Radiographic Assessment of Pediatric Condylar Fractures after Conservative Treatment with Functional Appliances—A Systematic Review

 ,
, 
 ,
, 
Abstract
:1. Introduction
- -
- reducing muscle activity of the anterior temporals muscle in the short-term (≤3 months) [9], and balancing the muscle activity on both sides [10]. Even if scientific evidence is missing, it has been hypothesized that occlusal splints act as an adjunct to relieve pain and tenderness of the masticatory muscles [11,12]. This may be due to the fact that orthopedic appliances induce elongation of the masseter muscles (“muscular stretching”) [13], as well as a transitory reduction of jaw-closing muscle activity (“muscular relaxation”) [14,15].
- -
- improving function: in combination with joint mobilization exercises, orthopedic appliances avoid any restriction of mandibular movements due to postoperative pain, muscle protective co-contraction, surgical scars, and adherences [16]; based on the theory of craniofacial growth proposed by Moss et al., a “scar-free technique” can preserve the integrity of the functional matrix, so that the genetic guidance will direct the soft tissue envelope of the temporomandibular joint to rebuild the condylar process [17].
- -
- avoiding occlusal instability due to inadequate mandibular vertical growth of the mandible, e.g., compensatory teeth overeruption on the “healthy” side [18].
2. Materials and Methods
2.1. Search Strategy
- -
- population: (((((((((Mandibular Fractures * (All Fields)) OR Craniocerebral trauma * (All Fields)) OR Jaw diseases * (All Fields)) OR Jaw * (All Fields)) OR Dental Occlusion, Traumatic * (All Fields)))
- -
