3.1. LCA Results of Health Behaviors in Chinese Elderly
In this study, LatentGold4.5 was used to conduct an exploratory LCA of manifest variables of the health behaviors in CLHLS in 2005, 2008, 2011 and 2014 and to determine whether there are latent class variables with a significant explanatory power among the manifest variables of health behaviors in all waves. Based on manifest variables of the health behaviors in each wave, six latent class models were constructed from a Null model with only one class. The LCA fit indexes of each wave survey (see
Table 3) demonstrates that, among the manifest health behaviors in all four waves, there exists the latent variable of health behaviors in the Chinese elderly. In addition, the BIC value was used as the main fit index to determine model fitness. Relative to models in all the waves, Model 5 is the best model.
According to the conditional probability (horizontally or vertically) of health behavior variables in LCA, and its possible impact directions (“+” or “−“) on the health of the elderly (see
Appendix A Table A1), the health behaviors in each wave can be grouped into five classes: Negative, relatively negative, fair, relatively positive, and positive.
Table 4 presents the latent class probability for Chinese elderly’s health behaviors in each wave survey.
3.2. Evolution Results of Health Behaviors in Chinese Elderly
The evolution of health behaviors generally has three trends: better, unchanged, and worse. Interactive analysis was first used to describe the results of the health behaviors in the elderly in our study. As shown in
Table 5, from 2005 to 2014, the health behaviors in the Chinese elderly are generally changing in a more positive trend. However, it is acknowledged that to determine the evolutionary trends of the health behaviors in the elderly based only on the classes at the beginning and end of the wave may be biased, as this approach does not consider the adjustment of health behaviors over the course of the decade. Moreover, this practice could also not clearly present the evolutionary trends of elderly’s health behaviors. In view of this point, based on the 4 wave panel data over ten years of elderly’s health behaviors, three GMMs were established by using Mplus7.0 (
https://www.statmodel.com/verhistory.shtml). The fit indexes of each model are shown in
Table 6. Except for the Null Model with only one class in the three models, the BIC of Model 2 is the smallest, thus it is the optimal model. While Model 3 classifies the evolution of elderly’s health behaviors into three classes, one of the health behaviors’ evolution classes accounts for only 1.9% of the sample size (approximately 52 people), and the evolutionary trend is not highly differentiated from other classes. Considering all of these factors, Model 2 was the optimal model.
The estimated values of the intercept factors and the slope factors corresponding to GMM are presented in
Table 7. The mean of the intercept factors and the slope factors was −3.261 (
p < 0.01) and 0.278 (
p < 0.01) in class 1, 0 and −0.130 (
p < 0.01) in class 2. By comparing the mean of the slope factors of the two classes, it can be found that the evolutionary trend of the health behaviors type represented by class 1 is increasing and that of class 2 is decreasing. This study has uniformly adjusted the health behaviors variables generated by the LCA. That is, the higher the value represented, the better the health behavior type. It can be inferred that in class 1, health behaviors over 10 years have been optimized, and health behaviors in class 2 remained unchanged. As the results of the health behaviors’ evolution can generally be divided into three classes of better, unchanged, and worse, it can be concluded that class 2 represents a trend towards worse or unchanged over the past decade.
The essence of behavior modification is the use of theories of learning to deal with the individual behaviors, emotions and other aspects for treatment. The goal of behavior modification includes not only eliminating the specific bad behaviors of the individual but also cultivating and developing good behaviors [
35,
36]. Considering all the theoretical and quantitative significance of the evolutionary outcomes of the two classes of health behaviors, it can be inferred that Class 1 represents a positive type of evolution defined as “modified”, which accounts for approximately 77.2% of the total sample size; Class 2 stands for the class of health behaviors whose evolutionary trend is negative or unchanged, which is defined as “non-modified”, accounting for approximately 22.8% of the total sample size.
