Self-Reported vs. Measured Height, Weight, and BMI in Young Adults

 , , , , and
, , , , and
Abstract
:1. Introduction & Background
2. Methods
3. Results
4. Accuracy of Self-Reported versus Measured Height, Weight, and BMI
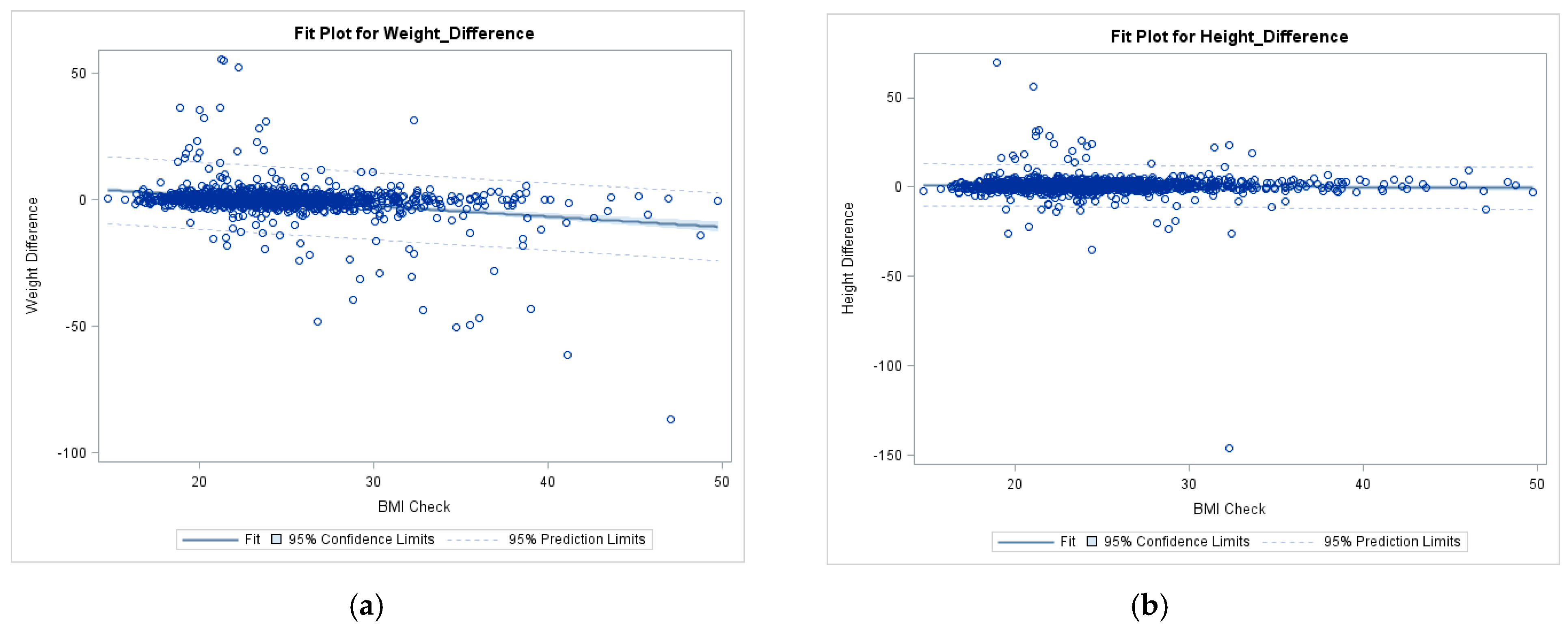
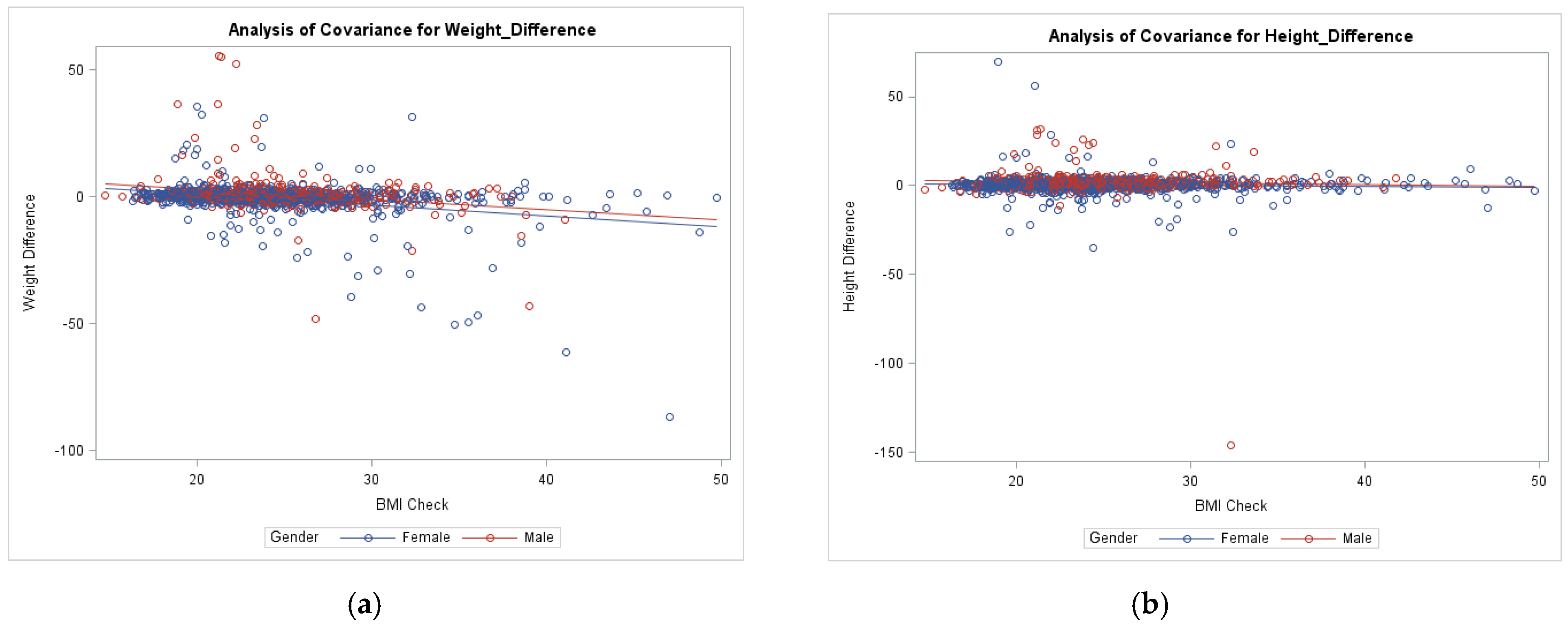
5. Effect of BMI on Self-Reported Height and Weight
6. Discussion
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arnold, M.; Leitzmann, M.; Freisling, H.; Bray, F.; Romieu, I.; Renehan, A.; Soerjomataram, I. Obesity and cancer: An update of the global impact. Cancer Epidemiol. 2016, 41, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Zobel, E.H.; Hansen, T.W.; Rossing, P.; von Scholten, B.J. Global changes in food supply and the obesity epidemic. Curr. Obes. Rep. 2016, 5, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Flint, A.J.; Berrington de Gonzalez, A.; Bernstein, L.; Brotzman, M.; MacInnis, R.J.; Moore, S.C.; Robien, K.; Rosenberg, P.S.; Singh, P.N.; et al. Association between class III obesity (BMI of 40–59 kg/m2) and mortality: A pooled analysis of 20 prospective studies. PLoS Med. 2014, 11, e1001673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calle, E.E.; Thun, M.J. Obesity and cancer. Oncogene 2004, 23, 6365–6378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polednak, A.P. Estimating the number of US incident cancers attributable to obesity and the impact on temporal trends in incidence rates for obesity-related cancers. Cancer Detect. Prev. 2008, 32, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, E.A.; Trogdon, J.G.; Cohen, J.W.; Dietz, W. Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health Aff. 2009, 28, w822–w831. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014; US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Washington, DC, USA, 2015.
