
Validation of a New Prognostic Score in Patients with Ovarian Adenocarcinoma

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. Statistical Analysis
3. Results
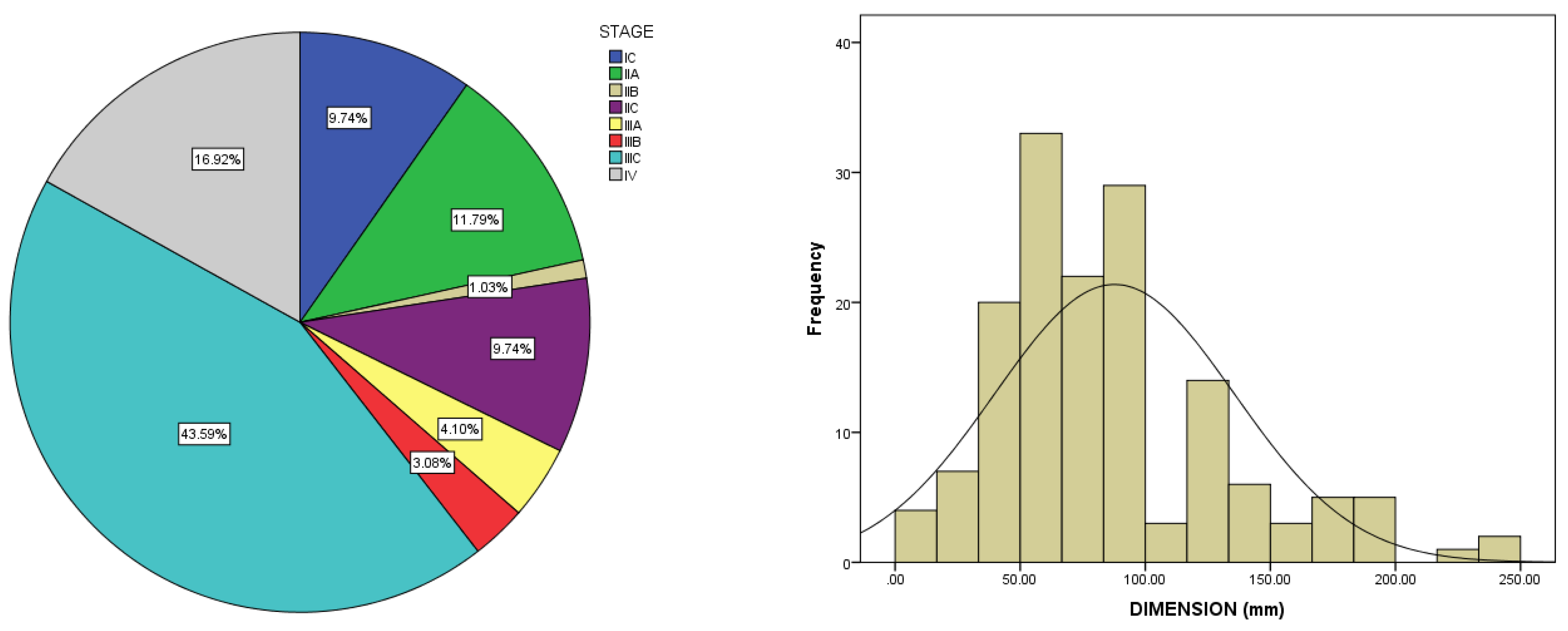
3.1. Baseline Characteristics
Oncologic Outcome and Prognostic Factors
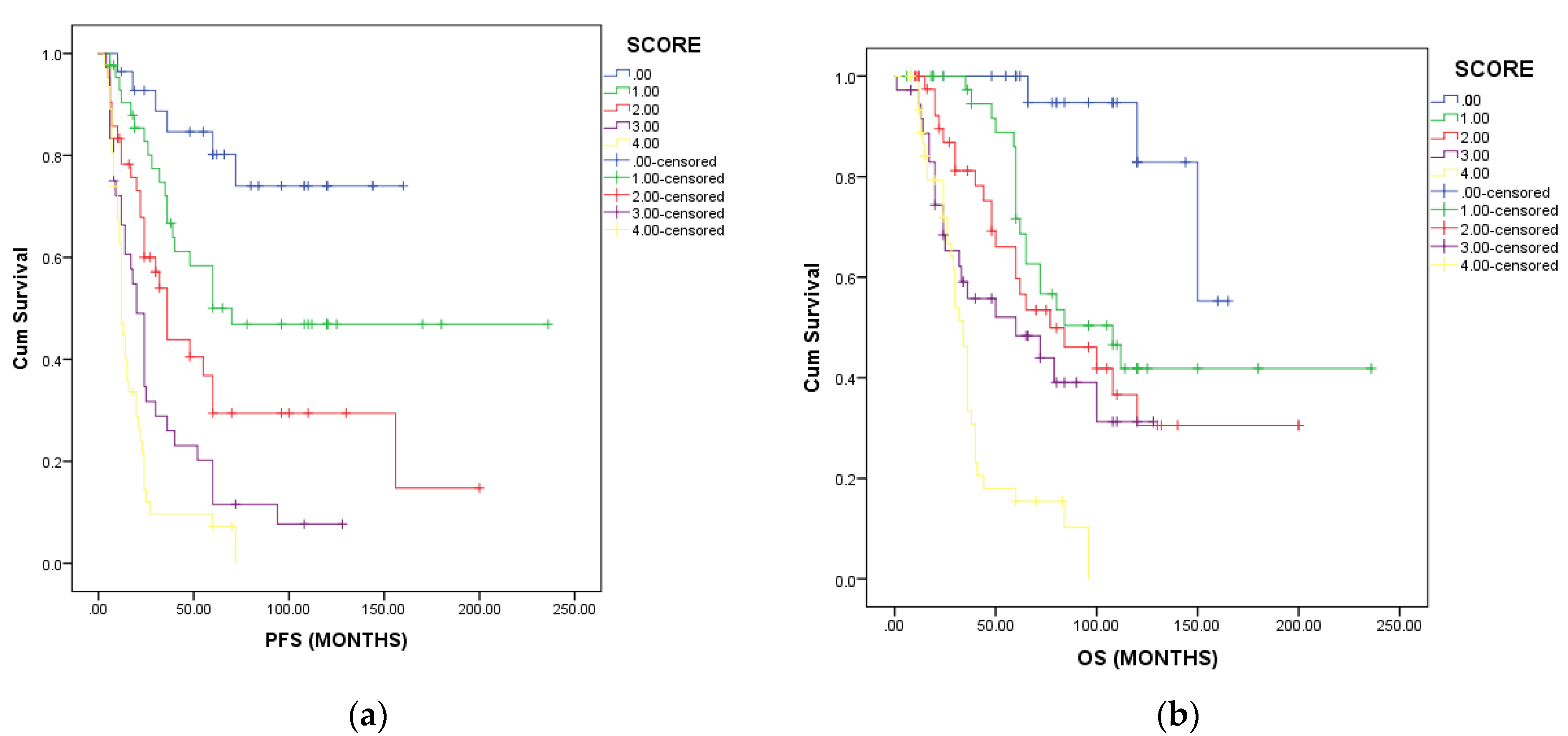
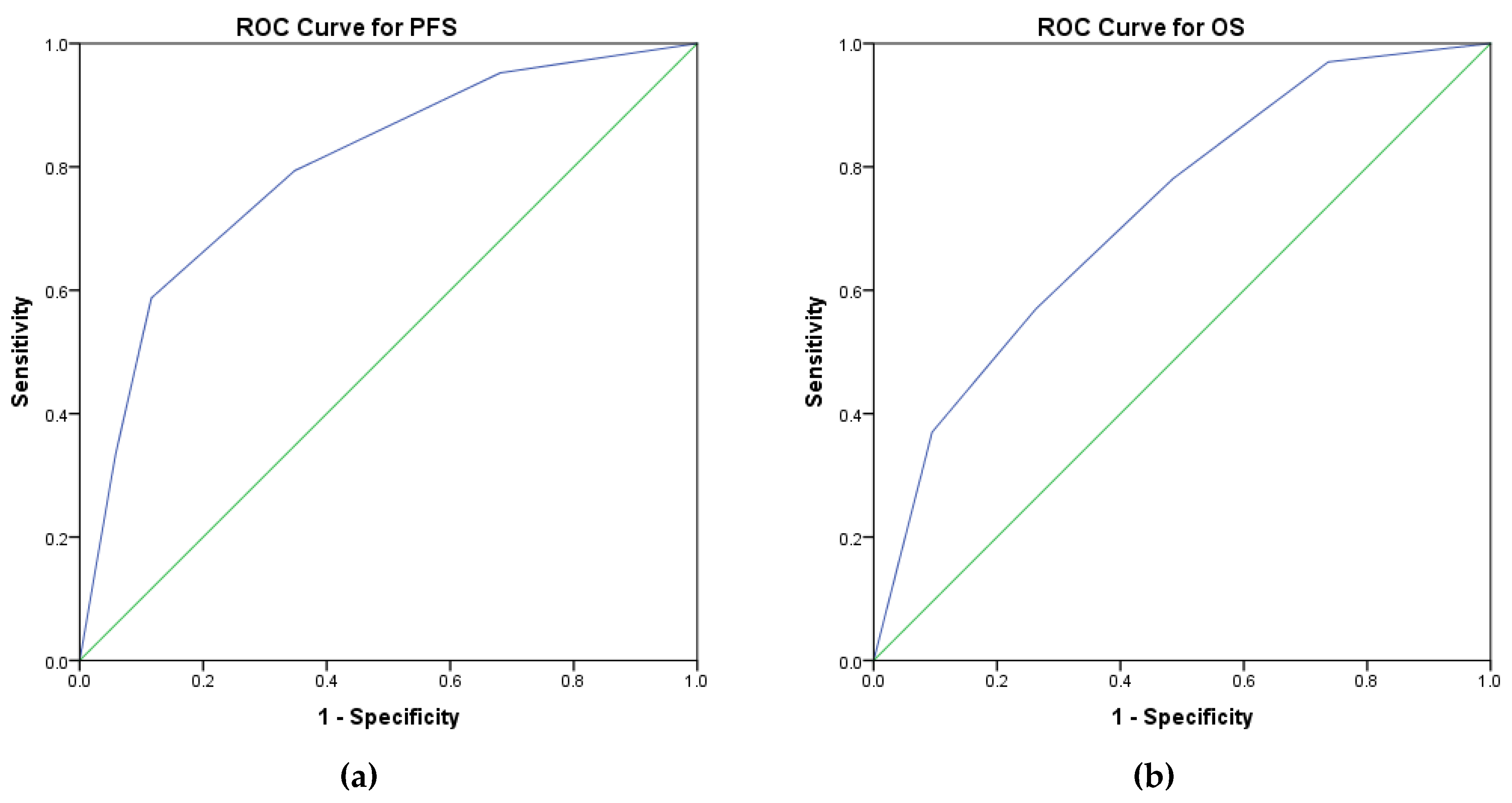
3.2. Prognostic Score
- performance status ECOG ≥ 1,
- presence of ascites,
- menopausal status,
- residual disease after surgery,
- presence of thrombocytosis.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cannistra, S.A. Cancer of the Ovary. N. Engl. J. Med. 2004, 351, 2519–2529. [Google Scholar] [CrossRef]
- Trifanescu, O.G.; Gales, L.N.; Serbanescu, G.L.; Zgura, A.F.; Iliescu, L.; Mehedintu, C.; Anghel, R.M. Long-Term Oncological Outcome in Patients with Cervical Cancer after 3 Trimodality Treatment (Radiotherapy, Platinum-Based Chemotherapy, and Robotic Surgery). Medicine 2021, 100, e25271. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Bristow, R.E.; Tomacruz, R.S.; Armstrong, D.K.; Trimble, E.L.; Montz, F.J. Survival Effect of Maximal Cytoreductive Surgery for Advanced Ovarian Carcinoma during the Platinum Era: A Meta-Analysis; Centre for Reviews and Dissemination: York, UK, 2002. [Google Scholar]
- Trifanescu, O.G.; Gales, L.N.; Tanase, B.C.; Marinescu, S.A.; Trifanescu, R.A.; Gruia, I.M.; Paun, M.A.; Rebegea, L.; Mitrica, R.; Serbanescu, L.; et al. Prognostic Role of Vascular Endothelial Growth Factor and Correlation with Oxidative Stress Markers in Locally Advanced and Metastatic Ovarian Cancer Patients. Diagnostics 2023, 13, 166. [Google Scholar] [CrossRef] [PubMed]
- du Bois, A. A Randomized Clinical Trial of Cisplatin/Paclitaxel Versus Carboplatin/Paclitaxel as First-Line Treatment of Ovarian Cancer. Cancer Spectrum Knowl. Environ. 2003, 95, 1320–1329. [Google Scholar] [CrossRef] [PubMed]
