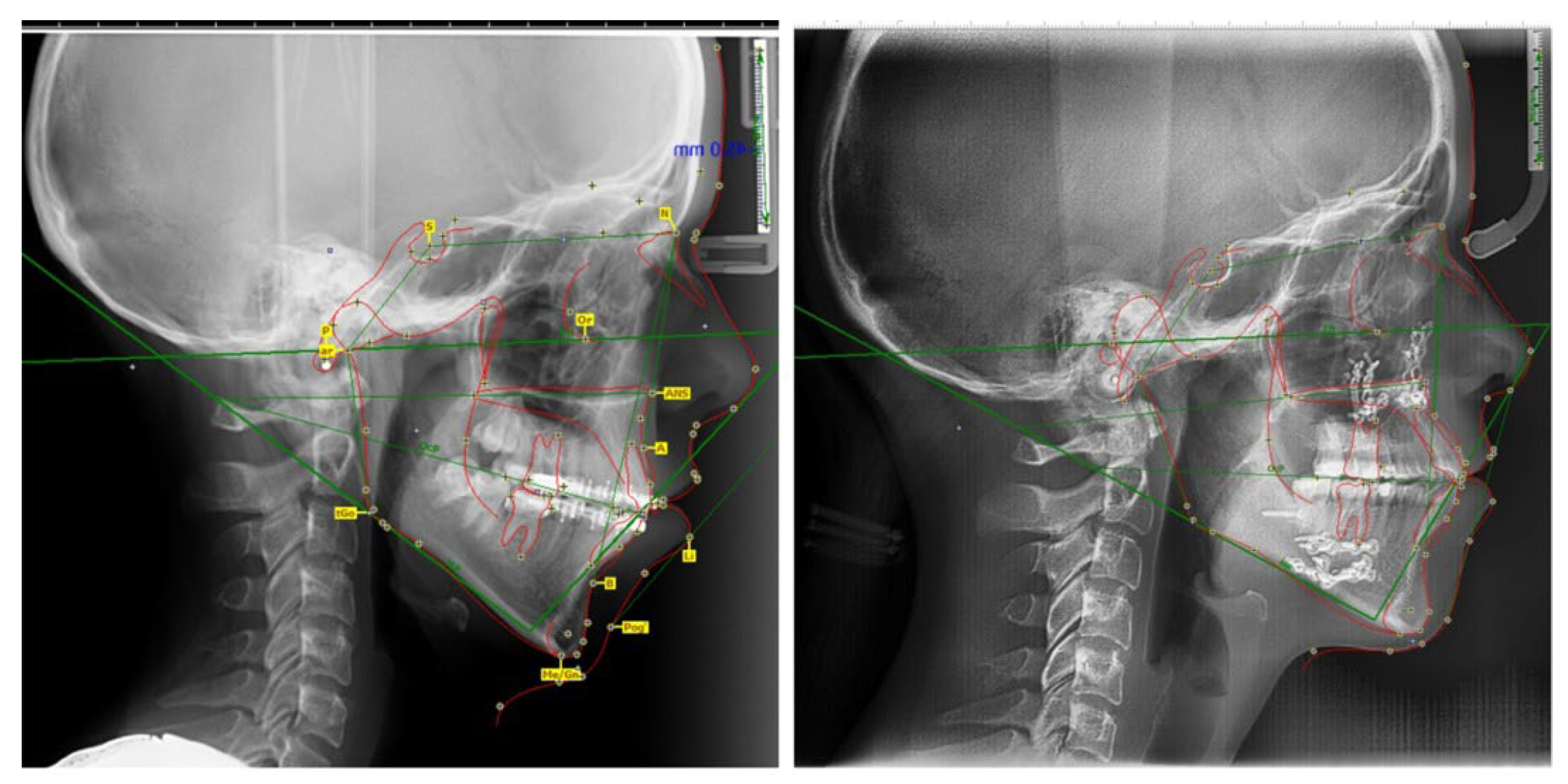
2.2. Results of Clinical and Paraclinical Examinations
2.3. Morphological Orthodontic Diagnosis
- Skeletal open bite in a 15.7-year-old patient with hyperleptoprosop morphological facial type (N-Gn/Zy-Zy = 111.66), high degree of hyperdivergence (FMA = 39.22°), bimaxillary dento-alveolar protrusion (IF = 120.85°, IMPA = 98.03°), 7 mm skeletal open-bite, and 3 mm vertical inocclusion of the anterior teeth;
- Skeletal class II relationships (SNA = 78.32°, SNB = 73.98°), bilateral half cusp class II molar and canine relationships;
- Labial incompetence, short upper lip, highly increased interlabial gap;
- Facial asymmetry;
- Excessive gingival exposure of 7 mm in smile;
- Bimaxillary anterior crowding.
