STI Health Disparities: A Systematic Review and Meta-Analysis of the Effectiveness of Preventive Interventions in Educational Settings

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Analysis
3. Results
3.1. Study Selection
3.2. Risk of Bias Assessment
3.3. Study Characteristics
3.4. Synthesis of Results
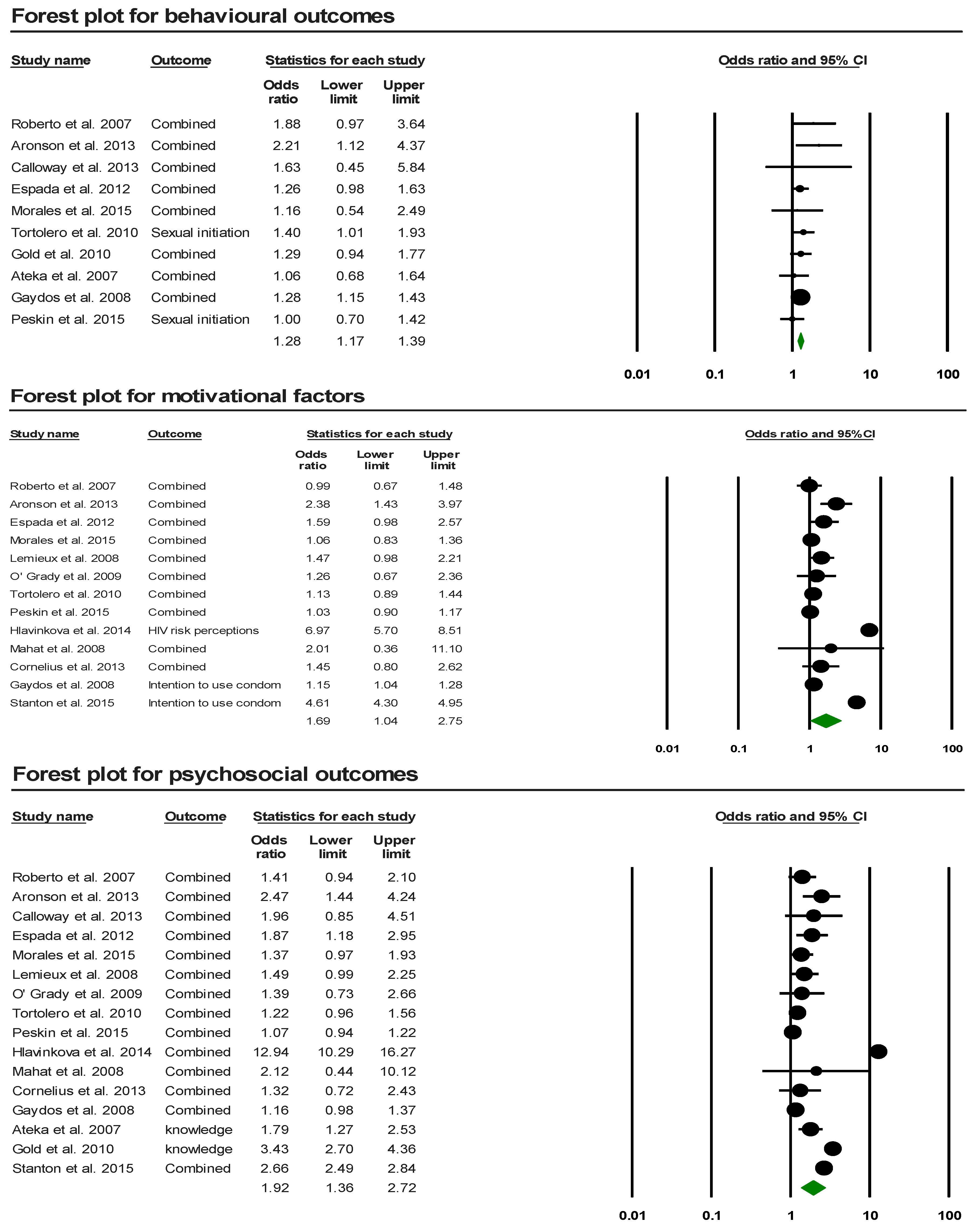
3.4.1. Effects of Interventions on the Behavioral and Psychosocial Outcomes
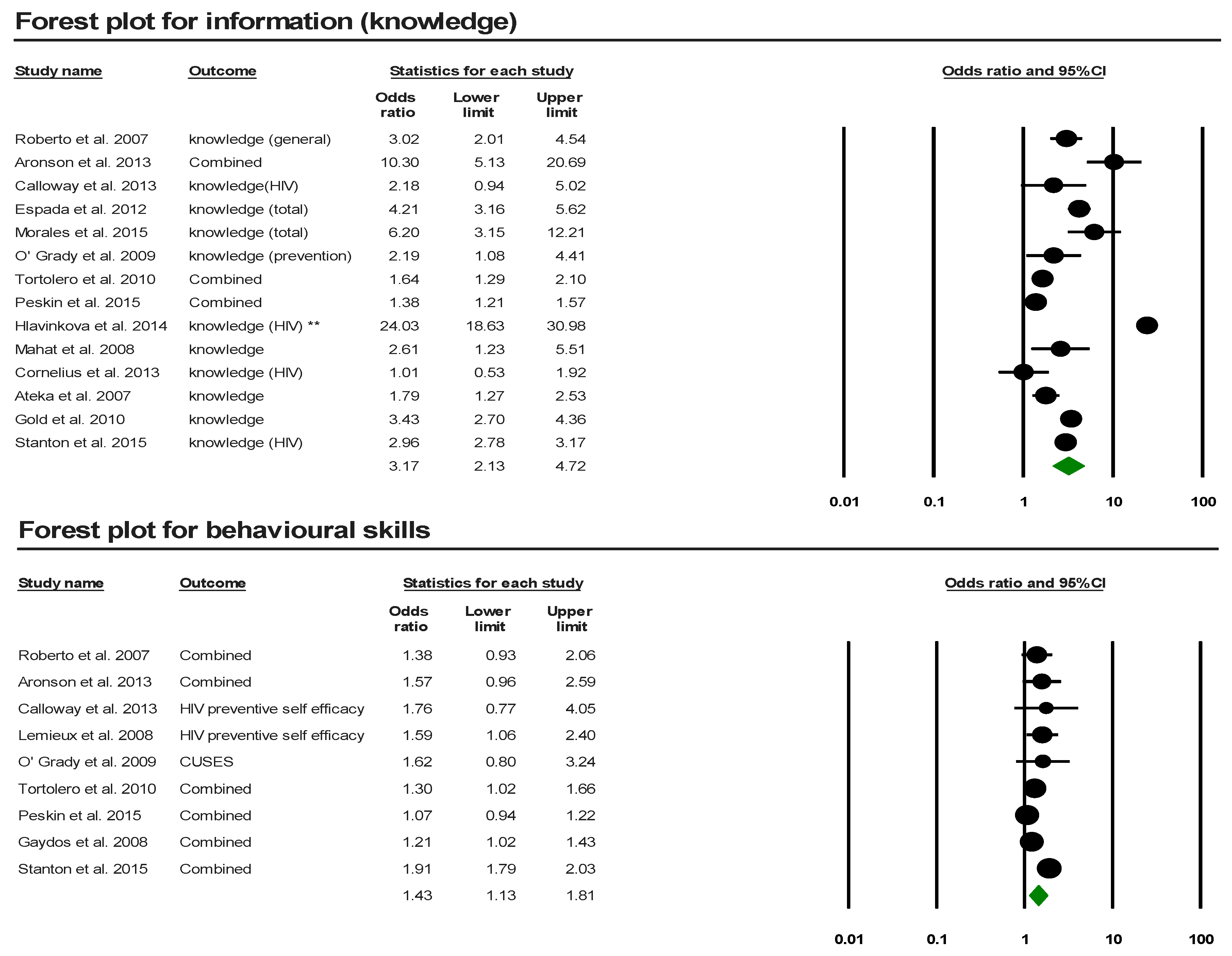
3.4.2. Effects of Interventions on the Psychosocial Sub-Categorical Outcomes
3.4.3. Effects of Interventions on the Specific Psychosocial and Behavioral Outcomes
3.4.4. Comparative Analysis
3.4.5. Subgroup Analysis
4. Discussion
4.1. Strength and Limitations
4.2. Recommendations for Future Research
5. Conclusions
6. Ethics Statement
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Sexually Transmitted Infections (STIs). Available online: http://www.who.int/en/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 23 June 2018).
- Smith, J. STD Statistics Worldwide—INFOGRAPHIC. Infographics Archive. 2012. Available online: https://www.infographicsarchive.com/health-beauty-safety/std-statistics-worldwide/ (accessed on 24 June 2018).
