Direct and Indirect Influences of Objective Socioeconomic Position on Adolescent Health: The Mediating Roles of Subjective Socioeconomic Status and Lifestyles



Abstract
:1. Introduction
Research Objectives
2. Materials and Methods
2.1. Participants and Procedure
2.2. Instruments
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics and Correlations
3.2. Measurement Model
3.2.1. Models Including Direct and Indirect Paths of SEP Indicators on Health
3.2.2. Models Including Direct Paths of SEP Indicators on Healthy Lifestyles
3.2.3. Model Including the Effect of the IOSEP on Health Directly and Indirectly through SSS and Lifestyles
3.2.4. Analysis of the Indirect Effects
4. Discussion
4.1. Methodological Considerations and Implications of this Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Solar, O.; Irwin, A. A Conceptual Framework for Action on the Social Determinants of Health; (Social Determinants of Health Discussion Paper 2); World Health Organization: Geneva, Switzerland, 2010; Available online: http://apps.who.int/iris/bitstream/10665/44489/1/9789241500852_eng.pdf (accessed on 20 May 2018).
- Marmot, M.; Bell, R. Fair society, healthy lives. Public Health 2012, 126, S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- West, P.; Sweeting, H. Evidence on equalisation in health in youth from the West of Scotland. Soc. Sci. Med. 2004, 59, 13–27. [Google Scholar] [CrossRef]
- West, P. Health inequalities in the early years: Is there equalisation in youth? Soc. Sci. Med. 1997, 44, 833–858. [Google Scholar] [CrossRef]
- Yngwe, M.Å.; Östberg, V. The family’s economic resources and adolescents’ health complaints—Do adolescents’ own economic resources matter? Eur. J. Public Health 2013, 23, 24–29. [Google Scholar] [CrossRef]
- Richter, M.; Moor, I.; van Lenthe, F.J. Explaining socioeconomic differences in adolescent self-rated health: The contribution of material, psychosocial and behavioural factors. J. Epidemiol. Commun. Health 2012, 66, 691–697. [Google Scholar]
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef]
- Font-Ribera, L.; Garcia-Continente, X.; Carmen Davo-Blanes, M.; Ariza, C.; Díez, E.; García Calvente, M.D.M.; Maroto, G.; Suarez, M.; Rajmil, L.; Grupo de Determinantes Sociales de la Sociedad Española de Epidemiología. The study of social inequalities in child and adolescent health in Spain. Gac. Sanit. 2014, 28, 316–325. [Google Scholar] [CrossRef]
- Galobardes, B.; Lynch, J.; Smith, G.D. Measuring socioeconomic position in health research. Brit. Med. Bull. 2007, 81–82, 21–37. [Google Scholar] [CrossRef]
- Ridolfo, H.; Maitland, A. Factors that influence the accuracy of adolescent proxy reporting of parental characteristics: A research note. J. Adolesc. 2011, 34, 95–103. [Google Scholar] [CrossRef]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Molcho, M.; Gabhainn, S.; Kelleher, C.C. Assessing the use of the Family Affluence Scale (FAS) among Irish schoolchildren. Irish Med. J. 2007, 100, 37–39. [Google Scholar]
- Doku, D.; Koivusilta, L.; Rimpelä, A. Indicators for measuring material affluence of adolescents in health inequality research in developing countries. Child Indic. Res. 2010, 3, 243–260. [Google Scholar] [CrossRef] [PubMed]
- Hollingshead, A.B. Four Factor Index of Social Status; Yale University: New Haven, CT, USA, 1975. [Google Scholar]
- Ray, A.; Wu, M. PISA 2000 Technical Report; OECD Publishing: Paris, France, 2003. [Google Scholar]
- Moreno-Maldonado, C.; Rivera, F.; Ramos, P.; Moreno, C. Measuring the socioeconomic position of adolescents: A proposal for a composite index. Soc. Indic. Res. 2018, 136, 17–538. [Google Scholar] [CrossRef]
- American Psychological Association, Task Force on Socioeconomic Status. Report of the APA Task Force on Socioeconomic Status; American Psychological Association: Washington, DC, USA, 2007. [Google Scholar]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Health Psychol. 2000, 19, 586–592. [Google Scholar] [CrossRef]
- Twenge, J.M.; Campbell, W.K. Self-esteem and socioeconomic status: A meta-analytic review. Pers. Soc. Psychol. Rev. 2002, 6, 59–71. [Google Scholar] [CrossRef]
- Goodman, E.; Huang, B.; Schafer-Kalkhoff, T.; Adler, N.E. Perceived socioeconomic status: A new type of identity that influences adolescents’ self-rated health. J. Adolescent Health 2007, 41, 479–487. [Google Scholar] [CrossRef]
- Elgar, F.; McKinnon, B.; Torsheim, T.; Schnohr, C.W.; Mazur, J.; Cavallo, F.; Currie, C. Patterns of socioeconomic inequality in adolescent health differ according to the measure of socioeconomic position. Soc. Indic. Res. 2016, 127, 1169–1180. [Google Scholar] [CrossRef]
- Huynh, V.W.; Chiang, J.J. Subjective social status and adolescent health: The role of stress and sleep. Youth Soc. 2018, 50, 926–946. [Google Scholar] [CrossRef]
- Ahlborg, M.; Svedberg, P.; Nyholm, M.; Morgan, A.; Nygren, J.M. Socioeconomic inequalities in health among Swedish adolescents - adding the subjective perspective. BMC Public Health 2017, 17, 838. [Google Scholar] [CrossRef]
- Iversen, A.C.; Holsen, I. Inequality in Health, Psychosocial Resources and Health Behavior in Early Adolescence: The Influence of Different Indicators of Socioeconomic Position. Child Indic. Res. 2008, 1, 291–302. [Google Scholar] [CrossRef]
- Sweeting, H.; Hunt, K. Adolescent socio-economic and school-based social status, health and well-being. Soc. Sci. Med. 2014, 121, 39–47. [Google Scholar] [CrossRef]
- Friestad, C.; Klepp, K.-I. Socioeconomic status and health behaviour patterns through adolescence: Results from a prospective cohort study in Norway. Eur. J. Public Health 2006, 16, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Moor, I.; Rathmann, K.; Stronks, K.; Levin, K.; Spallek, J.; Richter, M. Psychosocial and behavioural factors in the explanation of socioeconomic inequalities in adolescent health: A multilevel analysis in 28 European and North American countries. J. Epidemiol. Commun. Health 2014, 68, 912–921. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Promotion Glossary; WHO: Geneva, Switzerland, 1998; Available online: https://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf (accessed on 11 April 2019).