- Pfisterer, J.; Weber, B.; Reuss, A.; Kimmig, R.; du Bois, A.; Wagner, U.; Bourgeois, H.; Meier, W.; Costa, S.; Blohmer, J.-U.; et al. Randomized Phase III Trial of Topotecan Following Carboplatin and Paclitaxel in First-Line Treatment of Advanced Ovarian Cancer: A Gynecologic Cancer Intergroup Trial of the AGO-OVAR and GINECO. JNCI J. Natl. Cancer Inst. 2006, 98, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- du Bois, A.; Weber, B.; Rochon, J.; Meier, W.; Goupil, A.; Olbricht, S.; Barats, J.-C.; Kuhn, W.; Orfeuvre, H.; Wagner, U.; et al. Addition of Epirubicin As a Third Drug to Carboplatin-Paclitaxel in First-Line Treatment of Advanced Ovarian Cancer: A Prospectively Randomized Gynecologic Cancer Intergroup Trial by the Arbeitsgemeinschaft Gynaekologische Onkologie Ovarian Cancer Study Group and the Groupe d’Investigateurs Nationaux Pour l’Etude Des Cancers Ovariens. J. Clin. Oncol. 2016, 24, 1127–1135. [Google Scholar] [CrossRef]
- Winter, W.E., III; Maxwell, G.L.; Tian, C.; Carlson, J.W.; Ozols, R.F.; Rose, P.G.; Markman, M.; Armstrong, D.K.; Muggia, F.; McGuire, W.P. Prognostic Factors for Stage III Epithelial Ovarian Cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2007, 25, 3621–3627. [Google Scholar] [CrossRef]
- Rampersad, A.C.; Wang, Y.; Smith, E.R.; Xu, X.-X. Menopause and Ovarian Cancer Risk: Mechanisms and Experimental Support. Am. J. Clin. Exp. Obstet. Gynecol. 2015, 2, 14–23. [Google Scholar]
- Riman, T.; Nilsson, S.; Persson, I.R. Review of Epidemiological Evidence for Reproductive and Hormonal Factors in Relation to the Risk of Epithelial Ovarian Malignancies. Acta Obstet. Gynecol. Scand. 2004, 83, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Trifanescu, O.G.; Gales, L.N.; Trifanescu, R.A.; Anghel, R.M. Clinical Prognostic Factors in pre- and Post-Menopausal Women with Ovarian Carcinoma . Acta Endocrinol. 2018, 14, 353–359. [Google Scholar] [CrossRef]