- Nyholm, M.; Gullberg, B.; Merlo, J.; Lundqvist-Persson, C.; Råstam, L.; Lindblad, U. The validity of obesity based on self-reported weight and height: Implications for population studies. Obesity 2007, 15, 197. [Google Scholar] [CrossRef] [PubMed]
- Barrios, P.; Martin-Biggers, J.; Quick, V.; Byrd-Bredbenner, C. Reliability and criterion validity of self-measured waist, hip, and neck circumferences. BMC Med Res. Methodol. 2016, 16, 49. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.L.; Green, J.; Reeves, G.; Beral, V.; Cairns, B.J. Validity over time of self-reported anthropometric variables during follow-up of a large cohort of UK women. BMC Med Res. Methodol. 2015, 15, 81. [Google Scholar] [CrossRef] [PubMed]
- Sherry, B.; Jefferds, M.E.; Grummer-Strawn, L.M. Accuracy of adolescent self-report of height and weight in assessing overweight status: A literature review. Arch. Pediatr. Adolesc. Med. 2007, 161, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Thabane, L.; Beyene, J.; Raina, P. Power analysis for population-based longitudinal studies investigating gene-environment interactions in chronic diseases: A simulation study. PLoS ONE 2016, 11, e0149940. [Google Scholar] [CrossRef] [PubMed]
- Yorkin, M.; Spaccarotella, K.; Martin-Biggers, J.; Quick, V.; Byrd-Bredbenner, C. Accuracy and consistency of weights provided by home bathroom scales. BMC Public Health 2013, 13, 1194. [Google Scholar] [CrossRef] [PubMed]
- Bonn, S.E.; Lagerros, Y.T.; Bälter, K. How valid are Web-based self-reports of weight? J. Med. Internet Res. 2013, 15, e52. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.M.; Richardson, J.S. Peer Reviewed: Validity of Self-Reported Height, Weight, and Body Mass Index: Findings from the National Health and Nutrition Examination Survey, 2001–2006. Prev. Chronic Dis. 2009, 6, A121. [Google Scholar] [PubMed]
- Engstrom, J.L.; Paterson, S.A.; Doherty, A.; Trabulsi, M.; Speer, K.L. Accuracy of self-reported height and weight in women: An integrative review of the literature. J. Midwifery Women’s Health 2003, 48, 338–345. [Google Scholar] [CrossRef]
- Gorber, S.C.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: A systematic review. Obes. Rev. 2007, 8, 307–326. [Google Scholar] [CrossRef] [PubMed]
- Bowring, A.L.; Peeters, A.; Freak-Poli, R.; Lim, M.S.; Gouillou, M.; Hellard, M. Measuring the accuracy of self-reported height and weight in a community-based sample of young people. BMC Med Res. Methodol. 2012, 12, 175. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, H.; Weaver, D.; Hsiao, J.; Whitestone, J.; Kau, T.Y.; Whisler, R.; Ferri, R. Comparison of measured and self-reported anthropometric information among firefighters: Implications and applications. Ergonomics 2014, 57, 1886–1897. [Google Scholar] [CrossRef] [PubMed]
