Hip and Wrist-Worn Accelerometer Data Analysis for Toddler Activities


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Behavior Labeling
2.4. Accelerometer Data Processing
2.5. Statistical Analysis
3. Results
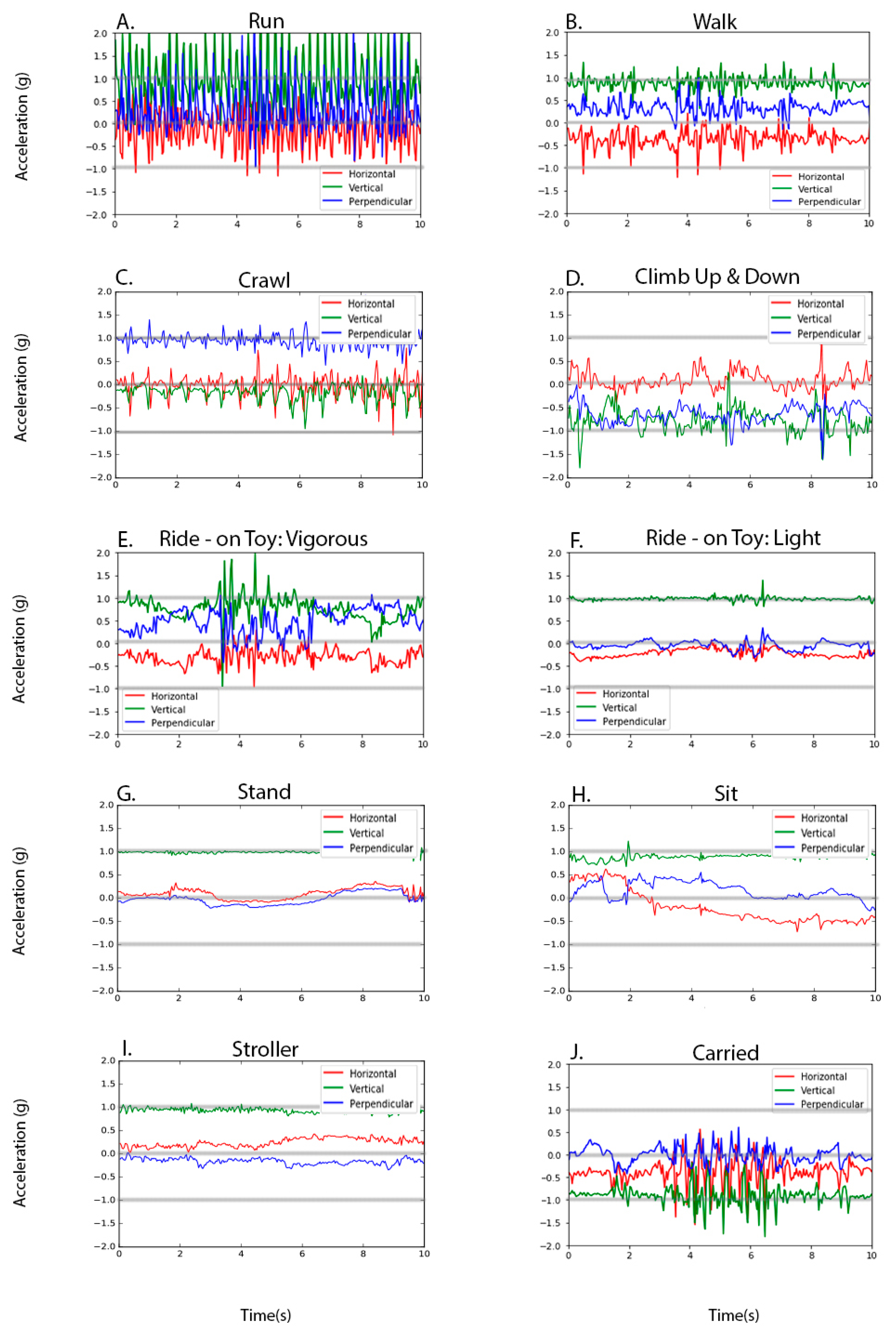
3.1. Sub-Aim One
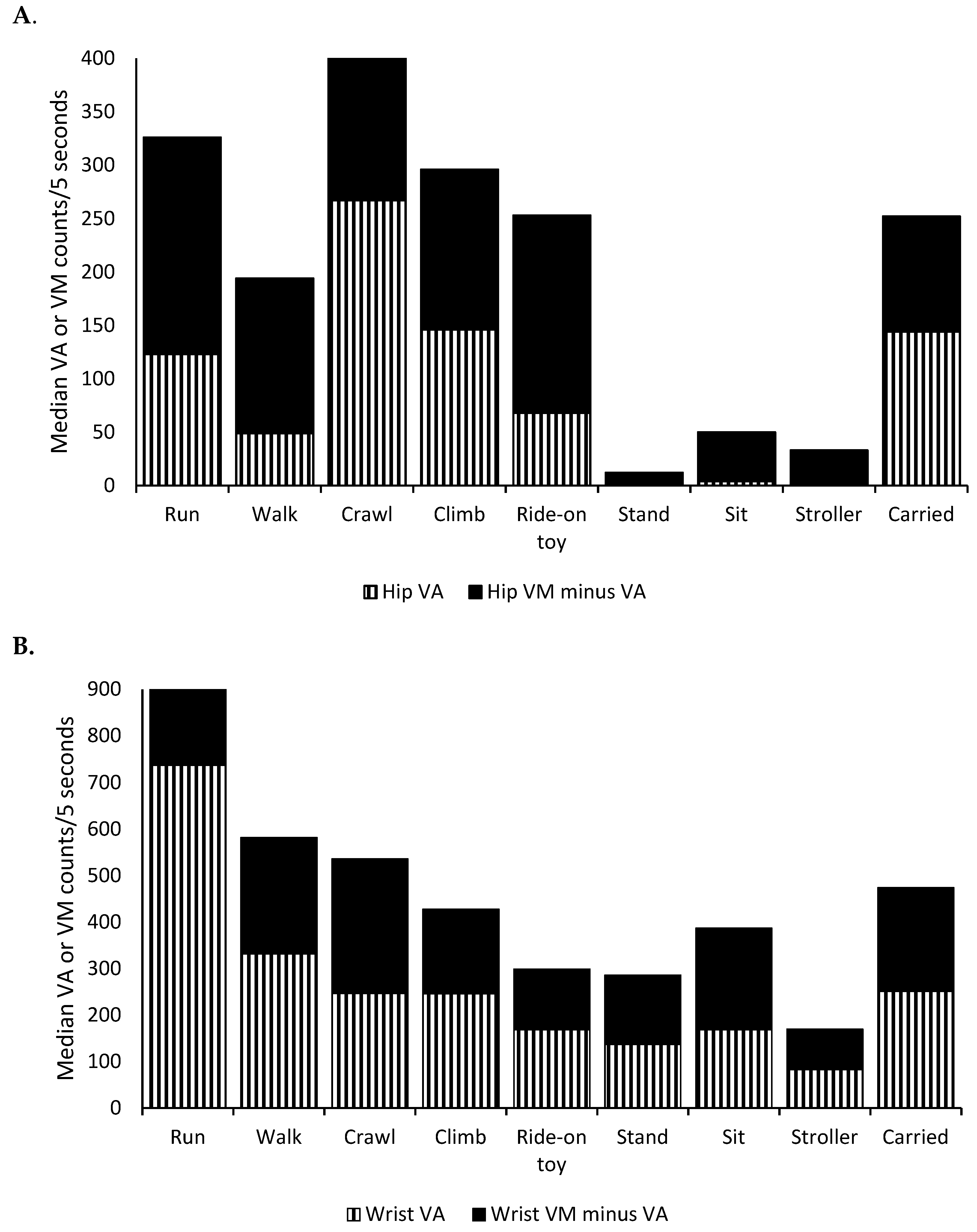
3.2. Sub-Aim Two
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Kwon, S.; Janz, K.; Letuchy, E.; Trudy, B.; Steven, L. Developmental trajectories of physical activity, sports, and television viewing during childhood to young adulthood. JAMA Pediatr. 2015, 169, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Hinkley, T.; Salmon, J.; Okely, A.D.; Crawford, D.; Hesketh, K. Preschoolers’ physical activity, screen time, and compliance with recommendations. Med. Sci. Sports Exerc. 2012, 44, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Beets, M.W.; Bornstein, D.; Dowda, M.; Pate, R.R. Compliance with national guidelines for physical activity in U.S. preschoolers: Measurement and interpretation. Pediatrics 2011, 127, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; O’Neill, J.R.; Brown, W.H.; Pfeiffer, K.A.; Dowda, M.; Addy, C.L. Prevalence of Compliance with a New Physical Activity Guideline for Preschool-Age Children. Child. Obes. 2015, 11, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Worobey, J. Physical activity in infancy: Developmental aspects, measurement, and importance. Am. J. Clin. Nutr. 2014, 99, 729S–733S. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Barber, S.E.; Cameron, N.; Clemes, S.A. The objective measurement of physical activity and sedentary behaviour in 2–3 year olds and their parents: A cross-sectional feasibility study in the bi-ethnic Born in Bradford cohort. BMC Public Health 2015, 15, 1109. [Google Scholar] [CrossRef] [PubMed]
- Hnatiuk, J.; Ridgers, N.D.; Salmon, J.; Campbell, K.; McCallum, Z.; Hesketh, K. Physical activity levels and patterns of 19-month-old children. Med. Sci. Sports Exerc. 2012, 44, 1715–1720. [Google Scholar] [CrossRef] [PubMed]
