Determinants of Occupational Safety Culture in Hospitals and other Workplaces—Results from an Integrative Literature Review


Abstract
:1. Introduction
- What are possible determinants of occupational safety culture from the perspective of employees in different workplaces (hospital, construction, manufacturing, and other industry sectors)?
- What implications for further research on determinants of occupational safety culture for the hospital workplace can be derived by comparing the hospital workplace with other workplaces?
2. Materials and Methods
2.1. Literature Search
2.1.1. Search Strategy
2.1.2. Inclusion and Exclusion Criteria
- “Sample”: The targeted sample comprised employees at different workplaces. Investigated workplaces were hospital workplaces and other workplaces (e.g., construction, manufacturing, services, and other industry sectors). We excluded studies conducted in some countries (Israel, Iran, Africa, Chile and Korea) [25,26,27,28,29,30,31,32,33,34,35], due to the difficulties to compare the results to the German healthcare system. Furthermore, we excluded studies at nuclear power stations or in the oil and gas industry since the comparison with workplaces in construction and manufacturing was of primary interest to us. In addition, the nuclear power and gas industries often focus on the prevention of accidents/serious incidents, whereas we were interested in the occupational safety culture “in everyday life”.
- “Phenomenon of Interest”: We included studies that described different determinants of an occupational safety culture. We excluded studies in which occupational safety culture at the workplace was not the main aspect.
- “Design”: We intended to consider studies with different research methods (questionnaire, qualitative interviews, focus group discussions).
- “Evaluation”: Studies of interest included the perceptions and experiences of employees on occupational safety culture. We used the seven clusters from Cornelissen et al. as a raster to evaluate and sort the determinants that were assessed in the individual studies.
- “Research type”: We included studies with different research designs (qualitative, quantitative, mixed-method) aiming to gain a more comprehensive view on utilized determinants of an occupational safety culture in different workplaces. We excluded intervention studies on occupational safety culture or on occupational safety as we did not want to evaluate the effects of individual interventions. Our interest was focused on the determinants identified in the studies.
2.1.3. Literature Search
2.1.4. Screening and Selection Procedure
2.2. Data Evaluation
2.2.1. Critical Appraisal
2.2.2. Data Analysis
3. Results
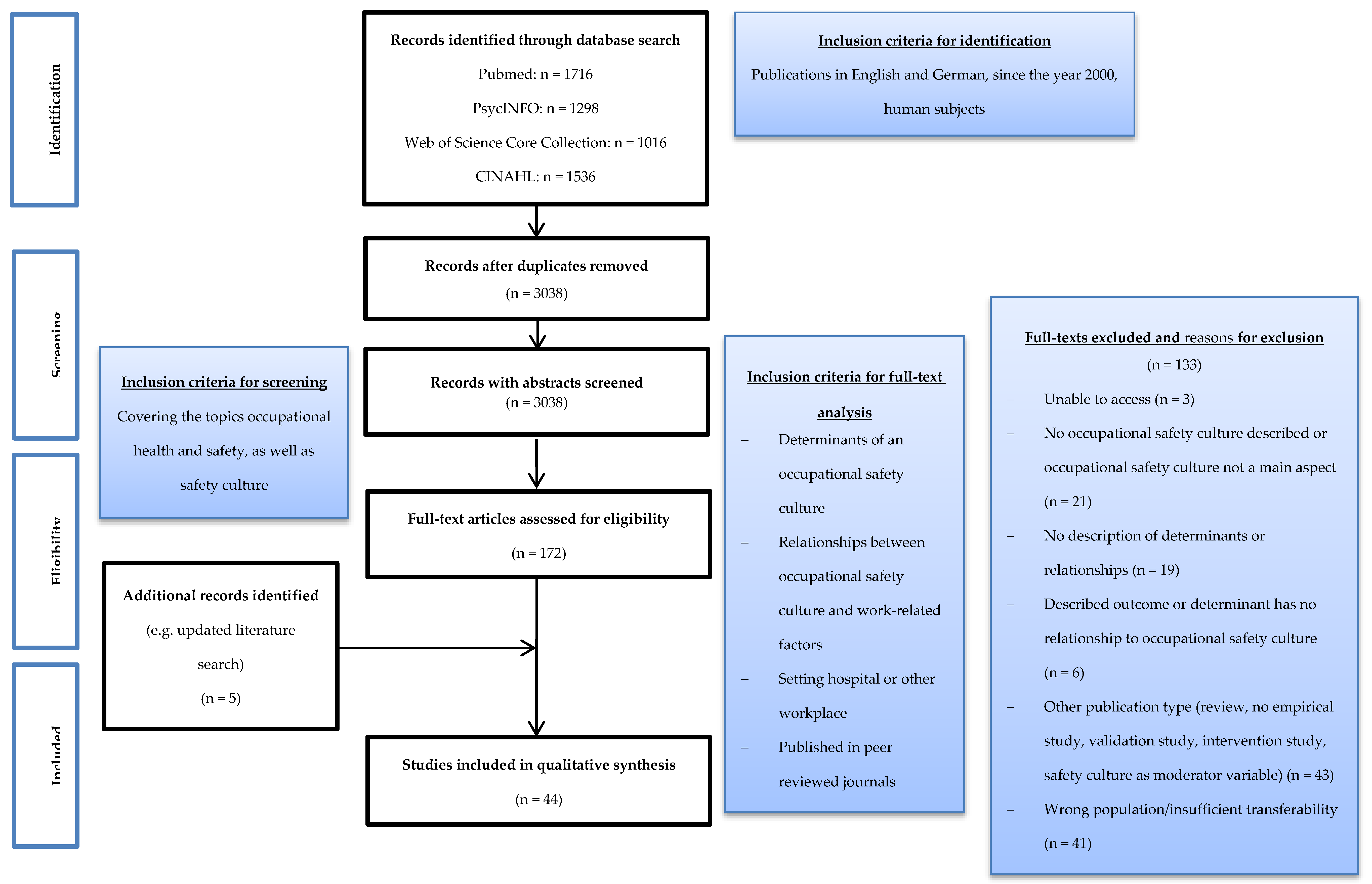
3.1. Summary of Search Results
3.2. Characteristics of Included Studies.
3.3. Determinants of An Occupational Safety Culture
3.3.1. Cluster “Workplace Characteristics and Circumstances”
3.3.2. Cluster “Climate and Culture”
3.3.3. Cluster “Management and Colleagues”
3.3.4. Cluster “Employee Characteristics”
3.3.5. Cluster “External (Factors)”
3.3.6. Cluster “Performance”
3.3.7. Cluster “Safety Outcomes”
3.3.8. Classification of the Studies into the Topics and Categories according to Cornelissen et al.
4. Discussion
4.1. Determinants of An Occupational Safety Culture
4.1.1. Cluster “Workplace Characteristics and Circumstances”
4.1.2. Cluster “Climate and Culture”
4.1.3. Cluster “Management and Colleagues”
4.1.4. Cluster “Employee Characteristics”
4.1.5. Cluster “External (Factors)”
4.1.6. Cluster “Performance”
4.1.7. Cluster “Safety Outcomes”
4.2. Summary and Recommendations for Future Studies
