
Infectious Diseases and Tropical Cyclones in Southeast China



Abstract
:1. Introduction
2. Materials and Methods
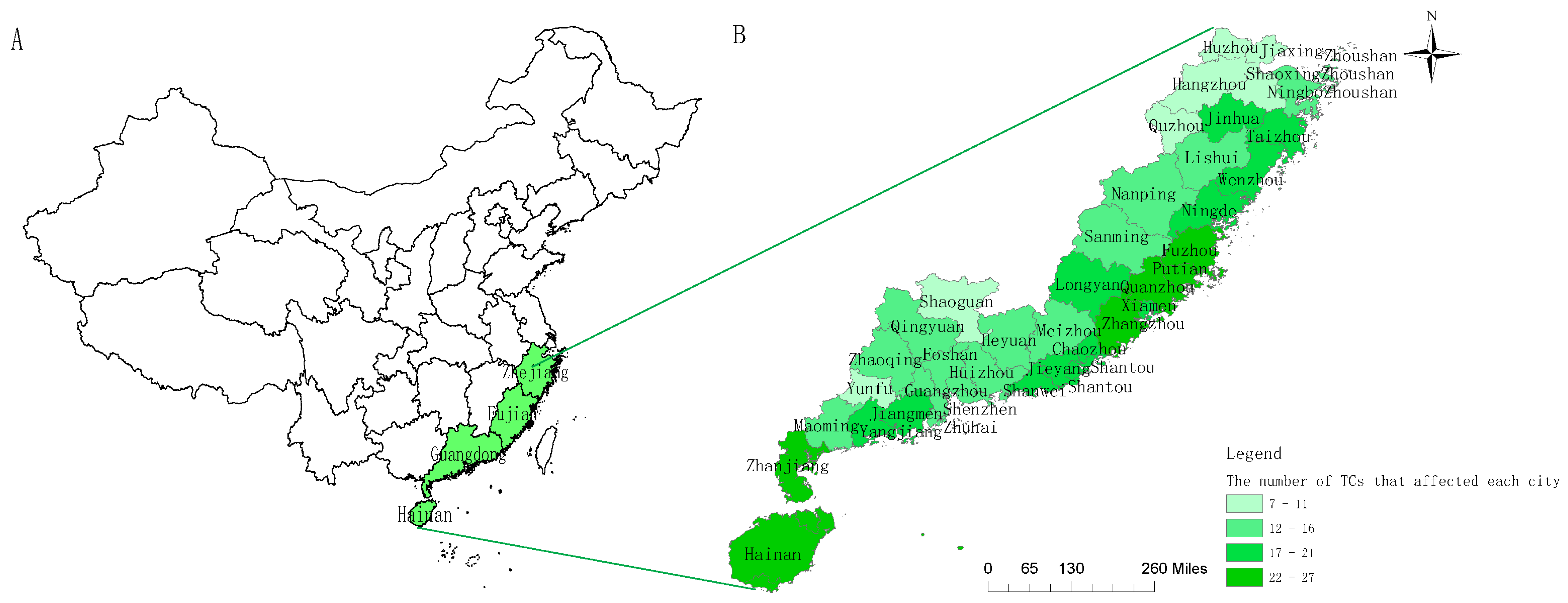
2.1. Study Areas and Study Period
2.2. Data Sources
2.2.1. Disease Data
2.2.2. Meteorological Data
2.2.3. Data of TCs
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Basic Information of TCs during the Study Period
3.2. Disease Frequencies in the Study Period
3.3. Disease Sensitivity to TCs
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ge, S.; Zhang, R. Disastrous weather trend under global climate change and its influence on offshore wind power. Eng. Sci. 2010, 12, 71–77. (In Chinese) [Google Scholar]
- Xiao, F.; Xiao, Z. Characteristics of tropical cyclones in China and their impacts analysis. Nat. Hazard. 2010, 54, 827–837. [Google Scholar]
- Fredrick, T.; Ponnaiah, M.; Murhekar, M.V. Cholera outbreak linked with lack of safe water supply following a tropical cyclone in Pondicherry, India, 2012. J. Health Popul. Nutr. 2015, 33, 31–38. [Google Scholar] [PubMed]
- Lin, C.Y.; Chiu, N.C.; Lee, C.M. Leptospirosis after typhoon. Am. J. Trop. Med. Hyg. 2012, 86, 187–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Shin, Y.; Kim, H.; Pak, H. Impacts of typhoon and heavy rain disasters on mortality and infectious diarrhea hospitalization in South Korea. Int. J. Envir. Health Res. 2013, 23, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.H.; de Arazoza, H.; Lounes, R. Temporal trends and regional variability of 2001–2002 multiwave DENV-3 epidemic in Havana City: Did Hurricane Michelle contribute to its severity? Trop. Med. Int. Health 2013, 18, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Xun, H.; Zhou, M. Impacts of tropical cyclones and accompanying precipitation on infectious diarrhea in cyclone landing areas of Zhejiang Province, China. Int. J. Envir. Res. Public Health 2015, 12, 1054–1068. [Google Scholar] [CrossRef] [PubMed]
- Myint, N.W.; Kaewkungwal, J.; Singhasivanon, P. Are there any changes in burden and management of communicable diseases in areas affected by Cyclone Nargis? Confl. Health 2011, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Ventura, R.J.; Muhi, E.; de los Reyes, V.C. A community-based gastroenteritis outbreak after Typhoon Haiyan, Leyte, Philippines, 2013. Western Pac. Surveill. Response J. 2015, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Vilain, P.; Pages, F.; Combes, X. Health impact assessment of cyclone Bejisa in