Consumption of Sugar-Sweetened Beverages Has a Dose-Dependent Effect on the Risk of Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Dose-Response Meta-Analysis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Methods
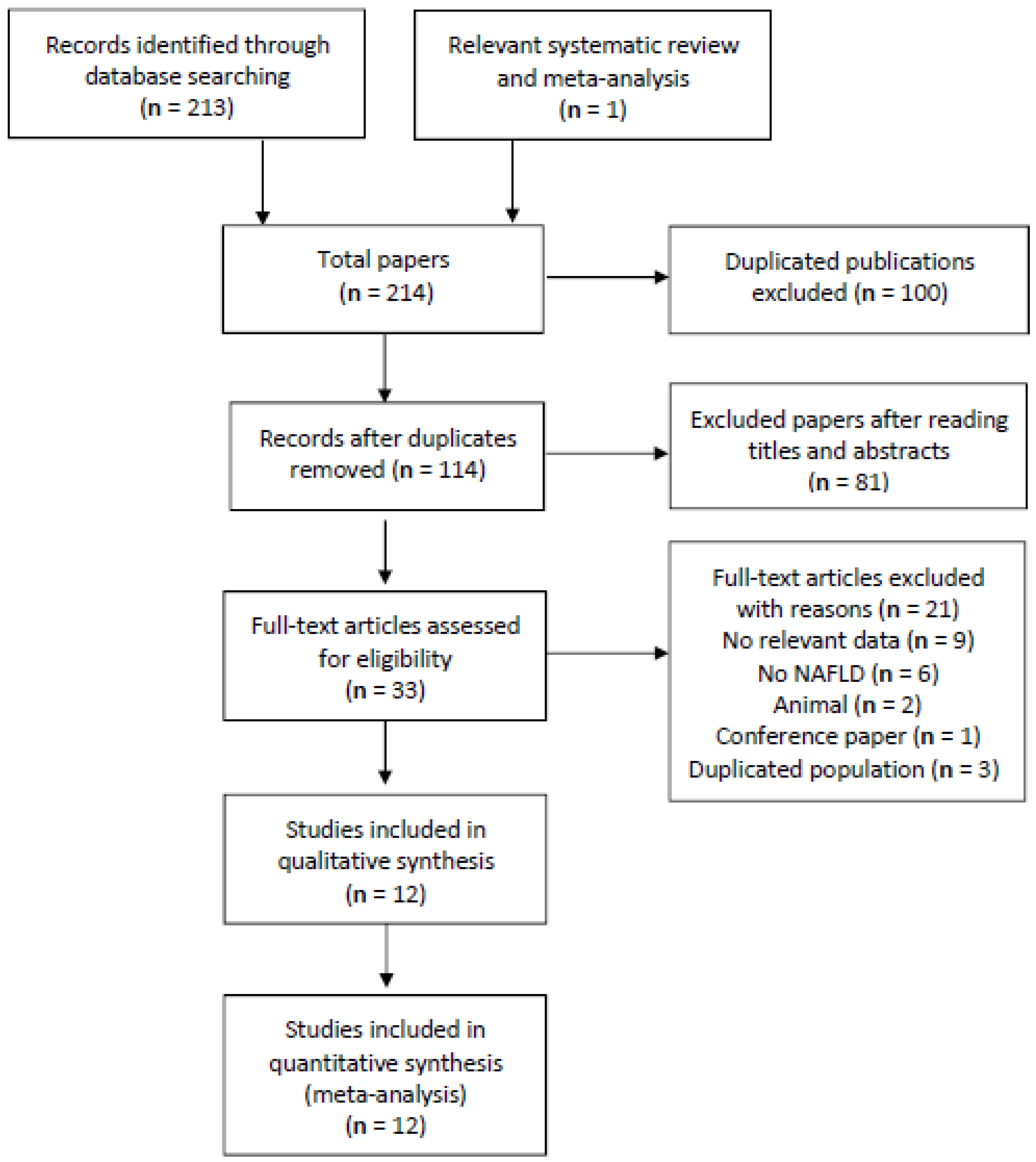
2.1. Search Strategy
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
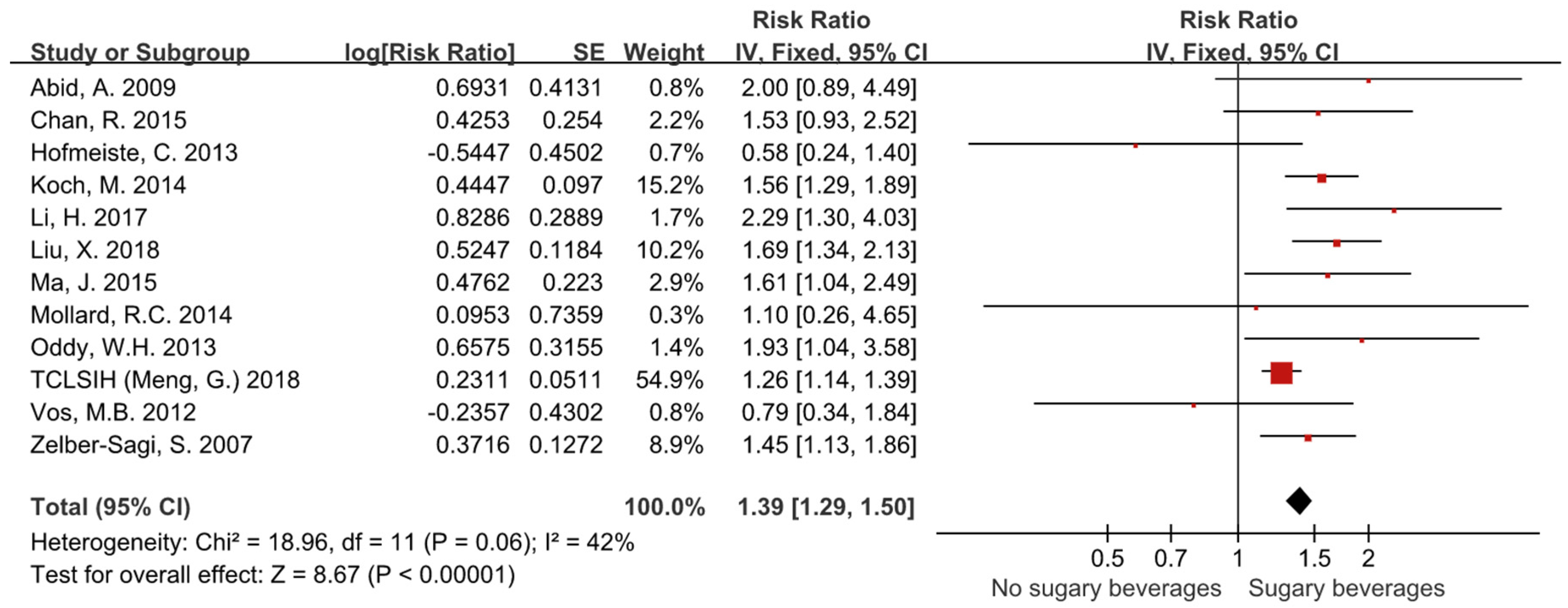
3.1. The Risk of NAFLD in Patients Consuming Sugar-Sweetened Beverages
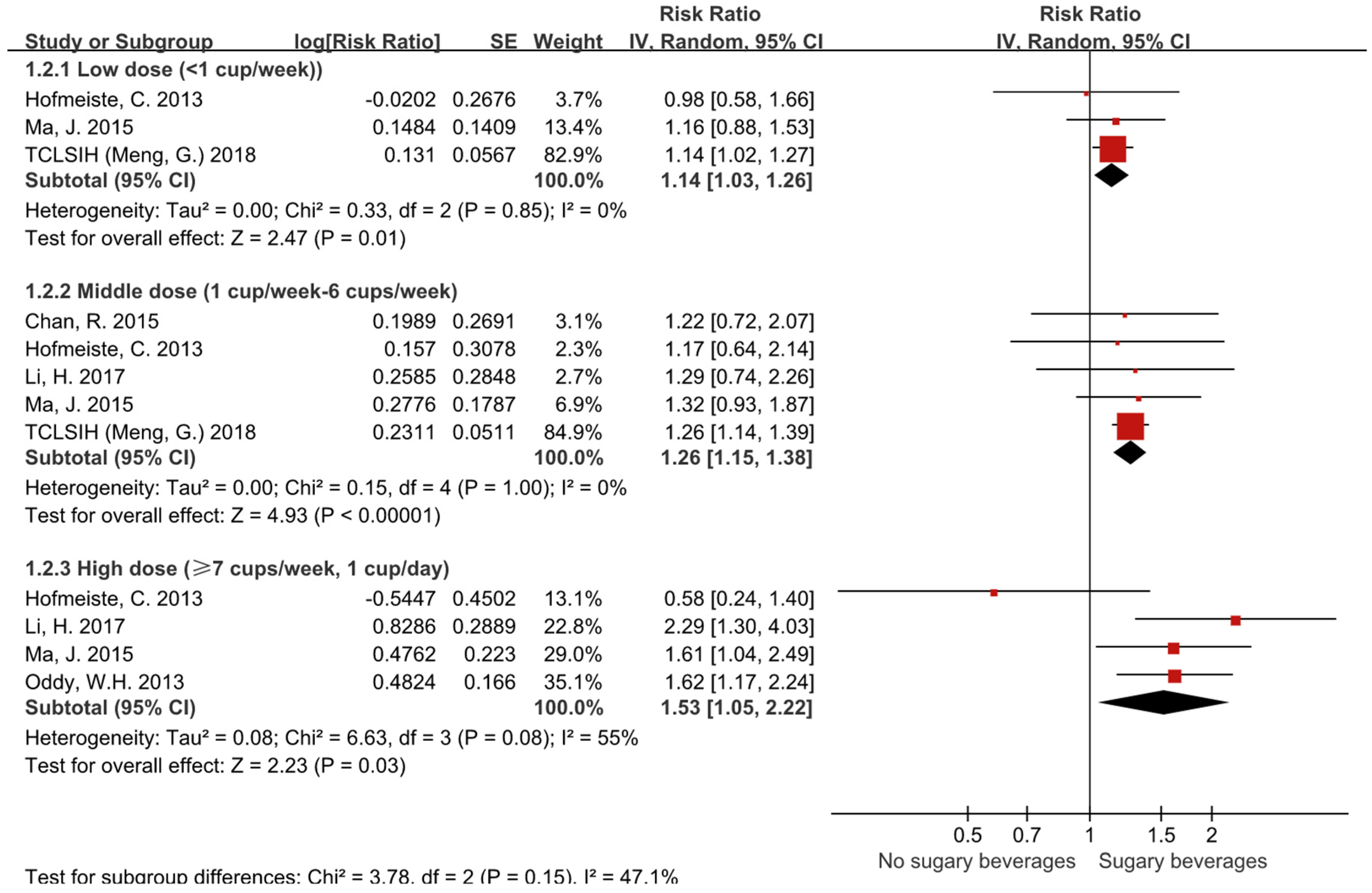
3.2. Subgroup Analyses on the Basis of Different Doses
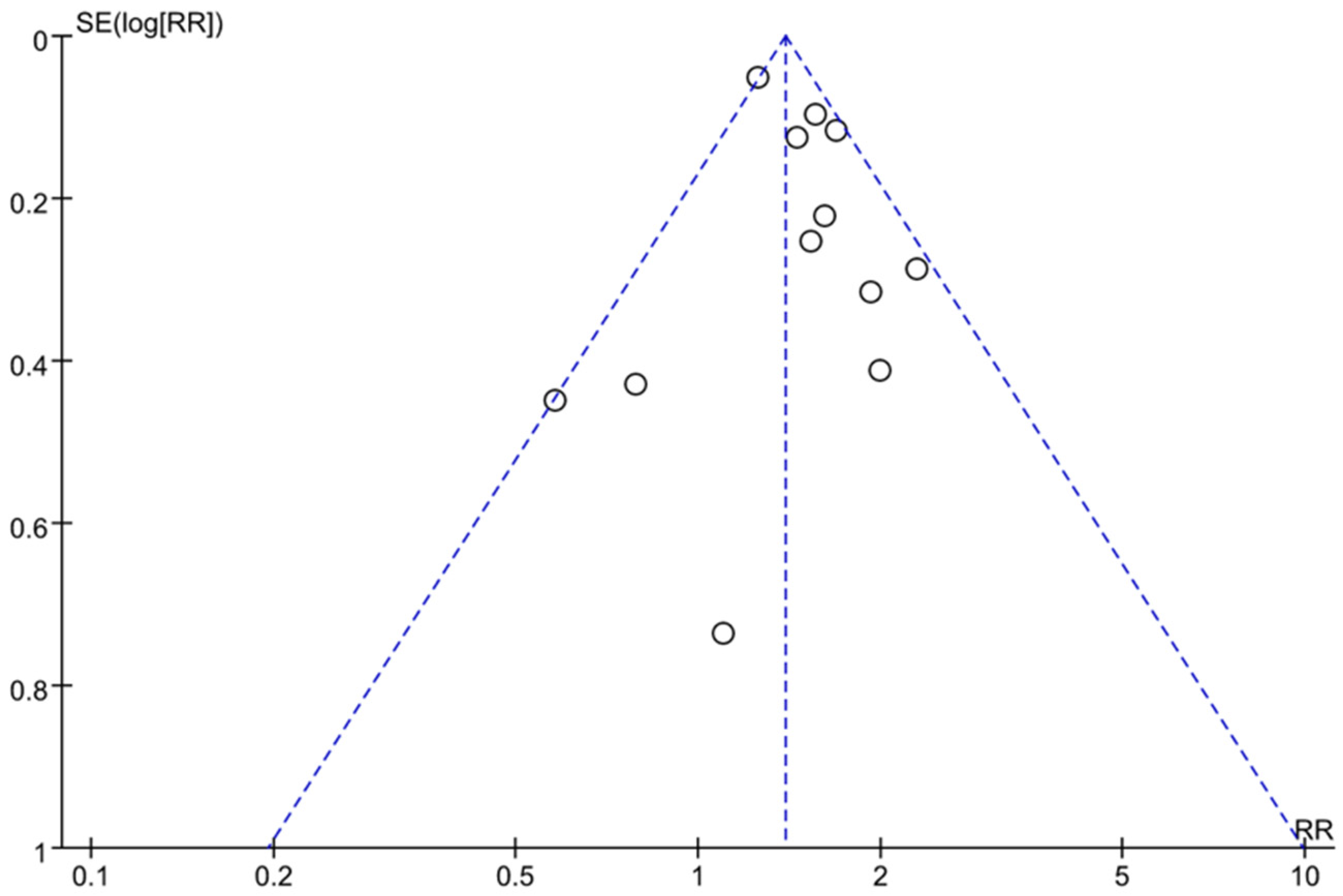
3.3. Assessment of Publication Bias
3.4. Sensitivity and Subgroup Analysis
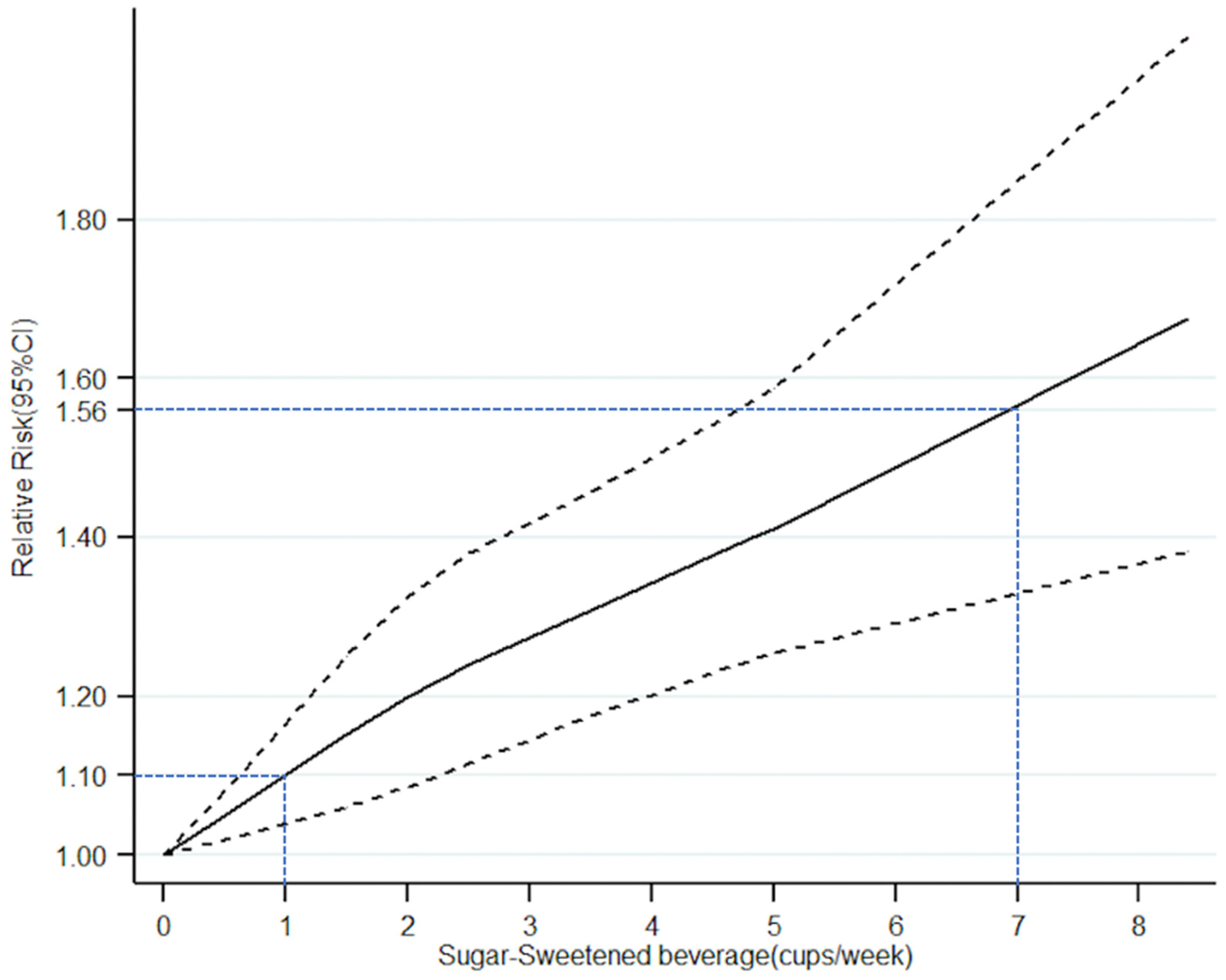
3.5. Dose-Response Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Allen, A.M.; Therneau, T.M.; Larson, J.J.; Coward, A.; Somers, V.K.; Kamath, P.S. Nonalcoholic fatty liver disease incidence and impact on metabolic burden and death: A 20 year-community study. Hepatology 2018, 67, 1726–1736. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Otgonsuren, M.; Henry, L.; Venkatesan, C.; Mishra, A.; Erario, M.; Hunt, S. Association of nonalcoholic fatty liver disease (NAFLD) with hepatocellular carcinoma (HCC) in the United States from 2004 to 2009. Hepatology 2015, 62, 1723–1730. [Google Scholar] [CrossRef]
- Smith, B.W.; Adams, L.A. Non-alcoholic fatty liver disease. Crit. Rev. Clin. Lab. Sci. 2011, 48, 97–113. [Google Scholar] [CrossRef]
- Bellentani, S.; Scaglioni, F.; Marino, M.; Bedogni, G. Epidemiology of non-alcoholic fatty liver disease. Dig. Dis. 2010, 28, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.G.; Farrell, G.C. Epidemiology of non-alcoholic fatty liver disease in China. J. Hepatol. 2009, 50, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Pimienta, T.G.; Batis, C.; Lutter, C.K.; Rivera, J.A. Sugar-Sweetened Beverages Are the Main Sources of Added Sugar Intake in the Mexican Population. J. Nutr. 2016, 146, 1888S–1896S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A. Fructose and risk of cardiometabolic