- Jung, E.J.; Eom, H.M.; Byun, J.M.; Kim, Y.N.; Lee, K.B.; Sung, M.S.; Kim, K.T.; Jeong, D.H. Different Features of the Histopathological Subtypes of Ovarian Tumors in Pre- and Postmenopausal Women. Menopause 2017, 24, 1028. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupaimoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic Thrombocytosis in Ovarian Cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.-P.; Huang, Q.-D.; Wan, T.; Tu, H.; Gu, H.-F.; Cao, J.-Y.; Liu, J.-H. Combined Score of Pretreatment Platelet Count and CA125 Level (PLT-CA125) Stratified Prognosis in Patients with FIGO Stage IV Epithelial Ovarian Cancer. J. Ovarian Res. 2019, 12, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, D.; Balega, J.; Sundar, S.; Kehoe, S.; Elattar, A.; Phillips, A.; Singh, K. Serum Albumin as a Predictor of Survival after Interval Debulking Surgery for Advanced Ovarian Cancer (AOC): A Retrospective Study. J. Investig. Surg. 2022, 35, 426–431. [Google Scholar] [CrossRef]
- Sørensen, S.M.; Schnack, T.H.; Høgdall, C. Impact of Residual Disease on Overall Survival in Women with Federation of Gynecology and Obstetrics Stage IIIB-IIIC vs Stage IV Epithelial Ovarian Cancer after Primary Surgery. Acta Obstet. Gynecol. Scand. 2019, 98, 34–43. [Google Scholar] [CrossRef]
- Ataseven, B.; Grimm, C.; Harter, P.; Heitz, F.; Traut, A.; Prader, S.; du Bois, A. Prognostic Impact of Debulking Surgery and Residual Tumor in Patients with Epithelial Ovarian Cancer FIGO Stage IV. Gynecol. Oncol. 2016, 140, 215–220. [Google Scholar] [CrossRef]