Reunion Island (France) using syndromic surveillance. Prehosp. Disaster Med. 2015, 30, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Kouadio, I.K.; Aljunid, S.; Kamigaki, T. Infectious diseases following natural disasters: Prevention and control measures. Expert Rev.Anti. Infect. Ther. 2012, 10, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Lane, K.; Charlesguzman, K.; Wheeler, K. Health effects of coastal storms and flooding in urban areas: A review and vulnerability assessment. J. Envir. Public Health 2013, 2013, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kraushar, M.L.; Rosenberg, R.E. A community-led medical response effort in the wake of Hurricane Sandy. Disaster Med. Public Health Prep. 2015, 9, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.; Ye, J.; Ou, W. Guangdong Statistical Yearbook, 2012; China Statistics Press: Beijing, China, 2012; pp. 55, 91, 95. (In Chinese) [Google Scholar]
- Yang, H. Fujian Statistical Yearbook, 2012; China Statistics Press: Beijing, China, 2012; pp. 47, 56, 84. (In Chinese) [Google Scholar]
- Yuan, J.; Li, X.; Hong, Y. Zhejiang Statistical Yearbook, 2012; China Statistics Press: Beijing, China, 2012; pp. 14, 42–44. (In Chinese) [Google Scholar]
- Fu, G.; Zhang, Z. Hainan Statistical Yearbook, 2012; China Statistics Press: Beijing, China, 2012; pp. 33, 57. (In Chinese) [Google Scholar]
- Communique of Main Data of Sampling Survey of Population Change in Zhejiang in 2011. Available online: http://www.zj.stats.gov.cn/tjgb/rkcydcgb/201203/t20120307_122195.html (accessed on 24 August 2011).
- Climatic Characteristics. Available online: http://www.gd-info.gov.cn/shtml/guangdong/gdgl/gdgk/dlgk/2011/08/30/48479.shtml (accessed on 24 August 2011).
- Yu, Z.; Chen, Y. The general climate situation of Fujian. Fujian Agric. 1996, 22. (In Chinese) [Google Scholar]
- Climate of Zhejiang. Available online: http://www.zj.gov.cn/art/2015/3/26/art_923_1543755.html (accessed on 26 March 2015).
- The General Climate Situation of Hainan. Available online: http://www.weather.com.cn/hainan/qxjjj/03/341906.shtml (accessed on 24 March 2010).
- Zhu, G.; Li, Y. Types and changes of Chinese climate zones from 1961 to 2013 based on Köppen climate classification. Arid Land Geogr. 2015, 38, 1121–1131. (In Chinese) [Google Scholar]
- Pidwirny, M. Climate Classification and Climatic Regions of the World. Available online: http://www.physicalgeography.net/fundamentals/7v.html (accessed on 28 February 2017).