4.3. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zohar, D. Safety climate: Conceptualization, measurement, and improvement. In Handbook of Occupational Health Psychology, 2nd ed.; Le Quick, J.C.T., Ed.; American Psychological Association: Washington, DC, USA, 2011. [Google Scholar]
- He, Y.; Wang, Y.; Payne, S.C. How is safety climate formed? A meta-analysis of the antecedents of safety climate. Organ. Psychol. Rev. 2019, 9, 124–156. [Google Scholar] [CrossRef]
- Beus, J.M.; McCord, M.A.; Zohar, D. Workplace safety. Organ. Psychol. Rev. 2016, 6, 352–381. [Google Scholar] [CrossRef]
- Clarke, S. An integrative model of safety climate: Linking psychological climate and work attitudes to individual safety outcomes using meta-analysis. J. Occup. Organ. Psychol. 2010, 83, 553–578. [Google Scholar] [CrossRef]
- Cornelissen, P.A.; van Hoof, J.J.; De Jong, M.D.T. Determinants of safety outcomes and performance: A systematic literature review of research in four high-risk industries. J. Saf. Res. 2017, 62, 127–141. [Google Scholar] [CrossRef]
- Halligan, M.; Zecevic, A. Safety culture in healthcare: A review of concepts, dimensions, measures and progress. BMJ Qual. Saf. 2011, 20, 338–343. [Google Scholar] [CrossRef]
- Pumar-Méndez, M.J.; Attree, M.; Wakefield, A. Methodological aspects in the assessment of safety culture in the hospital setting: A review of the literature. Nurse Educ. Today 2014, 34, 162–170. [Google Scholar] [CrossRef]
- Weaver, M.D.; Wang, H.E.; Fairbanks, R.J.; Patterson, D. The association between EMS workplace safety culture and safety outcomes. Prehosp. Emerg. Care 2012, 16, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.A.; Dominici, F.; Agnew, J.; Gerwin, D.; Morlock, L.; Miller, M.R. Do nurse and patient injuries share common antecedents? An analysis of associations with safety climate and working conditions. BMJ Qual. Saf. 2012, 21, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Wagner, A.; Rieger, M.A.; Manser, T.; Sturm, H.; Hardt, J.; Martus, P.; Lessing, C.; Hammer, A. Healthcare professionals’ perspectives on working conditions, leadership, and safety climate: A cross-sectional study. BMC Health Serv. Res. 2019, 19, 53. [Google Scholar] [CrossRef]
- Wagner, A.; Hammer, A.; Manser, T.; Martus, P.; Sturm, H.; Rieger, M.A. Do Occupational and Patient Safety Culture in Hospitals Share Predictors in the Field of Psychosocial Working Conditions? Findings from a Cross-Sectional Study in German University Hospitals. Int. J. Environ. Res. Public Health 2018, 15, 2131. [Google Scholar] [CrossRef] [Green Version]
- Wagner, A.; Michaelis, M.; Luntz, E.; Wittich, A.; Schrappe, M.; Lessing, C.; Rieger, M.A. Assessment of Patient and Occupational Safety Culture in Hospitals: Development of a Questionnaire with Comparable Dimensions and Results of a Feasibility Study in a German University Hospital. Int. J. Environ. Res. Public Health 2018, 15, 2625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturm, H.; Rieger, M.A.; Martus, P.; Ueding, E.; Wagner, A.; Holderried, M.; Maschmann, J. Do perceived working conditions and patient safety culture correlate with objective workload and patient outcomes: A cross-sectional explorative study from a German university hospital. PLoS ONE 2019, 14, e0209487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnew, C.; Flin, R.; Mearns, K. Patient safety climate and worker safety behaviours in acute hospitals in Scotland. J. Saf. Res. 2013, 45, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Trinkoff, A.M.; Le, R.; Geiger-Brown, J.; Lipscomb, J. Work schedule, needle use, and needlestick injuries among registered nurses. Infect. Control. Hosp. Epidemiol. 2007, 28, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Wicker, S.; Ludwig, A.-M.; Gottschalk, R.; Rabenau, H.F. Needlestick injuries among health care workers: Occupational hazard or avoidable hazard? Wien. Klin. Wochenschr. 2008, 120, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.M.; Slade, M.D.; Cantley, L.F.; Sakr, C.J. Evaluation of safety climate and employee injury rates in healthcare. Occup. Environ. Med. 2016, 73, 595–599. [Google Scholar] [CrossRef] [PubMed]
