

Pregnancy and Lactation-Associated Osteoporosis Successfully Treated with Romosozumab: A Case Report

 , , ,
, , ,
Abstract
:1. Introduction
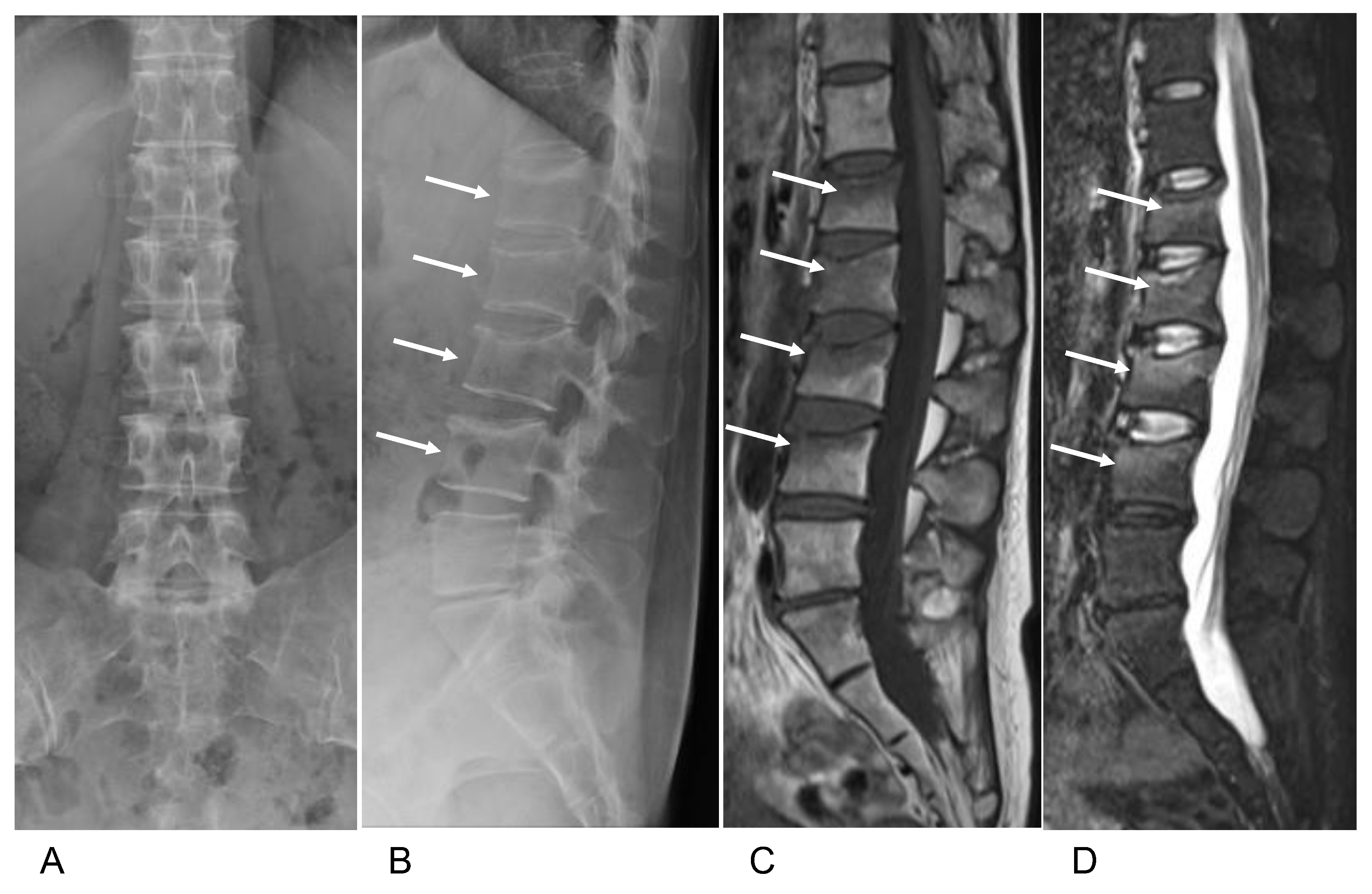
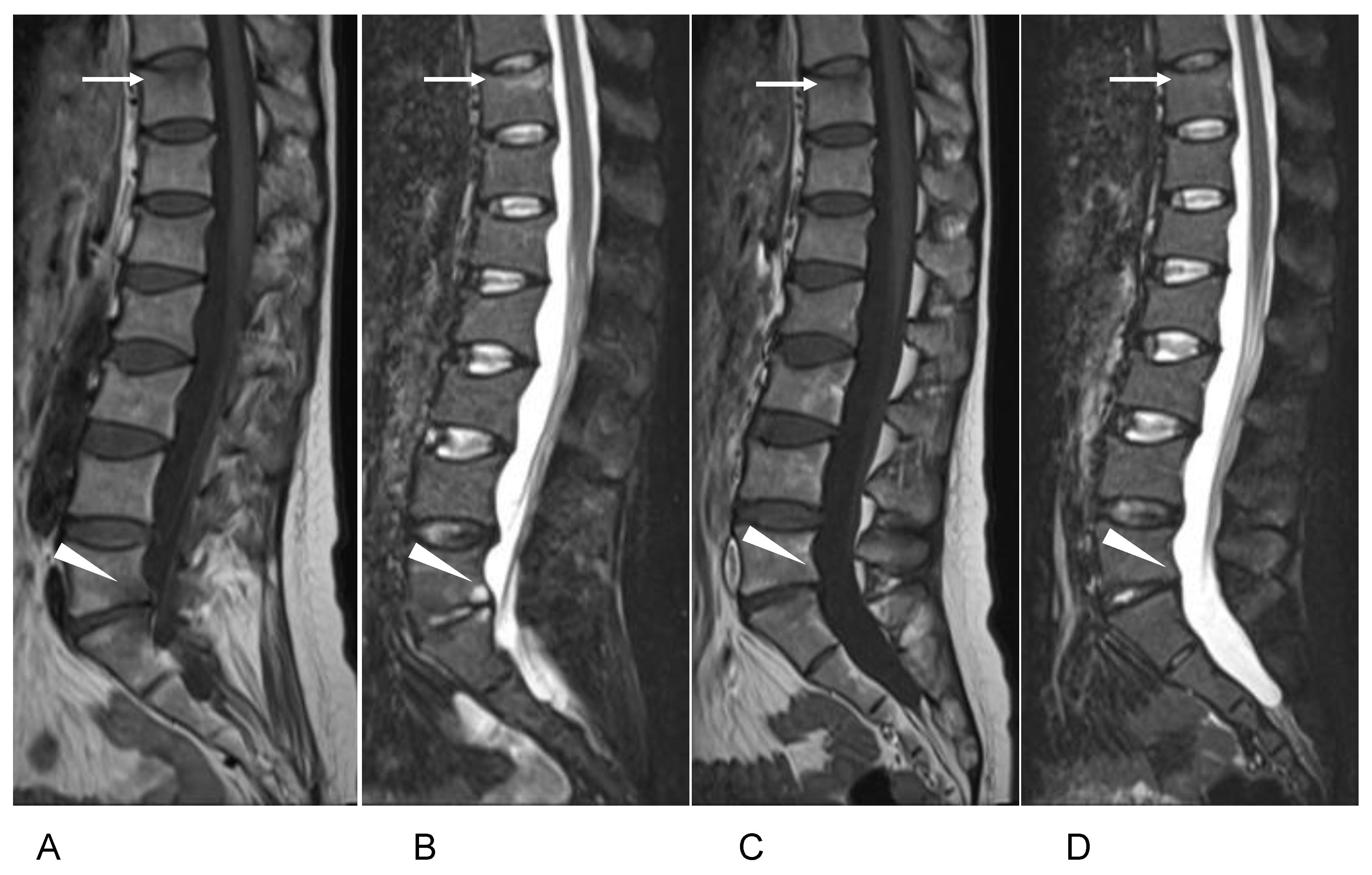
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kovacs, C.; Ralston, S. Presentation and management of osteoporosis presenting in association with pregnancy or lactation. Osteoporos. Int. 2015, 26, 2223–2241. [Google Scholar] [CrossRef] [PubMed]
- Laroche, M.; Talibart, M.; Cormier, C.; Roux, C.; Guggenbuhl, P.; Degboe, Y. Pregnancy-related fractures: A retrospective study of a French cohort of 52 patients and review of the literature. Osteoporos. Int. 2017, 28, 3135–3142. [Google Scholar] [CrossRef]
- Mäkitie, O.; Zillikens, M. Early-onset osteoporosis. Calcif. Tissue Int. 2022, 110, 546–561. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, J.; Gao, P.; Lv, F.; Song, Y.; Chang, X.; Zhao, D.; Wang, O.; Jiang, Y.; Xing, X.; et al. Clinical characteristics and bisphosphonates treatment of rare pregnancy- and lactation-associated osteoporosis. Clin. Rheumatol. 2018, 37, 3141–3150. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, S.; Grey, A.; Singh, R.; Reid, I. Bisphosphonates in pregnancy and lactation-associated osteoporosis. Osteoporos. Int. 2006, 17, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Zarattini, G.; Buffoli, P.; Isabelli, G.; Marchese, M. Pregnancy-associated osteoporosis with seven vertebral compression fractures, a case treated with strontium ranelate. Clin. Cases Miner. Bone Metab. 2014, 11, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Tanriover, M.; Oz, S.; Sozen, T.; Kilicarslan, A.; Guven, G. Pregnancy- and lactation-associated osteoporosis with severe vertebral deformities: Can strontium ranelate be a new alternative for the treatment? Spine J. 2009, 9, e20–e24. [Google Scholar] [CrossRef]
- Stumpf, U.; Kraus, M.; Hadji, P. Influence of denosumab on bone mineral density in a severe case of pregnancy-associated osteoporosis. Osteoporos. Int. 2021, 32, 2383–2387. [Google Scholar] [CrossRef]
- Ijuin, A.; Yoshikawa, H.; Asano, R.; Tsuburai, T.; Kikuchi, R.; Sakakibara, H. Teriparatide and denosumab treatment for pregnancy and lactation-associated osteoporosis with multiple vertebral fractures: A case study. Taiwan J. Obstet. Gynecol. 2017, 56, 863–866. [Google Scholar] [CrossRef]