disease. Curr. Atheroscler. Rep. 2012, 14, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Marriott, B.P.; Olsho, L.; Hadden, L.; Connor, P. Intake of added sugars and selected nutrients in the United States, National Health and Nutrition Examination Survey (NHANES) 2003–2006. Crit. Rev. Food Sci. Nutr. 2010, 50, 228–258. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Laohaphan, V.; Srivali, N. Transient ischemic attack related to sweetened beverage consumption. Am. J. Emerg. Med. 2015, 33, 462. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, M.D.; Lu, C.; Tutnauer, J.; Hartman, T.E.; Hwang, S.K.; Murphy, C.J.; Pauli, C.; Morris, R.; Taylor, S.; Bosch, K.; et al. High-fructose corn syrup enhances intestinal tumor growth in mice. Science 2019, 363, 1345–1349. [Google Scholar] [CrossRef]
- Malik, V.S.; Li, Y.; Pan, A.; De Koning, L.; Schernhammer, E.; Willett, W.C.; Hu, F.B. Long-Term Consumption of Sugar-Sweetened and Artificially Sweetened Beverages and Risk of Mortality in US Adults. Circulation 2019, 139, 2113–2125. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Evolution of inflammation in nonalcoholic fatty liver disease: The multiple parallel hits hypothesis. Hepatology 2010, 52, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Meng, G.; Zhang, B.; Yu, F.; Li, C.; Zhang, Q.; Liu, L.; Wu, H.; Xia, Y.; Bao, X.; Shi, H.; et al. Soft drinks consumption is associated with nonalcoholic fatty liver disease independent of metabolic syndrome in Chinese population. Eur. J. Nutr. 2018, 57, 2113–2121. [Google Scholar] [CrossRef] [PubMed]
- Hofmeiste, C.; Mark, M.H.; Atilla, S.A.; Suemeyra, O.; Bernhard, O.B.; Richard, A.M.; Wolfgang, K.U.; The EMIL-Study Group. Are soft drink consumption and fatty liver in any way connected? Ernaeh-Rungs Umsch. Int. 2013, 606, 82–88. [Google Scholar]
