
Germline DNA Damage Response Gene Mutations in Localized Prostate Cancer
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Sample Collection and NGS
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Group
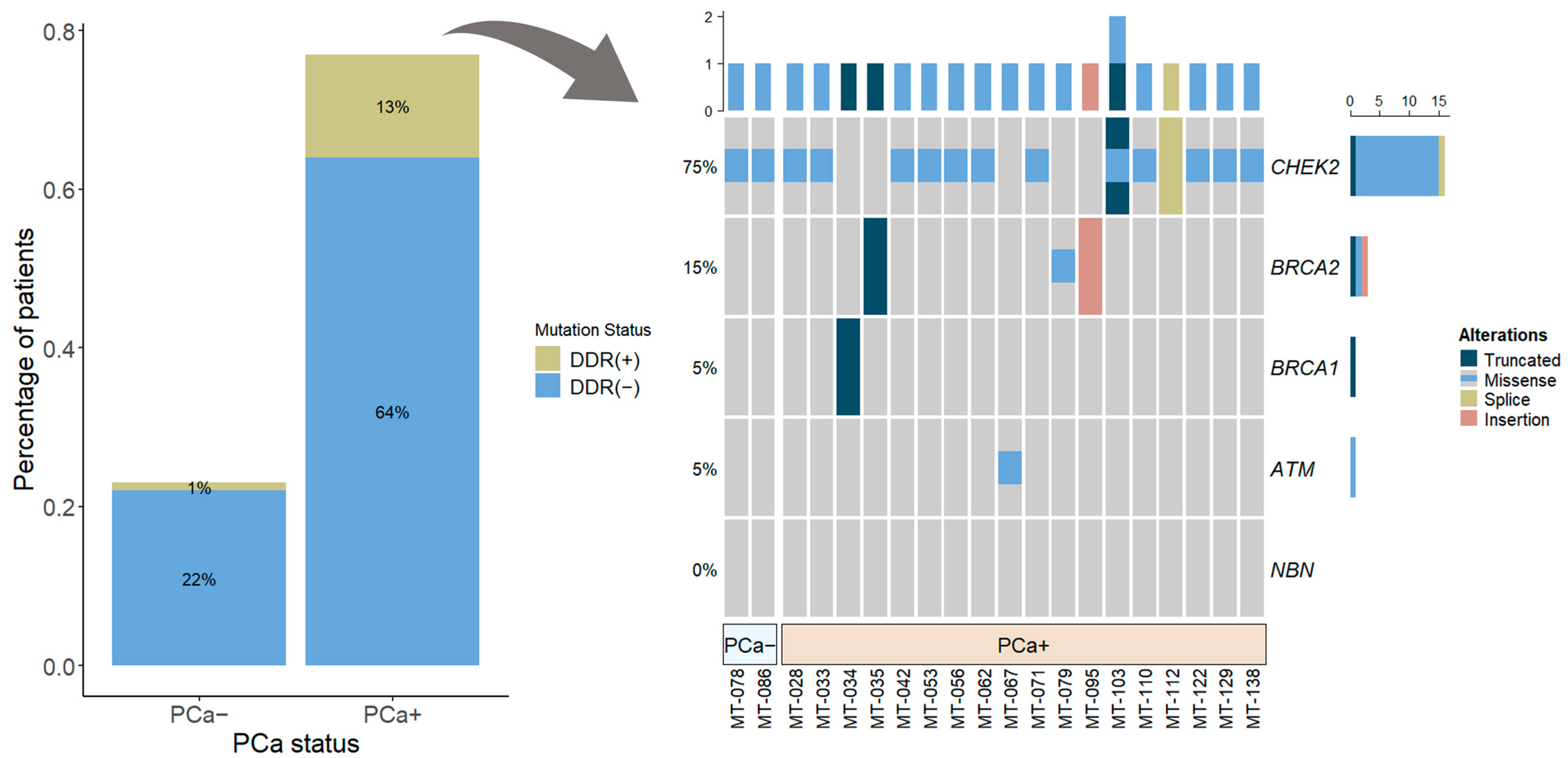
3.2. DDR Gene Mutations Rates