- Augustine, J.; Bridges, E. Young People and Sexually Transmitted Infections Underlying Risk Factors Leave Some More Vulnerable; Advocates for Youth: Washington, DC, USA, 2010; Available online: http://advocatesforyouth.org/publications/230 (accessed on 23 June 2018).
- Centers for Disease Control and Prevention. 2016 Sexually Transmitted Diseases Surveillance. 2017. Available online: https://www.cdc.gov/std/stats16/adolescents.htm (accessed on 4 July 2018).
- Davis, J.; Bauman, K. School Enrollment in the United States: 2011. September 2013. Available online: https://www.cdc.gov/std/stats16/adolescents.htm (accessed on 4 July 2018).
- Statistics Canada. A Portrait of Canadian Youth. Average Counts of Offenders in Federal Programs, Canada and Regions. 2018. Available online: https://www150.statcan.gc.ca/n1/pub/11-631-x/11-631-x2018001-eng.htm#a2 (accessed on 5 August 2018).
- UK Government. Department of Education. National Statistics—Schools, Pupils and Their Characteristics. January 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/719226/Schools_Pupils_and_their_Characteristics_2018_Main_Text.pdf (accessed on 5 August 2018).
- Adams, R. Almost Half of All Young People in England Go on to Higher Education. Guardian News and Media. 28 September 2017. Available online: https://www.theguardian.com/education/2017/sep/28/almost-half-of-all-young-people-in-england-go-on-to-higher-education (accessed on 5 August 2018).