- Ma, J.; Fox, C.S.; Jacques, P.F.; Speliotes, E.K.; Hoffmann, U.; Smith, C.E.; Saltzman, E.; McKeown, N.M. Sugar-sweetened beverage, diet soda, and fatty liver disease in the Framingham Heart Study cohorts. J. Hepatol. 2015, 63, 462–469. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Liu, Z.; Sui, X.; Wu, Q.; Wang, J.; Xu, C. Elemene injection as adjunctive treatment to platinum-based chemotherapy in patients with stage III/IV non-small cell lung cancer: A meta-analysis following the PRISMA guidelines. Phytomedicine 2018, 59, 152787. [Google Scholar] [CrossRef]
- Koch, M.; Borggrefe, J.; Barbaresko, J.; Groth, G.; Jacobs, G.; Siegert, S.; Lieb, W.; Muller, M.J.; Bosy-Westphal, A. Dietary patterns associated with magnetic resonance imaging-determined liver fat content in a general population study. Am. J. Clin. Nutr. 2014, 99, 369–377. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Halpern, Z.; Oren, R. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): A population-based study. J. Hepatol. 2007, 47, 711–717. [Google Scholar] [CrossRef]
- Mollard, R.C.; Senechal, M.; MacIntosh, A.C.; Hay, J.; Wicklow, B.A.; Wittmeier, K.D.; Sellers, E.A.; Dean, H.J.; Ryner, L.; Berard, L. Dietary determinants of hepatic steatosis and visceral adiposity in overweight and obese youth at risk of type 2 diabetes. Am. J. Clin. Nutr. 2014, 99, 804–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abid, A.; Taha, O.; Nseir, W.; Farah, R.; Grosovski, M.; Assy, N. Soft drink consumption is associated with fatty liver disease independent of metabolic syndrome. J. Hepatol. 2009, 51, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Herbison, C.E.; Jacoby, P.; Ambrosini, G.L.; O’Sullivan, T.A.; Ayonrinde, O.T.; Olynyk, J.K.; Black, L.J.; Beilin, L.J.; Mori, T.A.; et al. The Western dietary pattern is prospectively associated with nonalcoholic fatty liver disease in adolescence. Am. J. Gastroenterol. 2013, 108, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Peng, Y.; Chen, S.; Sun, Q. An observational study on the association between major dietary patterns and non-alcoholic fatty liver disease in Chinese adolescents. Medicine (Baltimore) 2018, 97, e0576. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.B.; Colvin, R.; Belt, P.; Molleston, J.P.; Murray, K.F.; Rosenthal, P.; Schwimmer, J.B.; Tonascia, J.; Unalp, A.; Lavine, J.E.; et al. Correlation of vitamin E, uric acid, and diet composition with histologic features of pediatric NAFLD. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 90–96. [Google Scholar] [CrossRef]