2.4. Therapeutic Objectives
2.5. Initial Combined Treatment Plan
2.6. Intraoperative Considerations
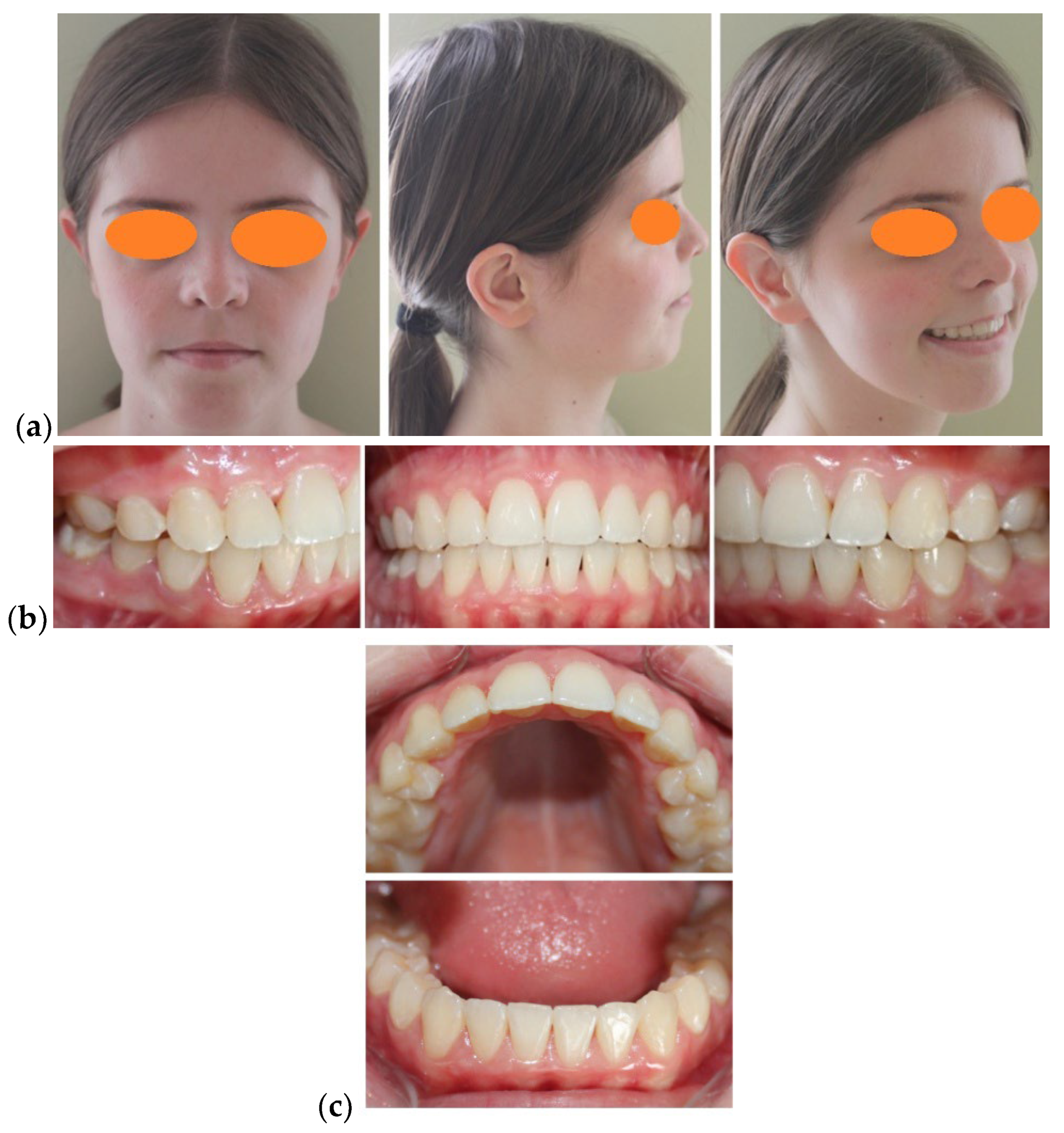
2.7. Treatment Outcome
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cole, J.B.; Spritz, R. The Genetics of Facial Morphology. In eLS; John Wiley & Sons Ltd.: Chichester, UK, 2017; pp. 1–9. [Google Scholar] [CrossRef]
- Abu, Alhaija, E. S.; Al Zo’ubi, I.A.; Al Rousan, M.E.; Hammad, M.M. Maximum occlusal bite forces in Jordanian individuals with different dentofacial vertical skeletal patterns. Eur. J. Orthod. 2010, 32, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Prasad, M.; Kannampallil, S.T.; Talapaneni, A.K.; George, S.A.; Shetty, S.K. Evaluation of arch width variations among different skeletal patterns in South Indian population. J. Nat. Sci. Biol. Med. 2013, 4, 94–102. [Google Scholar] [CrossRef]
- Forster, C.M.; Sunga, E.; Chung, C.H. Relationship between dental arch width and vertical facial morphology in untreated adults. Eur. J. Orthod. 2008, 30, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Satiroðlu, F.; Arun, T.; Iþik, F. Comparative data on facial morphology and muscle thickness using ultrasonography. Eur. J. Orthod. 2005, 27, 562–567. [Google Scholar] [CrossRef]
- Tsunori, M.; Mashita, M.; Kasai, K. Relationship between facial types and tooth and bone characteristics of the mandible obtained by CT scanning. Angle Orthod. 1998, 68, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Van Spronsen, P.H.; Weijs, W.A.; Valk, J.; Prahl-Andersen, B.; van Ginkel, F.C. A comparison of jaw muscle cross-sections of long-face and normal adults. J. Dent. Res. 1992, 71, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Kiliaridis, S.; Kälebo, P. Masseter muscle thickness measured by ultrasonography and its relation to facial morphology. J. Dent. Res. 1991, 70, 1262–1265. [Google Scholar] [CrossRef] [PubMed]
- Eöz, U.B.; Ceylan, I.; Aydemir, S. An investigation of mandibular morphology in subjects with different vertical facial growth patterns. Aust. Orthod. J. 2000, 16, 16–22. [Google Scholar]
- Tircoveluri, S.; Singh, J.R.; Rayapudi, N.; Karra, A.; Begum, M.; Challa, P.L. Correlation of Masseter Muscle Thickness and Intermolar Width—An Ultrasonography Study. J. Int. Oral Health. 2013, 5, 28–34. [Google Scholar]
- Banu, A.M.; Șerban, D.M.; Pricop, M.O.; Urechescu, H.C.; Roi, C.I.; Șerban, C.L. Craniofacial morphology and its relation to the eruption pattern of permanent teeth in the supporting zone of the dentition in a group of Romanian children in Timisoara. Rom. J. Morphol. Embryol. 2018, 59, 491–497. [Google Scholar] [PubMed]
- Bittner, C.; Pancherz, H. Facial morphology and malocclusions. Am. J. Orthod. Dentofac. Orthop. 1990, 97, 308–315. [Google Scholar] [CrossRef]
- Bratu, D.C.; Balan, R.A.; Szuhanek, C.A.; Pop, S.I.; Bratu, E.A.; Popa, G. Craniofacial morphology in patients with Angle Class II division 2 malocclusion. Rom. J. Morphol. Embryol. 2014, 55, 909–991. [Google Scholar] [PubMed]
