Geriatric Nutritional Risk Index as a Tool to Evaluate Impact of Malnutrition Risk on Mortality in Adult Patients with Polytrauma


 ,
, 
Abstract
:1. Background
2. Methods
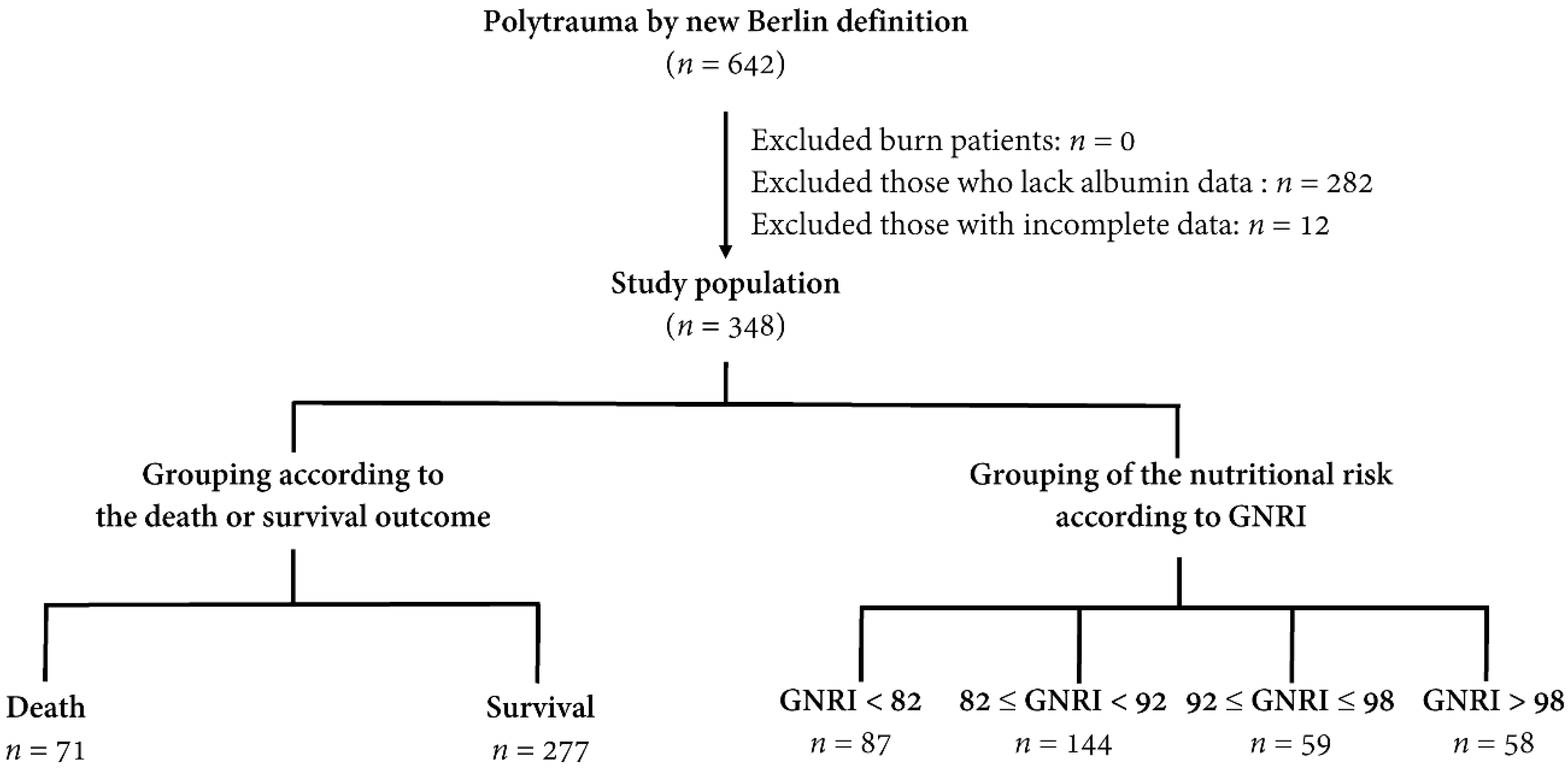
2.1. Study Population and Data Collection
2.2. Statistical Analyses
3. Results
3.1. Patient and Injury Characteristics of the Death and Survival Groups of Patients
3.2. Analysis of the Risk Factors for Mortality
3.3. Patient and Injury Characteristics of the Patients with Different Nutritional Risks
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dijkink, S.; Meier, K.; Krijnen, P.; Yeh, D.D.; Velmahos, G.C.; Schipper, I.B. Malnutrition and its effects in severely injured trauma patients. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2020. [Google Scholar] [CrossRef] [Green Version]
- Birkhahn, R.H.; Long, C.L.; Fitkin, D.; Jeevanandam, M.; Blakemore, W.S. Whole-body protein metabolism due to trauma in man as estimated by L-[15N]alanine. Am. J. Physiol. 1981, 241, E64–E71. [Google Scholar] [CrossRef]
- Dickerson, R.N.; Pitts, S.L.; Maish, G.O., 3rd; Schroeppel, T.J.; Magnotti, L.J.; Croce, M.A.; Minard, G.; Brown, R.O. A reappraisal of nitrogen requirements for patients with critical illness and trauma. J. Trauma Acute Care Surg. 2012, 73, 549–557. [Google Scholar] [CrossRef]
- Taylor, S.J.; Fettes, S.B.; Jewkes, C.; Nelson, R.J. Prospective, randomized, controlled trial to determine the effect of early enhanced enteral nutrition on clinical outcome in mechanically ventilated patients suffering head injury. Crit. Care Med. 1999, 27, 2525–2531. [Google Scholar] [CrossRef]
- Doig, G.S.; Heighes, P.T.; Simpson, F.; Sweetman, E.A. Early enteral nutrition reduces mortality in trauma patients requiring intensive care: A meta-analysis of randomised controlled trials. Injury 2011, 42, 50–56. [Google Scholar] [CrossRef]
- Van Bokhorst-de van der Schueren, M.A.; Guaitoli, P.R.; Jansma, E.P.; de Vet, H.C. Nutrition screening tools: Does one size fit all? A systematic review of screening tools for the hospital setting. Clin. Nutr. (Edinb. Scotl.) 2014, 33, 39–58. [Google Scholar] [CrossRef]
- Erstad, B.L. Serum Albumin Levels: Who Needs Them? Ann. Pharmacother. 2020. [Google Scholar] [CrossRef]
- Li, S.; Zhang, J.; Zheng, H.; Wang, X.; Liu, Z.; Sun, T. Prognostic Role of Serum Albumin, Total Lymphocyte Count, and Mini Nutritional Assessment on Outcomes After Geriatric Hip Fracture Surgery: A Meta-Analysis and Systematic Review. J. Arthroplast. 2019, 34, 1287–1296. [Google Scholar] [CrossRef]