- Dahlgren, G.; Whitehead, M. European Strategies for Tackling Social Inequities in Health: Levelling Up (Part 2) (WHOLIS E89384); World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2006; Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/103824/E89384.pdf (accessed on 6 July 2018).
- Mackenbach, J.P. Health Inequalities: Europe in Profile; An Independent Expert Report Commissioned by and Published under the Auspices of the United Kingdom; Presidency of the European Union: London, UK, 2006; Available online: https://www.who.int/social_determinants/resources/european_inequalities.pdf (accessed on 4 March 2018).
- Richter, M.; Erhart, M.; Vereecken, C.; Zambon, A.; Boyce, W.; Gabhainn, S. The role of behavioural factors in explaining socio-economic differences in adolescent health: A multilevel study in 33 countries. Soc. Sci. Med. 2009, 69, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Fismen, A.-S.; Samdal, O.; Torsheim, T. Family affluence and cultural capital as indicators of social inequalities in adolescent’s eating behaviours: A population-based survey. BMC Public Health 2012, 12, 1036. [Google Scholar] [CrossRef] [PubMed]
- Levin, K.; Currie, C. Inequalities in toothbrushing among adolescents in Scotland 1998–2006. Health Educ. Res. 2009, 24, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Costa-Tutusaus, L.; Guerra-Balic, M. Relationship between healthy lifestyle and sociodemographic factors in adolescents in catalonia: Application of VISA-TEEN Questionnaire. PLoS ONE 2016, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Turrell, G.; Hewitt, B.; Patterson, C.; Oldenburg, B. Measuring socio-economic position in dietary research: Is choice of socio-economic indicator important? Public Health Nutr. 2003, 6, 191–200. [Google Scholar] [CrossRef]
- Hamilton, S.F.; Hamilton, M.A. The transition to adulthood: Challenges of poverty and structural lag. In Handbook of Adolescent Psychology; Lerner, R.M., Steinberg, L., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2009; Volume 2, pp. 492–526. [Google Scholar]
- Moreno, C.; Ramos, P.; Rivera, F.; Jiménez-Iglesias, A.; García-Moya, I.; Sánchez-Queija, I.; Moreno-Maldonado, C.; Paniagua, C.; Villafuerte-Díaz, A.; Morgan, A. Informe técnico de los resultados obtenidos por el Estudio Health Behaviour in School-aged Children (HBSC) 2014 en España; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2016. [Google Scholar]
- Roberts, C.; Freeman, J.; Samdal, O.; Schnohr, C.W.; De Looze, M.; Gabhainn, S.; Iannotti, R.; Rasmussen, M. International HBSC Study Group. The Health Behaviour in School-aged Children (HBSC) study: Methodological developments and current tensions. Int. J. Public Health 2009, 54, 140–150. [Google Scholar] [CrossRef]
- Ramos, P.; Moreno, C.; Rivera, F.; Pérez, P. Integrated analysis of the health and social inequalities of Spanish adolescents. Int. J. Clin. Health Psychol. 2010, 10, 477–498. [Google Scholar]
- Organisation for Economic Co-operation and Development (OECD). Classifying Educational Programmes: Manual for ISCED-97 Implementation in OECD Countries; UNESCO Institute for Statistics: Paris, France, 1999. [Google Scholar]
- International Labour Office. International Standard Classification of Occupations: ISCO-08; ILO: Geneva, Switzerland, 1999. [Google Scholar]
- Currie, C.; Inchley, J.; Molcho, M.; Lenzi, M.; Veselska, Z.; Wild, F. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2013/14 Survey; Child and Adolescent Health Research Unit: St. Andrews University, St. Andrews, Scotland, 2014. [Google Scholar]
- Cantril, H. The pattern of human concerns; Rutgers University Press: New Brunswick, NJ, 1965. [Google Scholar]
- Ravens-Sieberer, U. The European Kidscreen Group. The KIDSCREEN Questionnaires—Quality of Life Questionnaires for Children and Adolescents—Handbook; Pabst Science Publisher: Lengerich, Germany, 2006. [Google Scholar]