- Saltaji, H.; Flores-Mir, C.; Major, P.W.; Youssef, M. The relationship between vertical facial morphology and overjet in untreated Class II subjects. Angle Orthod. 2012, 82, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Phor, D.; Upadhyay, S.; Sharma, A.; Vaidya, A. Correlation between Vertical Facial Patterns and Dental Arch Forms in Different Types of Skeletal Malocclusions. IOSR-JDMS 2018, 17, 67–88. [Google Scholar] [CrossRef]
- Al-Khateeb, E.A.; Al-Khateeb, S.N. Anteroposterior and vertical components of Class II division 1 and division 2 malocclusion. Angle Orthod. 2009, 79, 859–866. [Google Scholar] [CrossRef]
- Pancherz, H.; Zieber, K.; Hoyer, B. Cephalometric characteristics of Class II division 1 and Class II division 2 malocclusions: A comparative study in children. Angle Orthod. 1997, 67, 111–120. [Google Scholar] [CrossRef]
- Sayin, Ö.; Turkkaharaman, H. Cephalometric evaluation of nongrowing females with skeletal and dental Class II, division 1 malocclusion. Angle Orthod. 2004, 75, 656–660. [Google Scholar] [CrossRef]
- Karlsen, A.T.; Krogstad, O. Morphology and growth in convex profile facial patterns: A longitudinal study. Angle Orthod. 1999, 69, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Siriwat, P.P.; Jarabak, J.R. Malocclusion and facial morphology: Is there a relationship? Angle Orthod. 1985, 55, 127–138. [Google Scholar] [CrossRef]
- Al-Sairafi, E. The Characteristics of Craniofacial Complex of Class II Division 1 Malocclusion Patients in the Permanent Dentition. Master’s Thesis, Syria Tishreen University, Latakia, Syria, 2009. [Google Scholar]
- Silbermann, M.; Fmoynihan, F.M.; Maloney, P.L.; Ferullo, R.J.; Doku, H.C. Skeletal open bite associated with bimaxillary dento-alveolar protrusion, evaluation, and treatment. Br. J. Oral Surg. 1972, 10, 223–232. [Google Scholar] [CrossRef]
- Gonzalez, P.; Martínez, M.B.; Sierra, V.; Rueda, Z.V.; Botero-Mariaca, P. Tongue position assessment during oral phase deglutition in children with anterior open bite and normal vertical overbite. J. Indian Soc. Pedod. Prev. Dent. 2019, 37, 167–171. [Google Scholar] [PubMed]
- Farkas, L.G. (Ed.) Anthropometry of the Head and Face, 2nd ed.; Raven Press: New York, NY, USA, 1994. [Google Scholar]
- Prabu, N.M.; Kohila, K.; Sivaraj, S.; Prabu, P.S. Appraisal of the cephalometric norms for the upper and lower lips of the South Indian ethnic population. J. Pharm. Bioallied Sci. 2012, 4, S136–S138. [Google Scholar] [CrossRef] [PubMed]
- da Silva, A.M.; Magri, L.V.; Andrade, L.M.; da Silva, M.A. Three-dimensional analysis of facial morphology in Brazilian population with Caucasian, Asian, and Black ethnicity. J. Oral Res. Rev. 2017, 9, 1–7. [Google Scholar] [CrossRef]
- Bishara, S.E.; Cummins, D.M.; Jakobsen, J.R. The morphologic basis for the extraction decision in Class II, division 1 malocclusions: A comparative study. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 129–135. [Google Scholar] [CrossRef]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin. Orthod. 2005, 11, 119–129. [Google Scholar] [CrossRef]