- Loftus, T.J.; Brown, M.P.; Slish, J.H.; Rosenthal, M.D. Serum Levels of Prealbumin and Albumin for Preoperative Risk Stratification. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2019, 34, 340–348. [Google Scholar] [CrossRef]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and Clinical Significance. Jpen. J. Parenter. Enter. Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef] [Green Version]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). Jpen. J. Parenter. Enter. Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Cereda, E.; Zagami, A.; Vanotti, A.; Piffer, S.; Pedrolli, C. Geriatric Nutritional Risk Index and overall-cause mortality prediction in institutionalised elderly: A 3-year survival analysis. Clin. Nutr. 2008, 27, 717–723. [Google Scholar] [CrossRef]
- Cereda, E.; Vanotti, A. The new Geriatric Nutritional Risk Index is a good predictor of muscle dysfunction in institutionalized older patients. Clin. Nutr. 2007, 26, 78–83. [Google Scholar] [CrossRef]
- Cereda, E.; Pusani, C.; Limonta, D.; Vanotti, A. The ability of the Geriatric Nutritional Risk Index to assess the nutritional status and predict the outcome of home-care resident elderly: A comparison with the Mini Nutritional Assessment. Br. J. Nutr. 2009, 102, 563–570. [Google Scholar] [CrossRef]
- Durán Alert, P.; Milà Villarroel, R.; Formiga, F.; Virgili Casas, N.; Vilarasau Farré, C. Assessing risk screening methods of malnutrition in geriatric patients: Mini Nutritional Assessment (MNA) versus Geriatric Nutritional Risk Index (GNRI). Nutr. Hosp. 2012, 27, 590–598. [Google Scholar] [CrossRef]
- Han, J.Y.; Lee, K.H.; Kim, S.W.; Min, Y.J.; Cho, E.; Lee, Y.; Lee, S.H.; Kim, H.Y.; Lee, G.K.; Nam, B.H.; et al. A Phase II Study of Poziotinib in Patients with Epidermal Growth Factor Receptor (EGFR)-Mutant Lung Adenocarcinoma Who Have Acquired Resistance to EGFR-Tyrosine Kinase Inhibitors. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2017, 49, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Kushiyama, S.; Sakurai, K.; Kubo, N.; Tamamori, Y.; Nishii, T.; Tachimori, A.; Inoue, T.; Maeda, K. The Preoperative Geriatric Nutritional Risk Index Predicts Postoperative Complications in Elderly Patients with Gastric Cancer Undergoing Gastrectomy. In Vivo 2018, 32, 1667–1672. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Ahn, J.M.; Kang, D.Y.; Ko, E.; Kwon, O.; Lee, P.H.; Lee, S.W.; Kim, D.H.; Kim, H.J.; Kim, J.B.; et al. Nutritional status and risk of all-cause mortality in patients undergoing transcatheter aortic valve replacement assessment using the geriatric nutritional risk index and the controlling nutritional status score. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2020, 109, 161–171. [Google Scholar] [CrossRef]
