Use of Economic Evidence When Prioritising Public Health Interventions in Schools: A Qualitative Study with School Staff


{kind=link}
Abstract
:1. Introduction
2. Methods
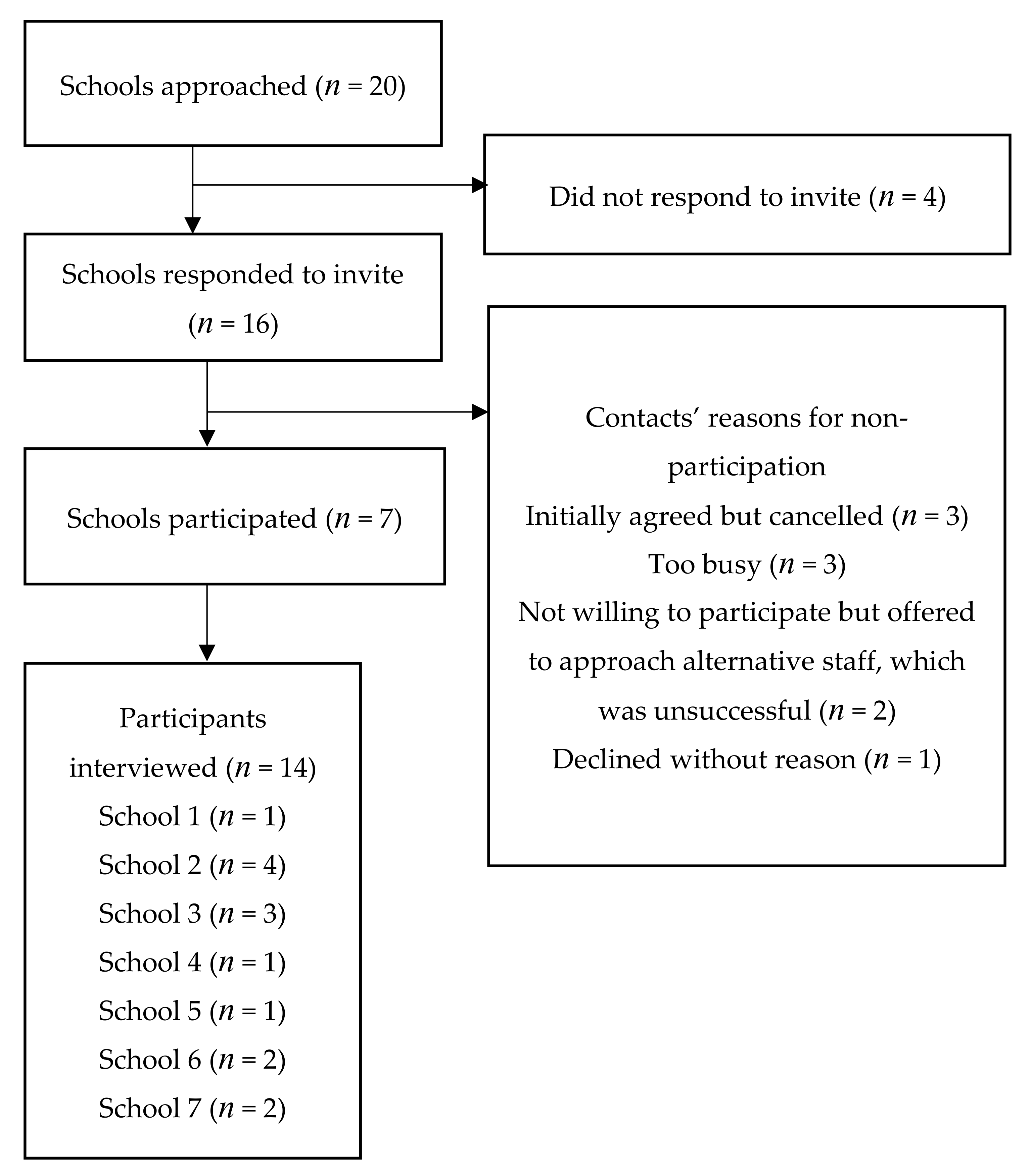
2.1. Sample and Recruitment
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Decision Making Process and Objectives
Schools do tend to get offered an awful lot of things to do, but it’s having someone to implement it, oversee it, get it started, get it finished so we can’t say ‘yes’ to everything, much as we’d like to [ID6, Pastoral role].
