Neighborhood Social Cohesion and Sleep Health by Age, Sex/Gender, and Race/Ethnicity in the United States

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. National Health Interview Survey
2.2. Study Population
2.3. Exposure Assessment: Neighborhood Social Cohesion
2.4. Outcome Assessment: Self-Reported Sleep Duration and Sleep Disturbances
2.5. Potential Confounders
2.6. Potential Modifiers: Age, Sex/Gender, and Race/Ethnicity
2.7. Statistical Analyses
3. Results
3.1. Study Population Characteristics
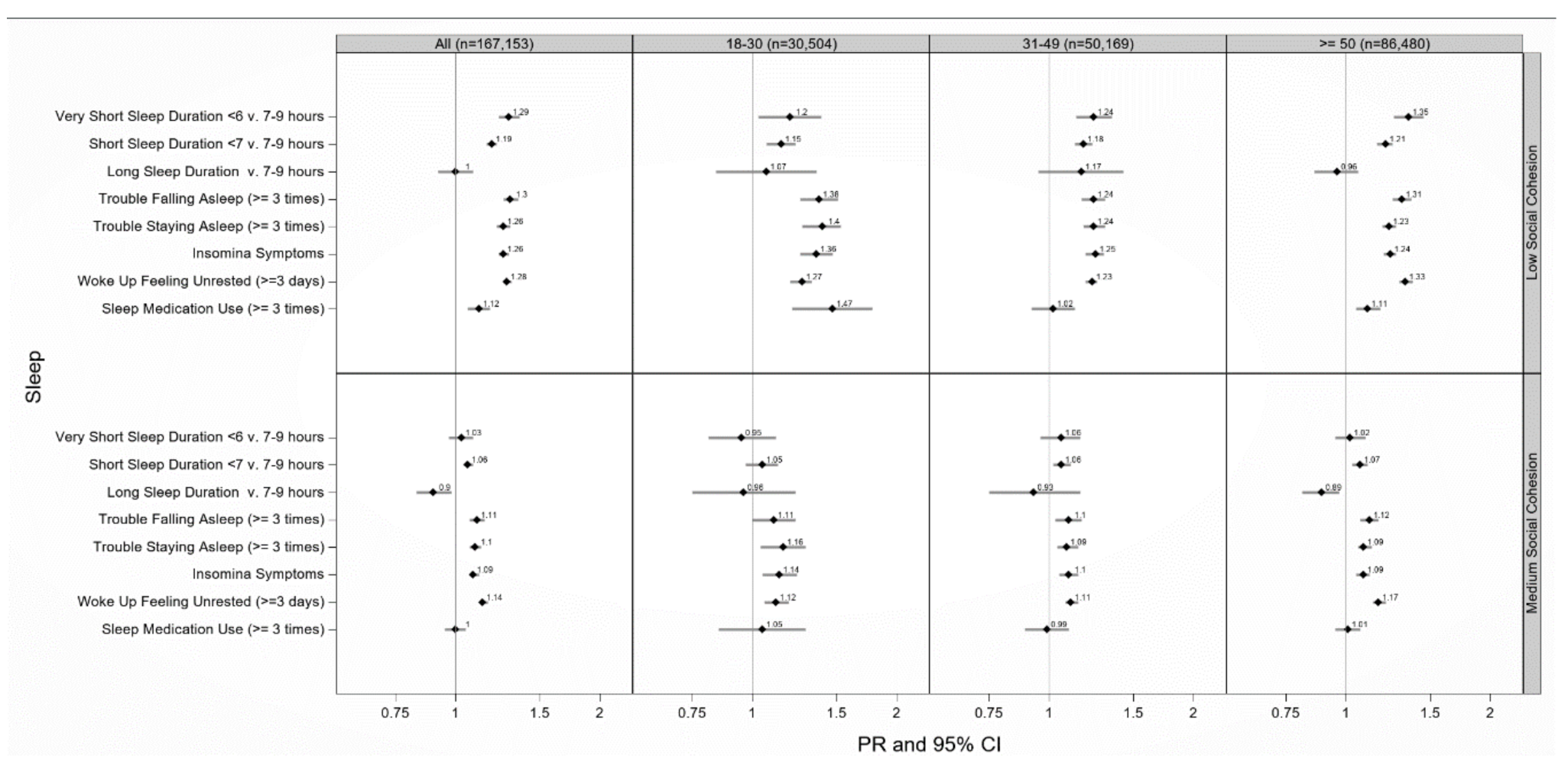
3.2. Neighborhood Social Cohesion and Multiple Sleep Dimensions
3.3. Neighborhood Social Cohesion and Multiple Sleep Dimensions by Age
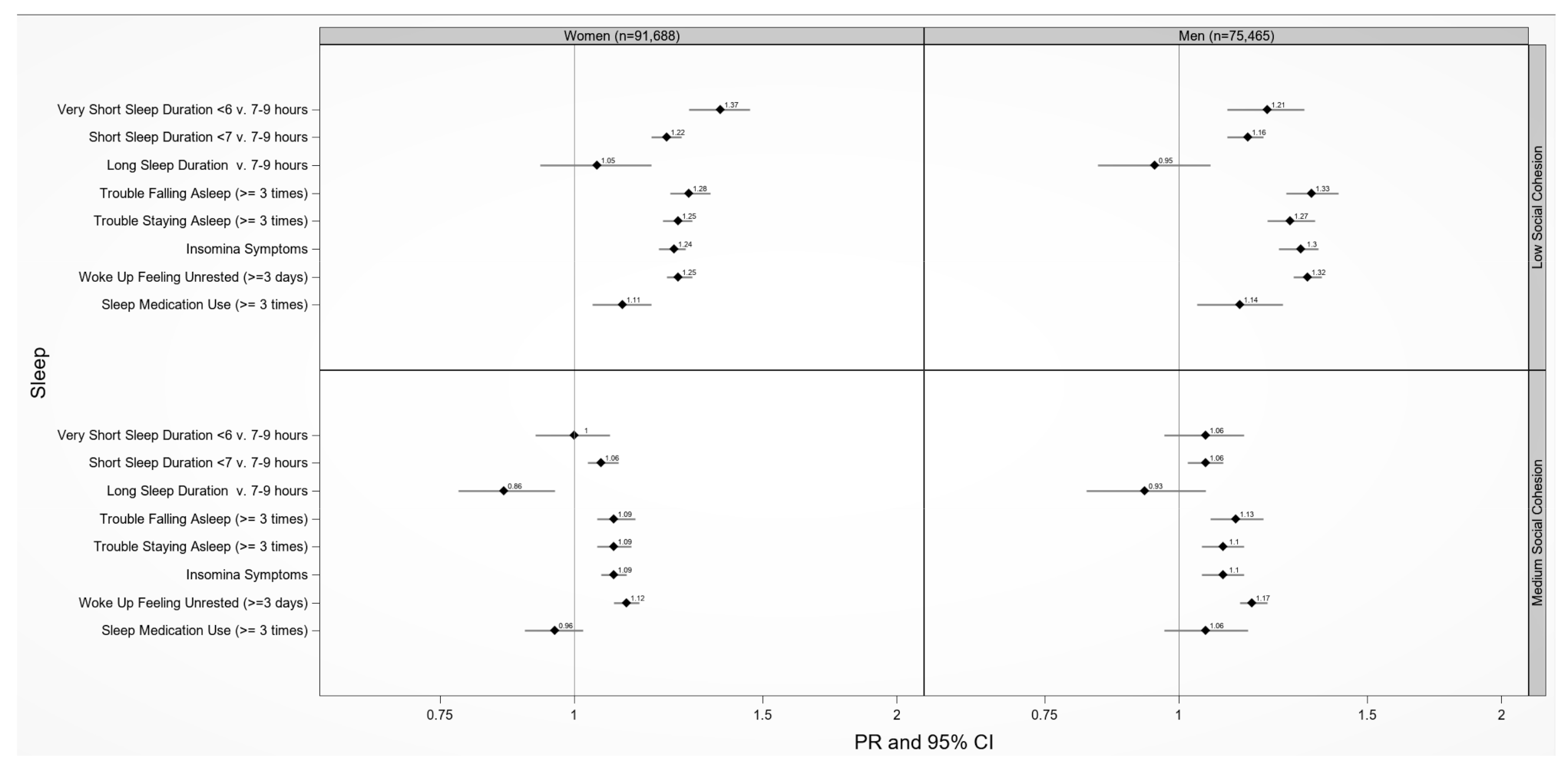
3.4. Neighborhood Social Cohesion and Multiple Sleep Dimensions by Sex/Gender
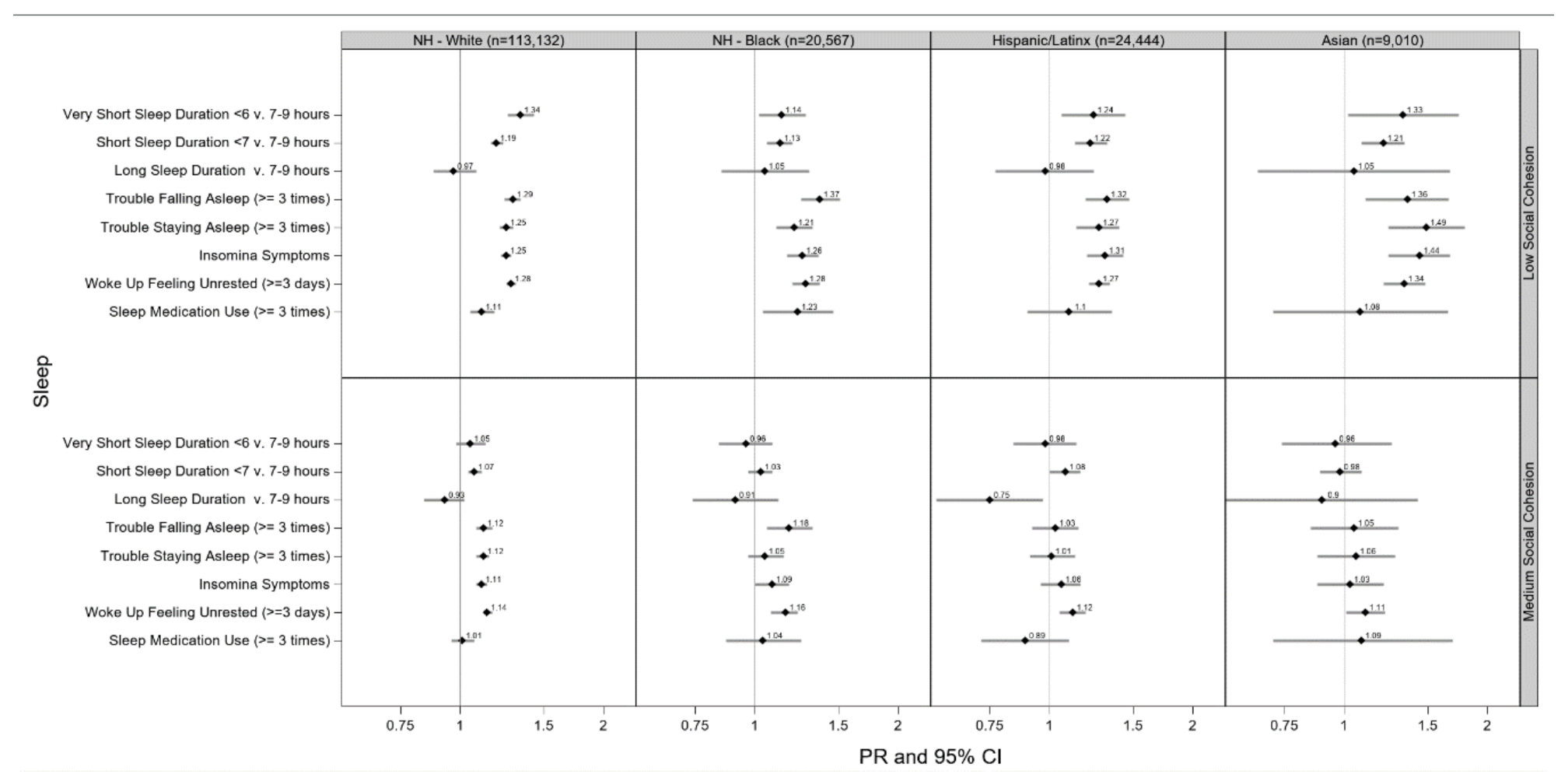
3.5. Neighborhood Social Cohesion and Multiple Sleep Dimensions by Race/Ethnicity
3.6. Neighborhood Social Cohesion and Multiple Sleep Dimensions by Age, Sex/Gender, and Race/Ethnicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine Report. