


Prediction of Acute Respiratory Distress Syndrome in Traumatic Brain Injury Patients Based on Machine Learning Algorithms

Abstract
:1. Introduction
2. Methods and Materials
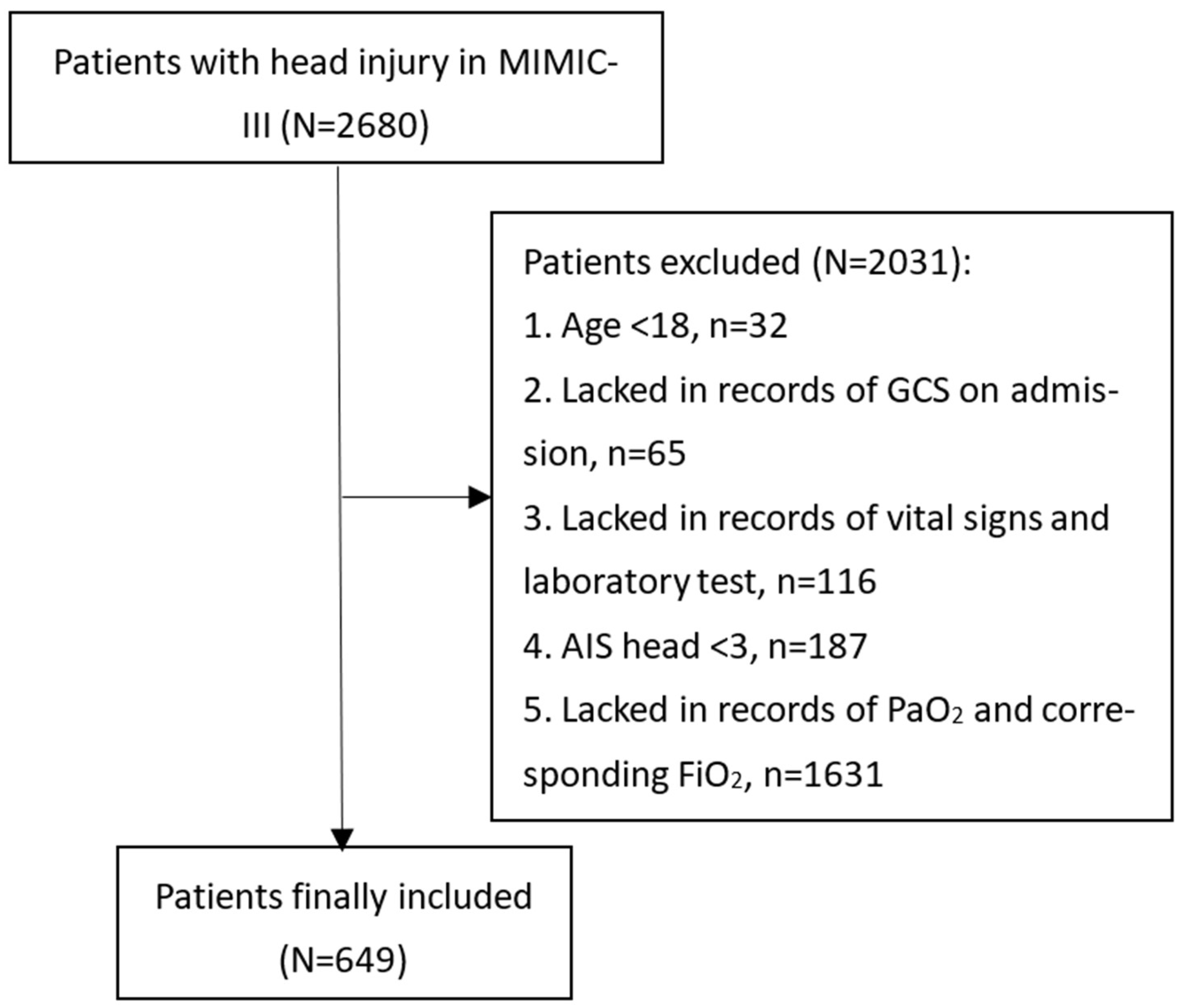
2.1. Patients
2.2. Study Variables
2.3. Statistical Analysis
2.4. Machine Learning Algorithms
3. Results
3.1. Comparison between Final Included Patients and Those Lacking Records of PaO2 and FiO2
3.2. Baseline Characteristics of Included TBI Patients
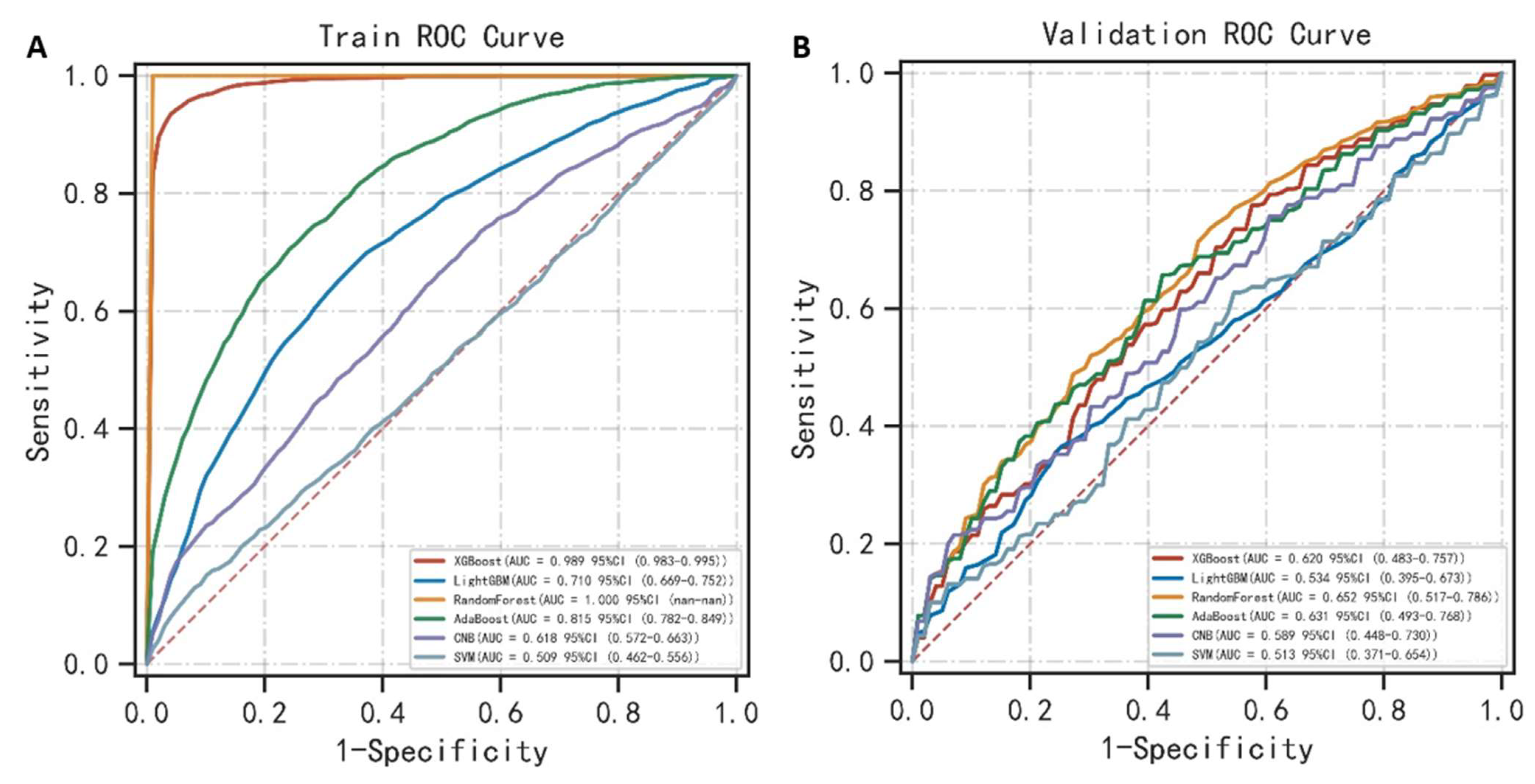
3.3. Performance of Machine Learning Algorithms for Predicting ARDS in TBI
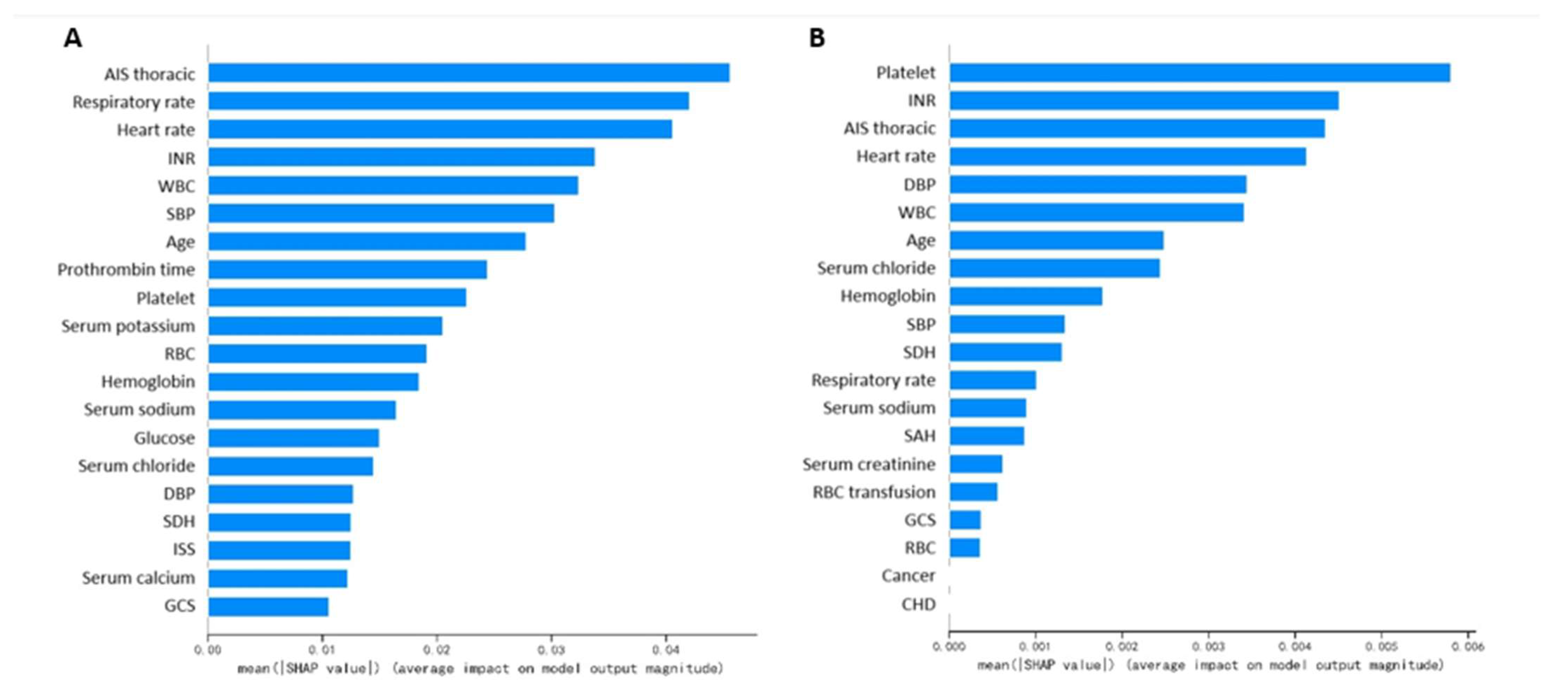
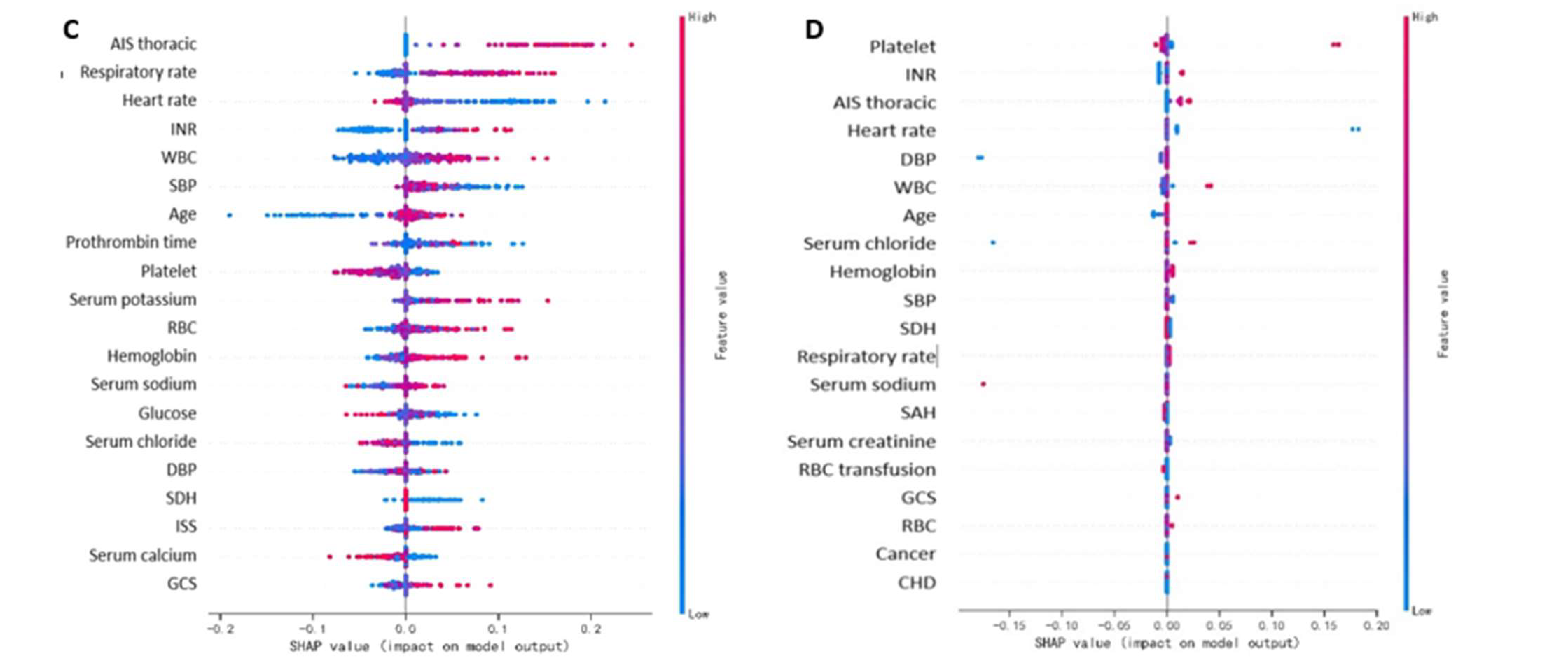
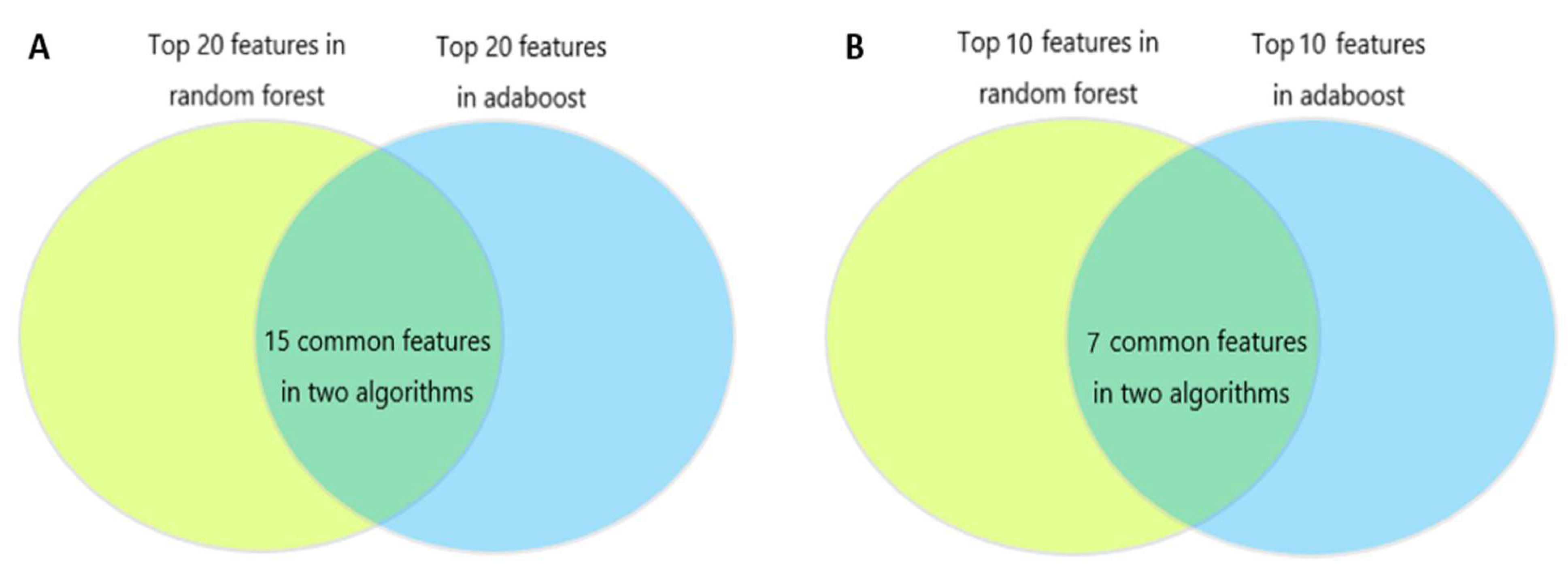
3.4. Important Features in Machine Learning Algorithms for Predicting ARDS in TBI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. JNS 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corral, L.; Javierre, C.F.; Ventura, J.L.; Marcos, P.; Herrero, J.I.; Manez, R. Impact of non-neurological complications in severe traumatic brain injury outcome. Crit. Care 2012, 16, R44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oddo, M.; Nduom, E.; Frangos, S.; MacKenzie, L.; Chen, I.; Maloney-Wilensky, E.; Kofke, W.A.; Levine, J.M.; LeRoux, P.D. Acute lung injury is an independent risk factor for brain hypoxia after severe traumatic brain injury. Neurosurgery 2010, 67, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Aisiku, I.P.; Yamal, J.-M.; Doshi, P.; Rubin, M.L.; Benoit, J.S.; Hannay, J.; Tilley, B.C.; Gopinath, S.; Robertson, C.S. The incidence of ARDS and associated mortality in severe TBI using the Berlin definition. J. Trauma Acute Care Surg. 2016, 80, 308–312. [Google Scholar] [CrossRef] [Green Version]