- intervention: (((((((((Jaw Fixation Techniques * (All Fields)) OR Diet * (All Fields)) OR diet therapy * (All Fields)) OR Pharmacologic Actions * (All Fields)) OR Occlusal Splints * (All Fields)) OR Orthodontics * (All Fields)) OR Dental Health Services * (All Fields)) OR Myofunctional Therapy* [All Fields]) OR Conservative treatment * (All Fields)))
- -
- comparison: (((child * (All Fields)) OR Adult Children * (All Fields)) OR adolescent * (All Fields)))
- -
- outcome: (((((((((((((Facial Asymmetry * (All Fields)) OR Fracture Healing * (All Fields)) OR Temporomandibular ankylosis * (All Fields)) OR Temporomandibular Joint Disorders * (All Fields)) OR (Growth and development * (All Fields))) OR Dental Occlusion * (All Fields)) OR Jaw Relation Record * (All Fields)) OR Mouth Rehabilitation * (All Fields)) OR Pain Measurement * (All Fields)) OR Quality of Life * (All Fields)) OR treatment outcomes * (All Fields)) OR evaluation * (All Fields)) OR Malocclusion * (All Fields)))
- -
- studies: ((((Observational Study (Publication Type)) OR Clinical Trial (Publication Type)) OR epidemiologic studies) OR Case Reports (Publication Type))
2.2. Study Selection
- -
- Age: 5–16 years;
- -
- Type of fracture: unilateral or bilateral condylar fracture;
- -
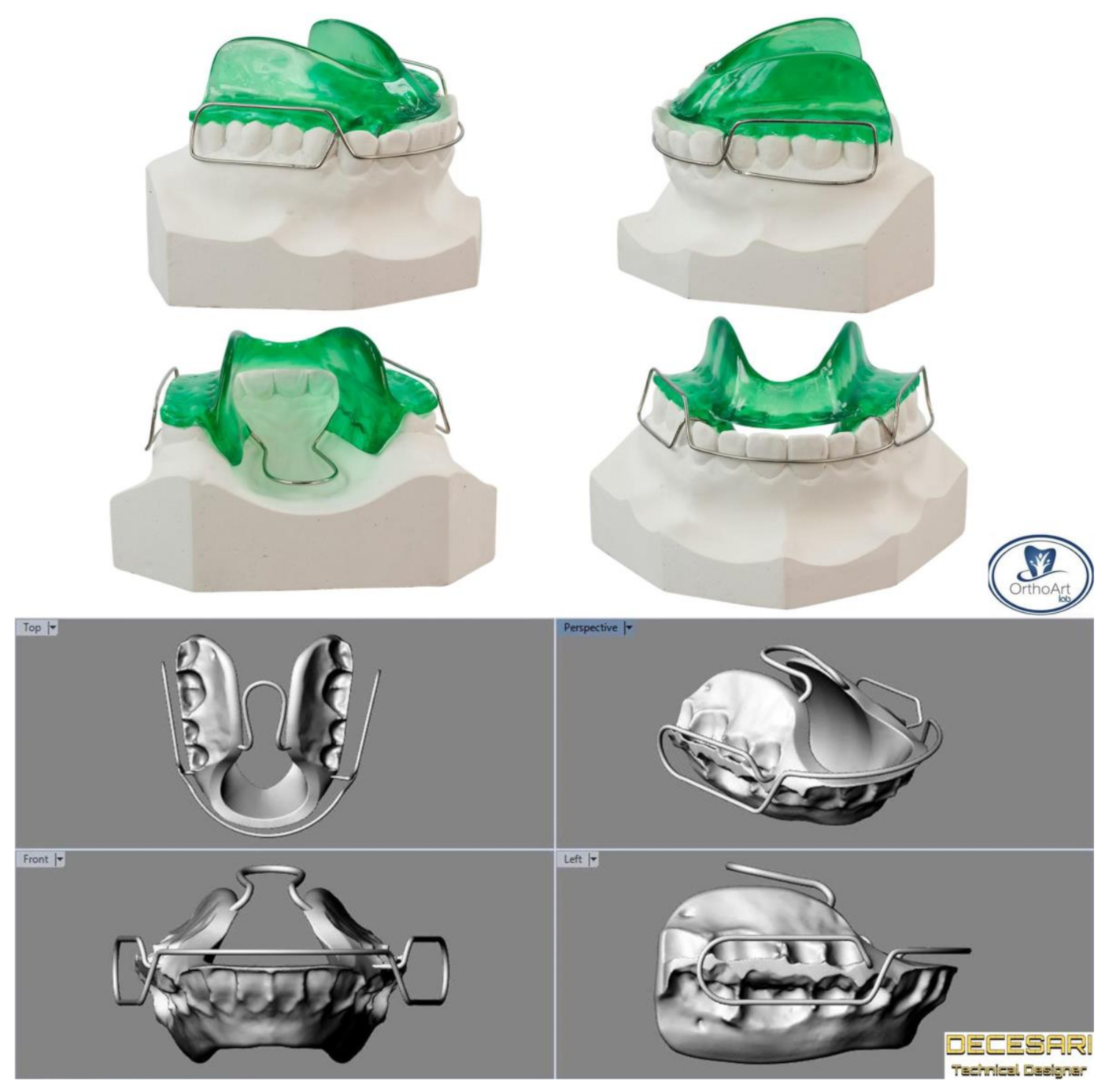
- Type of treatment: conservative treatment with functional appliances;
- -
- Follow-up: > six months;
- -
- Type of studies: prospective and retrospective human studies (in at least 10 patients), English language, with abstract available;
- -
- Clinical/radiographical assessment: temporomandibular joint (TMJ) examination before and after treatment;
- -
- History: absence of any systemic disease affecting bone and growth.