- McVicar, A. Workplace stress in nursing: A literature review. Adv. Nurs. 2003, 44, 633–642. [Google Scholar] [CrossRef]
- Schwatka, N.V.; Hecker, S.; Goldenhar, L.M. Defining and Measuring Safety Climate: A Review of the Construction Industry Literature. Ann. Occup. Hyg. 2016, 60, 537–550. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Verma, A. A review, simple meta-analysis and future directions of safety climate research in manufacturing organizations. Int. J. Occup. Saf. Ergon. 2018, 1–26. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology: Methodological issues in nursing research. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Luria, G.; Yagil, D. Safety perception referents of permanent and temporary employees: Safety climate boundaries in the industrial workplace. Accid. Anal. Prev. 2010, 42, 1423–1430. [Google Scholar] [CrossRef]
- Luria, G. The social aspects of safety management: Trust and safety climate. Accid. Anal. Prev. 2010, 42, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Zohar, D. A group-level model of safety climate: Testing the effect of group climate on microaccidents in manufacturing jobs. J. Appl. Psychol. 2000, 85, 587–596. [Google Scholar] [CrossRef]
- Zohar, D. The effects of leadership dimensions, safety climate, and assigned priorities on minor injuries in work groups. J. Organiz. Behav. 2002, 23, 75–92. [Google Scholar] [CrossRef]
- Zohar, D.; Luria, G. Climate as a social-cognitive construction of supervisory safety practices: Scripts as proxy of behavior patterns. J. Appl. Psychol. 2004, 89, 322–333. [Google Scholar] [CrossRef]
- Zarei, E.; Khakzad, N.; Reniers, G.; Akbarid, R. On the relationship between safety climate and occupational burnout in healthcare organizations. Saf. Sci. 2016, 89, 1–10. [Google Scholar] [CrossRef]
- Khosravi, Y.; Asilian-Mahabadi, H.; Hajizadeh, E.; Hassanzadeh-Rangi, N.; Bastani, H.; Khavanin, A.; Mortazavi, S.B. Modeling the Factors Affecting Unsafe Behavior in the Construction Industry from Safety Supervisors’ Perspective - PubMed. J. Res. Health Sci. 2014, 14, 29–35. [Google Scholar]
- Gyekye, S.A. Workers’ perceptions of workplace safety and job satisfaction. Int. J. Occup. Saf. Ergon. 2005, 11, 291–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyekye, S.A.; Salminen, S. Are “good soldiers” safety conscious? An examination of the relationship between organizational citizenship behaviors and perception of workplace safety. Soc. Behav. Personal. 2005, 33, 805–820. [Google Scholar] [CrossRef]
- Gyekye, S.A.; Salminen, S. Workplace safety perceptions and perceived organizational support: Do supportive perceptions influence safety perceptions? Int. J. Occup. Saf. Ergon. 2007, 13, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Dalal, R.S. Climate as situational strength: Safety climate strength as a cross-level moderator of the relationship between conscientiousness and safety behaviour. Eur. J. Work Organ. Psychol. 2016, 25, 120–132. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Specialist Unit for Review Evidence. Questions to Assist with the Critical Appraisal of Cross-Sectional Studies. Available online: https://www.cardiff.ac.uk/__data/assets/pdf_file/0010/1142974/SURE-CA-form-for-Cross-sectional_2018.pdf (accessed on 9 September 2020).