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; Colten, H.R.; Altevogt, B.M. (Eds.) National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Liu, Y. Prevalence of healthy sleep duration among adults US 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, C.N.; Canham, S.L.; Mojtabai, R.; Gum, A.M.; Dautovich, N.D.; Kohn, R.; Spira, A.P. Insomnia and health services utilization in middle-aged and older adults: Results from the Health and Retirement Study. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1512–1517. [Google Scholar] [CrossRef] [Green Version]
- Theorell-Haglow, J.; Miller, C.B.; Bartlett, D.J.; Yee, B.J.; Openshaw, H.D.; Grunstein, R.R. Gender differences in obstructive sleep apnoea, insomnia and restless legs syndrome in adults–What do we know? A clinical update. Sleep Med. Rev. 2018, 38, 28–38. [Google Scholar] [CrossRef]
- Chen, X.; Wang, R.; Zee, P.; Lutsey, P.L.; Javaheri, S.; Alcantara, C.; Jackson, C.L.; Williams, M.A.; Redline, S. Racial/Ethnic Differences in Sleep Disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2015, 38, 877–888. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.L.; Redline, S.; Emmons, K.M. Sleep as a potential fundamental contributor to disparities in cardiovascular health. Annu. Rev. Public Health 2015, 36, 417–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnethon, M.R.; De