- Mii, S.; Guntani, A.; Kawakubo, E.; Shimazoe, H.; Ishida, M. Impact of the Geriatric Nutritional Risk Index on the Long-Term Outcomes of Patients Undergoing Open Bypass for Intermittent Claudication. Circ. J. Off. J. Jpn. Circ. Soc. 2019, 83, 1349–1355. [Google Scholar] [CrossRef] [Green Version]
- Shibata, K.; Yamamoto, M.; Kano, S.; Koyama, Y.; Shimura, T.; Kagase, A.; Yamada, S.; Kobayashi, T.; Tada, N.; Naganuma, T.; et al. Importance of Geriatric Nutritional Risk Index assessment in patients undergoing transcatheter aortic valve replacement. Am. Heart J. 2018, 202, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Kubo, N.; Sakurai, K.; Tamura, T.; Toyokawa, T.; Tanaka, H.; Muguruma, K.; Yashiro, M.; Ohira, M. The impact of geriatric nutritional risk index on surgical outcomes after esophagectomy in patients with esophageal cancer. Esophagus Off. J. Jpn. Esophageal Soc. 2019, 16, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Choi, H.S.; Ko, Y.G.; Yun, D.H. Performance of the Geriatric Nutritional Risk Index in predicting 28-day hospital mortality in older adult patients with sepsis. Clin. Nutr. 2013, 32, 843–848. [Google Scholar] [CrossRef]
- Nishi, I.; Seo, Y.; Hamada-Harimura, Y.; Yamamoto, M.; Ishizu, T.; Sugano, A.; Sato, K.; Sai, S.; Obara, K.; Suzuki, S.; et al. Geriatric nutritional risk index predicts all-cause deaths in heart failure with preserved ejection fraction. Esc Heart Fail. 2019, 6, 396–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumura, T.; Mitani, Y.; Oki, Y.; Fujimoto, Y.; Ohira, M.; Kaneko, H.; Kawashima, T.; Nishio, M.; Ishikawa, A. Comparison of Geriatric Nutritional Risk Index scores on physical performance among elderly patients with chronic obstructive pulmonary disease. Heart Lung 2015, 44, 534–538. [Google Scholar] [CrossRef]
- Kuo, I.C.; Huang, J.C.; Wu, P.Y.; Chen, S.C.; Chang, J.M.; Chen, H.C. A Low Geriatric Nutrition Risk Index Is Associated with Progression to Dialysis in Patients with Chronic Kidney Disease. Nutrients 2017, 9, 1228. [Google Scholar] [CrossRef] [Green Version]
- Lidoriki, I.; Schizas, D.; Frountzas, M.; Machairas, N.; Prodromidou, A.; Kapelouzou, A.; Karavokyros, I.; Pikoulis, E.; Kales, S.N.; Liakakos, T. GNRI as a Prognostic Factor for Outcomes in Cancer Patients: A Systematic Review of the Literature. Nutr. Cancer 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Lv, G.Y.; An, L.; Sun, D.W. Geriatric Nutritional Risk Index Predicts Adverse Outcomes in Human Malignancy: A Meta-Analysis. Dis. Markers 2019, 2019, 4796598. [Google Scholar] [CrossRef] [Green Version]