- Thiara, S.; Griesdale, D.E.; Henderson, W.R.; Sekhon, M.S. Effect of Cerebral Perfusion Pressure on Acute Respiratory Distress Syndrome. The Canadian journal of neurological sciences. J. Can. Sci. Neurol. 2018, 45, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Hendrickson, C.M.; Howard, B.M.; Kornblith, L.Z.; Conroy, A.S.; Nelson, M.F.; Zhuo, H.; Liu, K.D.; Manley, G.T.; Matthay, M.A.; Calfee, C.S.; et al. The acute respiratory distress syndrome following isolated severe traumatic brain injury. J. Trauma Acute Care Surg. 2016, 80, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Komisarow, J.M.; Chen, F.; Vavilala, M.S.; Laskowitz, D.; James, M.L.; Krishnamoorthy, V. Epidemiology and Outcomes of Acute Respiratory Distress Syndrome Following Isolated Severe Traumatic Brain Injury. J. Intensive Care Med. 2022, 37, 68–74. [Google Scholar] [CrossRef]
- Lou, M.; Chen, X.; Wang, K.; Xue, Y.; Cui, D.; Xue, F. Increased intracranial pressure is associated with the development of acute lung injury following severe traumatic brain injury. Clin. Neurol. Neurosurg. 2013, 115, 904–908. [Google Scholar] [CrossRef]
- Fan, T.H.; Huang, M.; Gedansky, A.; Price, C.; Robba, C.; Hernandez, A.V.; Cho, S.-M. Prevalence and Outcome of Acute Respiratory Distress Syndrome in Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Lung 2021, 199, 603–610. [Google Scholar] [CrossRef]