Chavez, P.J.; Zee, P.C.; Kim, K.Y.; Liu, K.; Goldberger, J.J.; Ng, J.; Knutson, K.L. Disparities in sleep characteristics by race/ethnicity in a population-based sample: Chicago Area Sleep Study. Sleep Med. 2016, 18, 50–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whinnery, J.; Jackson, N.; Rattanaumpawan, P.; Grandner, M.A. Short and long sleep duration associated with race/ethnicity, sociodemographics, and socioeconomic position. Sleep 2014, 37, 601–611. [Google Scholar] [CrossRef]
- Garbarino, S.; Magnavita, N. Sleep problems are a strong predictor of stress-related metabolic changes in police officers. A prospective study. PLoS ONE 2019, 14, e0224259. [Google Scholar] [CrossRef] [Green Version]
- Desantis, A.S.; Diez Roux, A.V.; Moore, K.; Baron, K.G.; Mujahid, M.S.; Nieto, F.J. Associations of neighborhood characteristics with sleep timing and quality: The Multi-Ethnic Study Of Atherosclerosis. Sleep 2013, 36, 1543–1551. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.A.; Brown, D.L.; Morgenstern, L.B.; Meurer, W.J.; Lisabeth, L.D. The association of neighborhood characteristics with sleep duration and daytime sleepiness. Sleep Health 2015, 1, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I.; Berkman, L.F. Social