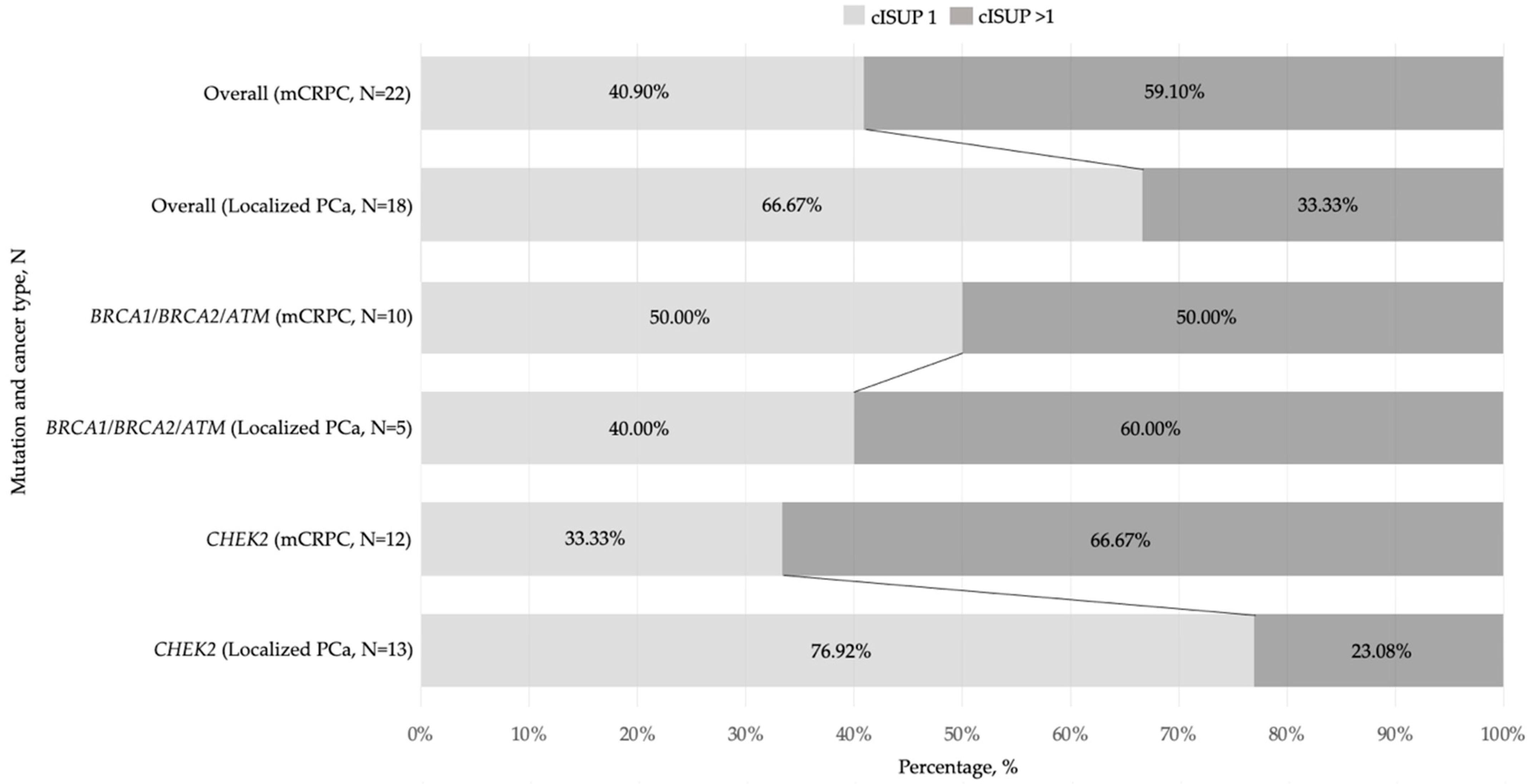
3.3. Clinical Characteristics of DDR Mutation-Positive PCa
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Burden Statistics and Trends across Europe|ECIS. Available online: https://ecis.jrc.ec.europa.eu/ (accessed on 30 October 2023).