- ARDS Definition of Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. Jama 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- A Alexiou, G.; Tzima, A.; Lianos, G.D.; Lampros, M.; Sotiropoulos, A.; Rizos, D.; Ygropoulou, O.; Zika, J.; Alexiou, E.-S.; Voulgaris, S. Neutrophil to lymphocyte ratio in the prediction of coagulopathy in traumatic brain injury. Biomark. Med. 2022, 16, 163–168. [Google Scholar] [CrossRef]
- Maegele, M.; Schöchl, H.; Menovsky, T.; Maréchal, H.; Marklund, N.; Buki, A.; Stanworth, S. Coagulopathy and haemorrhagic progression in traumatic brain injury: Advances in mechanisms, diagnosis, and management. Lancet Neurol. 2017, 16, 630–647. [Google Scholar] [CrossRef] [PubMed]
- Epstein, D.S.; Mitra, B.; O’Reilly, G.; Rosenfeld, J.V.; Cameron, P.A. Acute traumatic coagulopathy in the setting of isolated traumatic brain injury: A systematic review and meta-analysis. Injury 2014, 45, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Wafaisade, A.; Dgu, T.R.O.; Lefering, R.; Tjardes, T.; Wutzler, S.; Simanski, C.; Paffrath, T.; Fischer, P.; Bouillon, B.; Maegele, M. Acute coagulopathy in isolated blunt traumatic brain injury. Neurocrit. Care 2010, 12, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Talving, P.; Benfield, R.; Hadjizacharia, P.; Inaba, K.; Chan, L.S.; Demetriades, D. Coagulopathy in severe traumatic brain injury: A prospective study. J. Trauma 2009, 66, 55–61, discussion 61–62. [Google Scholar] [CrossRef] [PubMed]