- Griebeler, M.L.; Levis, S.; Beringer, L.M.; Chacra, W.; Gómez-Marín, O. Self-reported versus measured height and weight in Hispanic and non-Hispanic menopausal women. J. Women’s Health 2011, 20, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Tamakoshi, K.; Tsunekawa, T.; Otsuka, R.; Zhang, H.; Murata, C.; Nagasawa, N.; Matsushita, K.; Sugiura, K.; Yatsuya, H. Validity of self-reported height and weight in a Japanese workplace population. Int. J. Obes. 2005, 29, 1093. [Google Scholar] [CrossRef] [PubMed]
- Stommel, M.; Osier, N. Temporal changes in bias of body mass index scores based on self-reported height and weight. Int. J. Obes. 2013, 37, 461. [Google Scholar] [CrossRef] [PubMed]
- Nissinen, K.; Mikkilä, V.; Männistö, S.; Lahti-Koski, M.; Räsänen, L.; Viikari, J.; Raitakari, O.T. Sweets and sugar-sweetened soft drink intake in childhood in relation to adult BMI and overweight. The Cardiovascular Risk in Young Finns Study. Public Health Nutr. 2009, 12, 2018–2026. [Google Scholar] [CrossRef] [PubMed]
- Quick, V.; Byrd-Bredbenner, C.; Shoff, S.; White, A.A.; Lohse, B.; Horacek, T.; Kattelmann, K.; Phillips, B.; Hoerr, S.L.; Greene, G.; et al. Concordance of self-report and measured height and weight of college students. J. Nutr. Educ. Behav. 2015, 47, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Do, D.P.; Zheng, C. A marginal structural modeling strategy investigating short and long-term exposure to neighborhood poverty on BMI among US black and white adults. Health Place 2017, 46, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Burdette, A.M.; Needham, B.L. Neighborhood environment and body mass index trajectories from adolescence to adulthood. J. Adolesc. Health 2012, 50, 30–37. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| VARIABLE | Frequency (%) | Measured Ht (cm) | Self-Reported Ht (cm) | Ht p-Value | Measured Wt (kg) | Self-Reported Wt (kg) | Wt p-Value |
|---|---|---|---|---|---|---|---|
| N = 1562 | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Sex | <0.0001 * | <0.0001 * | |||||
| Male | 450 (29.8) | 175.3 ± 7.7 | 177.3 ± 7.2 | 76.0 ± 15.2 | 76.8 ± 14.5 | ||
| Female | 1064 (68.1) | 164.7 ± 7.1 | 164.7 ± 7.5 | 65.7 ± 15.2 | 65.2 ± 14.4 | ||
| Did not answer | 48 (3.1) | 168.6 ± 10.2 | 169.1 ± 10.3 | 65.9 ± 12.3 | 65.3 ± 12.8 | ||
| Race | 0.1269 | 0.0635 | |||||
| White | 881 (56.4) | 168.3 ± 8.6 | 169.0 ± 9.2 | 69.9 ± 15.9 | 69.9 ± 15.3 | ||
| Black or African American | 161 (10.3) | 167.0 ± 9.2 | 167.7 ± 9.8 | 69.6 ± 16.4 | 69.3 ± 14.5 | ||
| Asian | 142 (9.1) | 165.0 ± 8.9 | 165.6 ± 9.7 | 60.5 ± 12.4 | 60.9 ± 13.2 | ||
| American Indian/Alaska Native | 16 (1.0) | 170.7 ± 7.5 | 171.8 ± 8.4 | 77.6 ± 13.7 | 80.3 ± 14.1 | ||
| Native Hawaiian/other Pacific Islander | 10 (0.6) | 167.5 ± 9.3 | 168.7 ± 10.2 | 67.6 ± 14.1 | 69.5 ± 14.9 | ||