- Castro, E.; Goh, C.; Olmos, D.; Saunders, E.; Leongamornlert, D.; Tymrakiewicz, M.; Mahmud, N.; Dadaev, T.; Govindasami, K.; Guy, M.; et al. Germline BRCA mutations are associated with higher risk of nodal involvement, distant metastasis, and poor survival outcomes in prostate cancer. J. Clin. Oncol. 2013, 31, 1748–1757. [Google Scholar] [CrossRef] [PubMed]
- Leongamornlert, D.; Saunders, E.; Dadaev, T.; Tymrakiewicz, M.; Goh, C.; Jurgnauth-Little, S.; Kozarewa, I.; Fenwick, K.; Assiotis, I.; Barrowdale, D.; et al. Frequent germline deleterious mutations in DNA repair genes in familial prostate cancer cases are associated with advanced disease. Br. J. Cancer 2014, 110, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Castro, E.; Aragón, M.I.; Cendón, Y.; Cattrini, C.; López-Casas, P.P.; Olmos, D. Genetic aberrations in DNA repair pathways: A cornerstone of precision oncology in prostate cancer. Br. J. Cancer 2021, 124, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Abeshouse, A.; Ahn, J.; Akbani, R.; Ally, A.; Amin, S.; Andry, C.D.; Annala, M.; Aprikian, A.; Armenia, J.; Arora, A.; et al. The Molecular Taxonomy of Primary Prostate Cancer. Cell 2015, 163, 1011–1025. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; Attard, G.; et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef] [PubMed]
- Lang, S.H.; Swift, S.L.; White, H.; Misso, K.; Kleijnen, J.; Quek, R.G.W. A systematic review of the prevalence of DNA damage response gene mutations in prostate cancer. Int. J. Oncol. 2019, 55, 597–616. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Gomella, L.G.; Petrylak, D.P. When and How to Use PARP Inhibitors in Prostate Cancer: A Systematic Review of the Literature with an Update on On-Going Trials. Eur. Urol. Oncol. 2020, 3, 594–611. [Google Scholar] [CrossRef]
- Na, R.; Zheng, S.L.; Han, M.; Yu, H.; Jiang, D.; Shah, S.; Ewing, C.M.; Zhang, L.; Novakovic, K.; Petkewicz, J.; et al. Germline Mutations in ATM and BRCA1/2 Distinguish Risk for Lethal and Indolent Prostate Cancer and are Associated with Early Age at Death. Eur. Urol. 2017, 71, 740–747. [Google Scholar] [CrossRef]
- Marshall, C.H.; Fu, W.; Wang, H.; Baras, A.S.; Lotan, T.L.; Antonarakis, E.S. Prevalence of DNA repair gene mutations in localized prostate cancer according to clinical and pathologic features: Association of Gleason score and tumor stage. Prostate Cancer Prostatic Dis. 2018, 22, 59–65. [Google Scholar] [CrossRef]
- Wu, Y.; Yu, H.; Li, S.; Wiley, K.; Zheng, S.L.; LaDuca, H.; Gielzak, M.; Na, R.; Sarver, B.A.J.; Helfand, B.T.; et al. Rare Germline Pathogenic Mutations of DNA Repair Genes Are Most Strongly Associated with Grade Group 5 Prostate Cancer. Eur. Urol. Oncol. 2020, 3, 224–230. [Google Scholar] [CrossRef]
- Berchuck, J.E.; Zhang, Z.; Silver, R.; Kwak, L.; Xie, W.; Lee, G.-S.M.; Freedman, M.L.; Kibel, A.S.; Van Allen, E.M.; McKay, R.R.; et al. Impact of Pathogenic Germline DNA Damage Repair alterations on Response to Intense Neoadjuvant Androgen Deprivation Therapy in High-risk Localized Prostate Cancer. Eur. Urol. 2021, 80, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Hausler, R.; Le, A.N.; Kelly, G.; Powers, J.; Ding, J.; Feld, E.; Desai, H.; Morrison, C.; Doucette, A.; et al. Association of Inherited Mutations in DNA Repair Genes with Localized Prostate Cancer. Eur. Urol. 2022, 81, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.H.; Pritchard, C.C.; Montgomery, B.; Lin, D.W.; Nelson, P.S. Prostate Cancer Screening in a New Era of Genetics. Clin. Genitourin. Cancer 2017, 15, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.; Totaro, A.; Gandi, C.; Bientinesi, R.; Moretto, S.; Gavi, F.; Pierconti, F.; Iacovelli, R.; Bassi, P.; Sacco, E. Germline mutations in prostate cancer: A systematic review of the evidence for personalized medicine. Prostate Cancer Prostatic Dis. 2023, 26, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Castro, E.; Romero-Laorden, N.; del Pozo, A.; Lozano, R.; Medina, A.; Puente, J.; Piulats, J.M.; Lorente, D.; Saez, M.I.; Morales-Barrera, R.; et al. Prorepair-B: A Prospective Cohort Study of the Impact of Germline DNA Repair Mutations on the Outcomes of Patients with Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2019, 37, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S.; ESMO Guidelines Committee. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Nombela, P.; Lozano, R.; Aytes, A.; Mateo, J.; Olmos, D.; Castro, E. BRCA2 and Other DDR Genes in Prostate Cancer. Cancers 2019, 11, 352. [Google Scholar] [CrossRef] [PubMed]