- Ware, L.B.; Matthay, M.A.; Parsons, P.E.; Thompson, B.T.; Januzzi, J.L.; Eisner, M.D. Pathogenetic and prognostic significance of altered coagulation and fibrinolysis in acute lung injury/acute respiratory distress syndrome. Crit. Care Med. 2007, 35, 1821–1828. [Google Scholar] [CrossRef]
- Hasegawa, N.; Husari, A.W.; Hart, W.T.; Kandra, T.G.; Raffin, T.A. Role of the coagulation system in ARDS. Chest 1994, 105, 268–277. [Google Scholar] [CrossRef]
- Frantzeskaki, F.; Armaganidis, A.; Orfanos, S.E. Immunothrombosis in Acute Respiratory Distress Syndrome: Cross Talks between Inflammation and Coagulation. Respir. Int. Rev. Thorac. Dis. 2017, 93, 212–225. [Google Scholar] [CrossRef]
- Prabhakaran, P.; Ware, L.B.; White, K.E.; Cross, M.T.; Matthay, M.A.; Olman, M.A. Elevated levels of plasminogen activator inhibitor-1 in pulmonary edema fluid are associated with mortality in acute lung injury. Am. J. Physiol. Lung Cell. Mol. Physiol. 2003, 285, L20–L28. [Google Scholar] [CrossRef] [Green Version]
- Yeung, E.; Miller, M.; Wung, C.; Behm, R.; Cagir, B.; Granet, P. Possible Predictive Factor of Acute Respiratory Distress Syndrome Development After Mild Traumatic Brain Injury: A Single Rural Trauma Center Preliminary Study. Cureus 2021, 13, e16508. [Google Scholar] [CrossRef]
- Killien, E.Y.; Mills, B.; Vavilala, M.S.; Watson, R.S.; O’Keefe, G.E.; Rivara, F.P. Association between age and acute respiratory distress syndrome development and mortality following trauma. J. Trauma Acute Care Surg. 2019, 86, 844–852. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall Patients (n = 649) | Non-ARDS Group (n = 328, 50.5%) | ARDS Group (n = 321, 49.5%) | p |
