Factors Contributing to CO Uptake and Elimination in the Body: A Critical Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Scope and Search Strategy
2.2. Inclusion and Exclusion Criteria
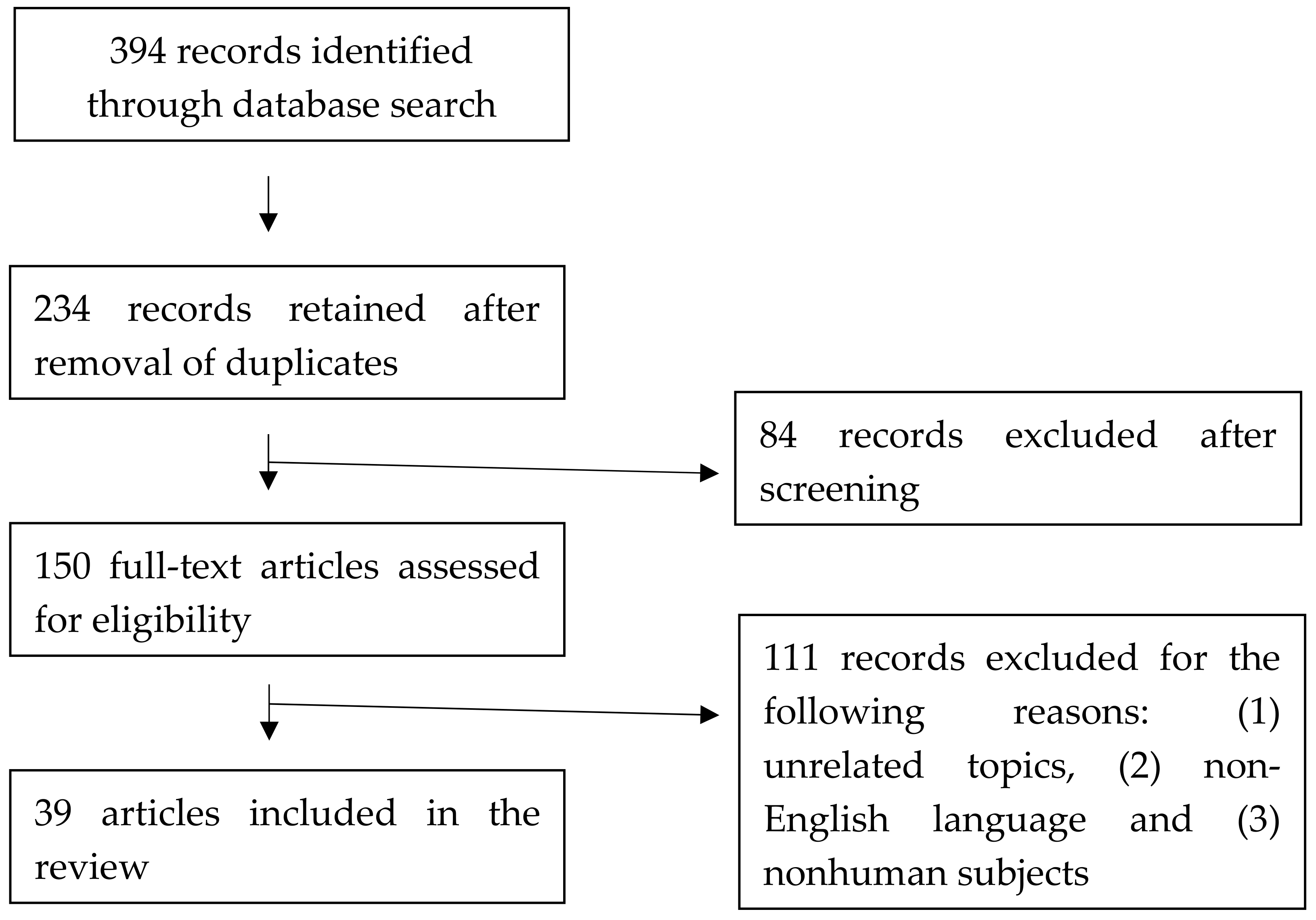
2.3. Search Results and Study Characteristics
3. Results and Discussion
3.1. Environmental Factors
3.1.1. CO Concentration in Ambient Air and Duration
3.1.2. Oxygen Concentration in Ambient Air
3.1.3. Altitude
3.2. Demographic Factors
3.2.1. Age
3.2.2. Sex
3.2.3. Smoking
3.2.4. Exercise
3.3. Physiological Factors
3.3.1. Lung Function
Ventilation Rate
Diffusion Capacity of CO (DLCO)
Chronic Obstructive Pulmonary Disease (COPD)
3.3.2. Cardiovascular Function
Blood Volume
Haemoglobin Mass
Diffusion Rate of CO Flux from Blood to Muscle Compartment
Muscle Mass
Anaemia
3.4. Treatment Factors
3.4.1. 100% Oxygen
3.4.2. HBO Therapy
3.4.3. Carbogen
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Coburn, R.F.; Forster, R.E.; Kane, P.B. Considerations of the physiological variables that determine the blood carboxyhemoglobin concentration in man. J. Clin. Investig. 1965, 44, 1899–1910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barañano, D.E.; Snyder, S.H. Neural roles for heme oxygenase: Contrasts to nitric oxide synthase. Proc. Natl. Acad. Sci. USA 2001, 98, 10996–11002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, M.C. Carbon monoxide poisoning. CMAJ 1985, 133, 392–399. [Google Scholar] [PubMed]
- Blumenthal, I. Carbon monoxide poisoning. J. R. Soc. Med. 2001, 94, 270–272. [Google Scholar] [CrossRef]
- Kao, L.W.; Nanagas, K.A. Carbon monoxide poisoning. Emerg. Med. Clin. North. Am. 2004, 22, 985–1018. [Google Scholar] [CrossRef] [Green Version]
- Weaver, L.K.; Hopkins, R.O.; Chan, K.J.; Churchill, S.; Elliott, C.G.; Clemmer, T.P.; Orme, J.F., Jr.; Thomas, F.O.; Morris, A.H. Hyperbaric oxygen for acute carbon monoxide poisoning. N. Engl. J. Med. 2002, 347, 1057–1067. [Google Scholar] [CrossRef]
- Erupaka, K.; Bruce, E.N.; Bruce, M.C. Prediction of Extravascular Burden of Carbon Monoxide (CO) in the Human Heart. Ann. Biomed. Eng. 2010, 38, 403–438. [Google Scholar] [CrossRef]
- Peterson, J.E.; Stewart, R.D. Predicting the carboxyhemoglobin levels resulting from carbon monoxide exposures. J. Appl. Physiol. 1975, 39, 633. [Google Scholar] [CrossRef]
- Weaver, L.K.; Howe, S.; Hopkins, R.; Chan, K.J. Carboxyhemoglobin half-life in carbon monoxide-poisoned patients treated with 100% oxygen at atmospheric pressure. Chest 2000, 117, 801–808. [Google Scholar] [CrossRef] [Green Version]
- Brochu, P.; Brodeur, J.; Krishnan, K. Derivation of cardiac output and alveolar ventilation rate based on energy expenditure measurements in healthy males and females. J. Appl. Toxicol. 2012, 32, 564–580. [Google Scholar] [CrossRef]
- Hsia, C.C.W. Respiratory Function of Hemoglobin. N. Engl. J. Med. 1998, 338, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Morgan, T.J. The oxyhaemoglobin dissociation curve in critical illness. Crit. Care Resusc. 1999, 1, 93–100. [Google Scholar] [PubMed]
