
Pneumocystis jirovecii Pneumonia Associated with COVID-19 in Patients with Interstitial Pneumonia


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
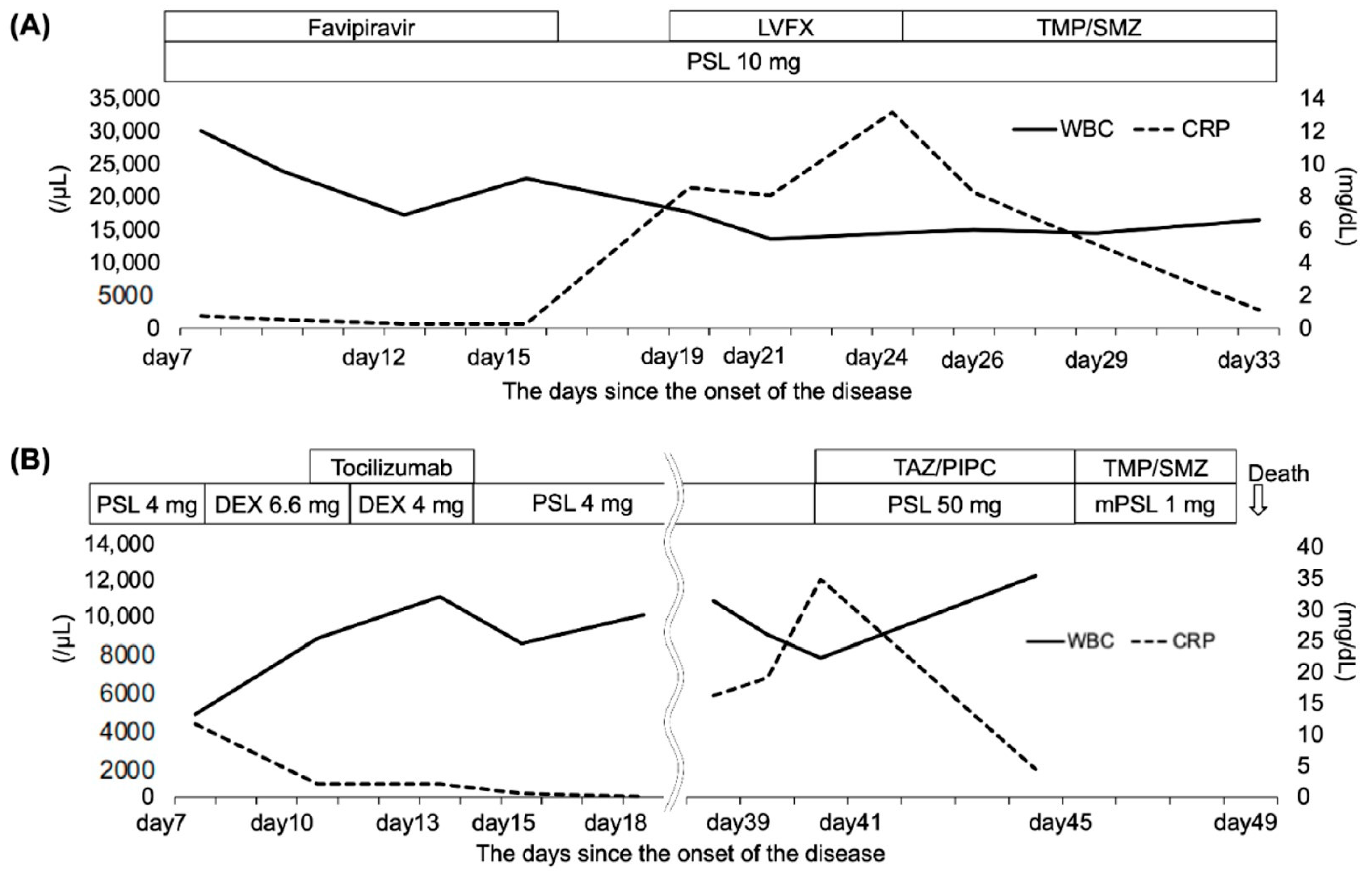
2.1. Case 1
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Recovery Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.C. Immunosuppressive agents and interstitial lung disease: What are the risks? Expert. Rev. Respir. Med. 2014, 8, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Kondoh, Y.; Kataoka, K.; Ando, M.; Awaya, Y.; Ichikado, K.; Kataoka, M.; Komase, Y.; Mineshita, M.; Ohno, Y.; Okamoto, H.; et al. COVID-19 and acute exacerbation of interstitial lung disease. Respir. Investig. 2021, 59, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Gerver, S.M.; Guy, R.; Wilson, K.; Thelwall, S.; Nsonwu, O.; Rooney, G.; Brown, C.S.; Muller-Pebody, B.; Hope, R.; Hal, V. National surveillance of bacterial and fungal coinfection and secondary infection in COVID-19 patients in England: Lessons from the first wave. Clin. Microbiol. Infect. 2021, 27, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Youngs, J.; Wyncoll, D.; Hopkins, P.; Arnold, A.; Ball, J.; Bicanic, T. Improving antibiotic stewardship in COVID-19: Bacterial co-infection is less common than with influenza. J. Infect. 2020, 81, e55–e57. [Google Scholar] [CrossRef] [PubMed]
- Ng, B.H.; Ban, A.Y.; Nik Abeed, N.N.; Faisal, M. Organising pneumonia manifesting as a late-phase complication of COVID-19. BMJ Case Rep. 2021, 14, e246119. [Google Scholar] [CrossRef] [PubMed]
- Gentile, I.; Viceconte, G.; Lanzardo, A.; Zotta, I.; Zappulo, E.; Pinchera, B.; Scotto, R.; Schiano Moriello, N.; Foggia, M.; Giaccone, A.; et al. Pneumocystis jirovecii Pneumonia in Non-HIV Patients Recovering from COVID-19: A Single-Center Experience. Int. J. Environ. Res. Public Health 2021, 18, 11399. [Google Scholar] [CrossRef] [PubMed]