To be more rigorous and scientific, this study set the classes of health behaviors in the elderly as categorical variables in the GMM. The GMM of class variables did not yield the evolutionary trend of the sample population but rather yielded the evolutionary trends of the subclasses as illustrated in
Figure 1,
Figure 2,
Figure 3,
Figure 4 and
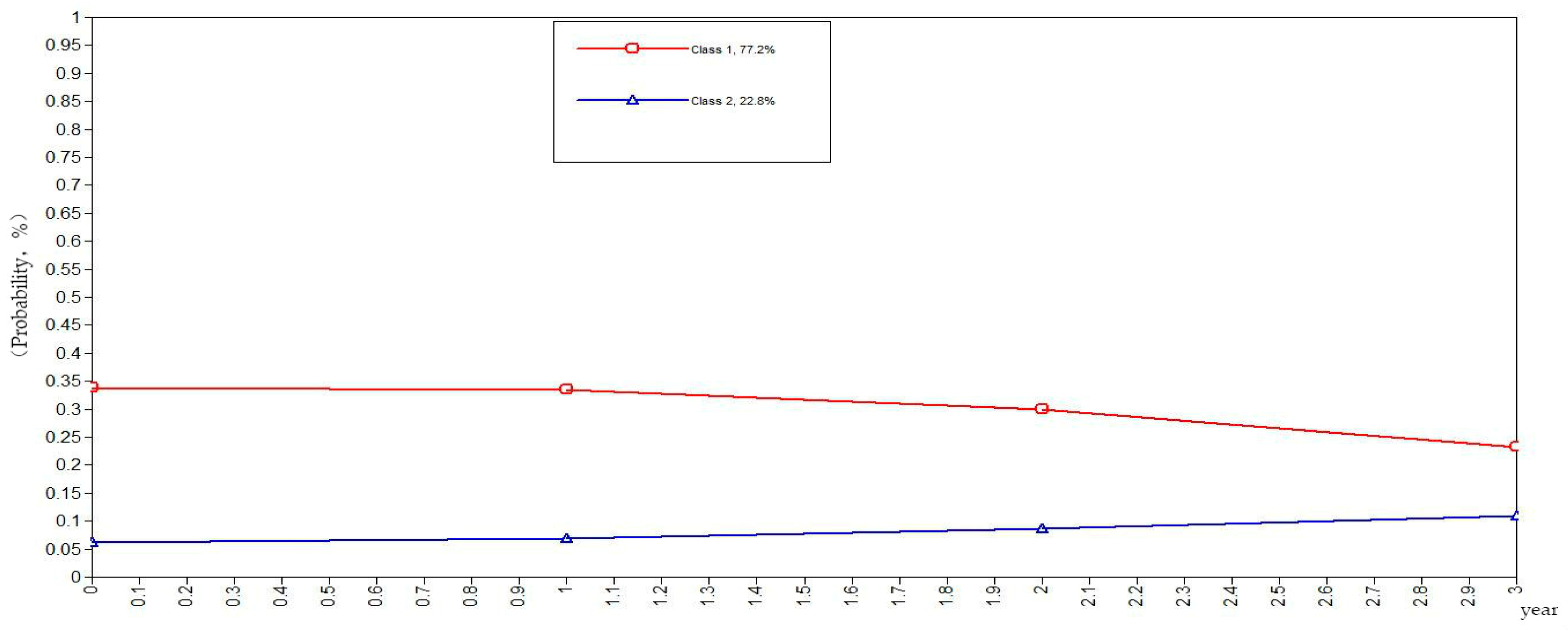
Figure 5. The ordinate in the graph represents the estimated probability value of health behavior modification, which ranges from 0–1. The abscissa represents different time periods. CLHLS data of the four waves in 2005, 2008, 2011, and 2014 are selected for this study. There are three time periods, and the abscissa value range is 0–3. It can be observed from