- Zhan, S. Epidemiology, 7th ed.; People’s Medical Publishing House: Beijing, China, 2012; p. 217. (In Chinese) [Google Scholar]
- The Notice of Management that Adjusting Part of the Notifiable Infectious Diseases from National Health and Family Planning Commission of the People’s Republic of China. Available online: http://www.nhfpc.gov.cn/jkj/s3577/201311/f6ee56b5508a4295a8d552ca5f0f5edd.shtml (accessed on 4 November 2013). (In Chinese)
- China Meteorological Administration. Yearbook of Tropical Cyclone, 2005–2011; China Meteorological Press: Beijing, China, 2007–2013. (In Chinese)
- General Administration of Quality Supervision, Inspection and Quarantine of the People’s Republic of China, Standardization Administration of the People’s Republic of China. Grade of Tropical Cyclone (GB/T 19201–2006); Standards Press of China: Beijing, China, 2006. (In Chinese)
- Chen, B.; Liang, W.; Liang, S. Analysis of the law of tropical cyclones that influence Huazhou in late 50 years. J. Meteorol. Res. Appl. 2009, 30, 109–111. (In Chinese) [Google Scholar]
- Wang, D.; Chen, H.; Fan, A. The spatial distribution of wind and rain of tropical cyclones in Zhejiang Province. Bull. Sci. Technol. 2010, 26, 39–45. (In Chinese) [Google Scholar]
- Xu, H.; Chen, H.; Zhao, L. Several statistical characteristics of tropical cyclones that influence Zhejiang. J. Zhejiang Meteorol. 2009, 30, 4–8. (In Chinese) [Google Scholar]
- Yang, C.; Li, S. The wind and rain types of tropical cyclones that influence Zhanjiang. Mar. Sci. Bull. 2003, 22, 15–20. (In Chinese) [Google Scholar]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, America, 2008. [Google Scholar]
- Kim, K.; Miriam, R.E.; Galatea, K. The 2006 California heat wave: impacts on hospitalizations and emergency department visits. Envir. Health Perspect. 2009, 117, 61–67. [Google Scholar]
- Ma, W.; Xu, X.; Peng, L. Impact of extreme temperature on hospital admission in Shanghai, China. Sci. Total Environ. 2011, 409, 3634–3637. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C. The significance test between constituent ratios in the same group. Acta Acad. Med. Taishan 1990, 11, 111–113. (In Chinese) [Google Scholar]
- World Health Organization. En fact Sheet 330: Diarrhoeal Disease. Available online: http://www.who.int/mediacentre/factsheets/fs330/en/index.html (accessed on 6 December 201l).
- Centers for Disease Control and Prevention (CDC). Infectious disease and dermatologic conditions in evacuees and rescue workers after Hurricane Katrina-multiple states, August–September, 2005. J. Am. Med. Assoc. 2005, 54, 961–964. [Google Scholar]
- Panda, S.; Pati, K.K.; Bhattacharya, M.K. Rapid situation & response assessment of diarrhoea outbreak in a coastal district following tropical cyclone AILA in India. India. J. Med. Res. 2011, 133, 395–400. [Google Scholar]
- Kang, R.; Xun, H.; Zhang, Y. Impacts of different grades of tropical cyclones on infectious diarrhea in Guangdong, 2005–2011. PLoS ONE 2015, 10, e0131423. [Google Scholar] [CrossRef] [PubMed]
- Kang, R.; Zhang, Y.; Jiang, B. Relationship between tropical cyclone and incidence of mumps in Zhejiang, China, 2005–2010. J. Envir. Health 2015, 32, 307–311. (In Chinese) [Google Scholar]
- Savage, L.E.; Christian, M.M.D.; Smith, M.S. The Canadian Armed Forces medical response to Typhoon Haiyan. Can. J. Surg. 2015, 58, S146–S152. [Google Scholar] [CrossRef] [PubMed]
- Shultz, J.M.; Russell, J.; Espinel, Z. Epidemiology of tropical cyclones: the dynamics of disaster, disease, and development. Epidemiol. Rev. 2005, 27, 21–35. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Climate | Guangdong [19] | Fujian [20] | Zhejiang [21] | Hainan [22] |
|---|---|---|---|---|
| General condition | It usually has high temperature and rainy days. It has a typical summer season for seven months each year and is one of the rainiest provinces in China. | It has four distinct seasons, with moderate temperature and abundant rainfall. | The same as Fujian. | It has a tropical climate. |