- Fonte, L.; Acosta, A.; Sarmiento, M.E.; Norazmi, M.N.; Ginori, M.; de Armas, Y.; Calderón, E.J. Overlapping of Pulmonary Fibrosis of Postacute COVID-19 Syndrome and Tuberculosis in the Helminth Coinfection Setting in Sub-Saharan Africa. Trop. Med. Infect. Dis. 2022, 7, 157. [Google Scholar] [CrossRef]
- Zhong-Jie, H.; Jia, X.; Ji-Ming, Y.; Li, L.; Wei, H.; Li-Li, Z.; Zhen, Z.; Yi-Zhou, Y.; Hong-Jun, L.; Ying-Mei, F.; et al. Lower Circulating Interferon-Gamma Is a Risk Factor for Lung Fibrosis in COVID-19 Patients. Front. Immunol. 2020, 11, 585647. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, T.; Saito, A.; Kuronuma, K.; Nishikiori, H.; Chiba, H. Pneumocystis jirovecii Pneumonia Associated with COVID-19 in Patients with Interstitial Pneumonia. Medicina 2022, 58, 1151. https://doi.org/10.3390/medicina58091151
Takahashi T, Saito A, Kuronuma K, Nishikiori H, Chiba H. Pneumocystis jirovecii Pneumonia Associated with COVID-19 in Patients with Interstitial Pneumonia. Medicina. 2022; 58(9):1151. https://doi.org/10.3390/medicina58091151
Chicago/Turabian StyleTakahashi, Tomoyuki, Atsushi Saito, Koji Kuronuma, Hirotaka Nishikiori, and Hirofumi Chiba. 2022. "Pneumocystis jirovecii Pneumonia Associated with COVID-19 in Patients with Interstitial Pneumonia" Medicina 58, no. 9: 1151. https://doi.org/10.3390/medicina58091151
APA StyleTakahashi, T., Saito, A., Kuronuma, K., Nishikiori, H., & Chiba, H. (2022). Pneumocystis jirovecii Pneumonia Associated with COVID-19 in Patients with Interstitial Pneumonia. Medicina, 58(9), 1151. https://doi.org/10.3390/medicina58091151