- Forbes, W.H.; Sargent, F.; Roughton, F.J.W. The rate of carbon monoxide uptake by normal men. Am. J. Physiol. 1945, 143, 594–608. [Google Scholar] [CrossRef]
- Benignus, V.A.; Hazucha, M.J.; Smith, M.V.; Bromberg, P.A. Prediction of carboxyhemoglobin formation due to transient exposure to carbon monoxide. J. Appl. Physiol. 1994, 76, 1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, M.C.; Bruce, E.N. Analysis of factors that influence rates of carbon monoxide uptake, distribution, and washout from blood and extravascular tissues using a multicompartment model. J. Appl. Physiol. 2006, 100, 1171. [Google Scholar] [CrossRef]
- Collier, C.R.; Goldsmith, J.R. Interactions of carbon monoxide and hemoglobin at high altitude. Atmos. Environ. 1983, 17, 723–728. [Google Scholar] [CrossRef]
- Bueno, V.; Sant’Anna, O.A.; Lord, J.M. Ageing and myeloid-derived suppressor cells: Possible involvement in immunosenescence and age-related disease. Age 2014, 36, 9729. [Google Scholar] [CrossRef] [Green Version]
- Aziz, A.; Hansen, H.S.; Sechtem, U.; Prescott, E.; Ong, P. Sex-Related Differences in Vasomotor Function in Patients With Angina and Unobstructed Coronary Arteries. J. Am. Coll. Cardiol. 2017, 70, 2349–2358. [Google Scholar] [CrossRef]
- Klasner, A.E.; Smith, S.R.; Thompson, M.W.; Scalzo, A.J. Carbon monoxide mass exposure in a pediatric population. Acad. Emerg. Med. 1998, 5, 992–996. [Google Scholar] [CrossRef]
- Zavorsky, G.S.; Tesler, J.; Rucker, J.; Fedorko, L.; Duffin, J.; Fisher, J.A. Rates of carbon monoxide elimination in males and females. Physiol. Rep. 2014, 2, e12237. [Google Scholar] [CrossRef]
- Peterson, J.E.; Stewart, R.D. Absorption and Elimination of Carbon Monoxide by Inactive Young Men. Arch. Environ. Health Int. J. 1970, 21, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Pace, N.; Strajman, E.; Walker, E.L. Acceleration of Carbon Monoxide Elimination in Man by High Pressure Oxygen. Science 1950, 111, 652. [Google Scholar] [CrossRef] [PubMed]
- Burney, R.E.; Wu, S.-C.; Nemiroff, M.J. Mass carbon monoxide poisoning: Clinical effects and results of treatment in 184 victims. Ann. Emerg. Med. 1982, 11, 394–399. [Google Scholar] [CrossRef]
- Marshall, M.D.; Kales, S.N.; Christiani, D.C.; Goldman, R.H. Are reference intervals for carboxyhemoglobin appropriate? A survey of Boston area laboratories. Clin. Chem. 1995, 41, 1434. [Google Scholar] [CrossRef]
- Castleden, C.M.; Cole, P.V. Carboxyhaemoglobin levels of smokers and non-smokers working in the City of London. Br. J. Ind. Med. 1975, 32, 115–118. [Google Scholar] [CrossRef] [Green Version]
- Filley, G.F.; MacIntosh, D.J.; Wright, G.W. Carbon monoxide uptake and pulmonary diffusing capacity in normal subjects at rest and during exercise. J. Clin. Investig. 1954, 33, 530–539. [Google Scholar] [CrossRef] [Green Version]
- Tikuisis, P.; Kane, D.M.; McLellan, T.M.; Buick, F.; Fairburn, S.M. Rate of formation of carboxyhemoglobin in exercising humans exposed to carbon monoxide. J. Appl. Physiol. 1992, 72, 1311. [Google Scholar] [CrossRef]
- Penney, D.G. Carbon Monoxide, 1st ed.; CRC Press: Boca Raton, FL, USA, 1996. [Google Scholar]
