Factors Influencing Abortion Decision-Making Processes among Young Women



Abstract
:1. Introduction
2. Materials and Methods
2.1. Location of the Study
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Consideration
2.5. Concepts
3. Results
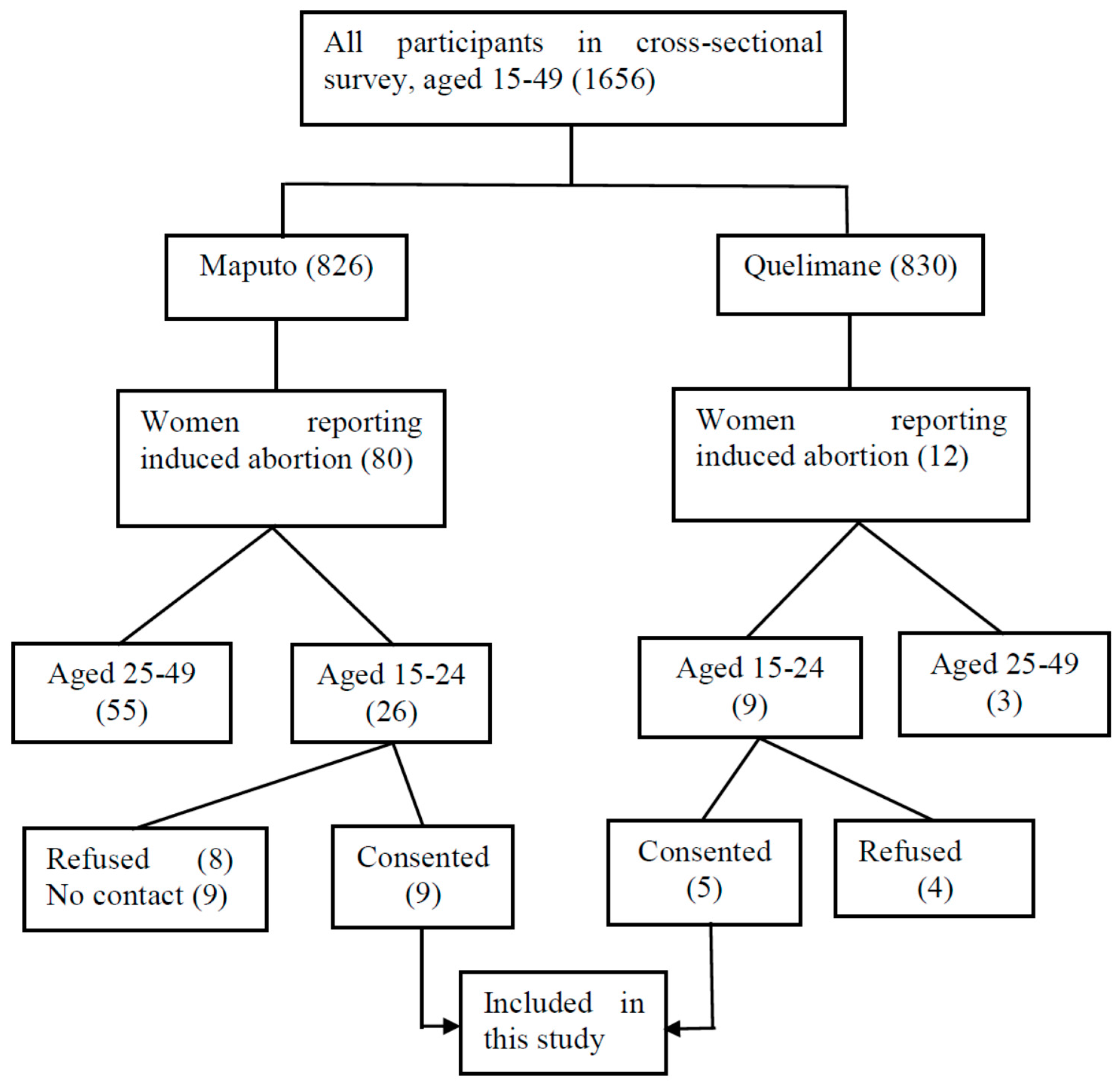
3.1. Characteristics of the Participants
3.2. Abortions Stories
3.3. Abortion Following an Unwanted Pregnancy
3.4. Abortion Following a Wanted Pregnancy
3.5. Location of the Abortion: Home-Based Versus Hospital-Based
3.6. Abortion Procedure
3.7. Legal Procedure
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Guttmacher Institute. In Brief: Facts on the Sexual and Reproductive Health of Adolescent Women in the Developing World Context. Available online: http://www.guttmacher.org/pubs/FB-Adolescents-SRH.pdf (accessed on 23 October 2015).