- Borkhoff, C.M.; Heale, L.D.; Anderson, L.N.; Tremblay, M.S.; Maguire, J.L.; Parkin, P.C.; Birken, C.S. Objectively measured physical activity of young Canadian children using accelerometry. Appl. Physiol. Nutr. Metab. 2015, 40, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Hesketh, K.D.; Rhodes, R.E.; Rinaldi, C.M.; Spence, J.C.; Carson, V. Role of parental and environmental characteristics in toddlers’ physical activity and screen time: Bayesian analysis of structural equation models. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 17. [Google Scholar] [CrossRef]
- Hager, E.R.; Gormley, C.E.; Latta, L.W.; Treuth, M.S.; Caulfield, L.E.; Black, M.M. Toddler physical activity study: Laboratory and community studies to evaluate accelerometer validity and correlates. BMC Public Health 2016, 16, 936. [Google Scholar] [CrossRef]
- Kuzik, N.; Clark, D.; Ogden, N.; Harber, V.; Carson, V. Physical activity and sedentary behaviour of toddlers and preschoolers in child care centres in Alberta, Canada. Can. J. Public Health 2015, 106, e178–e183. [Google Scholar] [CrossRef] [PubMed]
- Raza, H.; Zhou, S.M.; Todd, C.; Christian, D.; Marchant, E.; Morgan, K.; Khanom, A.; Hill, R.; Lyons, R.A.; Brophy, S. Predictors of objectively measured physical activity in 12-month-old infants: A study of linked birth cohort data with electronic health records. Pediatr. Obes. 2019, 14, e12512. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Fees, B.S.; Haar, S.J.; Murray, A.D.; Crowe, L.K. Identification and validity of accelerometer cut-points for toddlers. Obesity 2012, 20, 2317–2319. [Google Scholar] [CrossRef]
- Oftedal, S.; Bell, K.L.; Davies, P.S.; Ware, R.S.; Boyd, R.N. Validation of accelerometer cut points in toddlers with and without cerebral palsy. Med. Sci. Sports Exerc. 2014, 46, 1808–1815. [Google Scholar] [CrossRef] [PubMed]
- Ellis, K.; Kerr, J.; Godbole, S.; Staudenmayer, J.; Lanckriet, G. Hip and Wrist Accelerometer Algorithms for Free-Living Behavior Classification. Med. Sci. Sports Exerc. 2016, 48, 933–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, Y.; Park, J.W. Child activity recognition based on cooperative fusion model of a triaxial accelerometer and a barometric pressure sensor. IEEE J. Biomed. Health Inform. 2013, 17, 420–426. [Google Scholar] [PubMed]