2.3. Data Extraction
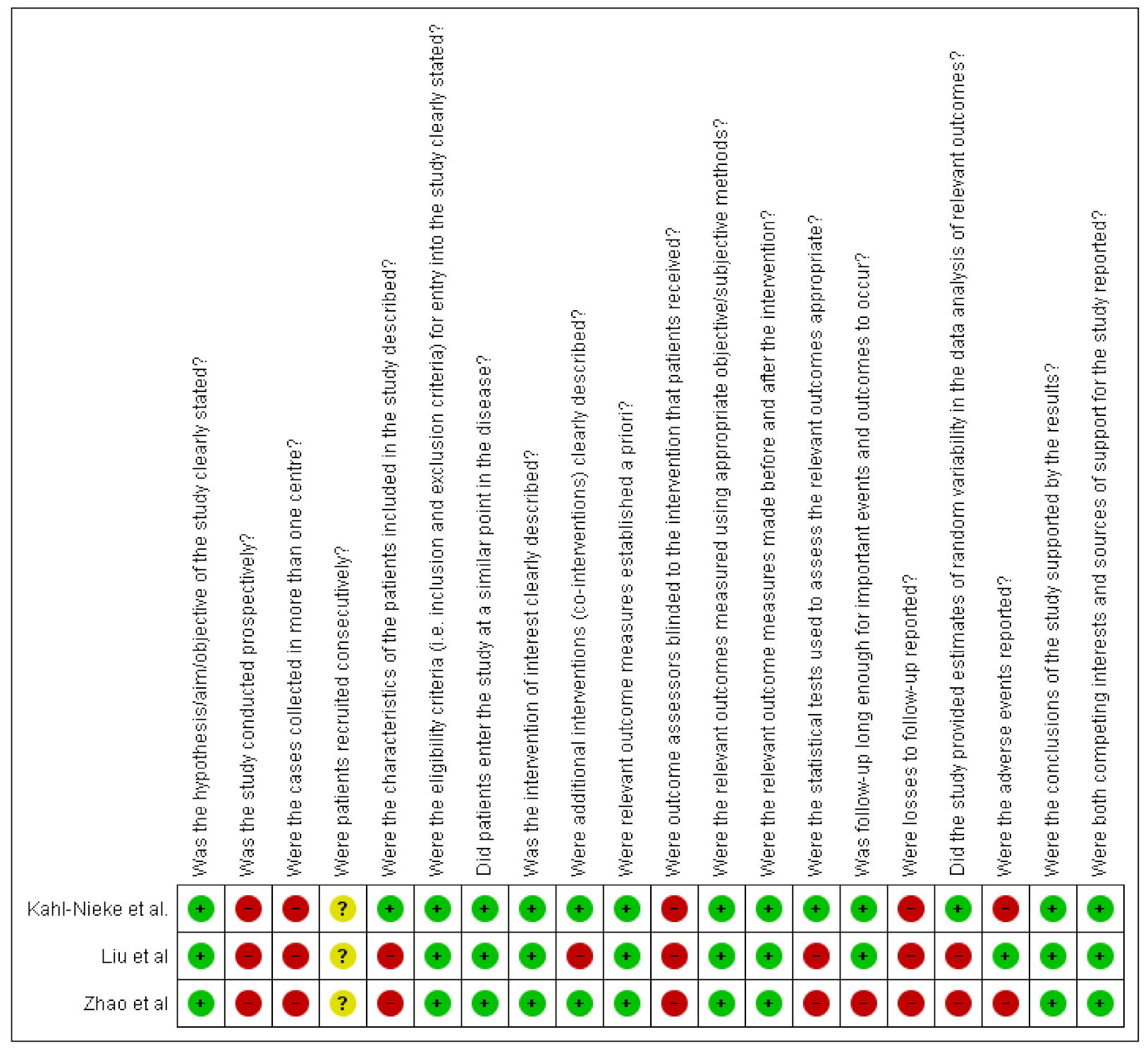
2.4. Quality Assessment
3. Results
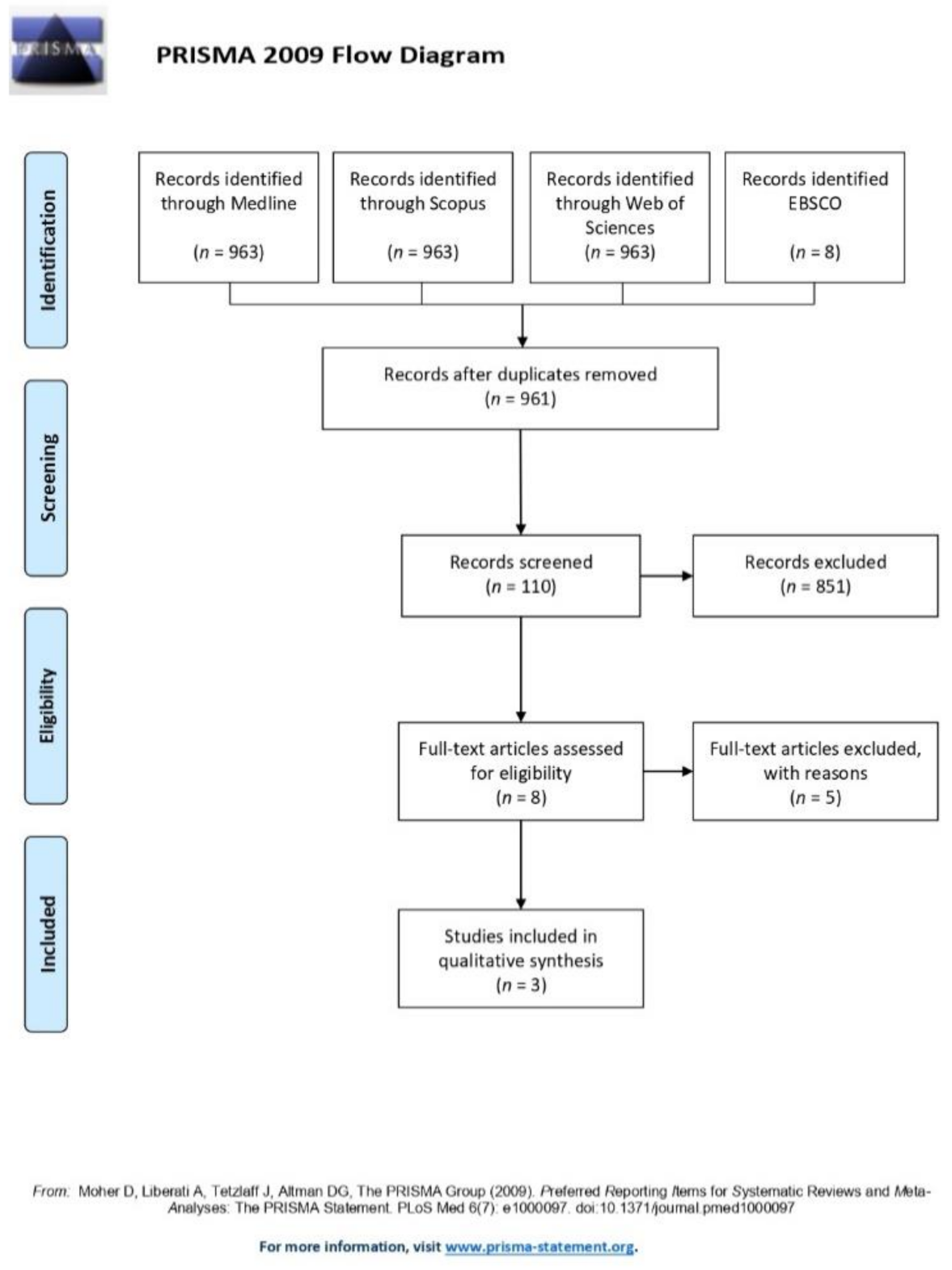
3.1. Search Results
- -
- Population: about 21% of the retrieved papers (21 articles) were excluded because of the wrong age group and fracture type (studies on adults, and/or fractures of the mandibular angle or symphysis/body;
- -
- Intervention: about 27% of the retrieved papers (27 articles) were excluded because the surgical intervention did not meet the inclusion criteria;
- -
- Comparison: about 19% of the retrieved papers (19 articles) were excluded because they compared different plates’ and screws’ designs for rigid internal fixation of the mandible;
- -
- Outcome: about 16% of the retrieved papers (16 articles) were excluded because they assessed only functional outcomes after conservative treatment of mandibular fractures;
- -
- Study: about 11% of the retrieved papers (11 articles) were excluded because they were narrative or systematic reviews;
- -
- Other reasons: about 8% of the retrieved papers (eight articles) were excluded because the full text was not available.