- Kearns, A.; Whitley, E.; Bond, L.; Egan, M.; Tannahill, C. The psychosocial pathway to mental well-being at the local level: Investigating the effects of perceived relative position in a deprived area context. J. Epidemiol. Commun. Health 2013, 67, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Erhart, M.; Rajmil, L.; Herdman, M.; Auquier, P.; Bruil, J.; Power, M.; Duer, W.; Abel, T.; Czemy, L. Reliability, construct and criterion validity of the KIDSCREEN-10 score: A short measure for children and adolescents’ well-being and health-related quality of life. Qual. Life Res. 2010, 19, 1487–1500. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; Technical Report No. 916; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Casals-Peidró, E. Hábitos de higiene oral en la población escolar y adulta española. RCOE: Revista del Ilustre Consejo General de Colegios de Odontólogos y Estomatólogos de España 2005, 10, 389–401. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Sallis, J.F.; Long, B. A physical activity screening measure for use with adolescents in primary care. Arch. Pediat. Adol. Med. 2001, 155, 554–559. [Google Scholar] [CrossRef]
- Pate, R.R.; Freedson, P.S.; Sallis, J.F.; Taylor, W.C.; Sirard, J.; Trost, S.G.; Dowda, M. Compliance with physical activity guidelines: Prevalence in a population of children and youth. Ann. Epidemiol. 2002, 12, 303–308. [Google Scholar] [CrossRef]
- Ramos, P.; Rivera, F.; Jiménez-Iglesias, A.; Moreno, C. Análisis de clúster de la actividad física y las conductas sedentarias de los adolescentes españoles, correlación con la salud biopsicosocial. Rev. Psicol. Deporte 2012, 21, 0099–0106. [Google Scholar]
- Leger, D.; Beck, F.; Richard, J.-B.; Godeau, E. Total sleep time severely drops during adolescence. PLoS ONE 2012, 7, e45204. [Google Scholar] [CrossRef]
- Botello-Harbaum, M.; Haynie, D.L.; Murray, K.W.; Iannotti, R.J. Cigarette smoking status and recurrent subjective health complaints among US school-aged adolescents. Child Care Health Dev. 2011, 37, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Zaborskis, A.; Sumskas, L.; Maser, M.; Pudule, I. Trends in drinking habits among adolescents in the Baltic countries over the period of transition: HBSC survey results, 1993–2002. BMC Public Health 2006, 6, 77. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2003. [Google Scholar]
- Enders, C.K.; Bandalos, D.L. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Struct. Equ. Model. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Joreskog, K.; Sorbom, D. LISREL VIII: Analysis of Linear Structural Relations; Scientific Software: Mooresville, IN, USA, 1992. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.-T.; Wen, Z. In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct. Equ. Model. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Martin-Storey, A.; Marcellin, S.; Purtell, K.M.; Tougas, A.M.; Lessard, A. “It’s about having money, but also happiness:” A qualitative investigation of how adolescents understand subjective status in themselves and others. J. Adolesc. 2018, 68, 198–206. [Google Scholar] [CrossRef]
- Elgar, F.; Pförtner, T.-K.; Moor, I.; De Clercq, B.; Stevens, G.W.; Currie, C. Socioeconomic inequalities in adolescent health 2002–2010: A time-series analysis of 34 countries participating in the Health Behaviour in School-aged Children study. Lancet 2015, 385, 2088–2095. [Google Scholar] [CrossRef]
- Pfortner, T.K.; Guenther, S.; Levin, K.A.; Torsheim, T.; Richter, M. The use of parental occupation in adolescent health surveys. An application of ISCO-based measures of occupational status. J. Epidemiol. Commun. Health 2015, 69, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G.; Pickett, K.E. Income inequality and population health: A review and explanation of the evidence. Soc. Sci. Med. 2006, 62, 1768–1784. [Google Scholar] [CrossRef] [PubMed]