- Centers for Disease Control and Prevention. NCHHSTP Newsroom. 2015. Available online: https://www.cdc.gov/nchhstp/newsroom/2015/nhpc-press-release-schools-teaching-prevention.html (accessed on 23 June 2018).
- Public Health Agency of Canada. Report on Sexually Transmitted Infections in Canada: 2013–2014. Canada.ca. 2017. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/report-sexually-transmitted-infections-canada-2013-14.html (accessed on 24 June 2018).
- UNSW—The Kirby Institute for Infection and Immunity in Society. Annual Surveillance Report of HIV, Viral Hepatitis, STIs 2016. Australian Blood Donors Surveillance Report 2016. Available online: https://kirby.unsw.edu.au/report/annual-surveillance-report-hiv-viral-hepatitis-stis-2016 (accessed on 23 June 2018).
- Family Planning Association. Sexually Transmitted Infections Factsheet. 2016. Available online: https://www.fpa.org.uk/factsheets/sexually-transmitted-infections (accessed on 5 August 2018).
- Boyce, W.; Doherty, M.; Fortin, C.; MacKinnon, D. Canadian Youth, Sexual Health and HIV/AIDS Study: Factors Influencing Knowledge, Attitudes and Behaviours; Council of Ministers of Education, Canada: Toronto, ON, Canada, 2003. Available online: https://www.cmec.ca/Publications/Lists/Publications/Attachments/180/CYSHHAS_2002_EN.pdf (accessed on 5 August 2018).
- Drago, F.; Ciccarese, G.; Zangrillo, F.; Gasparini, G.; Cogorno, L.; Riva, S.; Javor, S.; Cozzani, E.; Broccolo, F.; Esposito, S.; et al. A Survey of Current Knowledge on Sexually Transmitted Diseases and Sexual Behaviour in Italian Adolescents. Int. J. Environ. Res. Public Health 2016, 13, 422. [Google Scholar] [CrossRef] [PubMed]
- von Rosen, F.T.; von Rosen, A.J.; Müller-Riemenschneider, F.; Damberg, I.; Tinnemann, P. STI Knowledge in Berlin Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 110. [Google Scholar] [CrossRef] [PubMed]
- Genuis, S.J.; Genuis, S.K. Managing the sexually transmitted disease pandemic: A time for reevaluation. Am. J. Obstet. Gynecol. 2004, 191, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Canadian Guidelines on Sexually Transmitted Infections. Greece—Where Are You Travelling?—Travel Health—Public Health Agency of Canada. 2018. Available online: https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/sexually-transmitted-infections.html (accessed on 23 June 2018).
- Genuis, S.J. Are condoms the answer to rising rates of non-HIV sexually transmitted infection? No. BMJ 2008, 336, 184–185. [Google Scholar] [CrossRef] [PubMed]
- Kann, L.; McManus, T.; Harris, W.H.; Shanklin, S.L.; Flint, K.H.; Hawkins, J.; Queen, B.; Lowry, R.; Olsen, E.O.; Chyen, D.; et al. Youth Risk Behavior Surveillance—United States, 2015. MMWR Surveill. Summ. 2016, 65, 1–174. [Google Scholar] [CrossRef] [PubMed]
- Alberta Health Services. Teens and Trends: Get the Facts on Teen Sexuality; Sexual & Reproductive Health—Alberta Health Services Calgary Zone: Calgary, AB, Canada, 2014; Available online: https://teachingsexualhealth.ca/wp-content/uploads/sites/4/Teens-and-Trends-CALGARY-20141.pdf (accessed on 24 June 2018).
- Rotermann, M. Sexual behaviour and condom use of 15- to 24-year-olds in 2003 and 2009/2010. Health Rep. 2012, 23, 41–45. [Google Scholar] [PubMed]
- Gaydos, C.; Hardick, J. Point of care diagnostics for sexually transmitted infections: Perspectives and advances. Expert Rev. Anti-Infect. Ther. 2014, 12, 657–672. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sexually Transmitted Infections. Available online: http://apps.who.int/iris/bitstream/handle/10665/112323/WHO_RHR_14.10_eng.pdf;jsessionid=3B5EE62FB75E2C5F7615DEDEC9087B16?sequence=1 (accessed on 23 June 2018).
- Taylor, M.M.; Korenromp, E.; Wi, T. Pathways and progress to enhanced global sexually transmitted infection surveillance. PLoS Med. 2017, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. STDs Increase across the Country for the Third Year. Available online: https://www.cdc.gov/std/stats16/default.htm (accessed on 23 June 2018).
- Fishman, D.N.; Laupland, K.B. Sexually transmitted infections in Canada: A sticky situation. Can. J. Infect. Dis. Med. Microbiol. 2011, 22, 80–82. [Google Scholar] [CrossRef]
- Chapter: Factors That Contribute to the Hidden Epidemic. In The Hidden Epidemic: Confronting Sexually Transmitted Diseases; National Academies Press: Washington, DC, USA, 1997; Available online: https://www.nap.edu/read/5284/chapter/5 (accessed on 28 July 2018).