Figure 1 that the elderly with negative health behaviors have a lower estimated probability of behavior modification as their age increases, while the estimated probability of non-modification is slightly increased. What can be gathered from
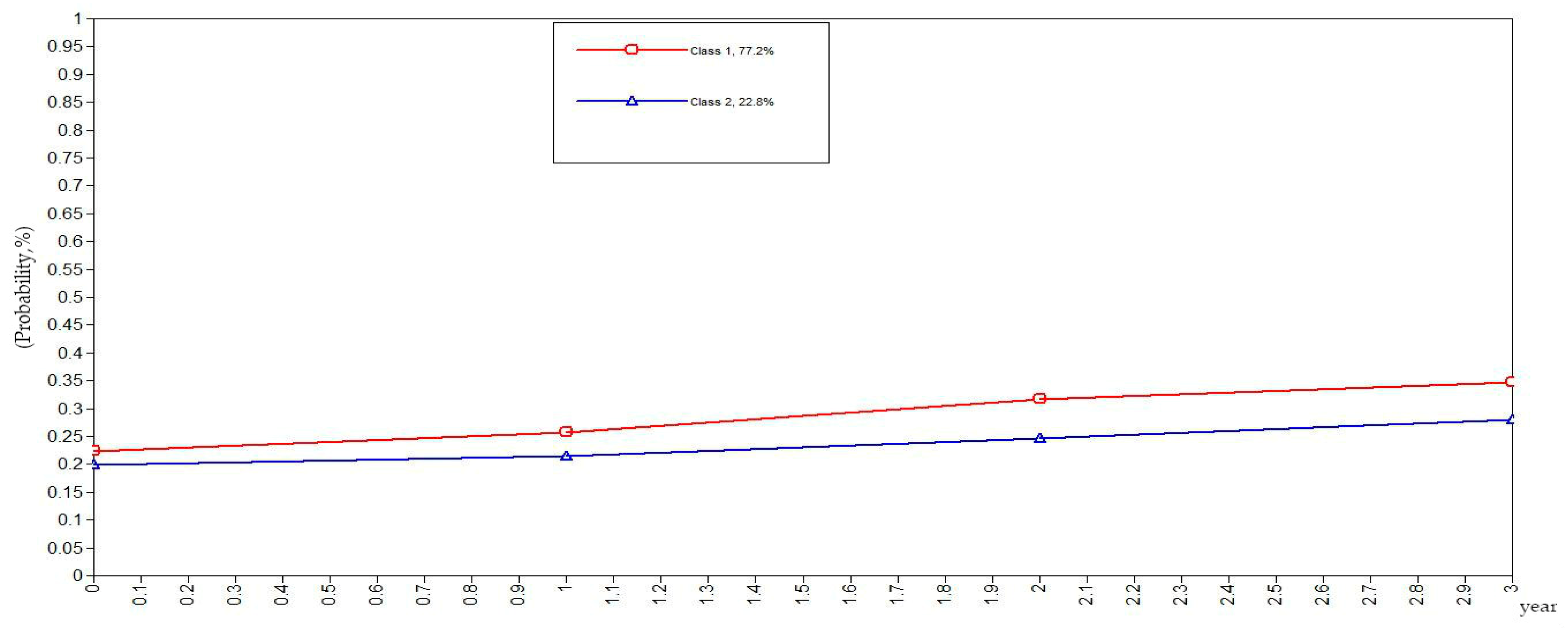
Figure 2 is that the modifications of the elderly with relatively negative health behaviors is similar to that of the elderly with negative health behaviors. From
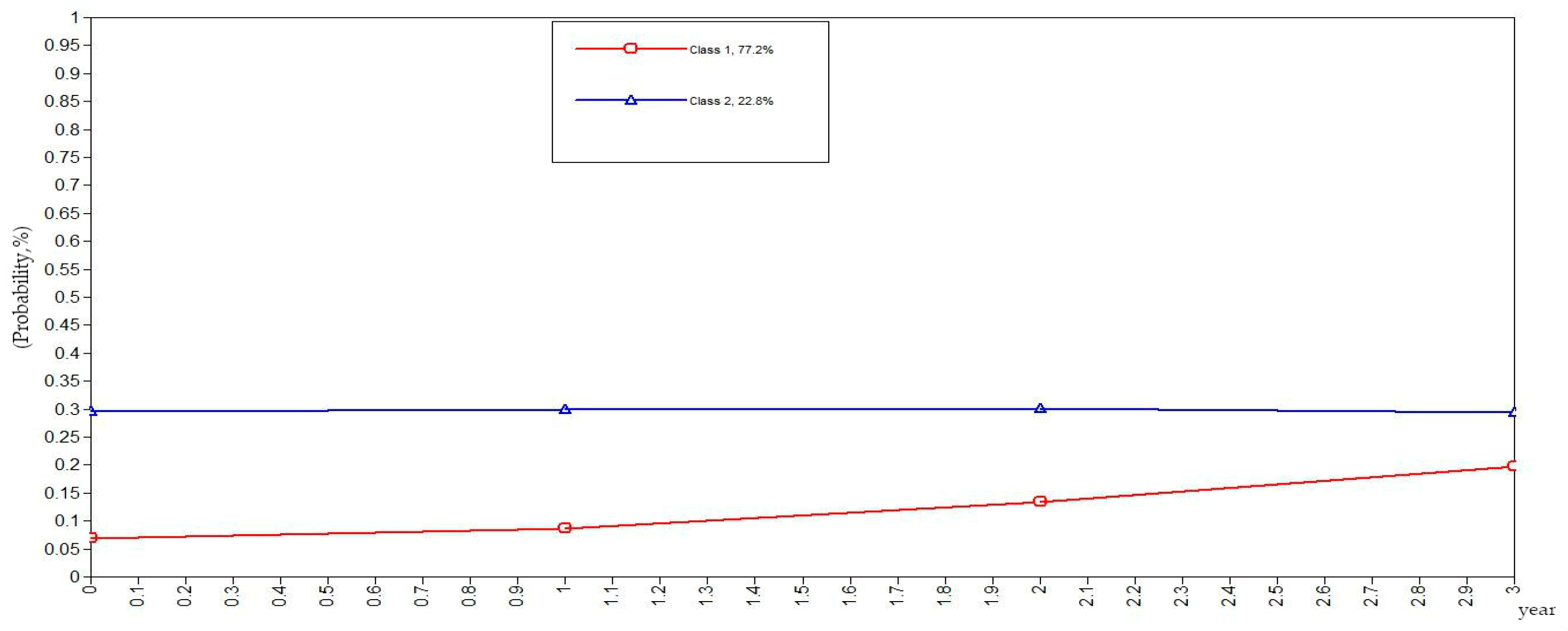
Figure 3, it can be found that the estimated probability of behavior modification with increasing age is higher for those with fair health behaviors, although the probability of those with non-modified behaviors is also