|---|---|---|---|---|
| Age (year) | 59.3 (38.8–77.4) | 57.2 (31.9–76.1) | 62.7 (44.0–78.1) | 0.027 |
| Male gender, n (%) | 424 (65.3%) | 208 (63.4%) | 216 (67.3%) | 0.300 |
| Comorbidities | ||||
| Diabetes, n (%) | 93 (14.3%) | 47 (14.3%) | 46 (14.3%) | 1.000 |
| Hypertension, n (%) | 187 (28.8%) | 85 (25.9%) | 102 (31.8%) | 0.099 |
| Hyperlipidemia, n (%) | 47 (7.2%) | 25 (7.6%) | 22 (6.9%) | 0.706 |
| Coronary heart disease, n (%) | 54 (8.3%) | 27 (8.2%) | 27 (8.4%) | 0.934 |
| Liver disease, n (%) | 21 (3.2%) | 10 (3.0%) | 11 (3.4%) | 0.786 |
| Chronic renal disease, n (%) | 24 (3.7%) | 11 (3.4%) | 13 (4.1%) | 0.638 |
| Malignancy, n (%) | 42 (6.5%) | 16 (4.9%) | 26 (8.1%) | 0.095 |
| Vital signs on admission | ||||
| Systolic blood pressure (mmHg) | 130 (113–146) | 131 (114–147) | 130 (112–144) | 0.584 |
| Diastolic blood pressure (mmHg) | 64 ± 17 | 64 ± 17 | 64 ± 16 | 0.811 |
| Heart rate (s−1) | 84 (71–97) | 84 (73–95) | 84 (71–98) | 0.959 |
| Respiratory rate (s−1) | 17 (14–20) | 17 (14–20) | 17 (14–20) | 0.299 |
| GCS | 6 (3–9) | 6 (3–9) | 6 (3–9) | 0.724 |
| AIS chest | 0 (0–3) | 0 (0–0) | 0 (0–3) | <0.001 |
| ISS | 20 (16–29) | 18 (16–25) | 22 (16–29) | 0.009 |
| Laboratory tests | ||||
| WBC (109/L) | 13.40 (10.00–18.10) | 13.30 (9.90–17.30) | 13.50 (10.10–18.80) | 0.348 |
| Platelet (109/L) | 228 (175–288) | 238 (190–292) | 221 (166–277) | 0.004 |
| RBC (109/L) | 4.07 (3.60–4.51) | 4.07 (3.63–4.48) | 4.09 (3.55–4.53) | 0.874 |