- Demaria, A. Challenges of sexually transmitted disease prevention and control: No magic bullet, but some bullets would still be appreciated. Clin. Infect. Dis. 2005, 41, 804–807. [Google Scholar] [CrossRef] [PubMed]
- Fenton, K.A. Resurgence of syphilis in England: Time for more radical and nationally coordinated approaches. Sex. Transm. Infect. 2001, 77, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. HIV among Youth. 2017. Available online: https://www.cdc.gov/hiv/group/age/youth/index.html (accessed on 29 January 2018).
- Canadian AIDS Treatment Information Exchange. School-Based Education. The Benefits of HIV Treatment | CATIE—Canada’s Source for HIV and Hepatitis C Information. Available online: https://www.catie.ca/en/hiv-canada/4/4-5/4-5-3 (accessed on 1 July 2018).
- Mason-Jones, A.J.; Crisp, C.; Momberg, M.; Koech, J.; De Koker, P.; Mathews, C. A systematic review of the role of school-based healthcare in adolescent sexual, reproductive, and mental health. Syst. Rev. 2012, 1, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. 2014. Available online: https://www.cdc.gov/healthyyouth/data/profiles/pdf/16_criteria.pdf (accessed on 5 December 2018).
- Australian Government. Department of Health—Third National Sexually Transmissible Infections Strategy 2014–2017. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-bbvs-sti (accessed on 29 January 2018).
- Jones, T.; Mitchell, A. Young People and HIV Prevention in Australian Schools. AIDS Educ. Prev. 2014, 26, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, M.M.; Lim, R.; Langford, C.; Seabrook, J.A.; Speechley, K.N.; Lynch, T. Sexual knowledge of Canadian adolescents after completion of high school sexual education requirements. Paediatr. Child Health 2013, 18, 74–80. [Google Scholar] [PubMed]
- The Ontario Student Trustees’ Association (OSTA-AECO). The Ontario Student, Parent, and Educator Survey. Canada.ca. 2017. Available online: https://www.osta-aeco.org/assets/2017_OSPES_Report.pdf (accessed on 5 December 2018).
- Phillips, K.P.; Martinez, A. Sexual and reproductive health education: Contracting teachers’, health partners’ and former students’ perspective. Can. J. Public Health 2010, 101, 374–379. [Google Scholar] [PubMed]
- Bird, Y.; Solis, L.H.; Mbonu, C.A. Sexual attitudes, norms, condom use, and adherence of Hispanic and non-Hispanic undergraduate students: A cross-sectional study of three community colleges in southwestern US. Patient Prefer Adherence 2016, 10, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Lindong, I.; Edwards, L.; Dennis, S.; Fajobi, O. Similarities and differences matter: Considering the influence of gender on Hiv prevention programs for young adults in an urban HBCU. Int. J. Environ. Res. Public Health 2017, 14, 2. [Google Scholar] [CrossRef]
- Foster, L.R.; Byers, E.S. Predictors of stigma and shame related to sexually transmitted infections: Attitudes, education, and knowledge. Can. J. Hum. Sex. 2008, 17, 193–202. [Google Scholar]
- Rouner, D.; Lindsey, R. Female adolescent communication about sexually transmitted diseases. Health Commun. 2006, 19, 29–38. [Google Scholar] [CrossRef]
- Synovitz, L.; Herbert, E.; Kelley, R.M.; Carlson, G. Sexual knowledge of college students in a southern state: Relationship to sexuality education. Am. J. Health Stud. 2002, 17, 163–172. [Google Scholar]
- Weinstein, R.B.; Walsh, J.L.; Ward, L.M. Testing a new measure of sexual health knowledge and its connections to students’ sex education, communication, confidence and condom use. Int. J. Sex Health 2008, 20, 212–221. [Google Scholar] [CrossRef]
- Viswanathan, M.; Ansari, M.T.; Berkman, N.D.; Chang, S.; Hartling, L.; McPheeters, M.; Santaguida, P.L.; Shamliyan, T.; Singh, K.; Tsertsvadze, A.; et al. Assessing the Risk of Bias of Individual Studies in Systematic Reviews of Health Care Interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews. AHRQ Methods for Effective Health Care; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 8 March 2012. Available online: https://www.ncbi.nlm.nih.gov/books/NBK91433/ (accessed on 4 July 2018).
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Heterogeneity in Meta-Analysis. Prospective, Retrospective, Case-Control, Cohort Studies—Stats Direct. Available online: https://www.statsdirect.com/help/meta_analysis/heterogeneity.htm (accessed on 5 August 2018).