- Selvakumar, S.; Sharan, M.; Singh, M.P. A Mathematical Model for the Elimination of Carbon Monoxide in Humans. J. Theor. Biol. 1993, 162, 321–336. [Google Scholar] [CrossRef]
- Kreck, T.; Shade, E.; Lamm, W.; McKinney, S.; Hlastala, M. Isocapnic Hyperventilation Increases Carbon Monoxide Elimination and Oxygen Delivery. Am. J. Respir. Crit. Care Med. 2001, 163, 458–462. [Google Scholar] [CrossRef] [Green Version]
- Bowley, N.B.; Hughes, J.M.B.; Steiner, R.E. The chest X-ray in pulmonary capillary haemorrhage: Correlation with carbon monoxide uptake. Clin. Radiol. 1979, 30, 413–417. [Google Scholar] [CrossRef]
- Park, J.O.; Choi, I.S.; Park, K.O. Normal Predicted Values of Single-Breath Diffusing Capacity of the Lung in Healthy Nonsmoking Adults. Korean J. Intern. Med. 1986, 1, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Bruce, E.N.; Bruce, M.C. A multicompartment model of carboxyhemoglobin and carboxymyoglobin responses to inhalation of carbon monoxide. J. Appl. Physiol. 2003, 95, 1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosselin, N.H.; Brunet, R.C.; Carrier, G. Determination of carboxyhaemoglobin in humans following low-level exposures to carbon monoxide. Inhal. Toxicol. 2009, 21, 1077–1091. [Google Scholar] [CrossRef] [PubMed]
- Özgür Dogan, N.; Corbacioglu, S.; Bildik, F.; Kilicaslan, I.; Gunaydın, G.; Günaydın, G.P.; Cevik, Y.; Ülker, V.; Hakoglu, O.; Gökcen, E. Determining the diagnostic value of endogenous carbon monoxide in Chronic Obstructive Pulmonary Disease exacerbations. J. Pak. Med. Assoc. 2014, 64, 1037–1041. [Google Scholar]
- Nambu, A.; Zach, J.; Schroeder, J.; Jin, G.Y.; Kim, S.S.; Kim, Y.-I.L.; Schnell, C.; Bowler, R.; Lynch, D.A. Relationships between diffusing capacity for carbon monoxide (DLCO), and quantitative computed tomography measurements and visual assessment for chronic obstructive pulmonary disease. Eur. J. Radiol. 2015, 84, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Sandek, K.; Bratel, T.; Lagerstrand, L. Effects on diffusing capacity and ventilation–perfusion relationships of budesonide inhalations for 2 months in chronic obstructive pulmonary disease (COPD). Respir. Med. 2001, 95, 676–684. [Google Scholar] [CrossRef] [Green Version]
- Murphy, T.F.; Sethi, S. Chronic Obstructive Pulmonary Disease. Drugs Aging 2002, 19, 761–775. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Laveneziana, P.; Webb, K.; Neder, J.A. Chronic Obstructive Pulmonary Disease: Clinical Integrative Physiology. Clin. Chest Med. 2014, 35, 51–69. [Google Scholar] [CrossRef]
- Crowley, T.J.; Andrews, A.E.; Cheney, J.; Zerbe, G.; Petty, T.L. Carbon monoxide assessment of smoking in chronic obstructive pulmonary disease. Addict. Behav. 1989, 14, 493–502. [Google Scholar] [CrossRef]
- Pugh, L.G.C.E. Blood volume changes in outdoor exercise of 8-10 hour duration. J. Physiol. 1969, 200, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Roughton, F.J.W.; Root, W.S. The fate of co in the body during recovery from mild carbon monoxide poisoning in man. Am. J. Physiol. Leg. Content 1945, 145, 239. [Google Scholar] [CrossRef] [PubMed]