- Shah, I.H.; Åhman, E. Unsafe abortion differentials in 2008 by age and developing country region: High burden among young women. Reprod. Health Matters 2012, 20, 169–173. [Google Scholar] [CrossRef]
- Ustá, M.B. O Problema do Aborto Inseguro. Outras Vozes. Available online: www.wlsa.org.mz/wp.../11/O-problema-do-aborto-inseguro.pdf (accessed on 3 March 2016).
- Hess, R.F. Women’s Stories of Abortion in Southern Gabon, Africa. J. Transcult. Nurs. 2007, 18, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Ahman, E.; Shah, I. Unsafe Abortion : Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2003, 5th ed.; World Health Organisation: Geneva, Switzerland, 2007; ISBN 978-92-4-159612-1. [Google Scholar]
- Ahman, E.; Shah, I. Unsafe Abortion: Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2000, 4th ed.; World Health Organization: Geneva, Switzerland, 2004; ISBN 92-4-159180-3. [Google Scholar]
- UNFPA. Girlhood, Not Motherhood: Preventing Adolescent Pregnancy; UNFPA: New York, USA, 2015; ISBN 978-0-89714-986-0. Available online: www.unfpa.org (accessed on 22 June 2017).
- Ahman, E.; Shah, I. Unsafe Abortion: Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2008, 6th ed.; World Health Organization: Geneva, Switzerland, 2011; ISBN 978-92-4-150111-8. [Google Scholar]
- Alhassan, A.Y.; Abdul-Rahim, A.; Akaabre, P.B. Knowledge, Awareness and Perceptions of Females on Clandestine Abortion in Kintampo North Municipality, Ghana. Eur. Sci. J. 2016, 12, 95–112. [Google Scholar]
- Gbagbo, F.Y.; Amo-Adjei, J.; Laar, A. Decision-Making for Induced Abortion in the Accra Metropolis, Ghana. Afr. J. Reprod. Health 2015, 19, 34–42. [Google Scholar] [PubMed]
- Olukoya, P. Reducing Maternal Mortality from Unsafe Abortion among Adolescents in Africa. Afr. J. Reprod. Health 2004, 8, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Plummer, M.L.; Wamoyi, J.; Nyalali, K.; Mshana, G.; Zachayo, S.; Ross, D.A.; Wight, D. Aborting and Suspending Pregnancy in Rural Tanzania: An Ethnography of Young People’s Beliefs and Practices. Stud. Fam. Plan. 2008, 39, 281–292. [Google Scholar] [CrossRef]
- Lim, L.; Wong, H.; Yong, E.; Singh, K. Profiles of Women Presenting for Abortions in Singapore: Focus on Teenage Abortions and Late Abortions. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Kabiru, C.W.; Ushie, B.A.; Mutua, M.M.; Izugbara, C.O. Previous induced abortion among young women seeking abortion-related care in Kenya : A cross-sectional analysis. BMC Pregnancy Childbirth 2016. [Google Scholar] [CrossRef] [PubMed]
- Ustá, M.B.; Mitchell, E.M.; Gebreselassie, H.; Brookman-Amissah, E.; Kwizera, A. Who is Excluded When Abortion Access is Restricted to Twelve Weeks? Evidence from Maputo, Mozambique. Reprod. Health Matters 2008, 16, 14–17. [Google Scholar] [CrossRef]
- Agadjanian, V. “Quasi-Legal” Abortion Services in a Sub-Saharan Setting: Users’ Profile and Motivations. Int. Fam. Plan. Perspect. 1998, 24, 111–116. [Google Scholar] [CrossRef]
- Machungo, F.; Zanconato, G.; Bergstrom, S. Reproductive Characteristics and Post- Abortion Health Consequences in Women Undergoing Illegal and Legal Abortion in Maputo. Soc. Sci. Med. 1997, 45, 1607–1613. [Google Scholar] [CrossRef]
- Hardy, E.; Bugalho, A.; Faúndes, A.; Duarte, G.A.; Bique, C. Comparison of Women Having Clandestine and Hospital abortions: Maputo, Mozambique. Reprod. Health Matters 1997, 9, 108–115. [Google Scholar] [CrossRef]
- Assembleia da República. Boletim da República: Lei No. 35/2014 de 31 de Dezembro. 14.o Suplemento Imprensa. Maputo, Mocambique; Report No. 105; 2014. Available online: http://www.wlsa.orgmz/wp-content/uploads/2014/11/lei-35_2014Codigo_Penal.pdf (accessed on 3 June 2015).
- Ministério da Saúde. Boletim da República: Diploma Ministerial No. 60/2017 de 20 de Setembro. Maputo, Moçambique; (I). Report No. 147; 2017. Available online: www.wlsa.org.mz/wp-content/.../Diploma_ministerial_60-2017.pdf (accessed on 20 October 2017).