- Hirose, S.; Miyazaki, S.; Yatsu, S.; Sato, A.; Ishiwata, S.; Matsumoto, H.; Shitara, J.; Murata, A.; Kato, T.; Suda, S.; et al. Impact of the Geriatric Nutritional Risk Index on In-Hospital Mortality and Length of Hospitalization in Patients with Acute Decompensated Heart Failure with Preserved or Reduced Ejection Fraction. J. Clin. Med. 2020, 9, 1169. [Google Scholar] [CrossRef] [Green Version]
- Kaito, S.; Wada, A.; Adachi, H.; Konuma, R.; Kishida, Y.; Nagata, A.; Konishi, T.; Yamada, Y.; Kumagai, T.; Yoshifuji, K.; et al. Geriatric nutritional risk index as a useful prognostic factor in second allogeneic hematopoietic stem cell transplantation. Ann. Hematol. 2020, 99, 1655–1665. [Google Scholar] [CrossRef]
- Kang, S.H.; Cho, K.H.; Park, J.W.; Yoon, K.W.; Do, J.Y. Geriatric Nutritional Risk Index as a prognostic factor in peritoneal dialysis patients. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2013, 33, 405–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokumoto, H.; Tominaga, H.; Arishima, Y.; Jokoji, G.; Akimoto, M.; Ohtsubo, H.; Taketomi, E.; Sunahara, N.; Nagano, S.; Ishidou, Y.; et al. Association between Bone Mineral Density of Femoral Neck and Geriatric Nutritional Risk Index in Rheumatoid Arthritis Patients Treated with Biological Disease-Modifying Anti-Rheumatic Drugs. Nutrients 2018, 10, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.T.; Hu, F.H.; Lien, T.J.; Chen, P.J.; Huang, T.P.; Tarng, D.C. Interaction between geriatric nutritional risk index and decoy receptor 3 predicts mortality in chronic hemodialysis patients. Am. J. Nephrol. 2014, 40, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Chien, P.C. Defining polytrauma by abbreviated injury scale ≥ 3 for a least two body regions is insufficient in terms of short-term outcome: A cross-sectional study at a level I trauma center. Biomed. J. 2018, 41, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Pape, H.C.; Lefering, R.; Butcher, N.; Peitzman, A.; Leenen, L.; Marzi, I.; Lichte, P.; Josten, C.; Bouillon, B.; Schmucker, U.; et al. The definition of polytrauma revisited: An international consensus process and proposal of the new ‘Berlin definition’. J. Trauma Acute Care Surg. 2014, 77, 780–786. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Cameron, P.A.; Wolfe, R. TRISS: Does it get better than this? Acad. Emerg. Med. 2004, 11, 181–186. [Google Scholar] [CrossRef]
- Glance, L.G.; Osler, T. Beyond the major trauma outcome study: Benchmarking performance using a national contemporary, population-based trauma registry. J. Trauma 2001, 51, 725–727. [Google Scholar] [CrossRef]