- Chan, R.; Wong, V.W.; Chu, W.C.; Wong, G.L.; Li, L.S.; Leung, J.; Chim, A.M.; Yeung, D.K.; Sea, M.M.; Woo, J.; et al. Diet-Quality Scores and Prevalence of Nonalcoholic Fatty Liver Disease: A Population Study Using Proton-Magnetic Resonance Spectroscopy. PLoS ONE 2015, 10, e0139310. [Google Scholar] [CrossRef] [PubMed]
- Li, H. Survey of Sugar-sweetened Beverages for inpatients and its effect on Metabolism. Master’s Thesis, Tianjin Medical University, Tianjin, China, 2017. (In Chinese). [Google Scholar]
- Xia, Y. The Associations between Dietary Patterns and Non-alcoholic Fatty Liver Disease. Ph.D. Thesis, Tianjin Medical University, Tianjin, China, 2019. (In Chinese). [Google Scholar]
- Asgari-Taee, F.; Zerafati-Shoae, N.; Dehghani, M.; Sadeghi, M.; Baradaran, H.R.; Jazayeri, S. Association of sugar sweetened beverages consumption with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Nutr. 2018, 14. [Google Scholar] [CrossRef] [PubMed]
- William, N.; Fares, N.; Nimer, A. Soft drinks consumption and nonalcoholic fatty liver disease. World J. Gastroenterol. 2010, 16, 2579–2588. [Google Scholar]
- Rippe, J.M.; Angelopoulos, T.J. Sucrose, High-Fructose Corn Syrup, and Fructose, Their Metabolism and Potential Health Effects: What Do We Really Know? Adv. Nutr. 2013, 4, 236–245. [Google Scholar] [CrossRef]
- Anania, F.A. Non-alcoholic fatty liver disease and fructose: Bad for us, better for mice. J. Hepatol. 2011, 55, 218–220. [Google Scholar] [CrossRef]
- Sánchez-Lozada, L.G.; Mu, W.; Roncal, C.; Sautin, Y.Y.; Abdelmalek, M.; Reungjui, S.; Le, M.; Nakagawa, T.; Lan, H.Y.; Yu, X.; et al. Comparison of free fructose and glucose to sucrose in the ability to cause fatty liver. Eur. J. Nutr. 2010, 49, 1–9. [Google Scholar] [CrossRef]