- Specialist Unit for Review Evidence. Questions to Assist with the Critical Appraisal of Cohort Studies. Available online: https://www.cardiff.ac.uk/__data/assets/pdf_file/0006/1142997/SURE-CA-form-for-Cohort_2018.pdf (accessed on 9 September 2020).
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. Educ. Inf. 2018, 34, 285–291. [Google Scholar]
- Davies, M. Concept mapping, mind mapping and argument mapping: What are the differences and do they matter? High. Educ. 2011, 62, 279–301. [Google Scholar] [CrossRef]
- Aljabri, D.; Vaughn, A.; Austin, M.; White, L.; Li, Z.; Naessens, J.; Spaulding, A. An Investigation of Healthcare Worker Perception of Their Workplace Safety and Incidence of Injury. Workplace Health Saf. 2020, 68, 214–225. [Google Scholar] [CrossRef]
- Beus, J.M.; Bergman, M.E.; Payne, S.C. The influence of organizational tenure on safety climate strength: A first look. Accid. Anal. Prev. 2010, 42, 1431–1437. [Google Scholar] [CrossRef]
- Brondino, M.; Silva, S.A.; Pasini, M. Multilevel approach to organizational and group safety climate and safety performance: Co-workers as the missing link. Saf. Sci. 2012, 50, 1847–1856. [Google Scholar] [CrossRef]
- Bronkhorst, B.; Vermeeren, B. Safety climate, worker health and organizational health performance. Int. J. Workplace Health Manag. 2016, 9, 270–289. [Google Scholar] [CrossRef]
- Bunner, J.; Prem, R.; Korunka, C. How Work Intensification Relates to Organization-Level Safety Performance: The Mediating Roles of Safety Climate, Safety Motivation, and Safety Knowledge. Front. Psychol. 2018, 9, 2575. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; McCabe, B.; Hyatt, D. Impact of individual resilience and safety climate on safety performance and psychological stress of construction workers: A case study of the Ontario construction industry. J. Saf. Res. 2017, 61, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Clarke, S.; Ward, K. The role of leader influence tactics and safety climate in engaging employees’ safety participation. Risk Anal. 2006, 26, 1175–1185. [Google Scholar] [CrossRef] [PubMed]
- Dal Corso, L. Mediation effects of safety climate and safety motivation on the relation between organizational climate and safety performance in the workplace. TPM 2008, 15, 77–90. [Google Scholar]
- DeJoy, D.M.; Schaffer, B.S.; Wilson, M.G.; Vandenberg, R.J.; Butts, M.M. Creating safer workplaces: Assessing the determinants and role of safety climate. J. Saf. Res. 2004, 35, 81–90. [Google Scholar] [CrossRef] [PubMed]
- DeJoy, D.M.; Della, L.J.; Vandenberg, R.J.; Wilson, M.G. Making work safer: Testing a model of social exchange and safety management. J. Saf. Res. 2010, 41, 163–171. [Google Scholar] [CrossRef]
- Fernández-Muñiz, B.; Montes-Peón, J.M.; Vázquez-Ordás, C.J. Safety culture: Analysis of the causal relationships between its key dimensions. J. Saf. Res. 2007, 38, 627–641. [Google Scholar] [CrossRef]
- Fernández-Muñiz, B.; Montes-Peón, J.M.; Vázquez-Ordás, C.J. Safety climate in OHSAS 18001-certified organisations: Antecedents and consequences of safety behaviour. Accid. Anal. Prev. 2012, 45, 745–758. [Google Scholar] [CrossRef]
- Garcia, A.M.; Boix, P.; Canosa, C. Why do workers behave unsafely at work? Determinants of safe work practices in industrial workers. Occup. Environ. Med. 2004, 61, 239–246. [Google Scholar]