slightly elevated. However, in this class, the estimated value of probability for modified behaviors is always higher than that of the non-modified ones. It is revealed in
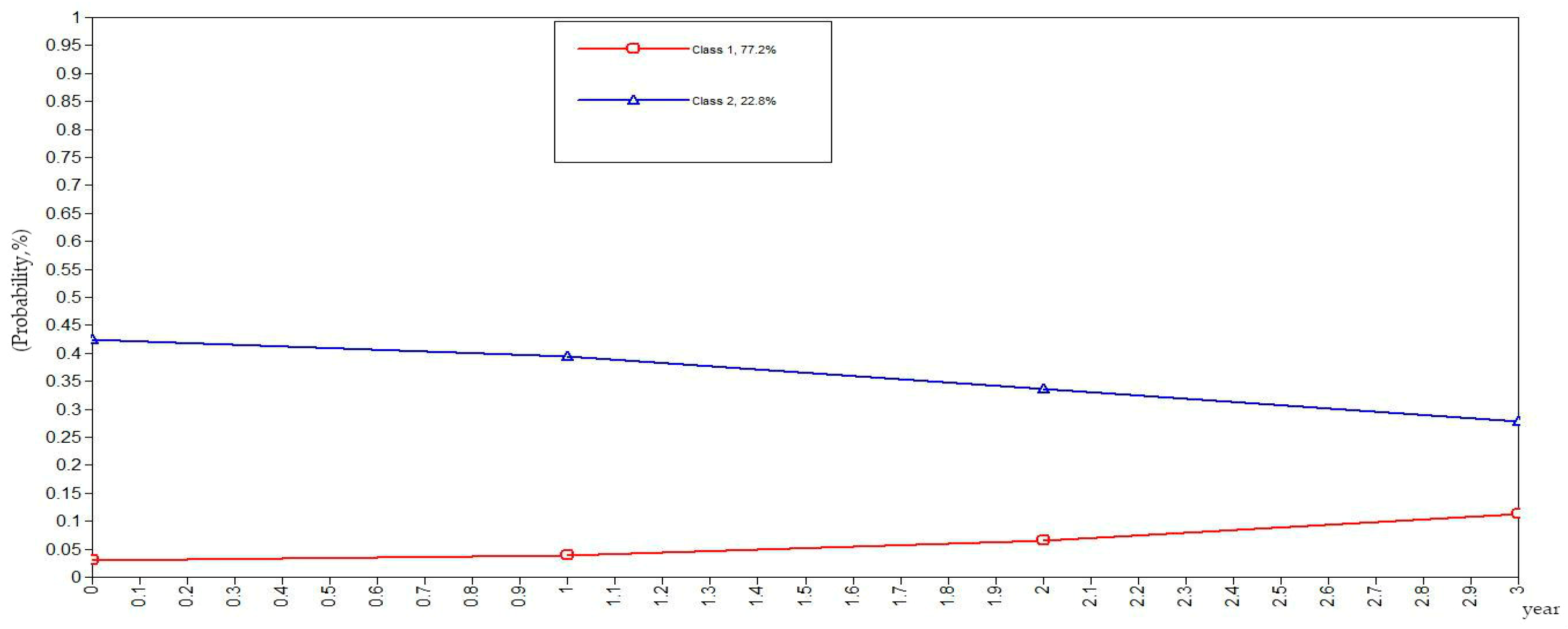
Figure 4 that the behavior modification probability value of the elderly with relatively positive healthy behaviors is higher, and the value of the elderly with non-modified behaviors is relatively stable. The estimated probability value of behavior modification in this class is always lower than the non-modified one. From
Figure 5, it is reflected that the estimated probability value of behavior modification for positive health behaviors gets higher with age, and the value of non-modified behaviors is decreasing.