- Cockrill, K.; Upadhyay, U.D.; Turan, J.; Foster, D.G. The Stigma of Having an Abortion: Development of a Scale and Characteristics of Women Experiencing Abortion Stigma. Perspect. Sex. Reprod. Health 2013, 45, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Hessini, L.; Mitchell, E.M.H. Conceptualising abortion stigma. Culture Health Sex. 2009, 11, 625–639. [Google Scholar] [CrossRef] [PubMed]
- Singh, S. Hospital Admissions Resulting from Unsafe Abortion: Estimates from 13 Developing Countries. Lancet 2006, 368, 1887–1892. [Google Scholar] [CrossRef]
- Ministério da Saude (MISAU); Instituto Nacional de Estatística (INE). Inquérito Demográfico e de Saúde 2011; Instituto Nacional de Estatística (INE): Maputo, Moçambique, 2013.
- Associação Mocambiçana Para Desenvolvimento da Família (AMODEFA). Estatisticas de Serviços Prestados em Saúde Sexual e Reproductiva; AMODEFA: Maputo, Moçambique, 2017. [Google Scholar]
- Direcção Nacional de Planificação. Relatório Nacional do Ministério da Saúde; Direcção Nacional de Planificação: Maputo, Moçambique, 2014.
- World Health Organization. Studying Unsafe Abortion: A Practical Guide; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Cleland, J.; Ingham, R.; Stone, N. Asking Young People about Sexual and Reproductive Behaviours: Illustrative Core Instruments; Special Programme of Research, Development and Research Training in Human Reproduction; UNP: Sri Jayawardenapura, Sri Lanka; UNFPA: New York, NY, USA; WHO: Geneva, Switzerland; World Bank: Washington, DC, USA, 2001. [Google Scholar]
- Creswell, J.W. Research Design Qualitative Quantitative and Mixed Methods Approach, 2nd ed.; SAGE Publications, Incorporated: London, UK, 2003; ISBN 0-7619-2441-8 (c). [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed.; Basics of Qualitative Research Grounded Theory Procedures and Techniques; SAGE: London, UK, 1998; ISBN 0-8039-5939-7. [Google Scholar]
- Bronfenbrenner, U. Ecological Model of Human Development. In International Encyclopedia of Education, 2nd ed.; Elsevier: Oxford, UK, 1994; Volume 3. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979; ISBN 0-674-22456-6. [Google Scholar]
- Gerhardt, T.E.; Silveira, D.T. Métodos de Pesquisa, 1st ed.; Universidade Federal do Rio Grande do Sul: Porto Alegre, Brazil, 2009; ISBN 9788538600718. [Google Scholar]
- John, O.L. Power Dynamics, Gender Relations and Decision-Making Regarding Induced Abortion among University Students in Nigeria. Afr. Popul. Stud. 2017, 31, 3324–3332. [Google Scholar]
- John, O.L. Sexual Behaviour, Unwanted Pregnancy and Tripartite Levels of Decision-Making Regarding Induced. Afr. J. Psychol. Study Soc. Issues 2016, 19, 61–89. [Google Scholar]
- Ezeah, P.; Chinyere, A. Gender Inequality in Reproductive Health Services and Sustainable Development in Nigeria: A Theoretical Analysis. Int. J. Sociol. Anthropol. 2015, 7, 46–53. [Google Scholar]
- Letamo, G. The Influence of Gender Role Attitudes on Risky Sexual Behaviour: Evidence from the 2008 Botswana AIDS Impact Survey III. Afr. Popul. Stud. 2011, 25, 402–418. [Google Scholar]
- Shearer, C.L.; Hosterman, S.J.; Gillen, M.M.; Lefkowitz, E.S. Are Traditional Gender Role Attitudes Associated with Risky Sexual Behavior and Condom-Related Beliefs? Sex Roles 2005, 52, 311–324. [Google Scholar] [CrossRef]
- Rollins, B.C.; Bahr, S. A Theory of Power Relationships in Marriage. J. Marriage Fam. 1976, 38, 619–627. [Google Scholar] [CrossRef]
- Amaro, H. Love, Sex, and Power: Considering Women’s Realities in HIV Prevention. Am. Psychol. 1995, 50, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Ngwena, C. Inscribing Abortion as a Human Right: Significance of the Protocol on the Rights of Women in Africa. Hum. Rights Q. 2010, 32, 783–864. [Google Scholar] [CrossRef]
- USAID. Avaliação da Corrupção: Moçambique. Relatório Final; December 2005. Available online: www pdf.usaid.gov/pdf_docs/Pnadg268.pdf (accessed on 25 October 2017).
- Ngwena, C. Using Human Rights to Combat Unsafe Abortion: What needs to be Done? Available online: www1.chr.up.ac.za/africlaw/charles_ngwenya.pdf (accessed on 25 October 2017).