| Hemoglobin (g/dL) | 12.70 (11.20–14.00) | 12.80 (11.30–13.90) | 12.60 (11.10–14.30) | 0.713 |
| Glucose (mg/dL) | 149 (121–186) | 143 (118–186) | 153 (123–185) | 0.246 |
| Blood urea nitrogen (mg/dL) | 16 (12–22) | 16 (12–22) | 16 (12–22) | 0.275 |
| Serum creatinine (mg/dL) | 0.90 (0.70–1.10) | 0.90 (0.70–1.10) | 0.90 (0.70–1.10) | 0.522 |
| Serum sodium (mmol/L) | 140 (137–142) | 139 (137–142) | 140 (138–142) | 0.053 |
| Serum potassium (mmol/L) | 3.90 (3.60–4.30) | 3.90 (3.60–4.20) | 3.90 (3.60–4.30) | 0.195 |
| Serum chloride (mmol/L) | 105 (102–109) | 105 (101–109) | 105 (102–109) | 0.787 |
| Serum calcium (mmol/L) | 1.17 (1.06–8.20) | 1.19 (1.06–8.20) | 1.17 (1.05–8.20) | 0.561 |
| Prothrombin time (s) | 13.20 (12.60–14.30) | 13.00 (12.60–14.00) | 13.30 (12.70–14.70) | 0.002 |
| INR | 1.20 (1.10–1.30) | 1.10 (1.10–1.30) | 1.20 (1.10–1.40) | <0.001 |
| PaO2 on the first day (mmHg) | 228 (141–329) | 255 (196–364) | 179 (104–289) | <0.001 |
| FiO2 on the first day (%) | 100 (50–100) | 100 (50–100) | 100 (50–100) | 0.874 |
| PaO2/FiO2 ratio on the first day (mmHg) | 304 (190–428) | 356 (248–452) | 248 (143–361) | <0.001 |
| Intracranial injury types | ||||
| Epidural hemorrhage, n (%) | 174 (26.8%) | 103 (31.4%) | 71 (22.1%) | 0.008 |
| Subdural hemorrhage, n (%) | 339 (52.2%) | 187 (57.0%) | 152 (47.4%) | 0.014 |
| Subarachnoid hemorrhage, n (%) | 296 (45.6%) | 161 (49.1%) | 135 (42.1%) | 0.072 |
| Intraparenchymal hemorrhage, n (%) | 146 (22.5%) | 76 (23.2%) | 70 (21.8%) | 0.677 |
| Treatments | ||||