In general, elderly people with positive health behaviors have a better tendency for behavior modification. Among the various classes of health behaviors, the older the elderly with negative and relatively negative health behaviors is, the lower the probability of behavior modification will be. In addition, the elderly with fair, relatively positive and positive health behaviors would pay more attention to optimizing health behaviors as their age increases.
3.3. Influencing Factors of the Evolution of the Elderly’s Health Behaviors
In this study, the evolution results of the elderly’s health behaviors were processed as Bivariate variables (modified or non-modified). The Bivariate analysis model was used to estimate social health and services, SRH, family characteristics and individual characteristics of the evolution of health behaviors in the Chinese elderly, analyses were performed using Stata (Stata version 13.0 for Windows, StataCorp LP, College Station, TX, USA). The results are shown in
Table 8. In general, as the variables continue to increase, the explanatory power of the model is gradually increasing. Specifically, the R
2 of Model I is 0.180, suggesting that social security and services can explain the variance of 18.0% of the evolution of the elderly’s health behaviors. The R
2 of Model II is 0.189, and SRH can explain only the variance of 0.9% of the evolution of health behaviors. Model III’s R
2 is 0.201, and family characteristics can explain the variance of 1.2% of the evolution of the elderly’s health behaviors. Model IV’s R
2 is 0.253, so the individual characteristics can explain the variance of 5.2% of the evolution of the elderly’s health behaviors.
What can be inferred from the regression results of these variables is that the timely treatment of illness in childhood has a significant negative effect on behavior modifications of the elderly. The probability of behavior modification of the elderly who received timely medical treatment in childhood is significantly lower than those who did not. The former is approximately 26.3–39.9% lower than the latter (p < 0.05, p < 0.001), indicating that the accessibility of medical services in childhood significantly reduced the elderly’s emphasis on health behaviors and the sense of modification for risky health behaviors. The probability of behavior modification of elderly people with pensions is significantly lower than that of those without pensions. The former is approximately 63.9–88.2% lower than the latter (p < 0.001), indicating that pension plays a role as a reverse incentive in the evolution of health behaviors. The probability of behavior modification of the elderly whose self-rated their own health as “unhealthy” is significantly higher than those who chose “very healthy”; the former’s probability is 2.868–2.989 (p < 0.001) times higher than the latter’s. With one additional unit in family annual income (taking the natural logarithm), the probability of behavior modification of the elderly decreased by 17.8–26.9% (p < 0.001).
The probability of behavior modification of the elderly increased by 3.1% with one year of ageing (p < 0.001). The probability of behavior modification of the elderly was reduced by 6.5% (p < 0.001) with a one-year-advancement in attaining education. The urban/county/rural distinction in the evolution of health behaviors in the elderly is also very significant, and the probability of behavior modification of the elderly is notably lower in those living in urban settings. The probability of behavior modification of the elderly in the country is 1.813 times (p < 0.001) higher than those in urban areas, and the probability of behavior modification in the rural elderly is also noticeably higher than the urban elderly with the former being 3.06 times (p < 0.001) higher. The differences of evolution are also distinct between occupational types; the probability of behavior modification of the elderly who were engaged in the public sector before the age of 60 was 39.5% lower than those who worked as commercial, service or industrial staff before the age of 60 (p < 0.01). The probability of behavior modification of the elderly engaged in agricultural works before the age of 60 is notably higher than that of the elderly who were engaged in commercial, service, or industrial jobs before the age of 60, the former being 1.525 times higher than that of the latter (p < 0.05). Hence, it can be inferred that there is a low probability of behavior modification of the elderly with relatively high-level occupations before the age of 60 and between the occupational level and the optimization of health behaviors exists a reverse correlation.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





 Slope
Slope