| Average annual temperature | 18–24 °C | 17–21 °C | 15–18 °C | 22.5–25.6 °C |
| Average annual rainfall | 1350–2600 mm | 1100–2000 mm | 980–2000 mm | 1500–2500 mm |
| The Köppen Climate Classification [23] | Cfa | Cfa | Cfa | Cwa |
| Province | Year | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | ||
| Guangdong | 8 | 8 | 6 | 7 | 10 | 6 | 6 | 51 |
| Fujian | 6 | 5 | 5 | 8 | 4 | 5 | 3 | 36 |
| Zhejiang | 5 | 6 | 5 | 4 | 3 | 2 | 2 | 27 |
| Hainan | 4 | 3 | 2 | 3 | 7 | 3 | 5 | 27 |
| Disease | Number of Cases of Disease in Cyclone Period/per Day | Number of Cases of Disease in Non-Cyclone Period/per Day |
|---|---|---|
| Water-Food Transmitted | ||
| Bacillary dysentery | 24.3 | 21.0 |
| Typhoid fever | 4.1 | 4.5 |
| Paratyphoid fever | 8.8 | 4.1 |
| Other infectious diarrhea | 42.4 | 40.5 |
| Hepatitis A | 4.4 | 3.4 |
| Air Transmitted | ||
| Influenza | 9.5 | 7.1 |
| Influenza A (H1N1) | 9.5 | 7.4 |
| HFMD a | 67.5 | 71.0 |
| Measles | 8.0 | 10.8 |
| Rubella | 4.7 | 12.8 |
| Mumps | 13.9 | 18.8 |
| Varicella b | 8.3 | 9.2 |
| Mosquito Transmitted | ||
| Vivax malaria | 18.2 | 23.0 |
| Nontypeable malaria | 8.9 | 11.5 |
| Dengue fever | 5.6 | 5.0 |
| Contact Transmitted | ||
| Acute hemorrhagic conjunctivitis | 69.7 | 67.1 |
| Disease | Number of TCs Increasing the Risk (%) | Number of TCs Increasing the Risk with Statistical Significance (%) | Number of TCs Decreasing the Risk (%) | Number of TCs Decreasing the Risk with Statistical Significance (%) | Direction d of the Effect and P e | Range of RR |
|---|---|---|---|---|---|---|
| Water-Food Transmitted | ||||||
| Bacillary dysentery | 69 (10.22) | 4 (0.59) | 36 (5.33) | 1 (0.15) | ↑0.001 | 0.47–5.63 |
| Typhoid fever | 1 (0.15) | 0 (0) | 0 (0) | 0 (0) | ↑0.317 | 2.38 |
| Paratyphoid fever | 4 (0.59) | 0 (0) | 0 (0) | 0 (0) | ↑0.046 | 1.04–6.81 |
| Other infectious diarrhea | 246 (36.44) | 26 (3.85) | 206 (30.52) | 19 (2.81) | ↑0.060 | 0.23–14.33 |
| Hepatitis A | 4 (0.59) | 0 (0) | 3 (0.44) | 0 (0) | ↑0.705 | 0.75–2.26 |
| Air Transmitted | ||||||
| Influenza | 40 (5.93) | 8 (1.19) | 30 (4.44) | 11 (1.63) | ↑0.232 | 0.01–144.38 |
| Influenza A (H1N1) | 10 (1.48) | 5 (0.74) | 8 (1.19) | 6 (0.89) | ↑0.637 | 0–10.75 |
| HFMD b | 134 (19.85) | 26 (3.85) | 144 (21.33) | 28 (4.15) | ↓0.549 | 0.10–6.73 |
| Measles | 18 (2.67) | 1 (0.15) | 39 (5.78) | 4 (0.59) | ↓0.005 | 0.19–3.74 |
| Mumps | 84 (12.44) | 4 (0.59) | 136 (20.15) | 21 (3.11) | ↓<0.001 | 0.25–8.17 |
| Rubella | 0 (0) | 0 (0) | 3 (0.44) | 2 (0.3) | ↓0.083 | 0.13–0.43 |
| Varicella c | 28 (4.15) | 2 (0.3) | 50 (7.41) | 6 (0.89) | ↓0.013 | 0.12–14.24 |
| Mosquito Transmitted | ||||||
| Vivax malaria | 0 (0) | 0 (0) | 8 (1.19) | 0 (0) | ↓0.005 | 0.47–0.98 |
| Nontypeable malaria | 2 (0.3) | 0 (0) | 7 (1.04) | 1 (0.15) | ↓0.096 | 0.33–1.38 |
| Dengue fever | 4 (0.59) | 1 (0.15) | 0 (0) | 0 (0) | ↑0.046 | 1.11–34.38 |
| Contact Transmitted | ||||||
| Acute hemorrhagic conjunctivitis | 32 (4.74) | 22 (3.26) | 16 (2.37) | 13 (1.93) | ↑0.021 | 0.18–60.00 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, J.; Han, W.; Jiang, B.; Ma, W.; Zhang, Y. Infectious Diseases and Tropical Cyclones in Southeast China. Int. J. Environ. Res. Public Health 2017, 14, 494. https://doi.org/10.3390/ijerph14050494
Zheng J, Han W, Jiang B, Ma W, Zhang Y. Infectious Diseases and Tropical Cyclones in Southeast China. International Journal of Environmental Research and Public Health. 2017; 14(5):494. https://doi.org/10.3390/ijerph14050494
Chicago/Turabian StyleZheng, Jietao, Weixiao Han, Baofa Jiang, Wei Ma, and Ying Zhang. 2017. "Infectious Diseases and Tropical Cyclones in Southeast China" International Journal of Environmental Research and Public Health 14, no. 5: 494. https://doi.org/10.3390/ijerph14050494
APA StyleZheng, J., Han, W., Jiang, B., Ma, W., & Zhang, Y. (2017). Infectious Diseases and Tropical Cyclones in Southeast China. International Journal of Environmental Research and Public Health, 14(5), 494. https://doi.org/10.3390/ijerph14050494