- De Munter, L.; Polinder, S.; Lansink, K.W.; Cnossen, M.C.; Steyerberg, E.W.; de Jongh, M.A. Mortality prediction models in the general trauma population: A systematic review. Injury 2017, 48, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Champion, H.R.; Sacco, W.J.; Copes, W.S.; Gann, D.S.; Gennarelli, T.A.; Flanagan, M.E. A revision of the Trauma Score. J. Trauma 1989, 29, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Köseoğlu, Z.; Ozdoğan, M.; Kuvvetli, A.; Kösenli, O.; Oruç, C.; Onel, S.; Das, K.; Akova, A. Increased nutritional risk in major trauma: Correlation with complications and prolonged length of stay. Ulus. Travma Acil Cerrahi Derg. = Turk. J. Trauma Emerg. Surg. TJTES 2011, 17, 521–524. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.J.; Andersen, H.K.; Thomas, S. Early enteral nutrition within 24 h of intestinal surgery versus later commencement of feeding: A systematic review and meta-analysis. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2009, 13, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pusani, C.; Limonta, D.; Vanotti, A. The association of Geriatric Nutritional Risk Index and total lymphocyte count with short-term nutrition-related complications in institutionalised elderly. J. Am. Coll. Nutr. 2008, 27, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Limonta, D.; Pusani, C.; Vanotti, A. Assessing elderly at risk of malnutrition: The new Geriatric Nutritional Risk Index versus Nutritional Risk Index. Nutrition 2006, 22, 680–682. [Google Scholar] [CrossRef] [PubMed]
- Artinyan, A.; Orcutt, S.T.; Anaya, D.A.; Richardson, P.; Chen, G.J.; Berger, D.H. Infectious postoperative complications decrease long-term survival in patients undergoing curative surgery for colorectal cancer: A study of 12,075 patients. Ann. Surg. 2015, 261, 497–505. [Google Scholar] [CrossRef]
- Nathan, H.; Yin, H.; Wong, S.L. Postoperative Complications and Long-Term Survival After Complex Cancer Resection. Ann. Surg. Oncol. 2017, 24, 638–644. [Google Scholar] [CrossRef]
- Matsuo, Y.; Kumakura, H.; Kanai, H.; Iwasaki, T.; Ichikawa, S. The Geriatric Nutritional Risk Index Predicts Long-Term Survival and Cardiovascular or Limb Events in Peripheral Arterial Disease. J. Atheroscler. Thromb. 2020, 27, 134–143. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Zhou, X.; Zheng, C. The geriatric nutritional risk index independently predicts adverse outcomes in patients with pyogenic liver abscess. BMC Geriatr. 2019, 19, 14. [Google Scholar] [CrossRef] [Green Version]