- Bosma, H.; Brandts, L.; Simons, A.; Groffen, D.; van den Akker, M. Low socioeconomic status and perceptions of social inadequacy and shame: Findings from the Dutch SMILE study. Eur. J. Public Health 2014, 25, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Quon, E.C.; McGrath, J.J. Subjective socioeconomic status and adolescent health: A meta-analysis. Health Psychol. 2014, 33, 433. [Google Scholar] [CrossRef] [PubMed]
- Quon, E.C.; McGrath, J.J. Community, family, and subjective socioeconomic status: Relative status and adolescent health. Health Psychol. 2015, 34, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Jarrin, D.C.; McGrath, J.J.; Quon, E.C. Objective and subjective socioeconomic gradients exist for sleep in children and adolescents. Health Psychol. 2014, 33, 301. [Google Scholar] [CrossRef] [PubMed]
- Madruga, C.S.; Laranjeira, R.; Caetano, R.; Pinsky, I.; Zaleski, M.; Ferri, C.P. Use of licit and illicit substances among adolescents in Brazil: A national survey. Addict. Behav. 2012, 37, 1171–1175. [Google Scholar] [CrossRef]
- Borg, V.; Kristensen, T.S. Social class and self-rated health: Can the gradient be explained by differences in life style or work environment? Soc. Sci. Med. 2000, 51, 1019–1030. [Google Scholar] [CrossRef]
- Thrane, C. Explaining educational-related inequalities in health: Mediation and moderator models. Soc. Sci. Med. 2006, 62, 467–478. [Google Scholar] [CrossRef]
- Woodward, M.; Oliphant, J.; Lowe, G.; Tunstall-Pedoe, H. Contribution of contemporaneous risk factors to social inequality in coronary heart disease and all causes mortality. Prev. Med. 2003, 36, 561–568. [Google Scholar] [CrossRef]
- Torsheim, T.; Currie, C.; Boyce, W.; Samdal, O. Country material distribution and adolescents’ perceived health: Multilevel study of adolescents in 27 countries. J. Epidemiol. Commun. Health 2006, 60, 156–161. [Google Scholar] [CrossRef]
- Koivusilta, L.K.; Rimpela, A.H.; Kautiainen, S.M. Health inequality in adolescence. Does stratification occur by familial social background, family affluence, or personal social position? BMC Public Health 2006, 6, 1–13. [Google Scholar]
- Goodman, E.; Adler, N.E.; Kawachi, I.; Frazier, A.L.; Huang, B.; Colditz, G.A. Adolescents’ perceptions of social status: Development and evaluation of a new indicator. Pediatrics 2001, 108, E31. [Google Scholar] [CrossRef]
- Senn, T.E.; Walsh, J.L.; Carey, M.P. The mediating roles of perceived stress and health behaviors in the relation between objective, subjective, and neighborhood socioeconomic status and perceived health. Ann. Behav. Med. 2014, 48, 215–224. [Google Scholar] [CrossRef]
- De Vries, H.; van’t Riet, J.; Spigt, M.; Metsemakers, J.; van den Akker, M.; Vermunt, J.K.; Kremers, S. Clusters of lifestyle behaviors: Results from the Dutch SMILE study. Prev. Med. 2008, 46, 203–208. [Google Scholar] [CrossRef]
- Donovan, J.E.; Jessor, R.; Costa, F.M. Adolescent health behavior and conventionality-unconventionality: An extension of problem-behavior therapy. Health Psychol. 1991, 10, 52. [Google Scholar] [CrossRef]
- Stone-Romero, E.F.; Rosopa, P.J. The relative validity of inferences about mediation as a function of research design characteristics. Organ. Res. Methods 2008, 11, 326–352. [Google Scholar] [CrossRef]
- Seltzer, M.M.; Greenberg, J.S.; Floyd, F.J.; Pettee, Y.; Hong, J. Life course impacts of parenting a child with a disability. Am. J. Ment. Retard. 2001, 106, 265–286. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measures to Assess Socioeconomic Status | |
| Objective Socioeconomic Status. It was assessed using IOSEP (Index of Objective Socioeconomic Position), comprised of: | |