- Palot, S.; Evranos, B.; Aydin, C.; Cuhaci, N.; Ersoy, R.; Cakir, B. Effective treatment of severe pregnancy and lactation-related osteoporosis with teriparatide: Case report and review of the literature. Gynecol. Endocrinol. 2015, 31, 522–525. [Google Scholar] [CrossRef]
- Lampropoulou-Adamidou, K.; Trovas, G.; Triantafyllopoulos, I.; Yavropoulou, M.; Anastasilakis, A.; Anagnostis, P.; Toulis, K.; Makris, K.; Gazi, S.; Balanika, A.; et al. Teriparatide treatment in patients with pregnancy- and lactation-associated osteoporosis. Calcif. Tissue Int. 2021, 109, 554–562. [Google Scholar] [CrossRef]
- Lee, S.; Hong, M.; Park, S.; Park, H.; Kim, J.; Ahn, J. A case of teriparatide on pregnancy-induced osteoporosis. J. Bone Metab. 2013, 20, 111–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosman, F.; Crittenden, D.; Adachi, J.; Binkley, N.; Czerwinski, E.; Ferrari, S.; Hofbauer, L.; Lau, E.; Lewiecki, E.; Miyauchi, A.; et al. Romosozumab treatment in postmenopausal women with osteoporosis. N. Engl. J. Med. 2016, 375, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.; Petersen, J.; Brandi, M.; Karaplis, A.; Lorentzon, M.; Thomas, T.; Maddox, J.; Fan, M.; Meisner, P.; Grauer, A. Romosozumab or alendronate for fracture prevention in women with osteoporosis. N. Engl. J. Med. 2017, 377, 1417–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordin, B.; Roper, A. Post-pregnancy osteoporosis; a syndrome? Lancet 1955, 268, 431–434. [Google Scholar] [CrossRef]
- Hadji, P.; Boekhoff, J.; Hahn, M.; Hellmeyer, L.; Hars, O.; Kyvernitakis, I. Pregnancy-associated osteoporosis: A case-control study. Osteoporos. Int. 2017, 28, 1393–1999. [Google Scholar] [CrossRef]
- Qian, Y.; Wang, L.; Yu, L.; Huang, W. Pregnancy- and lactation-associated osteoporosis with vertebral fractures: A systematic review. BMC Musculoskelet. Disord. 2021, 22, 926. [Google Scholar] [CrossRef]
- Ofluoglu, O.; Ofluoglu, D. A case report: Pregnancy-induced severe osteoporosis with eight vertebral fractures. Rheumatol. Int. 2008, 29, 197–201. [Google Scholar] [CrossRef]
- Møller, U.; Streym, S.; Mosekilde, L.; Rejnmark, L. Changes in bone mineral density and body composition during pregnancy and postpartum. A controlled cohort study. Osteoporos. Int. 2012, 23, 1213–1223. [Google Scholar] [CrossRef]
- Uemura, H.; Yasui, T.; Kiyokawa, M.; Kuwahara, A.; Ikawa, H.; Matsuzaki, T.; Maegawa, M.; Furumoto, H.; Irahara, M. Serum osteoprotegerin/osteoclastogenesis-inhibitory factor during pregnancy and lactation and the relationship with calcium-regulating hormones and bone turnover markers. J. Endocrinol. 2002, 174, 353–359. [Google Scholar] [CrossRef]