- Cohen, P.A.; Powell, A.; Böhm, S.; Gilks, C.B.; Stewart, C.J.R.; Meniawy, T.M.; Bulsara, M.; Avril, S.; Brockbank, E.C.; Bosse, T.; et al. Pathological Chemotherapy Response Score Is Prognostic in Tubo-Ovarian High-Grade Serous Carcinoma: A Systematic Review and Meta-Analysis of Individual Patient Data. Gynecol. Oncol. 2019, 154, 441–448. [Google Scholar] [CrossRef] [Green Version]
- Santoro, A.; Angelico, G.; Piermattei, A.; Inzani, F.; Valente, M.; Arciuolo, D.; Spadola, S.; Mulè, A.; Zorzato, P.; Fagotti, A.; et al. Pathological Chemotherapy Response Score in Patients Affected by High Grade Serous Ovarian Carcinoma: The Prognostic Role of Omental and Ovarian Residual Disease. Front. Oncol. 2019, 9, 778. [Google Scholar] [CrossRef] [Green Version]
- Jónsdóttir, B.; Lomnytska, M.; Poromaa, I.S.; Silins, I.; Stålberg, K. The Peritoneal Cancer Index Is a Strong Predictor of Incomplete Cytoreductive Surgery in Ovarian Cancer. Ann. Surg. Oncol. 2021, 28, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Engbersen, M.P.; Lahaye, M.J.; Lok, C.A.R.; Koole, S.N.; Sonke, G.S.; Beets-Tan, R.G.H.; Van Driel, W.J. Peroperative Scoring Systems for Predicting the Outcome of Cytoreductive Surgery in Advanced-Stage Ovarian Cancer—A Systematic Review. Eur. J. Surg. Oncol. 2021, 47, 1856–1861. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.-N.; Wang, F. Prognostic Significance of Preoperative Serum Albumin in Epithelial Ovarian Cancer Patients: A Systematic Review and Dose–Response Meta-Analysis of Observational Studies. Cancer Manag. Res. 2018, 10, 815–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moorman, P.G.; Calingaert, B.; Palmieri, R.T.; Iversen, E.S.; Bentley, R.C.; Halabi, S.; Berchuck, A.; Schildkraut, J.M. Hormonal Risk Factors for Ovarian Cancer in Premenopausal and Postmenopausal Women. Am. J. Epidemiol. 2008, 167, 1059–1069. [Google Scholar] [CrossRef] [Green Version]