- Zhao, W.; Adolph, A.L.; Puyau, M.R.; Vohra, F.A.; Butte, N.F.; Zakeri, I.F. Support vector machines classifiers of physical activities in preschoolers. Physiol. Rep. 2013, 1, e00006. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Cliff, D.P.; Ahmadi, M.N.; Tuc, N.V.; Hagenbuchner, M. Sensor-enabled Activity Class Recognition in Preschoolers: Hip versus Wrist Data. Med. Sci. Sports Exerc. 2018, 50, 634–641. [Google Scholar] [CrossRef]
- Hagenbuchner, M.; Cliff, D.P.; Trost, S.G.; Van, T.N. Peoples GE. Prediction of activity type in preschool children using machine learning techniques. J. Sci. Med. Sport 2015, 18, 426–431. [Google Scholar] [CrossRef]
- John, D.; Freedson, P. ActiGraph and Actical physical activity monitors: A peek under the hood. Med. Sci. Sports Exerc. 2012, 44, S86–S89. [Google Scholar] [CrossRef]
- Kerr, J.; Patterson, R.E.; Ellis, K.; Godbole, S.; Johnson, E.; Lanckriet, G.; Staudenmayer, J. Objective Assessment of Physical Activity: Classifiers for Public Health. Med. Sci. Sports Exerc. 2016, 48, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Vanloo, C.M.; Okely, A.D.; Batterham, M.J.; Hinkley, T.; Ekelund, U.; Brage, S.; Reilly, J.J.; Trost, S.G.; Jones, R.A.; Janssen, X.; et al. Wrist Accelerometer Cut Points for Classifying Sedentary Behavior in Children. Med. Sci. Sports Exerc. 2017, 49, 813–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Lee, J.M.; Peters, B.P.; Gaesser, G.A.; Welk, G.J. Examination of different accelerometer cut-points for assessing sedentary behaviors in children. PLoS ONE 2014, 9, e90630. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.; Beets, M.; Saint-Maurice, P.; Weaver, R.; Cliff, D.; Drenowatz, C.; Moore, J.B.; Sui, M.; Brazendale, K. Wrist-Based Accelerometer Cut-Points to Identify Sedentary Time in 5–11-Year-Old Children. Children 2018, 5, 137. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Way, R.; Okely, A.D. Predictive validity of three ActiGraph energy expenditure equations for children. Med. Sci. Sports Exerc. 2006, 38, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; O’Neill, J.R.; Mitchell, J. Measurement of physical activity in preschool children. Med. Sci. Sports Exerc. 2010, 42, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of Accelerometer Cut-points for Predicting Activity Intensity in Youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Behavior | Description | Frequency | Accelerometer Data in Seconds |
|---|---|---|---|
| n | Mean (Median) | ||
| Run | Running forward from one place to the other. | 20 | 7.5 (5.0) |
| Walk | Walking forward from one place to the other. Taking a few side steps to grab something, for example, was not considered as “walk.” | 244 | 7.3 (6.0) |
| Crawl | Moving forward on two hands and two knees to the ground | 29 | 6.8 (5.0) |
| Climb | Walking up or down the stairs or a soft foam climber | 47 | 8.3 (8.0) |
| Ride-on toy | Sitting on a ride-on toy and moving forward using two feet. Sitting without moving forward or sitting and being pushed by an adult, for example, was not considered as “ride-on toy.” | 40 | 10.3 (10.7) |
| Stand | Standing still without lifting a foot. Moving in place was not considered “standing” | 129 | 6.9 (5.0) |
| Sit * | Sitting on the ground for play such as block play. Sitting on a ride-on toy or a slide, for example, was not considered as “sit.” | 84 | 14.5 (9.5) |
| Stroller | Sitting on a stroller or wagon while it is being pushed by an adult | 36 | 12.0 (10.5) |
| Carried | Being held by an adult while the adult is walking. Being held by an adult without walking was not considered as “carried.” | 35 | 9.9 (14.0) |
| Hip Vertical Counts | Hip Vector Magnitudes | Wrist Vertical Counts | Wrist Vector Magnitudes | |
|---|---|---|---|---|
| Estimate ± SE | Estimate ± SE | Estimate ± SE | Estimate ± SE | |
| Run | 145 ± 14 ** | 352 ± 24 ** | 774 ± 41 ** | 1178 ± 62 ** |
| Walk | 52 ± 12 | 191 ± 21 | 345 ± 37 | 596 ± 55 |
| Crawl | 241 ± 14 ** | 410 ± 24 ** | 247 ± 42 | 528 ± 64 |