Well, I’m the head teacher, so normally if there’s an initiative or anything like that and if I’m enthusiastic about it, it normally gets done [ID12, Leader].
I’d quite like to go to governors and show them you know that this is what we’re investing in, this is part of our curriculum and this is the impact it’s had [ID9, Leader].
I think, personally, it depends on the type of leaders you’ve got in school. It depends on people’s own personal passion. I mean in every school you go in, there probably is somebody who’s into sport and I think if they’re really keen and they go up to the Senior Leaders; have a talk to them about it; show them research about the positives of it, and then I think that’s how you can drive it [ID7, Leader/teacher].
Schools’ priority has to be what we’re measured on, as it is in all sort of walks of life; be it, hospitals; be it doctors’ surgeries; be it the police. We’ve now all got targets that we’re working towards. If you ask us to go and dedicate a certain amount of time to something that is not directly going to impact on those targets, it’s always going to be hard [ID11, Safeguarding role].
If you’ve got two hours of non-stop, you know, Maths and English, you’re going to have that kind of level of concentration that will just dip. I mean nobody can concentrate for that length of time. By having a bit of a burst of exercise actually supports that and helps [ID12, Leader].
Obviously I have to decide whether I feel that the intervention is going to be of any benefit to the children, mainly academically because I think that’s our reason to be here but equally for the wellbeing as well and I think the two go hand in hand [ID12, Leader].
Obviously academic levels, we’re in a vulnerable school and anything towards that is important…. At the end of the day, they can be as bright as anything but if they can’t get off their sofa because they’re too big then they’ve got real issues [ID9, Leader].
The way our ethos is, it’s about getting the children healthy, out of this cycle of unhealthiness and obesity which, looking at some of the children already, it’s a major concern what they’re going to be like in four or five years’ time [ID9, Leader].
We do feel we’re fighting the tide against social media, and the more we can get our children physically active, the better… We’re becoming a nation of children who live indoors rather than playing outside [ID11, Safeguarding role].
As a school, I’d prioritise as much as we could affect…. Obviously, we can’t control all the things that happen outside school. We need to educate them about that and I think that education is what we’re here for and I think we do do that….If you’re doing something regularly—something like The Daily Mile will have a direct impact much more effectively than preaching about what they might eat because I don’t think children have control of that very often [ID12, Leader].
We have done brain breaks and checking in and seeing how everybody is at different points in the day but there isn’t, a government initiative to follow so we’ve just made our own from others’ [ID14, Teacher].
3.2. Evidence
You get the data for obesity and the BMI data. We’re really low, we’re one of the worst schools in Birmingham [ID10, Leader/teacher].
I am very conscious of the obesity levels within our children, not just at our school, nationally and wanted to be involved in something to try and change and influence that [ID11, Safeguarding role].
This needs promotion because I think lots of schools would be willing to do it if they had the knowledge that it was actually going to be beneficial [ID12, Leader].
So we trial it for six weeks and then we look at the end of the six weeks. Has it made the impact? Has it not? If it hasn’t, then we’ll look at different ways to adjust it and change it so it does [ID7, Leader/teacher].
I think you’ve got to bring in some enjoyment levels of children because to lead an active lifestyle or healthy lifestyle they’ve got to enjoy some form of exercise. If they don’t enjoy it they’re not going to do it when they’re older [ID1, Teacher].
I think the economic one is the most difficult one. I think the wellbeing one would make sense to people [ID2, Leader].
I think if there were proven benefits I don’t think it would matter so much that there was a cost to it because as a school we’re trying things that will improve wellbeing, mental health and, physical health [ID14, Teacher].
I think it might have taken some academic time away but actually, the benefits to those academic studies are probably bigger than the time that they’ve lost [ID12, Leader].
I think you’d have to really prove its effectiveness and the impact of it because it’s public funds and it’s like anything we do; we, we have to measure impact, and I know this is a time thing, so I suppose, it is a cost [ID2, Leader].
So, for example, if we were trying to reduce BMI, and we wanted to pay for somebody to come in and do a sporting activity over a period of time, we would want to see a measurable decrease [ID10, Leader/teacher].