- Wentzensen, N.; Poole, E.M.; Trabert, B.; White, E.; Arslan, A.A.; Patel, A.V.; Setiawan, V.W.; Visvanathan, K.; Weiderpass, E.; Adami, H.-O.; et al. Ovarian Cancer Risk Factors by Histologic Subtype: An Analysis from the Ovarian Cancer Cohort Consortium. J. Clin. Oncol. 2016, 34, 2888–2898. [Google Scholar] [CrossRef]
- Hu, J.; Jiao, X.; Zhu, L.; Guo, H.; Wu, Y. Establishment and Verification of the Nomogram That Predicts the 3-Year Recurrence Risk of Epithelial Ovarian Carcinoma. BMC Cancer 2020, 20, 938. [Google Scholar] [CrossRef]
- Yu, L.; Deng, L.; Li, J.; Zhang, Y.; Hu, L. The Prognostic Value of Vascular Endothelial Growth Factor in Ovarian Cancer: A Systematic Review and Meta-Analysis. Gynecol. Oncol. 2013, 128, 391–396. [Google Scholar] [CrossRef]
- Didžiapetrienė, J.; Bublevič, J.; Smailytė, G.; Kazbarienė, B.; Stukas, R. Significance of Blood Serum Catalase Activity and Malondialdehyde Level for Survival Prognosis of Ovarian Cancer Patients. Medicina 2014, 50, 204–208. [Google Scholar] [CrossRef]
- Komatsu, H.; Oishi, T.; Itamochi, H.; Shimada, M.; Sato, S.; Chikumi, J.; Sato, S.; Nonaka, M.; Sawada, M.; Wakahara, M.; et al. Serum Vascular Endothelial Growth Factor-A as a Prognostic Biomarker for Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2017, 27, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Trifanescu, O.; Gruia, M.I.; Gales, L.; Trifanescu, R.; Pascu, A.M.; Poroch, V.; Toma, S.; Poiana, C.; Anghel, R. Malondialdehyde as a Prognostic Marker in Patients with Ovarian Adenocarcinoma. Rev. Chim. 2019, 70, 2561–2565. [Google Scholar] [CrossRef]
- Armbrust, R.; Richter, R.; Woopen, H.; Hilpert, F.; Harter, P.; Sehouli, J. Impact of Health-Related Quality of Life (HRQoL) on Short-Term Mortality in Patients with Recurrent Ovarian, Fallopian or Peritoneal Carcinoma (the NOGGO-AGO QoL Prognosis-Score-Study): Results of a Meta-Analysis in 2209 Patients. ESMO Open 2021, 6, 100081. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.-Y.; Tai, Y.-J.; Chen, Y.-L.; Chiang, Y.-C.; Hsu, H.-C.; Cheng, W.-F. Ovarian Cancer Risk Score Predicts Chemo-Response and Outcome in Epithelial Ovarian Carcinoma Patients. J. Gynecol. Oncol. 2020, 32, e18. [Google Scholar] [CrossRef] [PubMed]