- Ouyang, X.; Cirillo, P.; Sautin, Y.; McCall, S.; Bruchette, J.L.; Diehl, A.M.; Johnson, R.J.; Abdelmalek, M.F. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J. Hepatol. 2008, 48, 993–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, N.K.; Bundy, V.; Kanto, W.; Davis, C.L.; Bernard, P.J.; Zhu, H.; Gutin, B.; Dong, Y. Greater fructose consumption is associated with cardiometabolic risk markers and visceral adiposity in adolescents. J. Nutr. 2012, 142, 251–257. [Google Scholar] [CrossRef]
- Bahuguna, R.; Younis, K.S.; Jain, A. Influence of feeding practices on dental caries. A case-control study. Eur. J. Paediatr. Dent. 2013, 14, 55–58. [Google Scholar]
- Rizkalla, S.W. Health implications of fructose consumption: A review of recent data. Nutr. Metab. (Lond.) 2010, 7, 82. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J.A.; Sharma, A.J.; Grellinger, L.; Vos, M.B. Consumption of added sugars is decreasing in the United States. Am. J. Clin. Nutr. 2011, 94, 726–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.A.; Gale, E.A. Diabetes, insulin use, and cancer risk: Are observational studies part of the solution or part of the problem? Diabetes 2010, 59, 1129–1131. [Google Scholar] [CrossRef] [PubMed]
- Pisani, P.; Faggiano, F.; Krogh, V.; Palli, D.; Vineis, P.; Berrino, F. Relative validity and reproducibility of a food frequency dietary questionnaire for use in the Italian EPIC centers. Int. J. Epidemiol. 1997, 26 (Suppl. 1), 152–160. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Age/Sexes | Study Design | Cases/Non-Cases, Total Number | Sugar-Sweetened Beverage Consumption | Results, Adjusted OR (95% CI) | Exposure Definition and Exposure Measurement | Confounder Adjustment | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Abid, A. 2009 [22] | Israel | 43 ± 12 y, M/F | Cross-sectional study | 60/30, 90 | NA | 2 (0.89, 4.47) | Soft drinks, FFQ | Adjusted for OR, age, sex, smoking habits, physical activity, dietary composition, BMI, metabolic syndrome, triglyceride, HOMA and metabolic biomarkers. | 8 |