- Roberto, A.J.; Zimmerman, R.S.; Carlyle, K.E.; Abner, E.L. A Computer-based Approach to Preventing Pregnancy, STD, and HIV in Rural Adolescents. J. Health Commun. 2007, 12, 53–76. [Google Scholar] [CrossRef] [PubMed]
- Morales, A.; Espada, J.P.; Orgilés, M. A 1-year follow-up evaluation of a sexual-health education program for Spanish adolescents compared with a well-established program. Eur. J. Public Health 2015, 26, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tortolero, S.R.; Markham, C.M.; Peskin, M.F.; Shegog, R.; Addy, R.C.; Escobar-Chaves, S.L.; Baumler, E.R. It’s Your Game: Keep It Real: Delaying Sexual Behavior with an Effective Middle School Program. J. Adolesc. Health 2010, 46, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, J.B.; Dmochowski, J.; Boyer, C.; Lawrence, J.S.; Lightfoot, M.; Moore, M. Text-Messaging-Enhanced HIV Intervention for African American Adolescents: A Feasibility Study. J. Assoc. Nurses AIDS Care 2013, 24, 256–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronson, R.E.; Rulison, K.L.; Graham, L.F.; Pulliam, R.M.; Mcgee, W.L.; Labban, J.D.; Dingman, D.; Rhodes, S.D. Brothers Leading Healthy Lives: Outcomes From the Pilot Testing of a Culturally and Contextually Congruent HIV Prevention Intervention for Black Male College Students. AIDS Educ. Prev. 2013, 25, 376–393. [Google Scholar] [CrossRef]
- Calloway, D.S.; Long-White, D.N.; Corbin, D.E. Reducing the Risk of HIV/AIDS in African American College Students. Health Promot. Pract. 2014, 15, 181–188. [Google Scholar] [CrossRef]
- Espada, J.P.; Orgilés, M.; Morales, A.; Ballester, R.; Huedo-Medina, T.B. Effectiveness of a School HIV/AIDS Prevention Program for Spanish Adolescents. AIDS Educ. Prev. 2012, 24, 500–513. [Google Scholar] [CrossRef] [Green Version]
- Gaydos, C.A.; Hsieh, Y.H.; Galbraith, J.S.; Barnes, M.; Waterfield, G.; Stanton, B. Focus-on-Teens, sexual risk-reduction intervention for high-school adolescents: Impact on knowledge, change of risk-behaviours, and prevalence of sexually transmitted diseases. Int. J. STD AIDS 2008, 19, 704–710. [Google Scholar] [CrossRef]
- Lemieux, A.; Fisher, J.; Pratto, F. Reaching (and not preaching to) adolescents: A music-based HIV prevention intervention. Health Psychol. 2008, 27, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Hlavinkova, L.; Mentel, A.; Kollarova, J.; Kristufkova, Z. Effectiveness of a prevention campaign on HIV/AIDS knowledge among adolescents in Eastern Slovakia. Int. J. Public Health 2014, 59, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Gold, J.; Lim, M.S.; Hocking, J.S.; Keogh, L.A.; Spelman, T.; Hellard, M.E. Determining the Impact of Text Messaging for Sexual Health Promotion to Young People. Sex. Transm. Dis. 2011, 38, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Stanton, B. Teachers’ Patterns of Implementation of an Evidence-Based Intervention and Their Impact on Student Outcomes: Results from a Nationwide Dissemination over 24-Months Follow-Up. AIDS Behav. 2015, 19, 1828–1840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ateka, G.K. Evaluation of the City of Houston HIV/STD Prevention Program in Houston Independent School District (HISD) High Schools; The University of Texas Health Science Center at Houston School of Public Health: Houston, TX, USA, August 2006; Available online: https://digitalcommons.library.tmc.edu/dissertations/AAI3241393/ (accessed on 5 August 2018).
- O’Grady, M.A.; Wilson, K.; Harman, J.J. Preliminary findings from a brief, peer-led safer sex intervention for college students living in residence halls. J. Prim. Prev. 2009, 30, 716–731. [Google Scholar] [CrossRef] [PubMed]
- Peskin, M.F.; Shegog, R.; Markham, C.M.; Thiel, M.; Baumler, E.R.; Addy, R.C.; Gabay, E.K.; Emery, S.T. Efficacy of Its Your Game-Tech: A Computer-Based Sexual Health Education Program for Middle School Youth. J. Adolesc. Health 2015, 56, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Mahat, G.; Scoloveno, M.A.; Leon, T.D.; Frenkel, J. Preliminary Evidence of an Adolescent HIV/AIDS Peer Education Program. J. Pediatr. Nurs. 2008, 23, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.D.; Fisher, W.A.; Misovich, S.J.; Kimble, D.L.; Malloy, T.E. Changing AIDS risk behavior: Effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population. Health Psychol. 1996, 15, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Sadovszky, V.V.; Draudt, B.; Boch, S. A Systematic Review of Reviews of Behavioral Interventions to Promote Condom Use. Worldviews Evid. Based Nurs. 2014, 11, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Is Our Sexual Double Standard Going Away? Psychology Today. Sussex Publishers. Available online: https://www.psychologytoday.com/us/blog/strictly-casual/201403/is-our-sexual-double-standard-going-away (accessed on 5 August 2018).
- Lefkowitz, E.S.; Shearer, C.L.; Gillen, M.M.; Espinosa-Hernandez, G. Advances in pediatrics. U.S. National Library of Medicine, 2014. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4244004/ (accessed on 5 August 2018).
- Sexually Transmitted Diseases. Heart Disease and Stroke | Healthy People 2020. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/sexually-transmitted-diseases (accessed on 8 July 2018).