- Millstein, J.; Budden, T.; Goode, E.L.; Anglesio, M.S.; Talhouk, A.; Intermaggio, M.P.; Leong, H.S.; Chen, S.; Elatre, W.; Gilks, B.; et al. Prognostic Gene Expression Signature for High-Grade Serous Ovarian Cancer. Ann. Oncol. 2020, 31, 1240–1250. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PFS | OS | |||
|---|---|---|---|---|
| Characteristics | Median PFS (Months) | p | Median OS (Months) | p |
| Eastern Cooperative Oncology Group (ECOG) | ||||
| ECOG 0 | 60 | 112 | ||
| ECOG 1 | 20 | 0.002 | 40 | 0.0001 |
| ECOG 2 | 10 | 0.001 | 30 | 0.0001 |
| Menopause | ||||
| No | 60 | 150 | ||
| Yes | 24 | 0.001 | 60 | 0.005 |
| Residual disease | ||||
| Yes | 15 | 38 | ||
| No | 156 | <0.0001 | NR | 0.0003 |
| R1 cm | ||||
| 0 | 156 | NR | ||
| 0–1 cm | 20 | <0.0001 | 60 | 0.0002 |
| More 1 cm | 12 | <0.0001 | 34 | 0.0001 |
| G | ||||
| G2 | 72 | 150 | ||
| G3 | 21 | <0.0001 | 50 | 0.0001 |
| Histopathology (HP) | ||||
| Serous | 24 | 0.002 | 62 | NS |
| Mucinous | 60 | NS | 72 | |
| Endometrioid | 70 | NS | 110 | |
| Clear Cell | 30 | NS | NR | |
| Ascites | ||||
| Yes | 22 | 44 | ||
| No | 48 | 0.027 | 120 | 0.005 |
| Thrombocytosis | ||||
| Yes | 60 | 36 | ||
| No | 20 | 0.0001 | 152 | 0.0001 |
| PFS | OS | |||||
|---|---|---|---|---|---|---|
| Characteristics | HR | PFS 95%CI | p | HR | OS 95%CI | p |
| ECOG | ||||||
| ECOG 0 | 1 | 1 | ||||
| ECOG 1, 2 | 2.71 | 1.96–3.73 | 0.001 | 3.19 | 2.20–4.64 | 0.001 |
| Thrombocytosis | ||||||
| No | 1 | 1 | ||||
| Yes | 2.48 | 1.72–3.58 | 0.0001 | 3.33 | 2.16–5.13 | 0.0001 |
| Menopause | ||||||
| No | 1 | 1 | ||||