- Gershon, R.R.; Karkashian, C.D.; Grosch, J.W.; Murphy, L.R.; Escamilla-Cejudo, A.; Flanagan, P.A.; Bernacki, E.; Kasting, C.; Martin, L. Hospital safety climate and its relationship with safe work practices and workplace exposure incidents. Am. J. Infect. Control. 2000, 28, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.A.; Neal, A. Perceptions of Safety at Work: A Framework for Linking Safety Climate to Safety Performance, Knowledge, and Motivation. J. Occup. Health Psychol. 2000, 5, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Halbesleben, J.R.B.; Leroy, H.; Dierynck, B.; Simons, T.; Savage, G.T.; McCaughey, D.; Leon, M.R. Living up to safety values in health care: The effect of leader behavioral integrity on occupational safety. J. Occup. Health Psychol. 2013, 18, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Hicks, G.; Buttigieg, D.; de Cieri, H. Safety climate, strain and safety outcomes. J. Manag. Organ. 2016, 22, 19–31. [Google Scholar] [CrossRef]
- Huang, Y.-H.; Ho, M.; Smith, G.S.; Chen, P.Y. Safety climate and self-reported injury: Assessing the mediating role of employee safety control. Accid. Anal. Prev. 2006, 38, 425–433. [Google Scholar] [CrossRef]
- Kath, L.M.; Magley, V.J.; Marmet, M. The role of organizational trust in safety climate’s influence on organizational outcomes. Accid. Anal. Prev. 2010, 42, 1488–1497. [Google Scholar] [CrossRef]
- Katz, A.S.; Pronk, N.P.; McLellan, D.; Dennerlein, J.; Katz, J.N. Perceived Workplace Health and Safety Climates: Associations with Worker Outcomes and Productivity. Am. J. Prev. Med. 2019, 57, 487–494. [Google Scholar] [CrossRef]
- Larsson, S.; Pousette, A.; Törner, M. Psychological climate and safety in the construction industry-mediated influence on safety behaviour. Saf. Sci. 2008, 46, 405–412. [Google Scholar] [CrossRef]
- Manapragada, A.; Bruk-Lee, V.; Thompson, A.H.; Heron, L.M. When safety climate is not enough: Examining the moderating effects of psychosocial hazards on nurse safety performance. J. Adv. Nurs. 2019, 75, 1207–1218. [Google Scholar] [CrossRef]
- McCaughey, D.; McGhan, G.; DelliFraine, J.L.; Brannon, S.D. Perception is reality: How patients contribute to poor workplace safety perceptions. Health Care Manag. Rev. 2011, 36, 18–27. [Google Scholar] [CrossRef]
- McCaughey, D.; DelliFraine, J.L.; McGhan, G.; Bruning, N.S. The negative effects of workplace injury and illness on workplace safety climate perceptions and health care worker outcomes. Saf. Sci. 2013, 51, 138–147. [Google Scholar] [CrossRef]
- McCaughey, D.; DelliFraine, J.; Erwin, C.O. Best practices to promote occupational safety and satisfaction: A comparison of three North American hospitals. Adv. Health Care Manag. 2015, 17, 137–159. [Google Scholar] [CrossRef] [PubMed]
- McLinton, S.S.; Dollard, M.F.; Tuckey, M.R. New perspectives on psychosocial safety climate in healthcare: A mixed methods approach. Saf. Sci. 2018, 109, 236–245. [Google Scholar] [CrossRef]
- McLinton, S.S.; Afsharian, A.; Dollard, M.F.; Tuckey, M.R. The dynamic interplay of physical and psychosocial safety climates in frontline healthcare. Stress Health 2019, 35, 650–664. [Google Scholar] [CrossRef] [PubMed]
- Milijić, N.; Mihajlović, I.; Nikolić, D.; Živković, Ž. Multicriteria analysis of safety climate measurements at workplaces in production industries in Serbia. Int. J. Ind. Ergon. 2014, 44, 510–519. [Google Scholar] [CrossRef]
- Neal, A.; Griffin, M.A.; Hart, P. The impact of organizational climate on safety climate and individual behavior. Saf. Sci. 2000, 34, 99–109. [Google Scholar] [CrossRef]