| Biracial | 21 (1.3) | 168.8 ± 10.3 | 165.8 ± 8.8 | 72.9 ± 18.3 | 68.5 ± 13.9 | ||
| Other | 64 (4.1) | 167.8 ± 9.6 | 168.8 ± 10.3 | 67.6 ± 15.7 | 66.3 ± 13.9 | ||
| Did not answer | 267 (17.1) | 168.2 ± 8.5 | 168.8 ± 9.2 | 67.9 ± 15.8 | 69.8 ± 17.1 | ||
| State | 0.0248 * | <0.0001 * | |||||
| Alabama | 112 (7.2) | 168.7 ± 8.7 | 163.4 ± 9.3 | 71.1 ± 18.8 | 70.4 ± 18.6 | ||
| Florida | 399 (25.5) | 166.1 ± 8.1 | 166.8 ± 8.5 | 64.1 ± 13.1 | 63.7 ± 12.4 | ||
| Kansas | 111 (7.1) | 169.1 ± 9.2 | 169.7 ± 9.9 | 72.9 ± 17.6 | 72.4 ± 17.6 | ||
| Maine | 197 (12.6) | 169.7 ± 8.5 | 169.2 ± 9.3 | 72.6 ± 17.5 | 71.4 ± 15.4 | ||
| New York | 187 (12.0) | 167.4 ± 9.7 | 169.0 ± 10.3 | 66.0 ± 13.1 | 67.4 ± 13.5 | ||
| South Dakota | 136 (8.7) | 167.8 ± 8.0 | 168.1 ± 8.5 | 69.7 ± 14.7 | 72.8 ± 16.3 | ||
| Tennessee | 227 (14.5) | 169.3 ± 9.3 | 170.4 ± 10.2 | 69.8 ± 15.3 | 72.5 ± 15.0 | ||
| West Virginia | 193 (12.4) | 167.1 ± 8.7 | 167.8 ± 9.4 | 70.6 ± 17.5 | 71.7 ± 16.8 | ||
| Appalachian Status | 0.1493 | 0.2510 | |||||
| Appalachian | 185 (11.8) | 169.2 ± 9.2 | 169.8 ± 10.0 | 72.2 ± 17.6 | 71.7 ± 15.7 | ||
| Non-Appalachian | 1140 (73.0) | 167.8 ± 8.8 | 168.5 ± 9.4 | 68.7 ± 15.8 | 68.6 ± 15.2 | ||
| Did not answer | 237 (15.2) | 166.9 ± 8.4 | 167.6 ± 9.1 | 65.9 ± 14.1 | 67.0 ± 15.8 |
| Measure | Overall Sample | Males | Females | p-Value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Measured Height | 167.85 ± 8.8 | 175.3 ± 7.7 | 164.7 ± 7.1 | |
| Self-Reported Height | 168.6 ± 9.6 | 177.3 ± 7.2 | 164.8 ± 7.9 | |
| Height Difference | 0.71 ± 3.9 | 2.0 ± 4.3 | 0.12 ± 3.5 | <0.0001 * |
| Measured Weight | 68.68 ± 15.8 | 76.0 ± 15.2 | 65.7 ± 15.2 | |
| Self-Reported Weight | 68.8 ± 15.4 | 76.8 ± 14.5 | 65.2 ± 14.4 | |
| Weight Difference | −0.05 ± 7.0 | 1.1 ± 7.2 | −0.61 ± 6.9 | <0.0001 * |
| Frequency (%) | Frequency (%) | Frequency (%) | ||
| Measured BMI Categories | (N = 1522) | (N = 442) | (N = 1034) | |
| 0—Underweight | 83 (5.53) | 15 (3.3) | 63 (5.9) | |
| 1—Normal Weight | 906 (59.5) | 256 (56.9) | 624 (58.6) | |
| 2—Overweight | 380230 (25.0) | 126 (28.0) | 241 (22.7) | |
| 3—Obese | 152 153 (10.1) | 45 (10.0) | 106 (10.0) | |
| Self-Report BMI Categories | (N = 1322) | (N = 419) | (N = 864) | |
| 0—Underweight | 64 (4.8) | 15 (3.6) | 45 (5.2) | |
| 1—Normal Weight | 805 (60.9) | 241 (57.5) | 539 (62.4) | |
| 2—Overweight | 330 (25.0) | 125 (29.8) | 195 (22.6) | |
| 3—Obese | 123 (9.3) | 38 (9.1) | 85 (9.8) |
| Measured to Self-Reported BMI Categories | Agreement | |
|---|---|---|
| Overall Sample | κ = 0.77 (95% CI, 0.74 to 0.80), p < 0.0001 | Good |
| Sex | ||
| Male | κ = 0.79 (95% CI, 0.73 to 0.84), p < 0.0001 | Good |
| Female | κ = 0.76 (95% CI, 0.72 to 0.80), p < 0.0001 | Good |
| Race | ||