- Doran, F.; Nancarrow, S. Barriers and facilitators of access to first-trimester abortion services for women in the developed world: A systematic review. J. Fam. Plan. Reprod. Health Care 2015, 41, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Pickles, C. Lived Experiences of the Choice on Termination of Pregnancy Act 92 of 1996: Bridging the Gap for Women in Need. South Afr. J. Hum. Rights 2013, 29, 515–535. [Google Scholar] [CrossRef]
- Mantshi, E.T.; Laetitia, C.R. “I am all alone”: Factors influencing the provision of termination of pregnancy services in two South African provinces. Glob. Health Action 2017, 10, 1–10. [Google Scholar] [CrossRef]
- Ngwena, C. The Recognition of Access to Health Care as a Human Right in South Africa: Is It Enough? Health Hum. Rights 2000, 5, 26–44. [Google Scholar] [CrossRef] [PubMed]
- Braam, T.; Hessini, L. The Power Dynamics Perpetuating Unsafe Abortion in Africa: A Feminist Perspective. Afr. J. Reprod. Health 2004, 8, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Chandra-Mouli, V.; Svanemyr, J.; Amin, A.; Fogstad, H.; Say, L.; Girard, F.; Temmerman, M. Twenty Years After International Conference on Population and Development: Where Are We With Adolescent Sexual and Reproductive Health and Rights? J. Adolesc. Health 2015, 56, S1–S6. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics of Respondents | Categories | Median/Number |
|---|---|---|
| Age (median, range) | - | 21 (min: 17; max: 24) |
| Age at sexual activity onset (median, range) | - | 15.5 (min: 14; max: 18) |
| Education attainment (number) | Primary school | 4 |
| Secondary School | 8 | |
| University | 2 | |
| Religion (number) | Catholic + Evangelic | 13 |
| Muslim | 1 | |
| Occupation (number) | Studying | 5 |
| Without occupation | 8 | |
| Vendor | 1 | |
| Abortion procedure | Number of clients | |
| Provider characteristics | Skilled | 12 |
| Unskilled | 2 | |
| Location of abortion | Health facility | 7 |
| Outside of health facility | 7 | |
| Treatment for abortion | Pills | 5 |
| Aspiration/curettage | 8 | |
| Traditional medicine | 1 | |
| Followed legal procedure | Yes | 0 |
| No | 14 |
| Abortion Stories | Personal | Interpersonal | Environmental |
|---|---|---|---|
| Unwanted pregnancy (5 + 1 *) | Unable to be a mother | Lack of support | The result of rape |
| Had a bad past experience | |||
| Has another child | |||
| Wanted to study | |||
| Financial problems | |||
| Felt depressed | |||
| Abortion although pregnancy is wanted (7) | Partner did not recognize the child | ||
| Convinced by sister | |||
| Afraid of being sent away | |||
| Convinced/forced by mother | |||
| Partner did not want the child | |||
| Partner’s behaviour changed | |||
| Partner was married | |||
| Unskilled provider (2) | Carried out by partner Carried out by mother | ||
| Abortion outside hospital (8) | Unaware of legal obligations | Provider told us to go to his home | Abortion services are not available in the local healthcare settings |
| Lack of money | Fear of signing a document | ||
| Abortion at home (2) | Mother said that they would kill me at hospital | ||
| Decided by partner | |||
| Technical procedure | Decided by provider (aspiration, curettage **, pills ***) | ||
| Husband gave traditional medicine (1) | |||
| Why the legal procedure is not followed in the hospital (6) | Provider did not inform us about it | Information about legal procedures was not available |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frederico, M.; Michielsen, K.; Arnaldo, C.; Decat, P. Factors Influencing Abortion Decision-Making Processes among Young Women. Int. J. Environ. Res. Public Health 2018, 15, 329. https://doi.org/10.3390/ijerph15020329
Frederico M, Michielsen K, Arnaldo C, Decat P. Factors Influencing Abortion Decision-Making Processes among Young Women. International Journal of Environmental Research and Public Health. 2018; 15(2):329. https://doi.org/10.3390/ijerph15020329
Chicago/Turabian StyleFrederico, Mónica, Kristien Michielsen, Carlos Arnaldo, and Peter Decat. 2018. "Factors Influencing Abortion Decision-Making Processes among Young Women" International Journal of Environmental Research and Public Health 15, no. 2: 329. https://doi.org/10.3390/ijerph15020329
APA StyleFrederico, M., Michielsen, K., Arnaldo, C., & Decat, P. (2018). Factors Influencing Abortion Decision-Making Processes among Young Women. International Journal of Environmental Research and Public Health, 15(2), 329. https://doi.org/10.3390/ijerph15020329