- Neal, A.; Griffin, M.A. A study of the lagged relationships among safety climate, safety motivation, safety behavior, and accidents at the individual and group levels. J. Appl. Psychol. 2006, 91, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Nixon, A.E.; Lanz, J.J.; Manapragada, A.; Bruk-Lee, V.; Schantz, A.; Rodriguez, J.F. Nurse safety: How is safety climate related to affect and attitude? Work Stress 2015, 29, 401–419. [Google Scholar] [CrossRef]
- Nordlöf, H.; Wiitavaara, B.; Högberg, H.; Westerling, R. A cross-sectional study of factors influencing occupational health and safety management practices in companies. Saf. Sci. 2017, 95, 92–103. [Google Scholar] [CrossRef]
- Oliver, A.; Tomás, J.M.; Cheyne, A. Safety climate: Its nature and predictive power. Psychol. Spain 2006, 10, 28–36. [Google Scholar]
- Pandit, B.; Albert, A.; Patil, Y.; Al-Bayati, A.J. Impact of safety climate on hazard recognition and safety risk perception. Saf. Sci. 2019, 113, 44–53. [Google Scholar] [CrossRef]
- Probst, T.M. Safety and insecurity: Exploring the moderating effect of organizational safety climate. J. Occup. Health Psychol. 2004, 9, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Probst, T.M.; Brubaker, T.L.; Barsotti, A. Organizational injury rate underreporting: The moderating effect of organizational safety climate. J. Appl. Psychol. 2008, 93, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Probst, T.M. Organizational safety climate and supervisor safety enforcement: Multilevel explorations of the causes of accident underreporting. J. Appl. Psychol. 2015, 100, 1899–1907. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.A.; Arezes, P.M.; Leão, C.P. Safety climate and its relationship with furniture companies’ safety performance and workers’ risk acceptance. Theor. Issues Ergon. Sci. 2015, 16, 412–428. [Google Scholar] [CrossRef] [Green Version]
- Schwatka, N.V.; Rosecrance, J.C. Safety climate and safety behaviors in the construction industry: The importance of co-workers commitment to safety. Work 2016, 54, 401–413. [Google Scholar] [CrossRef]
- Silver, S.R.; Boiano, J.M. Differences in Safety Climate Perception by Health Care Worker, Work Schedule, and Workplace Characteristics. Am. J. Med. Qual. 2019, 34, 165–175. [Google Scholar] [CrossRef]
- Stone, P.W.; Gershon, R.R.M. Nurse work environments and occupational safety in intensive care units. Policy Polit. Nurs. Pract. 2006, 7, 240–247. [Google Scholar] [CrossRef]
- Tholén, S.L.; Pousette, A.; Törner, M. Causal relations between psychosocial conditions, safety climate and safety behaviour–A multi-level investigation. Saf. Sci. 2013, 55, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Tomás, J.M.; Cheyne, A.; Oliver, A. The Relationship Between Safety Attitudes and Occupational Accidents. Eur. Psychol. 2011, 16, 209–219. [Google Scholar] [CrossRef]
- Zadow, A.J.; Dollard, M.F.; Mclinton, S.S.; Lawrence, P.; Tuckey, M.R. Psychosocial safety climate, emotional exhaustion, and work injuries in healthcare workplaces. Stress Health 2017, 33, 558–569. [Google Scholar] [CrossRef] [PubMed]
- EU-OSHA. Foresight on New and Emerging Occupational Safety and Health Risks Associated with Digitalisation by 2025: European Risk Observatory Report. Available online: https://osha.europa.eu/sites/default/files/publications/documents/Foresight_new_OSH_risks_2025_report.pdf (accessed on 9 September 2020).