| Yes | 2.02 | 1.35–3.01 | 0.001 | 2.25 | 1.41–3.59 | 0001 |
| R0 | ||||||
| Yes | 1 | 1 | ||||
| No | 5.12 | 3.43–7.65 | 0.0001 | 4.07 | 2.59–6.39 | 0.0001 |
| G | ||||||
| G2 | 1 | 1 | ||||
| G3 | 2.50 | 1.77–3.53 | 0.001 | 2.24 | 1.65–3.24 | 0.001 |
| HP | ||||||
| Serous | 1 | 1 | ||||
| Non-serous | 0.68 | 0.61–0.90 | 0.008 | 0.56 | 0.5–1 | NS |
| Ascites | ||||||
| No | 1 | 1 | ||||
| Yes | 1.95 | 1.35–2.80 | 0.03 | 2.31 | 1.52–3.5 | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trifanescu, O.G.; Mitrica, R.I.; Gales, L.N.; Marinescu, S.A.; Motas, N.; Trifanescu, R.A.; Rebegea, L.; Gherghe, M.; Georgescu, D.E.; Serbanescu, G.L.; et al. Validation of a New Prognostic Score in Patients with Ovarian Adenocarcinoma. Medicina 2023, 59, 229. https://doi.org/10.3390/medicina59020229
Trifanescu OG, Mitrica RI, Gales LN, Marinescu SA, Motas N, Trifanescu RA, Rebegea L, Gherghe M, Georgescu DE, Serbanescu GL, et al. Validation of a New Prognostic Score in Patients with Ovarian Adenocarcinoma. Medicina. 2023; 59(2):229. https://doi.org/10.3390/medicina59020229
Chicago/Turabian StyleTrifanescu, Oana Gabriela, Radu Iulian Mitrica, Laurentia Nicoleta Gales, Serban Andrei Marinescu, Natalia Motas, Raluca Alexandra Trifanescu, Laura Rebegea, Mirela Gherghe, Dragos Eugen Georgescu, Georgia Luiza Serbanescu, and et al. 2023. "Validation of a New Prognostic Score in Patients with Ovarian Adenocarcinoma" Medicina 59, no. 2: 229. https://doi.org/10.3390/medicina59020229
APA StyleTrifanescu, O. G., Mitrica, R. I., Gales, L. N., Marinescu, S. A., Motas, N., Trifanescu, R. A., Rebegea, L., Gherghe, M., Georgescu, D. E., Serbanescu, G. L., Bashar, H. H., Dragosloveanu, S., Cristian, D. A., & Anghel, R. M. (2023). Validation of a New Prognostic Score in Patients with Ovarian Adenocarcinoma. Medicina, 59(2), 229. https://doi.org/10.3390/medicina59020229