| RBC during the first 24 h, n (%) | 87 (13.4%) | 51 (15.5%) | 36 (11.2%) | 0.105 |
| Platelet during the first 24 h, n (%) | 73 (11.2%) | 28 (8.5%) | 45 (14.0%) | 0.027 |
| Anticoagulants during the first 24 h, n (%) | 156 (24.0%) | 79 (24.1%) | 77 (24.0%) | 0.977 |
| Antiplatelets during the first 24 h, n (%) | 5 (0.7%) | 2 (0.6%) | 3 (0.9%) | 0.636 |
| Vasopressor during the first 24 h, n (%) | 88 (13.6%) | 46 (14.0%) | 42 (13.1%) | 0.726 |
| Mechanical ventilation, n (%) | 591 (91.1%) | 299 (91.2%) | 292 (91.0%) | 0.931 |
| Neurosurgery, n (%) | 259 (39.9%) | 129 (39.3%) | 130 (40.5%) | 0.761 |
| Length of ICU stay (days) | 5.7 (2.4–12.1) | 3.8 (1.9–8.4) | 7.3 (3.8–14.7) | <0.001 |
| Length of hospital stay (days) | 10.1 (4.9–18.5) | 7.9 (4.0–15.7) | 12.4 (6.2–23.0) | <0.001 |
| 30-day mortality, n (%) | 191 (29.4%) | 95 (29.0%) | 96 (29.9%) | 0.792 |
| Classification Models | AUC (95% CI) | Accuracy | Sensitivity | Specificity | PPV | NPV | F1 Score |
|---|---|---|---|---|---|---|---|
| XGBoost | 0.989 (0.983–0.995) | 0.952 | 0.947 | 0.960 | 0.959 | 0.946 | 0.953 |
| Light GBM | 0.710 (0.669–0.752) | 0.675 | 0.676 | 0.682 | 0.681 | 0.677 | 0.674 |
| Random Forest | 1.000 | 0.998 | 1.000 | 1.000 | 1.000 | 0.997 | 1.000 |
| AdaBoost | 0.815 (0.782–0.849) | 0.736 | 0.724 | 0.752 | 0.742 | 0.736 | 0.731 |
| CNB | 0.618 (0.572–0.663) | 0.592 | 0.694 | 0.495 | 0.574 | 0.624 | 0.626 |
| SVM | 0.509 (0.462–0.556) | 0.538 | 0.253 | 0.822 | 0.629 | 0.534 | 0.305 |
| Classification Models | AUC (95% CI) | Accuracy | Sensitivity | Specificity | PPV | NPV | F1 Score |