- Prommer, N.; Schmidt, W. Loss of CO from the intravascular bed and its impact on the optimised CO-rebreathing method. Eur. J. Appl. Physiol. 2007, 100, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Bruce, E.N.; Bruce, M.C.; Erupaka, K. Prediction of the rate of uptake of carbon monoxide from blood by extravascular tissues. Respir. Physiol. Neurobiol. 2008, 161, 142–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, R.C.; Wang, Z.; Heo, M.; Ross, R.; Janssen, I.; Heymsfield, S.B. Total-body skeletal muscle mass: Development and cross-validation of anthropometric prediction models. Am. J. Clin. Nutr. 2000, 72, 796–803. [Google Scholar] [CrossRef]
- Möller, P.; Sylvén, C. Myoglobin in human skeletal muscle. Scand. J. Clin. Lab. Investig. 1981, 41, 479–482. [Google Scholar] [CrossRef]
- Woehlck, H.J.; Mei, D.; Dunning 3rd, M.B.; Ruiz, F. Mathematical Modeling of Carbon Monoxide Exposures from Anesthetic Breakdown Effect of Subject Size, Hematocrit, Fraction of Inspired Oxygen, and Quantity of Carbon Monoxide. Anesthesiology 2001, 94, 457–460. [Google Scholar] [CrossRef] [Green Version]
- Ozturan, I.U.; Yaka, E.; Suner, S.; Ozbek, A.E.; Alyesil, C.; Dogan, N.O.; Yilmaz, S.; Pekdemir, M. Determination of carboxyhemoglobin half-life in patients with carbon monoxide toxicity treated with high flow nasal cannula oxygen therapy. Clin. Toxicol. 2019, 57, 617–623. [Google Scholar] [CrossRef]
- Kim, Y.-M.; Shin, H.-J.; Choi, D.-w.; Kim, J.-M.; Lee, S.-W.; Jeong, S.-H.; Kim, H. Comparison of high-flow nasal cannula oxygen therapy and conventional reserve-bag oxygen therapy in carbon monoxide intoxication: A pilot study. Am. J. Emerg. Med. 2019. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Bal, U.; Sönmez, B.M.; Inan, S.; Iscanli, M.D.; Yilmaz, F. The efficiency of continuous positive airway Press. therapy in carbon monoxide poisoining in the emergency department. Eur. J. Emerg. Med. 2019. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Caglar, B.; Serin, S.; Yilmaz, G.; Torun, A.; Parlak, I. The Impact of Treatment with Continuous Positive Airway Pressure on Acute Carbon Monoxide Poisoning. Prehospital Disaster Med. 2019, 34, 588–591. [Google Scholar] [CrossRef]
- Buckley, N.A.; Juurlink, D.N.; Isbister, G.; Bennett, M.H.; Lavonas, E.J. Hyperbaric oxygen for carbon monoxide poisoning. Cochrane Database Syst. Rev. 2011, 4, CD002041. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.-T.; Shen, C.-H.; Lin, F.-G.; Chou, Y.-C.; Croxford, B.; Leonardi, G.; Huang, K.-L. Prognostic factors of carbon monoxide poisoning in Taiwan: A retrospective observational study. BMJ Open 2019, 9, e031135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernst, A.; Zibrak, J.D. Carbon monoxide poisoning. N. Engl. J. Med. 1998, 339, 1603–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, T.A.; Lawson, D.D.; Ledingham, I.M.; Norman, J.N.; Sharp, G.R.; Smith, G. Carbogen in Experimental Carbon-monoxide Poisoning. Br. Med. J. 1961, 2, 1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sein Anand, J.; Schetz, D.; Waldman, W.; Wiśniewski, M. Hyperventilation with Maintenance of Isocapnia. An Old New Method in Carbon Monoxide Intoxication. PLoS ONE 2017, 12, e0170621. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.A.; Iscoe, S.; Fedorko, L.; Duffin, J. Rapid elimination of CO through the lungs: Coming full circle 100 years on. Exp. Physiol. 2011, 96, 1262–1269. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Field | Factor | Results | Experiment | Control | Reference |
|---|---|---|---|---|---|
| Environment | CO concentration increase | CO uptake rate increase | Range: 0.01%–0.2% CO | Forbes et al. (1945) | |
| Range: 0–523 CO ppm | Peterson and Stewart (1970) | ||||
| Range: 8.7–1000 CO ppm | Peterson and Stewart (1975) | ||||
| Duration of exposure longer | CO uptake amount increase | Range: 0–270 min | Forbes et al. (1945) | ||
| Range: 15–480 min | Peterson and Stewart (1970) | ||||
| Range: 0–1440 min (50 CO ppm) | Benignus et al. (1994) | ||||
| O2 concentration increase | CO uptake rate decrease | Oxygen | Air | Forbes et al. (1945) | |
| Altitude increase | CO uptake rate increase | 16,000 ft; 40,000 ft | 0 ft | Forbes et al. (1945) | |
| Exercise increase | CO uptake rate increase | Hard work | Rest | Forbes et al. (1945) | |
| CO uptake rate increase | Light exercise; moderate exercise | Resting | Filley et al. (1954) | ||
| No difference | Moderate exercise | Low exercise | Tikuisis et al. (1992) | ||
| Physiology | Ventilation rate increase | CO uptake rate increase | Range: 6–30 L/min | Forbes et al. (1945) | |
| CO uptake rate increase | Range: 5.8–105 L/min | Filley et al. (1954) | |||
| Diffusion capacity of CO (DLCO) increase | CO uptake rate increase | 36.3 cm3/min/mmHg | 16.9 cm3/min/mmHg | Filley et al. (1954) | |
| CO uptake rate increase | Range: 5–30 mL/min/torr | Bruce and Bruce (2003) | |||
| CO uptake rate increase | - | - | Gosselin et al. (2009) | ||
| Blood volume increase | CO uptake rate increase | - | - | Coburn et al. (1965) | |
| Diffusion rate of CO flux from blood to muscle compartment in crease | CO uptake rate increase | Range: 0–100 mL/min/torr | Bruce et al. (2008) | ||
| Muscle mass | Less important | - | - | Bruce and Bruce (2006) | |
| Anaemia | CO uptake rate increase | Haematocrits of 18% and 30% | Haematocrits of 42% and 60% | Woehlck et al. (2001) | |
| Field | Factor | Results | Experiment | Control | Reference |
|---|---|---|---|---|---|
| Environment | CO concentration increase | CO half-life longer | 200.8 CO ppm for 60 min | 51.6 CO ppm for 60 min | Peterson and Stewart (1970) |
| Duration of exposure longer | CO half-life longer | 1250 CO ppm for 40 min | 10,000 CO ppm for 5 min | Bruce and Bruce (2006) | |
| (same CO dose in two groups) | |||||
| O2 concentration increase | CO half-life shorter | 100% oxygen | - | Weaver et al. (2000) | |
| 2.5 atm, 100% oxygen (HBO) | - | Pace et al. (1950) | |||
| Demography | Age increase | No difference | Range: 9–86 years old | Burney et al. (1982) | |
| >40 years old | <40 years old | Weaver et al. (2000) | |||