- McCaughey, D.; Halbesleben, J.R.B.; Savage, G.T.; Simons, T.; McGhan, G.E. Safety leadership: Extending workplace safety climate best practices across health care workforces. Adv. Health Care Manag. 2013, 14, 189–217. [Google Scholar] [CrossRef] [PubMed]
- Christian, M.S.; Bradley, J.C.; Wallace, J.C.; Burke, M.J. Workplace safety: A meta-analysis of the roles of person and situation factors. J. Appl. Psychol. 2009, 94, 1103–1127. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cluster | Topics and Categories |
|---|---|
| 1. Workplace characteristics and circumstances | Physical work environment: Company size, workplace hazards, safety equipment, safety of equipment, physical workplace (design) Work characteristics: work characteristics, perceived workplace safety, goal setting, stress, shifts, working hours, job demands, job resources, production pressure, task clarity, safety control Workforce: contract type, job level, workforce quantity, workforce composition, unions, HR |
| 2. Climate and culture | Organizational climate and culture: Organizational climate, organizational culture Safety climate and culture: safety climate, safety culture |
| 3. Management and colleagues | Management attitudes and behaviours: leadership style, management attitudes, management behaviours, safety importance for management Co-worker attitudes and behaviours: co-worker attitudes, co-worker behaviours Management of safety: management of safety, inspections, accident analysis and record keeping, safety representations, sanctions, rewards, accident reducing measures, training, safety communication, safety policies and procedures, safety meetings and activities |
| 4. Employee characteristics | Employee demographics: age, gender, education, disabilities, psychophysical states Career and job attitudes: tenure/experience, employee work attitudes, trust Safety characteristics: employee safety attitudes, safety motivation, safety knowledge (sharing), responsibility Lifestyle: work-life balance, marital status, children, lifestyle, lifestyle disorders and substance abuse |
| 5. External | Governmental bodies: law and legislation, governmental bodies Stakeholders: client involvement, customer satisfaction Socio-economic: economic factors, insurance, and costs of safety |
| 6. Performance | Safety-related performance: safety performance, PPE use, safety compliance, safety participation Organizational performance: organizational performance, financial performance, (employee) work performance, organizational quality performance, production performance, environmental performance |
| 7. Safety outcomes | Incidents Accidents Injuries |
| Author and Year of Publication | (1) Workplace Characteristics and Circumstances | (2) Climate and Culture | (3) Management and Colleagues | (4) Employee Characteristics | (5) External | (6) Performance | (7) Safety Outcomes | Summary of Investigated Factors (According to Cornelissen et al. [5]) |
|---|---|---|---|---|---|---|---|---|
| Aljabri et al. 2020 [41] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Bronkhorst et al. 2016 [44] | X | X | X | X | (1) (3) (4) (7) | |||
| Dal Corso 2008 [48] | X | X | X | X | (2) (3) (4) (6) | |||
| Gershon et al. 2000 [54] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Halbesleben et al. 2013 [56] | X | X | X | (3) (6) (7) | ||||
| Manapragada et al. 2019 [62] | X | X | X | (1) (3) (6) | ||||
| McCaughey et al. 2011 [63] | X | X | (1) (3) | |||||
| McCaughey et al. 2013 [64] | X | X | X | X | (1) (3) (4) (7) | |||
| McCaughey et al. 2015 [65] | X | X | X | X | (1) (3) (4) (7) | |||
| McLinton et al. 2018 [66] | X | X | X | X | (1) (3) (4) (7) | |||
| McLinton et al. 2019 [67] | X | X | X | X | (1) (3) (4) (7) | |||
| Neal et al. 2000 [69] | X | X | X | X | X | (1) (2) (3) (4) (6) | ||
| Neal et al. 2006 [70] | X | X | X | X | (3) (4) (6) (7) | |||
| Nixon et al. 2015 [71] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Silver et al. 2019 [80] | X | X | X | (1) (3) (4) | ||||
| Stone et al. 2006 [81] | X | X | X | X | (1) (2) (4) (7) | |||
| Zadow et al. 2017 [84] | X | X | X | X | (1) (3) (4) (7) | |||
| Summary of counting | 14/17 | 3/17 | 16/17 | 14/17 | 0/17 | 8/17 | 12/17 |
| Author and Year of Publication | (1) Workplace Characteristics and Circumstances | (2) Climate and Culture | (3) Management and Colleagues | (4) Employee Characteristics | (5) External | (6) Performance | (7) Safety Outcomes | Summary of Investigated Factors (According to Cornelissen et al. [5]) |
|---|---|---|---|---|---|---|---|---|
| Beus et al. 2010 [42] | X | X | X | (1) (3) (4) | ||||
| Brondino et al. 2012 [43] | X | X | X | X | (1) (3) (4) (6) | |||