| Climb | 169 ± 13 ** | 324 ± 22 ** | 249 ± 38 | 432 ± 57 * |
| Ride-on toy | 100 ± 13 ** | 297 ± 22 ** | 182 ± 39 ** | 308 ± 58 ** |
| Stand | 1 ± 12 ** | 19 ± 21 ** | 121 ± 37 ** | 264 ± 55 ** |
| Sit | 8 ± 12 * | 65 ± 21 ** | 189 ± 37 ** | 388 ± 55 ** |
| Stroller | 7 ± 13 * | 57 ± 22 ** | 116 ± 38 ** | 251 ± 57 ** |
| Carried | 149 ± 14 ** | 258 ± 23 * | 289 ± 40 | 519 ± 60 |
| Rank | Feature | D’ | Feature | Feature Importance |
|---|---|---|---|---|
| 1 | FFT SD of z | 0.64 | SD of VM | 0.039 |
| 2 | z FFT max of z | 0.61 | FFT median of y | 0.034 |
| 3 | FFT SD of x | 0.47 | FFT mean weighted of y | 0.033 |
| 4 | SD of z | 0.45 | FFT median of x | 0.027 |
| 5 | FFT max of z | 0.44 | FFT mean weighted of x | 0.026 |
| 6 | Kurtosis of VM | 0.43 | Max of VM | 0.024 |
| 7 | Min of z | 0.41 | FFT mean of y | 0.021 |
| 8 | Kurtosis of y | 0.39 | Min of MV | 0.020 |
| 9 | Min of VM | 0.36 | FFT mean weight of z | 0.019 |
| 10 | SD of x | 0.33 | Kurtosis of VM | 0.018 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, S.; Zavos, P.; Nickele, K.; Sugianto, A.; Albert, M.V. Hip and Wrist-Worn Accelerometer Data Analysis for Toddler Activities. Int. J. Environ. Res. Public Health 2019, 16, 2598. https://doi.org/10.3390/ijerph16142598
Kwon S, Zavos P, Nickele K, Sugianto A, Albert MV. Hip and Wrist-Worn Accelerometer Data Analysis for Toddler Activities. International Journal of Environmental Research and Public Health. 2019; 16(14):2598. https://doi.org/10.3390/ijerph16142598
Chicago/Turabian StyleKwon, Soyang, Patricia Zavos, Katherine Nickele, Albert Sugianto, and Mark V. Albert. 2019. "Hip and Wrist-Worn Accelerometer Data Analysis for Toddler Activities" International Journal of Environmental Research and Public Health 16, no. 14: 2598. https://doi.org/10.3390/ijerph16142598
APA StyleKwon, S., Zavos, P., Nickele, K., Sugianto, A., & Albert, M. V. (2019). Hip and Wrist-Worn Accelerometer Data Analysis for Toddler Activities. International Journal of Environmental Research and Public Health, 16(14), 2598. https://doi.org/10.3390/ijerph16142598