| CO half-life shorter | 4–12 years old | - | Klasner et al. (1998) | ||
| Sex | No difference | Female | Male | Burney et al. (1982) | |
| Female | Male | Weaver et al. (2000) | |||
| CO half-life shorter | Female | Male | Pace et al. (1950) | ||
| Female | Male; | Zavorsky et al. (2014) | |||
| Smoking | No difference | Smokers | Nonsmokers | Burney et al. (1982) | |
| Physiology | Ventilation rate increase | CO half-life shorter | Range: 4–10 L/min | Coburn et al. (1965) | |
| 15 and 30 L/min | 3 and 6 L/min | Selvakumar et al. (1993) | |||
| Range: 5–20 L/min | Kreck et al. (2001) | ||||
| Range: 4–40 L/min | Zavorsky et al. (2014) | ||||
| Chronic obstructive pulmonary disease (COPD) | No difference/CO half-life slightly longer | COPD patients | Normal subjects | Crowley et al. (1989) | |
| Blood volume increase | CO half-life shorter | - | - | Coburn et al. (1965) | |
| Range: 0.3–0.7 (Vb/VAwo) | Bruce and Bruce (2006) | ||||
| Haemoglobin mass increase | CO half-life longer | Male | Female | Zavorsky et al. (2014) | |
| Diffusion rate of CO flux from blood to muscle compartment increase | CO half-life shorter | Range: 0–2 mL/min/torr | Bruce et al. (2003) | ||
| Muscle mass | Less important | - | - | Bruce and Bruce (2006) | |
| Anaemia | CO half-life shorter | Anaemia | Polycythaemia | Zavorsky et al. (2014) | |
| Treatment | 100% oxygen | CO half-life shorter | 100% oxygen | - | Weaver et al. (2000) |
| High-flow nasal cannula (HFNC) | No difference | 100% oxygenwith high flow | 100% oxygen | Kim et al. (2019) | |
| Continuous positive airway pressure (CPAP) | CO half-life shorter | 100% oxygenwith positive pressure | 100% oxygen | Bal et al. (2019)Caglar et al. (2019) | |
| Hyperbaric oxygen (HBO) therapy | CO half-life shorter | 2.5 atm, 100% oxygen | - | Pace et al. (1950) | |
| 3 atmosphere absolute (ATA), 100% oxygen | 1 ATA, 100% oxygen | Peterson and Stewart (1970) | |||
| Carbogen | CO half-life shorter | Hyperventilation(6% CO2 in O2) | Without isocapnia | Sein Anand et al. (2017) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, K.-T.; Leonardi, G.S.; Croxford, B. Factors Contributing to CO Uptake and Elimination in the Body: A Critical Review. Int. J. Environ. Res. Public Health 2020, 17, 528. https://doi.org/10.3390/ijerph17020528
Pan K-T, Leonardi GS, Croxford B. Factors Contributing to CO Uptake and Elimination in the Body: A Critical Review. International Journal of Environmental Research and Public Health. 2020; 17(2):528. https://doi.org/10.3390/ijerph17020528
Chicago/Turabian StylePan, Ke-Ting, Giovanni S. Leonardi, and Ben Croxford. 2020. "Factors Contributing to CO Uptake and Elimination in the Body: A Critical Review" International Journal of Environmental Research and Public Health 17, no. 2: 528. https://doi.org/10.3390/ijerph17020528
APA StylePan, K. -T., Leonardi, G. S., & Croxford, B. (2020). Factors Contributing to CO Uptake and Elimination in the Body: A Critical Review. International Journal of Environmental Research and Public Health, 17(2), 528. https://doi.org/10.3390/ijerph17020528