| Education level of both parents | Scored on 4 levels, parental educational level was evaluated by the question “What level of education do your father and mother have?” The response options for the question referring to each parent were: “Never studied (does not know how to read or write, or does so with difficulty)”;“Basic/primary studies finished or unfinished” (specifying: “Something similar to what I am studying now” for the 11–12 year-old participants); “Secondary studies (like high-school or vocational school), finished or unfinished” (specifying: “They studied at a higher level than what I am currently studying” for the 11–12 year-old participants); “University studies, finished or unfinished”. The four education-levels corresponded with the International Standard Classification of Education (ISCED) adopted by the UNESCO General Conference in 1997 [41]: ISCED 0; ISCED 1-2; ISCED 3-4; and ISCED 5-6. |
| Occupational status of both parents | Classified in the 10 categories proposed by the International Standard Classification of Occupations (ISCO-08) at the highest level of aggregation [42], and adding an extra category to include unemployment. |
| Family Affluence Scale (FAS) | FAS was used to measure family material wealth through the six items that make up the latest version of the instrument [43]: Number of family cars or family computers, own bedrooms, number of bathrooms at home, family dishwasher, and family holidays abroad. Alpha reliability for the 6-item scale was 0.96, indicating excellent internal consistency. |
| Subjective Socioeconomic Status | |
| Perceived family wealth | It was assessed by the question: “How well-off do you think your family is?” The question has been used in the HBSC study since 1994 as an indicator of the adolescents’ subjective socioeconomic status. The 5 response options were classified in 4 categories: 1 (poor), 2 (not very poor), 3 (normal), and 4 (rich or very rich). |
| Measures to Evaluate Health | |
| GHS: Global Health Score. Composed of: | |
| Life satisfaction | Evaluated through the instrument “Cantril Ladder Scale” [44], which ranges from 0 the lowest perception of life satisfaction to 4 the highest. |
| Heath-related quality of life | Assessed through the instrument “Kidscreen”, consisting of 10 items that evaluate aspects of physical, psychological, and social health in a Likert scale of 5 points [45]. Alpha reliability for the 10-item scale was 0.83. |
| Self-reported health | Adolescents were asked how they rated their health with four response options: excellent, good, passable, or poor [46,47]. |
| Psychosomatic complaints | An HBSC-symptom checklist [48] was employed asking adolescents how often in the last six months they had experienced certain symptoms. Response options for each symptom ranged from “almost every day” to “rarely or never”, and the maximum frequency of experiencing any psychological or somatic symptom was calculated. The 8-item scale showed an alpha Combrach of 0.83 indicating good internal consistency. |
| Measures to Evaluate Healthy Lifestyles | |
| Global score of healthy lifestyles | |
| Frequency of breakfast | The adolescents were asked: “How often do you have breakfast (something more than a glass of milk or fruit juice)?” The responses were classified from 0—infrequently (never or almost never), 1—irregular (from 2 to 6 days a week), 2—daily (7 days a week). |
| Eating habits | The specific question was: “How many times a week do you eat/drink fruit/vegetables/sweets/sugary soft drinks?” The response categories collected information about the weekly consumption frequency of the cited products, classifying the responses in three categories. In the case of fruits and vegetables: 0—infrequently (never or less than once a week), 1—irregularly (from 1 to 6 times a week), 2—daily (every day, and every day more than once a day). In the case of sweets and soft drinks, the responses were classified in the same way but inversely, with daily consumption being the least healthy (0). Current scientific evidence [49] was taken into consideration for the categorization of the responses as more or less healthy in the case of frequency of breakfast and dietary habits. |