3.2. Descriptive Analysis
3.3. Quality Assessment
4. Discussion
- -
- partial or full recovery of the joint morphology produce good to excellent functional results; Zhao et al. reported that, at one year of follow-up, all the patients (27 with unilateral, 13 with bilateral fractures) showed good to excellent clinical and functional recovery (maximum mouth opening >35 mm, lateral deviation during mouth opening <3 mm, absence of articular noise and pain, no instance of joint ankylosis, malocclusion, and facial asymmetry) [29]. Only 7% of patients with unilateral condylar fractures showed lateral deviation during mouth opening, while 8% of those with bilateral condylar fractures developed TMJ clicking. Similar results were found by Liu et al. [30]—out of 30 patients, everyone revealed good (n = 5) to excellent (n = 25) functional outcomes according to the Helkimo index [35,36].
- -
- ramal height discrepancies may be compensated by adaptive changes, even in severe condylar displacements. Rutges et al. reported that four patients out of 28 reported a difference of more than 10 mm; in that sample, two subjects had mild, and two had moderate occlusal clinical dysfunctions [37].
- -
- there is an absence of data collected before the injuries occurred. Rutges et al. found that the average difference of 3.4 mm of ramal height at 3.0 years’ follow-up was not significantly different from the control group, which showed a mean discrepancy of 3.0 mm between the two sides [37].
4.1. Limitations
4.2. Implications for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Imahara, S.D.; Hopper, R.A.; Wang, J.; Rivara, F.P.; Klein, M.B. Patterns and outcomes of pediatric facial fractures in the United States: A survey of the National Trauma Data Bank. J. Am. Coll. Surg. 2008, 207, 710–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iida, S.; Matsuya, T. Paediatric maxillofacial fractures: Their aetiological characters and fracture patterns. J. Craniomaxillofac. Surg. 2002, 30, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Moss, M.L. The functional matrix hypothesis revisited. 1. The role of mechanotransduction. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 8–11. [Google Scholar] [CrossRef]
- Reddy, N.V.; Reddy, P.B.; Rajan, R.; Ganti, S.; Jhawar, D.K.; Potturi, A. Analysis of patterns and treatment strategies for mandibular condyle fractures: Review of 175 condyle fractures with review of literature. J. Maxillofac. Oral Surg. 2013, 12, 315–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assael, L.A. Open versus closed reduction of adult mandibular condyle fractures: An alternative interpretation of the evidence. J. Oral Maxillofac. Surg. 2003, 61, 1333–1339. [Google Scholar] [CrossRef]
- Choi, K.Y.; Yang, J.D.; Chung, H.Y.; Cho, B.C. Current Concepts in the Mandibular Condyle Fracture Management Part II: Open Reduction Versus Closed Reduction. Arch. Plast. Surg. 2012, 39, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Phelps-Sandall, B.A.; Oxford, S.J. Effectiveness of oral hygiene techniques on plaque and gingivitis in patients placed in intermaxillary fixation. Oral Surg. Oral Med. Oral Pathol. 1983, 56, 487–490. [Google Scholar] [CrossRef]
- Tavares, C.A.; Allgayer, S. Conservative orthodontic treatment for a patient with a unilateral condylar fracture. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 75–84. [Google Scholar] [CrossRef]
- Lobbezoo, F.; van der Glas, H.W.; van Kampen, F.M.; Bosman, F. The effect of an occlusal stabilization splint and the mode of visual feedback on the activity balance between jaw-elevator muscles during isometric contraction. J. Dent. Res. 1993, 72, 876–882. [Google Scholar] [CrossRef]