|---|---|---|---|---|---|---|---|
| XGBoost | 0.620 (0.483–0.757) | 0.581 | 0.654 | 0.622 | 0.574 | 0.589 | 0.597 |
| Light GBM | 0.534 (0.395–0.673) | 0.527 | 0.436 | 0.727 | 0.534 | 0.517 | 0.448 |
| Random Forest | 0.652 (0.517–0.786) | 0.542 | 0.719 | 0.579 | 0.767 | 0.526 | 0.716 |
| AdaBoost | 0.631 (0.493–0.768) | 0.599 | 0.594 | 0.714 | 0.606 | 0.596 | 0.587 |
| CNB | 0.589 (0.448–0.730) | 0.567 | 0.577 | 0.668 | 0.555 | 0.584 | 0.547 |
| SVM | 0.513 (0.371–0.654) | 0.524 | 0.607 | 0.563 | 0.619 | 0.523 | 0.541 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, R.; Cai, L.; Zhang, J.; He, M.; Xu, J. Prediction of Acute Respiratory Distress Syndrome in Traumatic Brain Injury Patients Based on Machine Learning Algorithms. Medicina 2023, 59, 171. https://doi.org/10.3390/medicina59010171
Wang R, Cai L, Zhang J, He M, Xu J. Prediction of Acute Respiratory Distress Syndrome in Traumatic Brain Injury Patients Based on Machine Learning Algorithms. Medicina. 2023; 59(1):171. https://doi.org/10.3390/medicina59010171
Chicago/Turabian StyleWang, Ruoran, Linrui Cai, Jing Zhang, Min He, and Jianguo Xu. 2023. "Prediction of Acute Respiratory Distress Syndrome in Traumatic Brain Injury Patients Based on Machine Learning Algorithms" Medicina 59, no. 1: 171. https://doi.org/10.3390/medicina59010171
APA StyleWang, R., Cai, L., Zhang, J., He, M., & Xu, J. (2023). Prediction of Acute Respiratory Distress Syndrome in Traumatic Brain Injury Patients Based on Machine Learning Algorithms. Medicina, 59(1), 171. https://doi.org/10.3390/medicina59010171