| American Indian/Alaskan Native | κ = 0.66 (95% CI, 0.32 to 1.00), p < 0.0005 | Adequate |
| Asian | κ = 0.72 (95% CI, 0.60 to 0.84), p < 0.0001 | Good |
| Black or African American | κ = 0.84 (95% CI, 0.75 to 0.92), p < 0.0001 * | Very Good |
| Native Hawaiian/Pacific Islander | κ = 0.44 (95% CI, -0.13 to 1.00), p < 0.0160 | Poor |
| White | κ = 0.80 (95% CI, 0.77 to 0.84), p < 0.0001 * | Very Good |
| Biracial | κ = 0.42 (95% CI, 0.06 to 0.83), p < 0.0001 | Poor |
| Appalachian Status | ||
| Appalachian | κ = 0.71 (95% CI, 0.61 to 0.80), p < 0.0001 | Good |
| Non-Appalachian | κ = 0.79 (95% CI, 0.76 to 0.83), p < 0.0001 | Good |
| State | ||
| AL | κ = 0.69 (95% CI, 0.57 to 0.82), p < 0.0001 | Adequate |
| FL | κ = 0.74 (95% CI, 0.68 to 0.81), p < 0.0001 | Good |
| KS | κ = 0.83 (95% CI, 0.74 to 0.93), p < 0.0001 * | Very Good |
| ME | κ = 0.74 (95% CI, 0.65 to 0.83), p < 0.0001 | Good |
| NY | κ = 0.77 (95% CI, 0.68 to 0.86), p < 0.0001 | Good |
| SD | κ = 0.82 (95% CI, 0.69 to 0.94), p < 0.0001 * | Very Good |
| TN | κ = 0.81 (95% CI, 0.73 to 0.89), p < 0.0001 * | Very Good |
| WV | κ = 0.77 (95% CI, 0.67 to 0.87), p < 0.0001 | Good |
| Region | ||
| Northeastern | κ = 0.72 (95% CI, 0.65 to 0.78), p < 0.0001 | Good |
| Southeastern | κ = 0.80 (95% CI, 0.76 to 0.85), p < 0.0001 * | Very Good |
| Northwestern | κ = 0.64 (95% CI, 0.24 to 1.00), p < 0.0028 | Adequate |
| Southwestern | κ = 0.95 (95% CI, 0.86 to 1.00), p < 0.0001 * | Very Good |
| Midwest | κ = 0.81 (95% CI, 0.74 to 0.88), p < 0.0001 * | Very Good |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olfert, M.D.; Barr, M.L.; Charlier, C.M.; Famodu, O.A.; Zhou, W.; Mathews, A.E.; Byrd-Bredbenner, C.; Colby, S.E. Self-Reported vs. Measured Height, Weight, and BMI in Young Adults. Int. J. Environ. Res. Public Health 2018, 15, 2216. https://doi.org/10.3390/ijerph15102216
Olfert MD, Barr ML, Charlier CM, Famodu OA, Zhou W, Mathews AE, Byrd-Bredbenner C, Colby SE. Self-Reported vs. Measured Height, Weight, and BMI in Young Adults. International Journal of Environmental Research and Public Health. 2018; 15(10):2216. https://doi.org/10.3390/ijerph15102216
Chicago/Turabian StyleOlfert, Melissa D., Makenzie L. Barr, Camille M. Charlier, Oluremi A. Famodu, Wenjun Zhou, Anne E. Mathews, Carol Byrd-Bredbenner, and Sarah E. Colby. 2018. "Self-Reported vs. Measured Height, Weight, and BMI in Young Adults" International Journal of Environmental Research and Public Health 15, no. 10: 2216. https://doi.org/10.3390/ijerph15102216
APA StyleOlfert, M. D., Barr, M. L., Charlier, C. M., Famodu, O. A., Zhou, W., Mathews, A. E., Byrd-Bredbenner, C., & Colby, S. E. (2018). Self-Reported vs. Measured Height, Weight, and BMI in Young Adults. International Journal of Environmental Research and Public Health, 15(10), 2216. https://doi.org/10.3390/ijerph15102216