- Vaida, L.L.; Bud, E.S.; Halitchi, L.G.; Cavalu, S.; Todor, B.I.; Negrutiu, B.M.; Moca, A.E.; Bodog, F.D. The Behavior of Two Types of Upper Removable Retainers—Our Clinical Experience. Children 2020, 7, 295. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.; Cevidanes, L.H.; Proffit, W.R. Stability and predictability of orthognathic surgery. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 273–277. [Google Scholar] [CrossRef]
- Vaida, L.; Corega, C.; Roşeanu, G. Letter to editor: Research regarding current self-related cognitions in patients with orthodontic treatment. J. Cogn. Behav. Psychot. 2009, 9, 131–133. Available online: http://scipio.ro/documents/13115/1e5f0445-c0dd-4811-95bb-f0648c4da898 (accessed on 2 May 2022).
- Baghdadi, Z.D.; Jbara, S.; Muhajarine, N. Children’s Drawing as a Projective Measure to Understand Their Experiences of Dental Treatment under General Anesthesia. Children 2020, 7, 73. [Google Scholar] [CrossRef] [PubMed]
- Corega, C.; Vaida, L.; Festila, D.; Bertossi, D. Bilateral pneumothorax and pneumomediastinum after orthognathic surgery. Chirurgia (Bucur). 2014, 109, 271–274. [Google Scholar] [PubMed]
- Vaida, L.; Pirte, A.; Corega, C.; Slavescu, D.; Mutiu, G. Correlations between the changes in patients’ facial morphology at the end of the orthodontic treatment and the psychological variables. Rom. J. Morphol. Embryol. 2009, 50, 625–629. Available online: http://www.rjme.ro/RJME/resources/files/500409625629.pdf (accessed on 2 May 2022). [PubMed]
- Conley, R.S.; Legan, H.L. Correction of Severe Vertical Maxillary Excess with Anterior Open Bite and Transverse Maxillary Deficiency. Angle Orthod. 2002, 72, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.S.; Dakir, A.; Krishnan, B.; Ebenezer, V.; Muthumani, K.; Arvindet, W. Surgery preceding orthodontics in bimaxillary cases. J. Pharm. Bioallied Sci. 2015, 7, S101–S106. [Google Scholar] [CrossRef] [PubMed]
- Jayaratne, Y.S.; Zwahlen, R.A.; Lo, J.; Cheung, L.K. Facial soft tissue response to anterior segmental osteotomies: A systematic review. Int. J. Oral Maxillofac. Surg. 2010, 39, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Paunonen, J.; Helminem, M.; Peltomaki, T. Duration of orthognathic-surgical treatment. Acta Odontol. Scand. 2017, 75, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Dowling, P.A.; Espeland, L.; Krogstad, O.; Stenvik, A.; Kelly, A. Duration of orthodontic treatment involving orthognathic surgery. Int. J. Adult Orthod. Orthognath. Surg. 1999, 14, 146–152. [Google Scholar]
- Luther, F.; Morris, D.O.; Karmezi, K. Orthodontic treatment following orthognathic surgery: How long does it take and why? A retrospective study. J. Oral Maxillofac. Surg. 2007, 65, 1969–1976. [Google Scholar] [CrossRef]
- Vaida, L.; Mutiu, G.; Tara, I.G.; Bodog, F. An Algorithm of Ethical Approach to the Orthodontic Patients. Iran. J. Public Health 2015, 44, 1296–1298. [Google Scholar] [PubMed]