| TCLSIH (Meng, G.) 2018 [13] | China | 41.2 ± 11.9 y, 13,529 M/13,261 F | Cross-sectional study | NA, 26,790 | 0, <1 cup/week, ≥1 cup/week | 1.26 (1.14, 1.4) | Soft drinks, FFQ | Adjusted for age, sex, BMI, OR, smoking status, drinker status, educational level, employment status, household income, family history of diseases, total energy intake, protein intake, carbohydrate intake, fat intake, EPA and DHA intake, physical activity and metabolic syndrome and consumption of other beverages. | 8 |
| Ma, J. 2015 [15] | USA | M ≥ 35 y, F ≥ 40y, M/F | Cross-sectional study | NA,2634 | 0, 1, 4, 10 servings/week | 1.61 (1.04, 2.5) | SSBs, FFQ | Adjusted for age, sex, energy intake, alcohol intake, dietary fiber, dietary fat, dietary protein, SSBs or diet soda, smoking and Framingham cohort. | 9 |
| Li, H. 2017 [27] | China | 45.15 ± 12.52 y, 325 M/80 F | Cross-sectional study | NA, 405 | 0, few (<1000 mL/week), many (>1000 mL/week) | 2.29 (1.3, 4.03) | SSBs, FFQ | NA | 6 |
| Koch, M. 2014 [19] | Germany | 67.6 y, M/F | Case-control study | 171/183, 354 | NA | 1.56 (1.29, 1.88) | Soft drinks, FFQ | Adjusted for age and sex, smoking status, smoking duration, physical activity, total energy intake and years of education. | 9 |
| Vos, M.B. 2012 [25] | USA | 12 ± 2.6 y, M/F | Cross-sectional study | NA, 149 | >6 SSBs/week | 0.79 (0.34, 1.87) | SSBs, FFQ | NA | 6 |
| Mollard, R.C. 2014 [21] | USA | 15.4 ± 1.8 y, M/F | Cross-sectional study | 21/47, 68 | NA | 1.1 (0.26, 4.67) | Soda, FFQ | Adjusted for available carbohydrate, fiber, protein, and total fat, carbohydrate, fiber, protein, total fat, age, and sex, BMI, ethnicity and cardiorespiratory fitness. | 8 |
| Chan, R. 2015 [26] | Hongkong, China | 48.1 ± 10.6 y, 332 M/465 F | Case control study | 220/577, 797 | 0, 1–71 mL/day, >71 mL/day | 1.53 (0.93, 2.52) | SSBs, FFQ | Adjusted for age, gender, BMI, smoker status, drinker status, central obesity, triglyceride > 1.7 mmol/L, reduced HDL-cholesterol, hypertension, impaired fasting glucose or diabetes and PNPLA3 genotypes. | 8 |
| Zelber-Sagi, S. 2007 [20] | Israel | 50.7 ± 10.4 y, 184 M/165 F | Cross-sectional study | 108/241, 349 | NA | 1.4 (1.13, 1.85) | Soft drinks, FFQ | Adjusted for age, gender, BMI and total calories. | 8 |