- STD Prevention D. Program Operations Guidelines for STD Prevention. Available online: https://www.cdc.gov/std/program/community.pdf (accessed on 30 July 2018).
- Advocates for Youth. Available online: http://www.advocatesforyouth.org/publications/publications-a-z/1855-creating-a-strong-a-successful-peer-sexual-health-program (accessed on 5 August 2018).
- Tolli, M.V. Effectiveness of peer education interventions for HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people: A systematic review of European studies. Health Educ. Res. 2012, 27, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.R.; Free, C. Recent evaluations of the peer-led approach in adolescent sexual health education: A systematic review. Perspect. Sex. Reprod. Health 2008, 40, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Ergene, T.; Cok, F.; Tumer, A.; Unal, S. A controlled-study of preventative effects of peer education and single-session lectures on HIV/AIDS knowledge and attitudes among university students in Turkey. AIDS Educ. Prev. 2005, 17, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Kauth, M.R.; Christoff, K.A.; Sartor, J.; Sharp, S. HIV sexual risk reduction among college women: Applying a peer influence model. J. Coll. Stud. Dev. 1993, 34, 346–351. [Google Scholar]
- Kauffman, C.; Hue, L. Sustaining youth peer HIV/STD prevention education. AIDS STD Health Promot. Exch. 1997, 3, 3–7. [Google Scholar]
- Noar, S.M.; Black, H.G.; Pierce, L.B. Efficacy of computer technology-based HIV prevention interventions: A meta-analysis. AIDS 2009, 23, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.V.; Murray, E.; Rait, G.; Mercer, C.H.; Morris, R.W.; Peacock, R.; Cassell, J.; Nazareth, I. Interactive computer-based interventions for sexual health promotion. Cochrane Database Syst. Rev. 2010, 9, CD006483. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. The Chief Public Health Officer’s Report on the State of Public Health in Canada 2014—Digital Technology as a Tool for Public Health. Canada.ca. 2014. Available online: https://www.canada.ca/en/public-health/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/chief-public-health-officer-report-on-state-public-health-canada-2014-public-health-future/digital-technology-as-a-tool-for-public-health.html (accessed on 5 August 2018).
- Allison, S.; Bauermeister, J.A.; Bull, S.; Lightfoot, M.; Mustanski, B.; Shegog, R.; Levine, D. The intersection of youth, technology, and new media with sexual health: Moving the research agenda forward. J. Adolesc. Health 2012, 51, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Valaitis, R.; Hunter, D.; Lam, A.; Murray, N. Technology to Encourage the Adoption of Health Promoting/Protecting Behaviours: A Comprehensive Literature Review; Public Health Agency of Canada: Ottawa, ON, Canada, Feburary 2014; unpublished. [Google Scholar]
- Kachur, R.; Mesnick, J.; Liddon, N. Adolescents, Technology and Reducing Risk for HIV, STDs and Pregnancy. 2013. Available online: https://www.cdc.gov/std/life-stages-populations/Adolescents-white-paper.pdf (accessed on 4 July 2018).
- Cassell, M.M.; Jackson, C.; Cheuvront, B. Health communication on the internet: An effective channel for health behaviour change? J. Health Commun. 1998, 3, 71–79. [Google Scholar]
- Bickmore, T.; Giorgino, T. Health dialog systems for patients and consumers. J. Biomed. Inform. 2006, 39, 556–571. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Articles | Bias | Within Studies Risk of Bias | ||||
|---|---|---|---|---|---|---|
| Selection | Performance | Attrition | Detection | Reporting | ||
| Roberto et al., 2007 [48] | + | + | + | + | + | Low risk of bias |
| Morales et al., 2015 [49] | + | − | + | + | + | Low risk of bias |
| Tortolero et al., 2010 [50] | + | − | + | + | + | Low risk of bias |
| Cornelius et al., 2013 [51] | + | − | + | + | + | Low risk of bias |
| Aronson et al., 2013 [52] | − | − | + | + | + | Moderate risk of bias |
| Calloway et al., 2013 [53] | − | − | + | + | + | Moderate risk of bias |
| Espada et al., 2012 [54] | + | − | + | + | − | Moderate risk of bias |
| Gaydos et al., 2008 [55] | + | − | + | − | + | Moderate risk of bias |
| Lemieux et al., 2008 [56] | + | − | + | − | + | Moderate risk of bias |
| Hlavinkova et al., 2014 [57] | − | − | + | + | + | Moderate risk of bias |
| Gold et al., 2010 [58] | + | − | + | − | + | Moderate risk of bias |
| Stanton et al., 2015 [59] | + | − | + | + | − | Moderate risk of bias |
| Ateka et al., 2007 [60] | + | − | − | − | + | High risk of bias |
| O’Grady et al., 2009 [61] | + | − | − | − | + | High risk of bias |
| Peskin et al., 2015 [62] | + | − | + | − | − | High risk of bias |
| Mahat et al., 2008 [63] | − | − | − | + | + | High risk of bias |
| Author, Year of Publication, and Location | Interventions | Settings | Study | ||||