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Story, M.; Nanney, M.S.; Schwartz, M.B. Schools and Obesity Prevention: Creating School Environments and Policies to Promote Healthy Eating and Physical Activity. Milbank Q. 2009, 87, 71–100. [Google Scholar] [CrossRef]
- Littlecott, H.J.; Long, S.; Hawkins, J.; Murphy, S.; Hewitt, G.; Eccles, G.; Fletcher, A.; Moore, G.F. Health Improvement and Educational Attainment in Secondary Schools: Complementary or Competing Priorities? Exploratory Analyses from the School Health Research Network in Wales. Health Educ. Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norris, E.; van Steen, T.; Direito, A.; Stamatakis, E. Physically active lessons in schools and their impact on physical activity, educational, health and cognition outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department for Education. Healthy Schools Rating Scheme; Department for Education: London, UK, 2019. [Google Scholar]
- Department for Education. School Food in England; Department for Education: London, UK, 2019. [Google Scholar]
- Department for Education. Relationships Education, Relationships and Sex Education (RSE) and Health Education; Department for Education: London, UK, 2020. [Google Scholar]
- CDC. CDC Healthy Schools. Available online: https://www.cdc.gov/healthyschools/wscc/index.htm (accessed on 23 September 2020).
- Ruggieri, D.G.; Bass, S.B. A Comprehensive Review of School-Based Body Mass Index Screening Programs and Their Implications for School Health: Do the Controversies Accurately Reflect the Research? J. Sch. Health 2014, 85, 61–72. [Google Scholar] [CrossRef]
- Public Health England. National Child Measurement Programme; Public Health England: London, UK, 2013. [Google Scholar]
- Nathan, N.; Wolfenden, L.; Williams, C.M.; Yoong, S.L.; Lecathelinais, C.; Bell, A.C.; Wyse, R.; Sutherland, R.; Wiggers, J. Adoption of obesity prevention policies and practices by Australian primary schools: 2006 to 2013. Health Educ. Res. 2015, 30, 262–271. [Google Scholar] [CrossRef] [Green Version]
- The Daily Mile Foundation. The Daily Mile. Available online: https://thedailymile.co.uk/about/ (accessed on 9 May 2018).
- The Daily Mile Foundation. The Daily Mile. Available online: https://thedailymile.co.uk/ (accessed on 23 September 2020).
- Jessiman, P.E.; Campbell, R.; Jago, R.; Van Sluijs, E.M.F.; Newbury-Birch, D. A qualitative study of health promotion in academy schools in England. BMC Public Health 2019, 19, 1186. [Google Scholar] [CrossRef]
- Arnold, J.; Bruce-Low, S.; Henderson, S.; Davies, J. Mapping and evaluation of physical activity interventions for school-aged children. Public Health 2016, 136, 75–79. [Google Scholar] [CrossRef]
- Cox, L.; Berends, V.; Sallis, J.F.; St John, J.M.; McNeil, B.; Gonzalez, M.; Agron, P. Engaging school governance leaders to influence physical activity policies. J. Phys. Act. Health 2011, 8 (Suppl. 1), S40–S48. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.T.; Charles, J.M.; Lloyd-Williams, H. Public health economics: A systematic review of guidance for the economic evaluation of public health interventions and discussion of key methodological issues. BMC Public Health 2013, 13, 1001. [Google Scholar] [CrossRef] [Green Version]
- Weatherly, H.; Drummond, M.; Claxton, K.; Cookson, R.; Ferguson, B.; Godfrey, C.; Rice, N.; Sculpher, M.; Sowden, A. Methods for assessing the cost-effectiveness of public health interventions: Key challenges and recommendations. Health Policy 2009, 93, 85–92. [Google Scholar] [CrossRef] [PubMed]
- NICE. Developing NICE Guidelines: The Manual; NICE: London, UK, 2014. [Google Scholar]
- Zanganeh, M.; Adab, P.; Li, B.; Frew, E. A Systematic Review of Methods, Study Quality, and Results of Economic Evaluation for Childhood and Adolescent Obesity Intervention. Int. J. Env. Res. Public Health 2019, 16, 485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breheny, K.; Adab, P.; Passmore, S.; Martin, J.; Lancashire, E.; Hemming, K.; Frew, E. A cluster randomised controlled trial evaluating the effectiveness and cost-effectiveness of the daily mile on childhood obesity and wellbeing; the Birmingham daily mile protocol. BMC Public Health 2018, 18, 126. [Google Scholar] [CrossRef] [PubMed]