- Scheffler, N.R.; Proffit, W.R.; Phillips, C. Outcomes and stability in patients with anterior open bite and long anterior face height treated with temporary anchorage devices and a maxillary intrusion splint. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 594–602. [Google Scholar] [CrossRef]
- Erverdi, N.; Keles, A.; Nanda, R. The use of skeletal anchorage in open bite treatment: A cephalometric evaluation. Angle Orthod. 2004, 74, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Xun, C.; Zeng, X.; Wang, X. Microscrew anchorage in skeletal anterior open bite treatment. Angle Orthod. 2007, 77, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, S.; Sakai, Y.; Tamamura, N.; Deguchi, T.; Takano-Yamamoto, T. Treatment of severe anterior open bite with skeletal anchorage in adults: Comparison with orthognathic surgery outcomes. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Scheffler, N.R.; Proffit, W.R. Miniscrew-supported posterior intrusion for treatment of anterior open bite. J. Clin. Orthod. 2014, 48, 158–168. [Google Scholar] [PubMed]
- Wirthlin, J.O.; Shetye, P.R. Orthodontist’s Role in Orthognathic Surgery. Semin. Plast. Surg. 2013, 27, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Profitt, W.R.; Turvey, T.A.; Phillips, C. Orthognathic surgery: A hierarchy of stability. Int. J. Adult Orthod. Orthognath. Surg. 1996, 11, 191–204. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Normal Values | Pre- Treatment | Before Orthognatic Surgery | After Orthognatic Surgery | Differences |
|---|---|---|---|---|---|
| FMA | 25 ± 3° | 39.22° | 36.13° | 28.23° | 10.99° |
| IMPA | 88 ± 3° | 98.03° | 93.22° | 91.14° | 6.89° |
| SNA | 82 ± 2° | 78.32° | 78.17° | 80.35° | −2.03° |
| SNB | 80 ± 2° | 73.98° | 74.12° | 78.22° | −4.24° |
| IF | 107° ± 5° | 120.85° | 107.32° | 111.80° | 9.05° |
| HFP/HFA | 0.69 | 0.52 | 0.54 | 0.64 | 0.12 |
| Upper lip length (mm) | 23.4 ± 3.42 | 14.5 | 14.7 | 16.8 | 2.3 |
| FMI | 81.9 | 111.6 | 110.2 | 84.3 | 27.3 |
| U1-SN | 103 ± 7° | 115.12° | 104.78° | 109.50° | 5.62° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaida, L.L.; Negruțiu, B.M.; Zetu, I.N.; Moca, A.E.; Bran, S. Substantial Improvements in Facial Morphology through Surgical-Orthodontic Treatment: A Case Report and Literature Review. Medicina 2022, 58, 1043. https://doi.org/10.3390/medicina58081043
Vaida LL, Negruțiu BM, Zetu IN, Moca AE, Bran S. Substantial Improvements in Facial Morphology through Surgical-Orthodontic Treatment: A Case Report and Literature Review. Medicina. 2022; 58(8):1043. https://doi.org/10.3390/medicina58081043
Chicago/Turabian StyleVaida, Luminița Ligia, Bianca Maria Negruțiu, Irina Nicoleta Zetu, Abel Emanuel Moca, and Simion Bran. 2022. "Substantial Improvements in Facial Morphology through Surgical-Orthodontic Treatment: A Case Report and Literature Review" Medicina 58, no. 8: 1043. https://doi.org/10.3390/medicina58081043
APA StyleVaida, L. L., Negruțiu, B. M., Zetu, I. N., Moca, A. E., & Bran, S. (2022). Substantial Improvements in Facial Morphology through Surgical-Orthodontic Treatment: A Case Report and Literature Review. Medicina, 58(8), 1043. https://doi.org/10.3390/medicina58081043