|---|---|---|---|---|---|---|---|
| Type | Providers | Study Design | Control | Evaluation | Characteristics of Participants | ||
| Roberto et al. [48] U.S. 2007 | Computer and internet-based intervention addressing pregnancy, HIV and STIs * | No in-person provider | High school | Pretest post-test control group design (randomization at school level) | No intervention | Baseline and 10 weeks after intervention | N = 326 Mean age—15.5 Sex—male and female Ethnicity—European American (majority) |
| Morales et al. [49] Spain 2015 | Culturally adapted HIV prevention and sexual health promotion program for Latino adolescents: “COMPAS (Skills for Adolescents with a Healthy Sexuality)” | Trained psychologists | High school | Pretest post-test control group design (randomization at school level) | No intervention | Baseline and 1 year after intervention | N = 1563 Mean age—14–16 Sex—male and female Ethnicity—Spanish |
| Tortolero et al. [50] U.S. 2010 | Computer-based plus classroom activities for HIV, STIs, and pregnancy prevention: “IYG (Its Your Game … Keep It Real!)” | Trained facilitators | Middle school | Pretest post-test control group design (randomization at school level) | Regular health classes | Baseline and 1 year after intervention | N = 907 Mean age—13 Sex—male and female Ethnicity—African American |
| Cornelius et al. [51] U.S. 2013 | Community-based HIV prevention program boosted with mobile cell phone (MCP) technology: “Becoming A Responsible Team (BART) curriculum” | Trained African American college graduate facilitators (peers) | Pilot study at university, participated by high school students | Pretest post-test treatment group only design | Baseline | Baseline, immediately, and 3 months after intervention | N = 40 Mean age—15.4 Sex—male and female Ethnicity—African American |
| Aronson et al. [52] U.S. 2013 | HIV preventive intervention for black male college students: “Brothers Leading Healthy Lives” | Trained peer facilitators and educators | College | Pretest post-test treatment group only design | Baseline | Baseline, immediately, and 3 months after intervention | N = 54 Age range—18–24 Sex—male Ethnicity—African American |
| Calloway et al. [53] U.S. 2013 | Preventive intervention addressing HIV and STIs for African American college students: “Playing it Safe: Protecting yourself from HIV/AIDS and other STIs” | Trained and certified peer educators | College | Pretest post-test control group design (randomization at class level) | No intervention | Baseline, immediately after intervention | N = 97 Mean Age—18 Sex—male and female (female 79%) Ethnicity—African American (majority) |
| Espada et al. [54] Spain 2012 | Culturally adapted HIV prevention and sexual health promotion program for Latino adolescents: “COMPAS (Skills for Adolescents with a Healthy Sexuality)” | Trained psychologists | High school | Pretest post-test control group design (randomization at school level) | No intervention | Baseline and immediately after intervention | N = 827 Mean age—15.73 Sex—male and female Ethnicity—Spanish |
| Gaydos et al. [55] U.S. 2008 | Community–university linked research and interventions addressing HIV and STIs: “Focus on Adolescents (FOA): modification of “Focus on Teens (FOT)” | Trained adult interventionists | High school | Pretest post-test treatment only group design (randomization at school level) | Baseline | Baseline, immediately, 6 months and 1 year after intervention | N = 1190 Mean age—14.9 Sex—male and female (female > 70%) Ethnicity—African American |
| Lemieux et al. [56] U.S. 2008 | Music-based HIV preventive intervention | Music Opinion Leaders (MOLs) (peers) | High school | Pretest post-test control group design (randomization at school level) | Regular health classes | Baseline and 3 months after intervention | N = 306 Mean age—16 Sex—male and female Ethnicity—multi-ethnicity (predominantly African American and Latinos) |
| Hlavinkova et al. [57] Slovakia 2014 | HIV prevention campaign: “Sunflower project” | Students organised, designed, and created contents of the campaign (peers) | High school and college | Pretest post-test treatment group only design | Baseline | Baseline and immediately after campaign | N = 533 Mean age—15.8 Sex—male and female Ethnicity—multi-ethnicity |
| Gold et al. [58] Australia 2010 | Sexual health promotion with text messaging focusing on chlamydia screening and condom use | No in-person provider is needed; researchers, professors, and students were involved in the study | No physical setting (most participants are high school graduates) | Pretest post-test treatment group only design | Baseline | Baseline and 2 weeks after intervention | N = 587 Median age—22 Sex—male and female Ethnicity—not mentioned |