| Tooth brushing | Evaluated with the question “How often do you brush your teeth?” The responses were classified in the following categories: 0—irregularly or never (less than once a day), 1—daily (once a day), 2—optimal (more than once a day). At least twice a day is an indicator of a universally accepted healthy lifestyle [50]. |
| Physical activity | Physical activity was evaluated by two questions adapted for their use in the HBSC [51]: (1) number of days over the past 7 days in which the adolescents were physically active for at least 60 minutes a day (moderate-to-vigorous physical activity), classified in three categories: 0—infrequently (less than two days a week), 1—irregularly (from 3 to 4 days a week), 2—regularly (5 days or more a week); (2) frequency that adolescents performed some physical activity in their free time that made them sweat or out of breath (vigorous physical activity), which was classified in three categories: 0—infrequently (never or less than once a month), 1—irregularly (once a month or once a week), 2—regularly (two days a week or more). The classification of more- or less-healthy behavior was based on recommendations established in scientific literature [52,53]. |
| Hours of sleep | An average score of the number of hours a day that adolescents sleep was calculated and classified in 3 groups according to criteria establishing a minimum of 8-hours of sleep for optimal rest in adolescence [54]. The responses were classified in 3 groups: 0—insufficient (less than 6.5 hours), 1—sufficient (between 6.5 and 7.5 hours) and 2—optimal rest (at least 8 hours of sleep). |
| Tobacco use | Assessed through the question: “How often do you smoke tobacco at present?” with 4 response options: “every day”, “smoke, at least once a week, but not every day”, “less than once a week” and “never smoked”. The responses were classified into three groups: 0—daily smokers, 1—experimenters (smoke, at least once a week, but not every day or less than once a week), and 2—never smoked. This classification has been previously employed [55]. |
| Alcohol consumption | Assessed by asking about their frequency of drinking beer, wine/sparkling wine, spirits/liquor, alcopops, and other alcoholic beverages, with 5 response options for each item: every day, every week, every month, rarely, and never. The maximum frequency of alcohol consumption was calculated independently of the type of alcoholic beverage, and were re-coded in 0—regular users (used at least one of the alcoholic beverages every week or more often); 1—irregular users (drank alcohol every month or every week); and 3—not users of alcohol (answered never for all alcoholic beverages). These categories have been used in previous HBSC studies [56]. |
| Mean | SD | Min. Max | n | % | % Missing | |
|---|---|---|---|---|---|---|
| Index of Objective Socioeconomic Position | 0.04 | 1.73 | (−5.32, 4.32) | 35.3 | ||
| Father’s occupational status | (1, 10) | 19.0 | ||||
| Unemployed | 1640 | 10.7 | ||||
| Elementary Occupations | 492 | 3.2 | ||||
| Plant and Machine Operators Assemblers | 1500 | 9.8 | ||||
| Craft and Related Trades Workers | 2400 | 15.6 | ||||
| Skilled Agricultural, Forestry and Fishery Workers | 873 | 5.7 | ||||
| Services and Sales Workers | 1817 | 11.8 | ||||
| Clerical Support Workers | 414 | 2.7 | ||||
| Technicians and Associate Professionals | 1135 | 7.4 | ||||
| Professionals | 1322 | 8.6 | ||||
| Managers | 829 | 5.4 | ||||
| Mother’s occupation | (1, 10) | 13.9 | ||||
| Unemployed | 4478 | 29.2 | ||||
| Elementary Occupations | 1410 | 9.2 | ||||
| Plant and Machine Operators Assemblers | 203 | 1.3 | ||||
| Craft and Related Trades Workers | 405 | 2.6 | ||||
| Skilled Agricultural, Forestry and Fishery Workers | 149 | 1.0 | ||||
| Services and Sales Workers | 2978 | 19.4 | ||||
| Clerical Support Workers | 886 | 5.8 | ||||
| Technicians and Associate Professionals | 710 | 4.6 | ||||