- Cohen, A.; Kamanda-Kosseh, M.; Dempster, D.; Zhou, H.; Müller, R.; Goff, E.; Colon, I.; Bucovsky, M.; Stubby, J.; Nickolas, T.; et al. Women with pregnancy and lactation-associated osteoporosis (PLO) have low bone remodeling rates at the tissue level. J. Bone Miner. Res. 2019, 34, 1552–1561. [Google Scholar] [CrossRef] [PubMed]
- Campos-Obando, N.; Oei, L.; Hoefsloot, L.; Kiewiet, R.; Klaver, C.; Simon, M.; Zillikens, M. Osteoporotic vertebral fractures during pregnancy: Be aware of a potential underlying genetic cause. J. Clin. Endocrinol. Metab. 2014, 99, 1107–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, N.; Kim, J.; Lee, S.; Kim, S.; Rhee, Y. Changes in bone mineral density and bone turnover markers during treatment with teriparatide in pregnancy- and lactation-associated osteoporosis. Clin. Endocrinol. 2018, 88, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Hassen-Zrour, S.; Korbâa, W.; Béjia, I.; Saidani, Z.; Bergaoui, N. Maternal and fetal outcome after long-term bisphosphonate exposure before conception. Osteoporos. Int. 2010, 21, 709–710. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Wajnberg, R.; Diav-Citrin, O. The outcome of pregnancy following pre-pregnancy or early pregnancy alendronate treatment. Reprod. Toxicol. 2006, 22, 578–579. [Google Scholar] [CrossRef]
- Losada, I.; Sartori, L.; Di Gianantonio, E.; Zen, M.; Clementi, M.; Doria, A. Bisphosphonates in patients with autoimmune rheumatic diseases: Can they be used in women of childbearing age? Autoimmun. Rev. 2010, 9, 547–552. [Google Scholar] [CrossRef]
- Bonnelye, E.; Chabadel, A.; Saltel, F.; Jurdic, P. Dual effect of strontium ranelate: Stimulation of osteoblast differentiation and inhibition of osteoclast formation and resorption in vitro. Bone 2008, 42, 129–138. [Google Scholar] [CrossRef]
- Silverman, S.; Christiansen, C. Individualizing osteoporosis therapy. Osteoporos. Int. 2012, 23, 797–809. [Google Scholar] [CrossRef]
- Cerit, E.; Cerit, M. A case of pregnancy and lactation associated osteoporosis in the third pregnancy; robust response to teriparatide despite delayed administration. Bone Rep. 2020, 13, 100706. [Google Scholar] [CrossRef]
- Choe, E.; Song, J.; Park, K.; Seok, H.; Lee, E.; Lim, S.; Rhee, Y. Effect of teriparatide on pregnancy and lactation-associated osteoporosis with multiple vertebral fractures. J. Bone Miner. Metab. 2012, 30, 596–601. [Google Scholar] [CrossRef]