- Naeije, M.; Hansson, T.L. Short-term effect of the stabilization appliance on masticatory muscle activity in myogenous craniomandibular disorder patients. J. Craniomandib. Disord. 1991, 5, 245–250. [Google Scholar]
- Kuzmanovic Pficer, J.; Dodic, S.; Lazic, V.; Trajkovic, G.; Milic, N.; Milicic, B. Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Michelotti, A.; Cioffi, I.; Rongo, R.; Borrelli, R.; Chiodini, P.; Svensson, P. Effects of Muscle Pain Induced by Glutamate Injections During Sustained Clenching on the Contraction Pattern of Masticatory Muscles. J. Oral Facial Pain Headache 2014, 28, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Manns, A.; Miralles, R.; Palazzi, C. EMG, bite force, and elongation of the masseter muscle under isometric voluntary contractions and variations of vertical dimension. J. Prosthet. Dent. 1979, 42, 674–682. [Google Scholar] [CrossRef]
- Bresin, A.; Bagge, U.; Kiliaridis, S. Adaptation of normal and hypofunctional masseter muscle after bite-raising in growing rats. Eur. J. Oral Sci. 2000, 108, 493–503. [Google Scholar] [CrossRef]
- Grunheid, T.; Langenbach, G.E.; Korfage, J.A.; Zentner, A.; van Eijden, T.M. The adaptive response of jaw muscles to varying functional demands. Eur. J. Orthod. 2009, 31, 596–612. [Google Scholar] [CrossRef] [Green Version]
- Jensen, T.; Jensen, J.; Norholt, S.E.; Dahl, M.; Lenk-Hansen, L.; Svensson, P. Open reduction and rigid internal fixation of mandibular condylar fractures by an intraoral approach: A long-term follow-up study of 15 patients. J. Oral Maxil. Surg. 2006, 64, 1771–1779. [Google Scholar] [CrossRef]
- Moss, M.L. The differential roles of periosteal and capsular functional matrices in orofacial growth. Eur. J. Orthod. 2007, 29, i96–i101. [Google Scholar] [CrossRef] [Green Version]
- Melsen, B.; Bjerregaard, J.; Bundgaard, M. The effect of treatment with functional appliance on a pathologic growth pattern of the condyle. Am. J. Orthod. Dentofac. Orthop. 1986, 90, 503–512. [Google Scholar] [CrossRef]
- Staderini, E.; Guglielmi, F.; Cornelis, M.A.; Cattaneo, P.M. Three-dimensional prediction of roots position through cone-beam computed tomography scans-digital model superimposition: A novel method. Orthod. Craniofacial Res. 2018. [Google Scholar] [CrossRef] [Green Version]
- Kahl-Nieke, B.; Fischbach, R.; Gerlach, K.L. CT analysis of temporomandibular joint state in children 5 years after functional treatment of condylar fractures. Int. J. Oral Maxillofac. Surg. 1994, 23, 332–337. [Google Scholar] [CrossRef]
- Staderini, E.; De Luca, M.; Candida, E.; Rizzo, M.I.; Rajabtork Zadeh, O.; Bucci, D.; Zama, M.; Lajolo, C.; Cordaro, M.; Gallenzi, P. Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina 2019, 55, 576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staderini, E.; Patini, R.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Three-Dimensional Assessment of Morphological Changes Following Nasoalveolar Molding Therapy in Cleft Lip and Palate Patients: A Case Report. Dent. J. 2019, 7, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marradi, F.; Staderini, E.; Zimbalatti, M.A.; Rossi, A.; Grippaudo, C.; Gallenzi, P. How to Obtain an Orthodontic Virtual Patient through Superimposition of Three-Dimensional Data: A Systematic Review. Appl. Sci. 2020, 10, 5354. [Google Scholar] [CrossRef]