| Stanton et al. [59] Bahamas 2015 | National evidence-based HIV prevention program for 6th grade students: “Focus on Youth in the Caribbean (FOYC)” | Trained teachers | Elementary school | Pretest post-test treatment group only design | Baseline | Baseline, immediately, and 1 year after intervention | N = 4470 (6th grade students) Mean age—10.4 Sex—male and female Ethnicity—African descendants (majority) |
| Ateka et al. [60] U.S. 2007 | Knowledge-based adolescent sexuality program: “City of Houston HIV and STD prevention program” | Trained teachers | High school | Intervention and control comparison at post-test only | Regular health classes | Compare the data of intervention and control schools over 1 academic year | N = 430 Mean age—15.3 Sex—male and female Ethnicity—African American and Hispanics (Majority) |
| O’Grady et al. [61] U.S. 2009 | Brief safe sex intervention for college students residing in residence halls: “Skills, Information, Motivation, Peer-led (SIMPL)” | Trained peer educators | College | Intervention and control comparison at post-test only | Information only | Immediately after sessions | N = 108 Mean age—18.85 Sex—male and female Ethnicity—White (majority) |
| Peskin et al. [62] U.S. 2015 | Computer-based sexual health education addressing pregnancy, HIV, and STIs: “IYG tech (Its Your Game … Keep It Real!)” | Trained facilitators | Middle school | Pretest post-test control group design (randomization at school level) | No intervention | Baseline and 1 year after intervention | N = 1374 Mean age—14.3 Sex—male and female Ethnicity—Hispanic (74%), African American (17%), others (9%) |
| Mahat et al. [63] U.S. 2008 | Peer Education Project (PEP) for HIV prevention: “Teens for AIDS Prevention (TAP)” | Trained peer educators (guided by nurses and teachers) | High school | Pre-test post-test control group design (no randomization) | Traditional sexual health education | Baseline and 5 months after intervention | N = 97 Mean age—14 Sex—male and female Ethnicity—multi-ethnicity |
| Outcome Measures | # of Studies | Pooled OR | Lower Limit | Upper Limit | Heterogeneity | |
|---|---|---|---|---|---|---|
| I2 | p-Value (Q Statistics) | |||||
| Behavioral outcomes | 10 | 1.28 | 1.17 | 1.39 | 0.00 | 0.648 |
| Sexual partners | 7 | 1.33 | 1.03 | 1.72 | 86.69 | 0.00 |
| Sexual activity | 8 | 1.06 | 0.86 | 1.31 | 64.72 | 0.01 |
| Condom use | 5 | 1.57 | 0.91 | 2.73 | 68.42 | 0.01 |
| HIV or STI testing | 1 | 1.26 | 0.93 | 1.72 | - | - |
| Alcohol or drug use before sex | 1 | 1.00 | 0.22 | 4.45 | - | - |
| Psychosocial outcomes | 16 | 1.92 | 1.36 | 2.72 | 96.95 | 0.00 |
| Information (knowledge) | 14 | 3.17 | 2.13 | 4.72 | 97.12 | 0.00 |
| Motivation | 13 | 1.69 | 1.04 | 2.75 | 98.67 | 0.00 |
| Attitude: condom use, abstinence | 6 | 1.37 | 1.10 | 1.69 | 56.63 | 0.04 |
| Norms and beliefs: condom | 4 | 1.42 | 1.00 | 2.04 | 70.78 | 0.02 |
| Norms and beliefs: abstinence | 2 | 1.16 | 1.03 | 1.30 | 0.00 | 0.96 |
| Norms and beliefs: peers | 4 | 1.07 | 0.96 | 1.19 | 0.00 | 0.70 |
| Risk perceptions | 4 | 2.06 | 0.66 | 6.48 | 98.98 | 0.00 |
| Intentions (preventive behaviors) | 10 | 1.68 | 0.97 | 2.9 | 99.00 | 0.00 |
| Behavioral skills | 9 | 1.43 | 1.13 | 1.81 | 89.91 | 0.00 |
| Condom efficacy | 6 | 1.44 | 1.11 | 1.87 | 89.20 | 0.00 |
| Refusal self-efficacy | 3 | 1.15 | 0.92 | 1.45 | 63.43 | 0.07 |
| HIV self-efficacy | 2 | 1.62 | 1.12 | 2.35 | 0.00 | 0.83 |
| Partner communication | 3 | 1.24 | 1.04 | 1.26 | 0.00 | 0.46 |
| Parental communication | 2 | 1.17 | 1.08 | 1.26 | 0.00 | 0.33 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mon Kyaw Soe, N.; Bird, Y.; Schwandt, M.; Moraros, J. STI Health Disparities: A Systematic Review and Meta-Analysis of the Effectiveness of Preventive Interventions in Educational Settings. Int. J. Environ. Res. Public Health 2018, 15, 2819. https://doi.org/10.3390/ijerph15122819
Mon Kyaw Soe N, Bird Y, Schwandt M, Moraros J. STI Health Disparities: A Systematic Review and Meta-Analysis of the Effectiveness of Preventive Interventions in Educational Settings. International Journal of Environmental Research and Public Health. 2018; 15(12):2819. https://doi.org/10.3390/ijerph15122819
Chicago/Turabian StyleMon Kyaw Soe, Nway, Yelena Bird, Michael Schwandt, and John Moraros. 2018. "STI Health Disparities: A Systematic Review and Meta-Analysis of the Effectiveness of Preventive Interventions in Educational Settings" International Journal of Environmental Research and Public Health 15, no. 12: 2819. https://doi.org/10.3390/ijerph15122819
APA StyleMon Kyaw Soe, N., Bird, Y., Schwandt, M., & Moraros, J. (2018). STI Health Disparities: A Systematic Review and Meta-Analysis of the Effectiveness of Preventive Interventions in Educational Settings. International Journal of Environmental Research and Public Health, 15(12), 2819. https://doi.org/10.3390/ijerph15122819