- Hellmeyer, L.; Boekhoff, J.; Hadji, P. Treatment with teriparatide in a patient with pregnancy-associated osteoporosis. Gynecol. Endocrinol. 2010, 26, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Fujita, R.; Endo, T.; Takahata, M.; Haraya, K.; Suzuki, H.; Oda, I.; Kanayama, M.; Asano, T.; Shigenobu, K.; Iwata, A.; et al. Real-world persistence of twice-weekly teriparatide and factors associated with the discontinuation in patients with osteoporosis. J. Bone Miner. Metab. 2022, 40, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Usui, T.; Funagoshi, M.; Seto, K.; Ide, K.; Tanaka, S.; Kawakami, K. Persistence of and switches from teriparatide treatment among women and men with osteoporosis in the real world: A claims database analysis. Arch. Osteoporos. 2018, 13, 54. [Google Scholar] [CrossRef] [PubMed]
- McClung, M.; Grauer, A.; Boonen, S.; Bolognese, M.; Brown, J.; Diez-Perez, A.; Langdahl, B.; Reginster, J.; Zanchetta, J.; Wasserman, S.; et al. Romosozumab in postmenopausal women with low bone mineral density. N. Engl. J. Med. 2014, 370, 412–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inose, H.; Ariga, A.; Motoyoshi, T.; Fukushima, K.; Tomizawa, S.; Kato, T.; Takahashi, K.; Yoshii, T.; Okawa, A. The real-world effect of 12 months of romosozumab treatment on patients with osteoporosis with a high risk of fracture and factors predicting the rate of bone mass increase: A multicenter retrospective study. JBMR Plus. 2022, 6, e10637. [Google Scholar] [CrossRef]
- Ebina, K.; Tsuboi, H.; Nagayama, Y.; Kashii, M.; Kaneshiro, S.; Miyama, A.; Nakaya, H.; Kunugiza, Y.; Hirao, M.; Okamura, G.; et al. Effects of prior osteoporosis treatment on 12-month treatment response of romosozumab in patients with postmenopausal osteoporosis. Joint Bone Spine 2021, 88, 105219. [Google Scholar] [CrossRef]
- Kobayakawa, T.; Suzuki, T.; Nakano, M.; Saito, M.; Miyazaki, A.; Takahashi, J.; Nakamura, Y. Real-world effects and adverse events of romosozumab in Japanese osteoporotic patients: A prospective cohort study. Bone Rep. 2021, 14, 101068. [Google Scholar] [CrossRef]
- Tominaga, A.; Wada, K.; Okazaki, K.; Nishi, H.; Terayama, Y.; Kodama, Y.; Kato, Y. Effect of the duration of previous osteoporosis treatment on the effect of romosozumab treatment. Osteoporos. Int. 2022, 33, 1265–1273. [Google Scholar] [CrossRef]