- Mendes, N.P.; Barros, T.A.; Rosa, C.O.B.; Franceschini, S. Nutritional Screening Tools Used and Validated for Cancer Patients: A Systematic Review. Nutr. Cancer 2019, 71, 898–907. [Google Scholar] [CrossRef]
- Torbahn, G.; Strauss, T.; Sieber, C.C.; Kiesswetter, E.; Volkert, D. Nutritional status according to the mini nutritional assessment (MNA)® as potential prognostic factor for health and treatment outcomes in patients with cancer—A systematic review. BMC Cancer 2020, 20, 594. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Death n = 71 | Survival n = 277 | p | ||
|---|---|---|---|---|---|
| Gender | 0.519 | ||||
| Male, n (%) | 52 | (73.2) | 192 | (69.3) | |
| Female, n (%) | 19 | (26.8) | 85 | (30.7) | |
| Age (years) | 56.4 | ±21.9 | 54.7 | ±19.5 | 0.522 |
| Co-morbidities | |||||
| DM, n (%) | 14 | (19.7) | 43 | (15.5) | 0.394 |
| HTN, n (%) | 16 | (22.5) | 81 | (29.2) | 0.261 |
| CAD, n (%) | 6 | (8.5) | 13 | (4.7) | 0.214 |
| ESRD, n (%) | 0 | (0.0) | 3 | (0.1) | - |
| Injury mechanism | 0.378 | ||||
| Blunt, n (%) | 71 | (100.0) | 274 | (98.9) | |
| Penetrating, n (%) | 0 | (0.0) | 3 | (1.1) | |
| SBP (mmHg) | 122.1 | ±55.1 | 119.9 | ±41.3 | 0.706 |
| RR (times/min) | 19.9 | ±7.1 | 20.4 | ±5.6 | 0.516 |
| GCS, median (IQR) | 5 | (3–8) | 11 | (6–15) | <0.001 |
| 3–8, n (%) | 54 | (76.1) | 123 | (44.4) | <0.001 |
| 9–12, n (%) | 4 | (5.6) | 34 | (12.3) | 0.109 |
| 13–15, n (%) | 13 | (18.3) | 120 | (43.3) | <0.001 |
| ISS, median (IQR) | 35 | (29–41) | 29 | (22–34) | <0.001 |
| 16–24, n (%) | 4 | (5.6) | 81 | (29.2) | <0.001 |
| ≥25, n (%) | 67 | (94.4) | 196 | (70.8) | <0.001 |
| Albumin (g/dL) | 2.7 | ±0.8 | 3.2 | ±0.7 | <0.001 |
| BMI | 25.4 | ±4.7 | 25.2 | ±4.4 | 0.673 |
| GNRI | 83.0 | ±10.4 | 89.0 | ±9.1 | <0.001 |
| LOS in hospital (days) | 14.7 | ±18.7 | 29.5 | ±17.6 | <0.001 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |||
| Gender | 1.2 | (0.68–2.17) | 0.520 | 1.2 | (0.62–2.50) | 0.538 |
| Age | 1.0 | (0.99–1.02) | 0.521 | 1.0 | (0.99–1.04) | 0.068 |
| DM | 1.3 | (0.69–2.61) | 0.395 | 2.2 | (0.93–5.18) | 0.072 |
| HTN | 0.7 | (0.38–1.30) | 0.262 | 0.5 | (0.24–1.18) | 0.119 |
| CAD | 1.9 | (0.69–5.12) | 0.220 | 1.7 | (0.48–5.96) | 0.408 |
| GCS | 0.85 | (0.79–0.90) | <0.001 | 0.88 | (0.83–0.95) | <0.001 |
| ISS | 1.09 | (1.06–1.13) | <0.001 | 1.07 | (1.04–1.11) | <0.001 |
| GNRI | 0.94 | (0.91–0.96) | <0.001 | 0.94 | (0.91–0.97) | <0.001 |
| Variables | Group 1 | Group 2 | Group 3 | Group 4 | p |
|---|---|---|---|---|---|
| n = 87 | n = 144 | n = 59 | n = 58 | ||
| Gender | 0.009 | ||||
| Male, n (%) | 51 (58.6) * | 99 (68.9) | 47 (79.7) | 47 (81.0) | |
| Female, n (%) | 36 (41.4) * | 45 (31.2) | 12 (20.3) | 11 (19.0) | |