| Oddy, W.H. 2013 [23] | Australia | 14 y/17 y, M/F | Cohort study | 151/844, 995 | Fourth quartile of soft drinks | 1.93 (1.04, 3.56) | Soft drinks, FFQ | Adjusted for western dietary pattern, healthy dietary pattern, sex, misreporting, TV viewing, frequency of physical activity and family income. | 9 |
| Liu, X. 2018 [24] | China | 16–23 y, M/F | Cross-sectional study | 221/1418,1639 | NA | 1.69 (1.34, 2.56) | Soft drinks, FFQ | Adjusted for age, sex, BMI, economic income, smoking status, educational level, physical activity, family history of diabetes and stroke and energy intake. | 8 |
| Hofmeiste, C. 2013 [14] | Germany | 10–65 y, M/F | Cross-sectional study | 374/1061, 1435 | rarely/never, several times/months, several times/weeks, daily | 0.58 (0.24, 1.40) | Soft drinks, FFQ | Adjusted for age, sex, BMI, WHR, sweets, metabolic syndrome, HTN and DM. | 8 |
| Subgroups | Number of Studies | RR (95% CI) | Statistical Method | p-Value | |
|---|---|---|---|---|---|
| All studies | 12 | 1.39 (1.29–1.50) | fixed | <0.00001 * | |
| Geographical location | Asian populations | 6 | 1.51 (1.27–1.79) | random | <0.00001 * |
| Non-Asian populations | 6 | 1.38 (1.05–1.83) | random | 0.02 * | |
| Study design | Cross-sectional study | 9 | 1.35 (1.24–1.46) | fixed | <0.00001 * |
| Case-control study | 2 | 1.56 (1.30–1.86) | fixed | <0.00001 * | |
| Cohort study | 1 | 1.93 (1.04–3.58) | fixed | 0.04 * | |
| Sample size | ≥500 | 6 | 1.44 (1.17–1.77) | random | 0.0006 * |
| <500 | 6 | 1.54 (1.34–1.77) | fixed | <0.00001 * | |
| NOS ≥ 8 | Yes | 10 | 1.38 (1.28–1.49) | fixed | <0.00001 * |
| No | 2 | 1.41 (0.50–3.99) | random | 0.52 | |
| Adjustment for Confounder | Yes | 10 | 1.38 (1.28–1.49) | fixed | <0.00001 * |
| No | 2 | 1.41 (0.50–3.99) | random | 0.52 | |
| Author | Intake Frequency (Cups/Week) | Midpoint Frequency (Cups/Week) | Case/n | OR (95% CI) |
|---|---|---|---|---|
| Li, H. 2017 | 0 | 0 | 80/199 | 1 |
| Few (<1000 mL/week) (<7 cups/week) | 3.5 | 85/202 | 1.30 (0.74–2.26) | |