- Chang, B.; Quan, Q.; Li, Y.; Qiu, H.; Peng, J.; Gu, Y. Treatment of osteoporosis, with a focus on 2 monoclonal antibodies. Med Sci Monit. 2018, 24, 8758–8766. [Google Scholar] [CrossRef]
- Leder, B.; Tsai, J.; Uihlein, A.; Wallace, P.; Lee, H.; Neer, R.; Burnett-Bowie, S. Denosumab and teriparatide transitions in postmenopausal osteoporosis (the DATA-Switch study): Extension of a randomised controlled trial. Lancet 2015, 386, 1147–1155. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Value | Normal Range | Before Treatment | Before Romosozumab | After 2 mo | After 6 mo | After 12 mo |
|---|---|---|---|---|---|---|
| TRACP-5b, mU/dL | 120–420 | 476 | 348 | 158 | 96 | 67 |
| Total PⅠNP, ng/mL | 16.8–98.2 | 76.1 | 113 | 71.4 | 30.7 | 26.0 |
| Before Treatment | Before Romo- Sozumab * | 2 mo | 4 mo | 6 mo | 8 mo | 12 mo | BMD Change at 12 mo vs. Baseline | |
|---|---|---|---|---|---|---|---|---|
| Lumbar spine (L1–4): | ||||||||
| BMD, g/cm2 | 0.852 | 0.842 | 0.879 | 0.920 | 0.978 | 1.019 | 1.053 | 23.6% |
| Z score | −2.1 | −2.2 | −1.9 | −1.6 | −1.1 | −0.8 | −0.5 | |
| Femoral neck: | ||||||||
| BMD, g/cm2 | 0.710 | 0.723 | 0.731 | 0.711 | 0.741 | 0.774 | 0.754 | 6.2% |
| Z score | −1.5 | −1.3 | −1.3 | −1.5 | −1.2 | −1.1 | −1.2 | |
| Total hip: | ||||||||
| BMD, g/cm2 | 0.726 | 0.721 | 0.770 | 0.788 | 0.795 | 0.797 | 0.807 | 11.2% |
| Z score | −1.7 | −1.7 | −1.3 | −1.2 | −1.1 | −1.1 | −1.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaneuchi, Y.; Iwabuchi, M.; Hakozaki, M.; Yamada, H.; Konno, S.-i. Pregnancy and Lactation-Associated Osteoporosis Successfully Treated with Romosozumab: A Case Report. Medicina 2023, 59, 19. https://doi.org/10.3390/medicina59010019
Kaneuchi Y, Iwabuchi M, Hakozaki M, Yamada H, Konno S-i. Pregnancy and Lactation-Associated Osteoporosis Successfully Treated with Romosozumab: A Case Report. Medicina. 2023; 59(1):19. https://doi.org/10.3390/medicina59010019
Chicago/Turabian StyleKaneuchi, Yoichi, Masumi Iwabuchi, Michiyuki Hakozaki, Hitoshi Yamada, and Shin-ichi Konno. 2023. "Pregnancy and Lactation-Associated Osteoporosis Successfully Treated with Romosozumab: A Case Report" Medicina 59, no. 1: 19. https://doi.org/10.3390/medicina59010019
APA StyleKaneuchi, Y., Iwabuchi, M., Hakozaki, M., Yamada, H., & Konno, S. -i. (2023). Pregnancy and Lactation-Associated Osteoporosis Successfully Treated with Romosozumab: A Case Report. Medicina, 59(1), 19. https://doi.org/10.3390/medicina59010019