- Saponaro, G.; Doneddu, P.; Gasparini, G.; Staderini, E.; Boniello, R.; Todaro, M.; D’Amato, G.; Pelo, S.; Moro, A. Custom made onlay implants in peek in maxillofacial surgery: A volumetric study. Childs Nerv. Syst. 2019. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [Green Version]
- Hausner, E.; Guddat, C.; Hermanns, T.; Lampert, U.; Waffenschmidt, S. Prospective comparison of search strategies for systematic reviews: An objective approach yielded higher sensitivity than a conceptual one. J. Clin. Epidemiol. 2016, 77, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kahl-Nieke, B.; Fischbach, R. Condylar restoration after early TMJ fractures and functional appliance therapy. Part I: Remodelling. J. Orofac. Orthop. 1998, 59, 150–162. [Google Scholar] [CrossRef]
- Liu, C.K.; Meng, F.W.; Tan, X.Y.; Xu, J.; Liu, H.W.; Liu, S.X.; Huang, H.T.; Yan, R.Z.; Hu, M.; Hu, K.J. Clinical and radiological outcomes after treatment of sagittal fracture of mandibular condyle (SFMC) by using occlusal splint in children. Br. J. Oral Maxillofac. Surg. 2014, 52, 144–148. [Google Scholar] [CrossRef]
- Zhao, Y.M.; Yang, J.; Bai, R.C.; Ge, L.H.; Zhang, Y. A retrospective study of using removable occlusal splint in the treatment of condylar fracture in children. J. Craniomaxillofac. Surg. 2014, 42, 1078–1082. [Google Scholar] [CrossRef]
- Alyahya, A.; Bin Ahmed, A.; Nusair, Y.; Ababtain, R.; Alhussain, A.; Alshafei, A. Mandibular condylar fracture: A systematic review of systematic reviews and a proposed algorithm for management. Br. J. Oral Maxillofac. Surg. 2020, 58, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Zide, M.F.; Kent, J.N. Indications for open reduction of mandibular condyle fractures. J. Oral Maxillofac. Surg. 1983, 41, 89–98. [Google Scholar] [CrossRef]
- Hjorth, T.; Melsen, B.; Moller, E. Masticatory muscle function after unilateral condylar fractures: A prospective and quantitative electromyographic study. Eur. J. Oral Sci. 1997, 105, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Hollender, L.; Lindahl, L. Radiographic Study of Articular Remodeling in Temporomandibular-Joint after Condylar Fractures. Scand. J. Dent. Res. 1974, 82, 462–465. [Google Scholar] [CrossRef]
- Hovinga, J.; Boering, G.; Stegenga, B. Long-term results of nonsurgical management of condylar fractures in children. Int. J. Oral Maxillofac. Surg. 1999, 28, 429–440. [Google Scholar] [CrossRef]
- Choi, K.Y.; Yang, J.D.; Chung, H.Y.; Cho, B.C. Current concepts in the mandibular condyle fracture management part I: Overview of condylar fracture. Arch. Plast. Surg. 2012, 39, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Helkimo, M. Studies on function and dysfunction of the masticatory system. II. Index for anamnestic and clinical dysfunction and occlusal state. Sven. Tandlak. Tidskr. Swed. Dent. J. 1974, 67, 101–121. [Google Scholar]
- Rutges, J.P.; Kruizinga, E.H.; Rosenberg, A.; Koole, R. Functional results after conservative treatment of fractures of the mandibular condyle. Br. J. Oral Maxillofac. Surg. 2007, 45, 30–34. [Google Scholar] [CrossRef]
- Cucurullo, R.; Giannuzzi, I.; Clivio, A.; Biagi, R. Management of unilateral condylar fracture in a 9.6-year-old female. Eur. J. Paediatr. Dent. 2009, 10, 95–101. [Google Scholar]
- Lindahl, L. Condylar fractures of the mandible. I. Classification and relation to age, occlusion, and concomitant injuries of teeth and teeth-supporting structures, and fractures of the mandibular body. Int. J. Oral Surg. 1977, 6, 12–21. [Google Scholar] [CrossRef]