| Many (>1000 mL/week) (>7 cups/week) | 8.4 | 127/281 | 2.29 (1.30–4.03) | |
| TCLSIH (Meng, G.) 2017 | Almost never | 0 | 4076/14,985 | 1 |
| <1 cup/week | 0.5 | 1211/4606 | 1.14 (1.02–1.27) | |
| ≥1 cups/week | 1.2 | 1971/7199 | 1.26 (1.14–1.40) | |
| TCLSIH (Xia, Y.) 2019 | 0 | 0 | 466/1200 | 1 |
| 2–3 cups/week | 2.5 | 588/1200 | 0.93 (0.75–1.16) | |
| 4–6 cups/week | 5 | 614/1200 | 1.12 (0.90–1.39) | |
| ≥1 cup/day (7 cups/week) | 8.4 | 732/1200 | 1.40 (1.11–1.76) | |
| Chan, R. 2015 | 0 | 0 | 87/231 | 1 |
| 1–71 mL/day (0–4 cups/week) | 2 | 47/163 | 1.22 (0.72–2.08) | |
| >71 mL/day (>4 cups/week) | 4.8 | 86/183 | 1.53 (0.93–2.52) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.; Wang, J.; Li, Z.; Lam, C.W.K.; Xiao, Y.; Wu, Q.; Zhang, W. Consumption of Sugar-Sweetened Beverages Has a Dose-Dependent Effect on the Risk of Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Dose-Response Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2192. https://doi.org/10.3390/ijerph16122192
Chen H, Wang J, Li Z, Lam CWK, Xiao Y, Wu Q, Zhang W. Consumption of Sugar-Sweetened Beverages Has a Dose-Dependent Effect on the Risk of Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Dose-Response Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(12):2192. https://doi.org/10.3390/ijerph16122192
Chicago/Turabian StyleChen, Hongwei, Jue Wang, Zheng Li, Christopher Wai Kei Lam, Ying Xiao, Qibiao Wu, and Wei Zhang. 2019. "Consumption of Sugar-Sweetened Beverages Has a Dose-Dependent Effect on the Risk of Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Dose-Response Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 12: 2192. https://doi.org/10.3390/ijerph16122192
APA StyleChen, H., Wang, J., Li, Z., Lam, C. W. K., Xiao, Y., Wu, Q., & Zhang, W. (2019). Consumption of Sugar-Sweetened Beverages Has a Dose-Dependent Effect on the Risk of Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Dose-Response Meta-Analysis. International Journal of Environmental Research and Public Health, 16(12), 2192. https://doi.org/10.3390/ijerph16122192