- Januskevicius, T.; Sabaliauskaite, R.; Dabkeviciene, D.; Vaicekauskaite, I.; Kulikiene, I.; Sestokaite, A.; Vidrinskaite, A.; Bakavicius, A.; Jankevicius, F.; Ulys, A.; et al. Urinary DNA as a tool for germline and somatic mutation detection in castration-resistant prostate cancer patients. Biomedicines 2023, 11, 761. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhami, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; Santis, M.D.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Gu, Z.; Eils, R.; Schlesner, M. Complex Heatmaps Reveal Patterns and Correlations in Multidimensional Genomic Data. Bioinformatics 2016, 32, 2847–2849. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dai, B.; Ye, D. CHEK2 Mutation and Risk of Prostate Cancer: A Systematic Review and Meta-Analysis. Int. J. Clin. Exp. Med. 2015, 8, 15708. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4658955 (accessed on 14 November 2023). [PubMed]
- Cybulski, C.; Wokolorczyk, D.; Kluzniak, W.; Jakubowska, A.; Gorski, B.; Gronwald, J.; Huzarski, T.; Kashyap, A.; Byrski, T.; Debniak, T.; et al. An Inherited NBN Mutation Is Associated with Poor Prognosis Prostate Cancer. Br. J. Cancer 2012, 108, 461–468. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Fizazi, K.; Piulats, J.M.; Reaume, M.N.; Ostler, P.; McDermott, R.; Gingerich, J.R.; Pintus, E.; Sridhar, S.S.; Bambury, R.M.; Emmenegger, U.; et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N. Engl. J. Med. 2023, 388, 719–732. [Google Scholar] [CrossRef]
- Bryce, A.H.; Piulats, J.M.; Reaume, P.J.; Ostler, R.S.; McDermott, J.R.; Gingerich, E.; Pintus, S.S.; Sridhar, W.; Abida, G.; Daugaard, A.; et al. Rucaparib for metastatic castration-resistant prostate cancer (mCRPC): TRITON3 interim overall survival and efficacy of rucaparib vs docetaxel or second-generation androgen pathway inhibitor therapy. J. Clin. Oncol. 2023, 41 (Suppl. S6), 18. [Google Scholar] [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | DDR(+), n = 18 | DDR(−), n = 89 | p Value |
|---|---|---|---|
| Age at PCa diagnosis, years (mean ± SD) | 61.56 (±5.66) | 63.69 (±7.70) | 0.268 |
| PSA level at PCa diagnosis, ng/mL (median (IQR)) | 5.79 (4.31) | 5.90 (3.73) | 0.739 |
| Prostate volume, mL (median (IQR)) | 55.77 (50.57) | 44.16 (20.63) | 0.057 |
| PSA density (median (IQR)) | 0.11 (0.07) | 0.14 (0.12) | 0.170 |
| cISUP grade group | |||
| <3, n (%) | 15 (83.33%) | 77 (86.62%) | 0.714 |
| ≥3, n (%) | 3 (16.67%) | 12 (13.48%) | |
| PI-RADS category based on the prostate mpMRI | |||
| PI-RADS 3, n (%) | 0 (0.00%) | 4 (4.50%) | 1.000 |
| PI-RADS 4, n (%) | 12 (66.66%) | 55 (61.79%) | |
| PI-RADS 5, n (%) | 6 (33.34%) | 30 (33.70%) | |
| EAU risk groups | |||
| Low-risk PCa, n (%) | 9 (50.00%) | 49 (55.06%) | 0.694 |
| Intermediate- or high-risk PCa, n (%) | 9 (50.00%) | 40 (44.94%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Januskevicius, T.; Vaicekauskaite, I.; Sabaliauskaite, R.; Matulevicius, A.; Vezelis, A.; Ulys, A.; Jarmalaite, S.; Jankevicius, F. Germline DNA Damage Response Gene Mutations in Localized Prostate Cancer. Medicina 2024, 60, 73. https://doi.org/10.3390/medicina60010073
Januskevicius T, Vaicekauskaite I, Sabaliauskaite R, Matulevicius A, Vezelis A, Ulys A, Jarmalaite S, Jankevicius F. Germline DNA Damage Response Gene Mutations in Localized Prostate Cancer. Medicina. 2024; 60(1):73. https://doi.org/10.3390/medicina60010073
Chicago/Turabian StyleJanuskevicius, Tomas, Ieva Vaicekauskaite, Rasa Sabaliauskaite, Augustinas Matulevicius, Alvydas Vezelis, Albertas Ulys, Sonata Jarmalaite, and Feliksas Jankevicius. 2024. "Germline DNA Damage Response Gene Mutations in Localized Prostate Cancer" Medicina 60, no. 1: 73. https://doi.org/10.3390/medicina60010073
APA StyleJanuskevicius, T., Vaicekauskaite, I., Sabaliauskaite, R., Matulevicius, A., Vezelis, A., Ulys, A., Jarmalaite, S., & Jankevicius, F. (2024). Germline DNA Damage Response Gene Mutations in Localized Prostate Cancer. Medicina, 60(1), 73. https://doi.org/10.3390/medicina60010073