| Age (years) | 56.2 ± 19.7 | 57.0 ± 19.9 | 51.3 ± 19.6 | 52.3 ± 20.7 | 0.191 |
| BMI | 20.0 ± 4.8 * | 25.3 ± 4.5 | 25.2 ± 4.0 | 26.9 ± 3.7 | 0.002 |
| Co-morbidities | |||||
| DM, n (%) | 10 (11.5) | 29 (20.1) | 10 (16.9) | 8 (13.8) | 0.348 |
| HTN, n (%) | 20 (23.0) | 44 (30.6) | 17 (28.8) | 16 (27.6) | 0.665 |
| CAD, n (%) | 4 (4.6) | 8 (5.6) | 6 (10.2) | 1 (1.7) | 0.238 |
| ESRD, n (%) | 0 (0.0) | 3 (2.1) | 0 (0.0) | 0 (0.0) | 0.232 |
| GCS, median (IQR) | 8 (3–15) | 11 (6–15) | 8 (5–15) | 8 (5–15) | 0.214 |
| 3–8, n (%) | 48 (55.2) | 65 (45.1) | 32 (54.2) | 32 (55.2) | 0.357 |
| 9–12, n (%) | 9 (10.3) | 19 (13.2) | 4 (6.8) | 6 (10.3) | 0.603 |
| 13–15, n (%) | 30 (34.5) | 60 (41.7) | 23 (39.0) | 20 (34.5) | 0.660 |
| ISS, median (IQR) | 29 (25–38) | 29 (25–36) | 29 (25–36) | 29 (22–34) | 0.593 |
| 1–15, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| 16–24, n (%) | 21 (24.1) | 31 (21.5) | 13 (22.0) | 20 (34.5) | 0.259 |
| ≥25, n (%) | 66 (75.9) | 113 (78.5) | 46 (78.0) | 38 (65.5) | 0.259 |
| Mortality, n (%) | 30 (34.5) * | 29 (20.1) | 5 (8.5) | 7 (12.1) | <0.001 |
| LOS in hospital (days) | 29.7 ± 24.4 | 26.1 ± 16.5 | 24.9 ± 13.6 | 24.3 ± 18.6 | 0.291 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, C.-H.; Wu, S.-C.; Chou, S.-E.; Su, W.-T.; Tsai, C.-H.; Li, C.; Hsu, S.-Y.; Hsieh, C.-H. Geriatric Nutritional Risk Index as a Tool to Evaluate Impact of Malnutrition Risk on Mortality in Adult Patients with Polytrauma. Int. J. Environ. Res. Public Health 2020, 17, 9233. https://doi.org/10.3390/ijerph17249233
Yeh C-H, Wu S-C, Chou S-E, Su W-T, Tsai C-H, Li C, Hsu S-Y, Hsieh C-H. Geriatric Nutritional Risk Index as a Tool to Evaluate Impact of Malnutrition Risk on Mortality in Adult Patients with Polytrauma. International Journal of Environmental Research and Public Health. 2020; 17(24):9233. https://doi.org/10.3390/ijerph17249233
Chicago/Turabian StyleYeh, Cheng-Hsi, Shao-Chun Wu, Sheng-En Chou, Wei-Ti Su, Ching-Hua Tsai, Chi Li, Shiun-Yuan Hsu, and Ching-Hua Hsieh. 2020. "Geriatric Nutritional Risk Index as a Tool to Evaluate Impact of Malnutrition Risk on Mortality in Adult Patients with Polytrauma" International Journal of Environmental Research and Public Health 17, no. 24: 9233. https://doi.org/10.3390/ijerph17249233
APA StyleYeh, C. -H., Wu, S. -C., Chou, S. -E., Su, W. -T., Tsai, C. -H., Li, C., Hsu, S. -Y., & Hsieh, C. -H. (2020). Geriatric Nutritional Risk Index as a Tool to Evaluate Impact of Malnutrition Risk on Mortality in Adult Patients with Polytrauma. International Journal of Environmental Research and Public Health, 17(24), 9233. https://doi.org/10.3390/ijerph17249233