| Professionals | 1703 | 11.1 | ||||
| Managers | 291 | 1.9 | ||||
| Father’s educational level | (1, 4) | 6.4 | ||||
| Pre-primary education | 232 | 1.5 | ||||
| Basic education | 4914 | 32.0 | ||||
| Secondary education | 5466 | 35.6 | ||||
| Higher education | 3752 | 24.5 | ||||
| Mother’s educational level | (1, 4) | 3.5 | ||||
| Pre-primary education | 257 | 1.7 | ||||
| Basic education | 4390 | 28.6 | ||||
| Secondary education | 5364 | 35.0 | ||||
| Higher education | 4797 | 31.3 | ||||
| Family Affluence Scale | 9.13 | 2.15 | (1, 14) | 9.4 | ||
| Subjective Socioeconomic Status | (1, 5) | 7.1 | ||||
| Poor | 121 | 0.8 | ||||
| Very poor | 812 | 5.3 | ||||
| Normal | 1037 | 6.8 | ||||
| Rich | 340 | 2.2 | ||||
| Very rich | 1377 | 9 | ||||
| Global Health Score | 0.13 | 0.97 | (−5.02, 2.69) | 20.6 | ||
| Life satisfaction | 8.78 | 2.02 | (1, 11) | 10.2 | ||
| Health-related quality of life | 35.22 | 4.56 | (10, 50) | 19.0 | ||
| Self-reported health | (1, 4) | 9.8 | ||||
| Poor | 116 | 0.8 | ||||
| Passable | 918 | 6.0 | ||||
| Good | 6963 | 45.4 | ||||
| Excellent | 5834 | 38.0 | ||||
| Psychosomatic complaints | (1, 5) | 9.8 | ||||
| Rarely | 2310 | 15.1 | ||||
| Never | 2957 | 19.3 | ||||
| Often | 1938 | 12.6 | ||||
| About every week | 2921 | 19.0 | ||||
| About every day | 3717 | 24.2 | ||||
| Healthy lifestyles score | 15.94 | 2.81 | (3, 22) | 29.00 |
| n | % | % Missing | |
|---|---|---|---|
| Breakfast consumption | 8.7 | ||
| Infrequently | 663 | 4.3 | |
| Irregular | 3634 | 23.7 | |
| Daily | 9705 | 63.3 | |
| Fruit consumption | 2.1 | ||
| Infrequently | 1835 | 12.0 | |
| Irregular | 7954 | 51.9 | |
| Daily | 5229 | 34.1 | |
| Vegetables consumption | 3.1 | ||
| Infrequently | 1598 | 10.4 | |
| Irregular | 10,089 | 65.8 | |
| Daily | 3180 | 20.7 | |
| Sweets consumption | 2.8 | ||
| Daily | 1977 | 12.9 | |
| Irregular | 8673 | 56.5 | |
| Infrequently | 4264 | 27.8 | |
| Sugary-drinks consumption | 3.1 | ||
| Daily | 3120 | 20.3 | |
| Irregular | 7826 | 51.0 | |
| Infrequently | 3913 | 25.5 | |
| Tooth brushing | 1.9 | ||
| Irregularly/never | 1144 | 7.5 | |
| Frequent | 3863 | 25.2 | |
| Optimal | 10,045 | 65.5 | |
| Moderate-to-vigorous physical activity | 5.1 | ||
| Irregular | 2655 | 17.3 | |
| Infrequently | 4468 | 29.1 | |
| Optimal | 7434 | 48.5 | |
| Vigorous physical activity | 14.2 | ||
| Infrequently | 1627 | 10.6 | |
| Irregular | 2018 | 13.2 | |
| Optimal | 9516 | 62.0 | |
| Hours of sleep | 3.3 | ||
| Insufficient | 637 | 4.2 | |
| Sufficient | 2269 | 14.8 | |
| Optimal rest | 11,921 | 77.7 | |
| Tobacco use | 3.3 | ||
| Daily | 435 | 2.8 | |
| Experimental | 722 | 4.7 | |
| Never | 13,672 | 89.1 | |
| Alcohol consumption | 2.1 | ||
| Weekly | 735 | 4.8 | |
| Infrequent | 5110 | 33.3 | |
| Never | 9172 | 59.8 | |
| Single Socioeconomic Objective Indicators | SSS | GHS | Single Health Indicators | HLS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.1 | 1.2 | 1.3 | 1.4 | 1.5 | 2 | 3 | 3.1 | 3.2 | 3.3 | 3.4 | 4 | ||
| 1 | IOSEP | 0.66 | 0.57 | 0.74 | 0.72 | 0.60 | 0.24 | 0.16 | 0.13 | 0.12 | 0.12 | −0.08 | 0.23 |
| 1.1 | OCC F | 0.22 | 0.36 | 0.26 | 0.28 | 0.16 | 0.09 | 0.08 | 0.06 | 0.07 | −0.05 | 0.12 | |
| 1.2 | OCC M | 0.23 | 0.38 | 0.24 | 0.11 | 0.06 | 0.05 | 0.03 | 0.05 | −0.05 | 0.10 | ||
| 1.3 | EDL F | 0.54 | 0.24 | 0.12 | 0.12 | 0.08 | 0.10 | 0.089 | −0.07 | 0.20 | |||
| 1.4 | EDL M | 0.27 | 0.12 | 0.13 | 0.09 | 0.11 | 0.10 | −0.07 | 0.21 | ||||
| 1.5 | FAS | 0.29 | 0.15 | 0.14 | 0.11 | 0.11 | −0.06 | 0.12 | |||||
| 2 | SSS | 0.18 | 0.18 | 0.13 | 0.14 | −0.09 | 0.07 | ||||||
| 3 | GHS | 0.78 | 0.84 | 0.60 | −0.51 | 0.39 | |||||||
| 3.1 | LS | 0.50 | 0.32 | −0.29 | 0.29 | ||||||||
| 3.2 | HRQoL | 0.38 | −0.29 | 0.35 | |||||||||
| 3.3 | SRH | −0.22 | 0.24 | ||||||||||
| 3.4 | PSC | −0.24 | |||||||||||
| Model 1 | Model 2 | Model 3 | Model 3b a | Model 4 b | Model 6 | Model 7 | |
|---|---|---|---|---|---|---|---|