| Bunner et al. 2018 [45] | X | X | X | X | (1) (3) (4) (6) | |||
| Chen et al. 2017 [46] | X | X | X | X | (1) (3) (4) (7) | |||
| Clarke et al. 2006 [47] | X | X | X | X | (1) (3) (4) (6) | |||
| DeJoy et al. 2004 [49] | X | X | X | X | (1) 3) (4) (6) | |||
| DeJoy et al. 2010 [50] | X | X | X | X | X | X | (1) (2) (3) (4) (6) (7) | |
| Fernández-Muñiz et al. 2007 [51] | X | X | X | X | (3) (4) (6) (7) | |||
| Fernández-Muñiz et al. 2012 [52] | X | X | X | X | X | X | (1) (3) (4) (5) (6) (7) | |
| Garcia et al. 2004 [53] | X | X | X | X | (1) (3) (4) (6) | |||
| Griffin et al. 2000 [55] | X | X | X | (1) (3) (4) (6) | ||||
| Hicks et al. 2016 [57] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Huang et al. 2006 [58] | X | X | X | (3) (4) (7) | ||||
| Kath et al. 2010 [59] | X | X | X | X | (1) (3) (4) (7) | |||
| Katz et al. 2019 [60] | X | X | X | X | (1) (4) (6) (7) | |||
| Larsson et al. 2008 [61] | X | X | X | (1) (4) (6) | ||||
| Milijić et al. 2014 [68] | X | X | X | X | (1) (3) (4) (7) | |||
| Nordlöf et al. 2017 [72] | X | X | X | X | X | X | (1) (3) (4) (5) (6) (7) | |
| Oliver et al. 2006 [73] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Pandit et al. 2019 [74] | X | X | X | X | (1) (3) (4) (7) | |||
| Probst et al. 2004 [75] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Probst et al. 2008 [76] | X | X | (3) (7) | |||||
| Probst et al. 2015 [77] | X | X | (3) (7) | |||||
| Rodrigues et al. 2015 [78] | X | X | X | X | (1) (3) (4) (6) | |||
| Schwatka et al. 2016 [79] | X | X | (3) (6) | |||||
| Tholén et al. 2013 [82] | X | X | X | (1) (3) (6) | ||||
| Tomás et al. 2011 [83] | X | X | X | X | X | (1) (3) (4) (6) (7) | ||
| Summary of counting | 21/27 | 1/27 | 25/27 | 23/27 | 2/27 | 19/27 | 16/27 |
| Cluster | Categories | Studies at Hospital Workplace | Studies at other Workplaces |
|---|---|---|---|
| 1. Workplace characteristics and circumstances | Physical work environment | [54,63,71,80,81] | [42,49,53,57,60,68,72,73,78,83] |
| Work characteristics | [41,44,62,63,64,65,66,67,69,80,84] | [42,43,45,46,49,50,52,53,57,59,60,61,72,74,75,82] | |
| Workforce | [41,44,64,66,80,84] | [43,45,46,47,53,57,60,68,72,73] | |
| 2. Climate and culture | Organizational climate and culture | [48,69,81] | [50] |
| Safety climate and culture | |||
| 3. Management and colleagues | Management attitudes and behaviours | [41,44,48,54,56,62,63,64,65,66,67,69,70,80,84] | [43,45,46,47,49,50,51,52,55,57,58,59,68,72,74,75,77,78,79,82,83] |
| Co-worker attitudes and behaviours | [44,63,64,65] | [43,46,49,79] | |
| Management of safety | [44,54,62,63,64,65,66,67,69,71,80,84] | [42,43,45,46,49,50,51,52,53,55,57,58,59,68,72,73,75,76,77,78,82,83] | |
| 4. Employee characteristics | Employee demographics | [41,44,54,64,65,66,80,81,84] | [43,46,47,49,53,57,60,68,72,73,78] |
| Career and job attitudes | [41,44,64,65,66,71,80,81] | [42,43,46,47,49,50,52,53,59,60,61,68,78] | |
| Safety characteristics | [48,65,69,70] | [45,46,51,55,59,61,68,72,73,74,75,83] | |
| Lifestyle | [44,67] | [50,60] | |
| 5. External | Governmental bodies | ||
| Stakeholders | [52] | ||
| Socio-economic | [72] | ||
| 6. Performance | Safety-related performance | [41,48,54,56,62,69,70,71] | [43,45,47,49,50,51,52,53,55,57,58,61,72,73,75,78,79,82,83] |
| Organizational performance | [52,60,72] | ||
| 7. Safety outcomes | Incidents | [66,67] | [46,72] |
| Accidents | [70] | [50,68,73,75,77,83] | |
| Injuries | [41,54,56,64,65,71,81,84] | [51,52,58,59,74,75,76,77] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, A.; Schöne, L.; Rieger, M.A. Determinants of Occupational Safety Culture in Hospitals and other Workplaces—Results from an Integrative Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6588. https://doi.org/10.3390/ijerph17186588
Wagner A, Schöne L, Rieger MA. Determinants of Occupational Safety Culture in Hospitals and other Workplaces—Results from an Integrative Literature Review. International Journal of Environmental Research and Public Health. 2020; 17(18):6588. https://doi.org/10.3390/ijerph17186588
Chicago/Turabian StyleWagner, Anke, Ladina Schöne, and Monika A. Rieger. 2020. "Determinants of Occupational Safety Culture in Hospitals and other Workplaces—Results from an Integrative Literature Review" International Journal of Environmental Research and Public Health 17, no. 18: 6588. https://doi.org/10.3390/ijerph17186588
APA StyleWagner, A., Schöne, L., & Rieger, M. A. (2020). Determinants of Occupational Safety Culture in Hospitals and other Workplaces—Results from an Integrative Literature Review. International Journal of Environmental Research and Public Health, 17(18), 6588. https://doi.org/10.3390/ijerph17186588