- Lindahl, L.; Hollender, L. Condylar fractures of the mandible. II. a radiographic study of remodeling processes in the temporomandibular joint. Int. J. Oral Surg. 1977, 6, 153–165. [Google Scholar] [CrossRef]
- Reynders, R.A.M.; Ronchi, L.; Ladu, L.; van Etten-Jamaludin, F.; Bipat, S. Insertion torque and success of orthodontic mini-implants: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 596–614. [Google Scholar] [CrossRef] [PubMed]
- Patini, R.; Staderini, E.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Case Reports in Pediatric Dentistry Journals: A Systematic Review about Their Effect on Impact Factor and Future Investigations. Dent. J. 2019, 7, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Huni, A.; Salazar, F.B.C.; Sharma, P.K.; Fleming, P.S. Understanding factors influencing compliance with removable functional appliances: A qualitative study. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 173–181. [Google Scholar] [CrossRef]
- Staderini, E.; Meuli, S.; Gallenzi, P. Orthodontic treatment of class three malocclusion using clear aligners: A case report. J. Oral Biol. Craniofacial Res. 2019, 9, 360–362. [Google Scholar] [CrossRef]
- Staderini, E.; Patini, R.; Meuli, S.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Indication of clear aligners in the early treatment of anterior crossbite: A case series. Dent. Press J. Orthod. 2020, 25, 33–43. [Google Scholar] [CrossRef]
- Strobl, H.; Emshoff, R.; Rothler, G. Conservative treatment of unilateral condylar fractures in children: A long-term clinical and radiologic follow-up of 55 patients. Int. J. Oral Maxillofac. Surg. 1999, 28, 95–98. [Google Scholar] [CrossRef]
- Deplagne, M.; Donazzan, M.; Carlier, C. Les Fractures De La Region Condylienne. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1966, 21, 417–418. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Country | Type of Study | Sample | Total Score (IHE) | Total Score (NIH) |
|---|---|---|---|---|---|---|
| Nieke et al. | 1998 | Germany | Retrospective case-control | T: 19 patients C: 20 patients | 14/20 | 8/9 |
| Zhao et al. | 2012 | China | Retrospective | 40 patients | 11/20 | 5/9 |
| Liu et al. | 2013 | China | Retrospective | 30 patients | 11/20 | 4/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staderini, E.; Patini, R.; Tepedino, M.; Gasparini, G.; Zimbalatti, M.A.; Marradi, F.; Gallenzi, P. Radiographic Assessment of Pediatric Condylar Fractures after Conservative Treatment with Functional Appliances—A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9204. https://doi.org/10.3390/ijerph17249204
Staderini E, Patini R, Tepedino M, Gasparini G, Zimbalatti MA, Marradi F, Gallenzi P. Radiographic Assessment of Pediatric Condylar Fractures after Conservative Treatment with Functional Appliances—A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9204. https://doi.org/10.3390/ijerph17249204
Chicago/Turabian StyleStaderini, Edoardo, Romeo Patini, Michele Tepedino, Giulio Gasparini, Maria Antonietta Zimbalatti, Francesca Marradi, and Patrizia Gallenzi. 2020. "Radiographic Assessment of Pediatric Condylar Fractures after Conservative Treatment with Functional Appliances—A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 24: 9204. https://doi.org/10.3390/ijerph17249204
APA StyleStaderini, E., Patini, R., Tepedino, M., Gasparini, G., Zimbalatti, M. A., Marradi, F., & Gallenzi, P. (2020). Radiographic Assessment of Pediatric Condylar Fractures after Conservative Treatment with Functional Appliances—A Systematic Review. International Journal of Environmental Research and Public Health, 17(24), 9204. https://doi.org/10.3390/ijerph17249204