| χ² | 343.92 | 55.62 | 1489.99 | 737.86 | 236.92 | 1424.03 | 883.14 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| gl | 24 | 5 | 32 | 31 | 7 | 12 | 39 |
| CFI | 0.981 | 0.990 | 0.913 | 0.960 | 0.979 | 0.873 | 0.967 |
| TLI | 0.971 | 0.981 | 0.878 | 0.941 | 0.954 | 0.778 | 0.940 |
| RMSA (CI 90%) | 0.029 (0.027, 0.032) | 0.027 (0.021, 0.034) | 0.057 (0.054, 0.059) | 0.039 (0.036, 0.041) | 0.046 (0.041, 0.051) | 0.091 (0.087, 0.095) | 0.038 (0.035, 0.040) |
| SRMR | 0.019 | 0.011 | 0,005 | 0.026 | 0.021 | 0.065 | 0.027 |
| Effects | B | SE | p | 95% CI |
|---|---|---|---|---|
| Models including only direct effects on health | ||||
| IOSEP (Model 1) | 0.265 | 0.014 | <0.001 | [0.238; 0.210] |
| R2 | 0.070 | |||
| SSS (Model 2) | 0.217 | 0.012 | <0.001 | [0.193; 0.241] |
| R2 | 0.047 | |||
| IOSEP (Model 3) | 0.215 | 0.014 | <0.001 | [0.187; 0.242] |
| SSS | 0.182 | 0.013 | <0.001 | [0.157; 0.207] |
| R2 | 0.079 | |||
| Models including only direct effects on healthy lifestyles | ||||
| IOSEP (Model 4) | 0.283 | 0.012 | <0.001 | [0.259; 0.307] |
| R2 | 0.080 | |||
| SSS (Model 5) | 0.062 | 0.010 | <0.001 | [0.041; 0.082] |
| R2 | 0.004 | |||
| IOSEP (Model 6) | 0.281 | 0.013 | <0.001 | [0.256; 0.305] |
| SSS | 0.013 | 0.011 | ns, 0.214 | [−0.008; 0.034] |
| R2 | 0.079 | |||
| Single mediator model (Model 3b) | ||||
| IOSEP to mediator (SSS) | 0.321 | 0.013 | <0.001 | [0.296; 0.347] |
| Mediator (SSS) to health | 0.146 | 0.013 | <0.001 | [0.120; 0.172] |
| Total effect of IOSEP on health | 0.271 | 0.014 | <0.001 | [0.244; 0.298] |
| Direct effect of IOSEP on health | 0.224 | 0.015 | <0.001 | [0.195; 0.253] |
| Total indirect effect of IOSEP on health through SSS | 0.047 | 0.005 | <0.001 | [0.038; 0.056] |
| R2 | 0.092 | |||
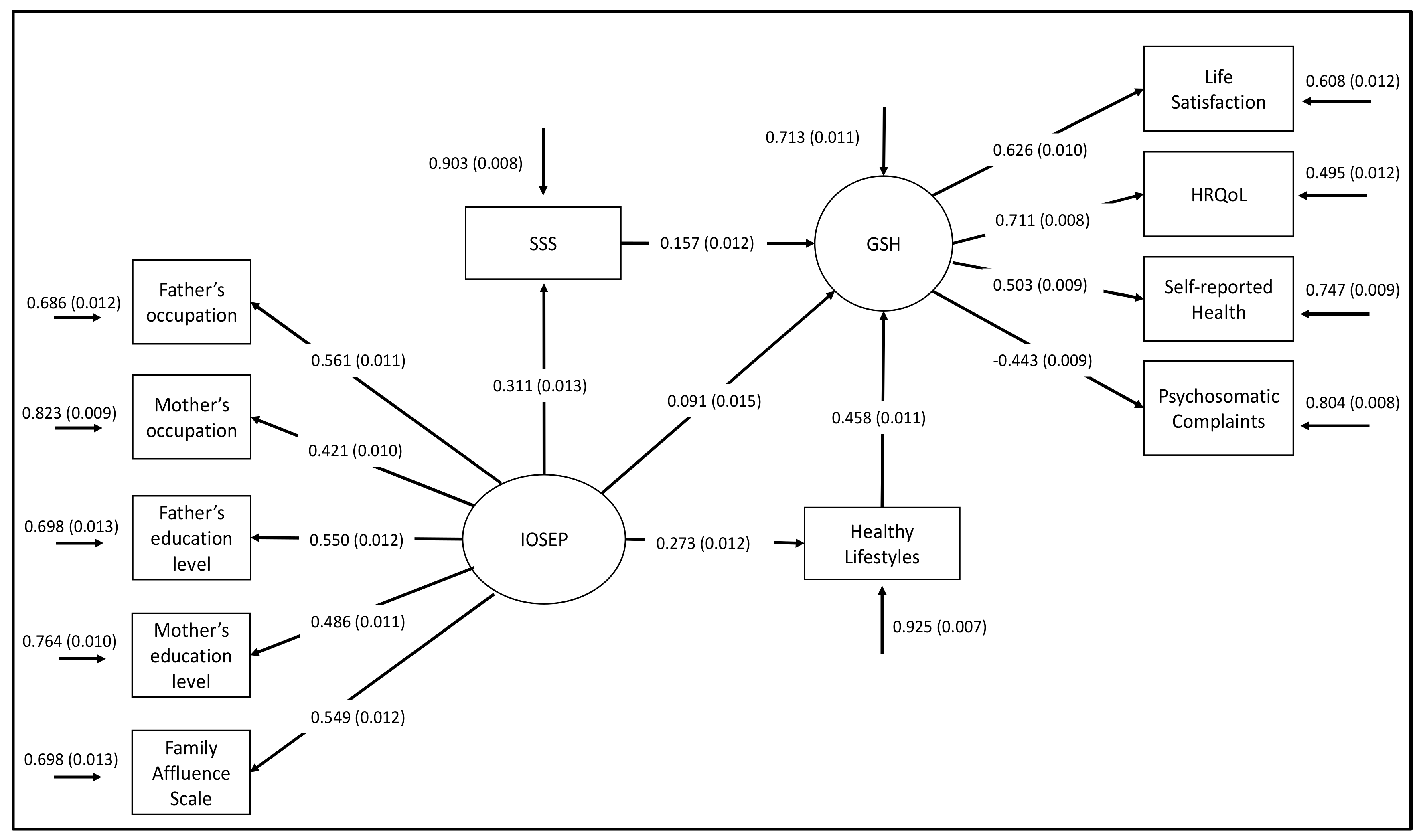
| Multiple mediator model (Model 7) | ||||
| IOSEP to mediators | ||||
| SSS | 0.311 | 0.013 | <0.001 | [0.286; 0.337] |
| Healthy lifestyles | 0.273 | 0.012 | <0.001 | [0.250; 0.297] |
| Mediator to health | ||||
| SSS | 0.157 | 0.012 | <0.001 | [0.133; 0.182] |
| Healthy lifestyles | 0.458 | 0.011 | <0.001 | [0.436; 0.480] |
| Total effect of IOSEP on health | 0.265 | 0.013 | <0.001 | [0.239; 0.291] |
| Direct effect of IOSEP on health | 0.091 | 0.015 | <0.001 | [0.062; 0.120] |
| Total indirect effect of IOSEP on health through mediators | 0.174 | 0.007 | <0.001 | [0.160; 0.188] |
| SSS | 0.049 | 0.004 | <0.001 | [0.040; 0.058] |
| Healthy lifestyles | 0.125 | 0.006 | <0.001 | [0.113; 0.137] |
| R2 | 0.287 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Maldonado, C.; Ramos, P.; Moreno, C.; Rivera, F. Direct and Indirect Influences of Objective Socioeconomic Position on Adolescent Health: The Mediating Roles of Subjective Socioeconomic Status and Lifestyles. Int. J. Environ. Res. Public Health 2019, 16, 1637. https://doi.org/10.3390/ijerph16091637
Moreno-Maldonado C, Ramos P, Moreno C, Rivera F. Direct and Indirect Influences of Objective Socioeconomic Position on Adolescent Health: The Mediating Roles of Subjective Socioeconomic Status and Lifestyles. International Journal of Environmental Research and Public Health. 2019; 16(9):1637. https://doi.org/10.3390/ijerph16091637
Chicago/Turabian StyleMoreno-Maldonado, Concepción, Pilar Ramos, Carmen Moreno, and Francisco Rivera. 2019. "Direct and Indirect Influences of Objective Socioeconomic Position on Adolescent Health: The Mediating Roles of Subjective Socioeconomic Status and Lifestyles" International Journal of Environmental Research and Public Health 16, no. 9: 1637. https://doi.org/10.3390/ijerph16091637
APA StyleMoreno-Maldonado, C., Ramos, P., Moreno, C., & Rivera, F. (2019). Direct and Indirect Influences of Objective Socioeconomic Position on Adolescent Health: The Mediating Roles of Subjective Socioeconomic Status and Lifestyles. International Journal of Environmental Research and Public Health, 16(9), 1637. https://doi.org/10.3390/ijerph16091637