- Breheny, K.; Passmore, S.; Adab, P.; Martin, J.; Hemming, K.; Lancashire, E.R.; Frew, E. Effectiveness and cost-effectiveness of The Daily Mile on childhood weight outcomes and wellbeing: A cluster randomised controlled trial. Int. J. Obes. 2020, 44, 812–822. [Google Scholar] [CrossRef] [Green Version]
- Schonert-Reichl, K.A.; Guhn, M.; Gadermann, A.M.; Hymel, S.; Sweiss, L.; Hertzman, C. Development and validation of the Middle Years Development Instrument (MDI): Assessing children’s well-being and assets across multiple contexts. Soc. Indic. Res. 2013, 114, 345–369. [Google Scholar] [CrossRef] [Green Version]
- Stevens, K.J. Working with children to develop dimensions for a preference-based, generic, pediatric, health-related quality-of-life measure. Qual. Health Res. 2010, 20, 340–351. [Google Scholar] [CrossRef]
- Jupp, V. The Sage Dictionary of Social Research Methods; Sage: London, UK, 2006. [Google Scholar]
- Sandelowski, M. Sample size in qualitative research. Res. Nurs. Health 1995, 18, 179–183. [Google Scholar] [CrossRef]
- QSR International. NVivo 12; QSR International: Doncaster, Australia, 2018. [Google Scholar]
- Coast, J.; Jackson, L. Chapter 5—Understanding Primary Data Analysis. In Qualitative Methods for Health Economics; Coast, J., Ed.; Rowman & Littlefield International Ltd.: London, UK, 2017. [Google Scholar]
- Oosterhoff, M.; Bosma, H.; van Schayck, O.C.; Evers, S.M.; Dirksen, C.D.; Joore, M.A. A systematic review on economic evaluations of school-based lifestyle interventions targeting weight-related behaviours among 4–12 year olds: Issues and ways forward. Prev. Med. 2018, 114, 115–122. [Google Scholar] [CrossRef]
- Williams, I.; Bryan, S. Understanding the limited impact of economic evaluation in health care resource allocation: A conceptual framework. Health Policy 2007, 80, 135–143. [Google Scholar] [CrossRef]
- Andronis, L.; Maredza, M.; Petrou, S. Measuring, valuing and including forgone childhood education and leisure time costs in economic evaluation: Methods, challenges and the way forward. Soc. Sci. Med. 2019, 237, 112475. [Google Scholar] [CrossRef]
- Melbourne Children’s. Comprehensive Monitoring Across Childhood and Early Adolescence: An Implementation Evaluation. Available online: https://www.melbournechildrens.com/atp/translation/comprehensive-monitoring-project/ (accessed on 25 September 2020).
- UBC. MDI Canada. Available online: http://earlylearning.ubc.ca/mdi/national-scale-out/ (accessed on 25 September 2020).
- Ogilvie, D.; Adams, J.; Bauman, A.; Gregg, E.W.; Panter, J.; Siegel, K.R.; Wareham, N.J.; White, M. Using natural experimental studies to guide public health action: Turning the evidence-based medicine paradigm on its head. J. Epidemiol. Community Health 2020, 74, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breheny, K.; Frew, E.; Williams, I.; Passmore, S.; Coast, J. Use of Economic Evidence When Prioritising Public Health Interventions in Schools: A Qualitative Study with School Staff. Int. J. Environ. Res. Public Health 2020, 17, 9077. https://doi.org/10.3390/ijerph17239077
Breheny K, Frew E, Williams I, Passmore S, Coast J. Use of Economic Evidence When Prioritising Public Health Interventions in Schools: A Qualitative Study with School Staff. International Journal of Environmental Research and Public Health. 2020; 17(23):9077. https://doi.org/10.3390/ijerph17239077
Chicago/Turabian StyleBreheny, Katie, Emma Frew, Iestyn Williams, Sandra Passmore, and Joanna Coast. 2020. "Use of Economic Evidence When Prioritising Public Health Interventions in Schools: A Qualitative Study with School Staff" International Journal of Environmental Research and Public Health 17, no. 23: 9077. https://doi.org/10.3390/ijerph17239077
APA StyleBreheny, K., Frew, E., Williams, I., Passmore, S., & Coast, J. (2020). Use of Economic Evidence When Prioritising Public Health Interventions in Schools: A Qualitative Study with School Staff. International Journal of Environmental Research and Public Health, 17(23), 9077. https://doi.org/10.3390/ijerph17239077