Cohesion, Social Capital, and Health. In Social Epidemiology; Kawachi, I., Berkman, L.F., Eds.; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Hale, L.; Hill, T.D.; Friedman, E.; Nieto, F.J.; Galvao, L.W.; Engelman, C.D.; Malecki, K.M.; Peppard, P.E. Perceived neighborhood quality, sleep quality, and health status: Evidence from the Survey of the Health of Wisconsin. Soc. Sci. Med. 2013, 79, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, D.A.; Al-Ajlouni, Y.A.; Duncan, S.D.T. Connecting Neighborhoods and Sleep Health. Soc. Epidemiol. Sleep 2019, 409–430. [Google Scholar]
- Hirotsu, C.; Tufik, S.; Andersen, M.L. Interactions between sleep, stress, and metabolism: From physiological to pathological conditions. Sleep Sci. 2015, 8, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnavita, N.; Di Stasio, E.; Capitanelli, I.; Lops, E.A.; Chirico, F.; Garbarino, S. Sleep Problems and Workplace Violence: A Systematic Review and Meta-Analysis. Front. Neurosci. 2019, 13, 997. [Google Scholar] [CrossRef]
- Johnson, D.A.; Simonelli, G.; Moore, K.; Billings, M.; Mujahid, M.S.; Rueschman, M.; Kawachi, I.; Redline, S.; Diez Roux, A.V.; Patel, S.R. The Neighborhood Social Environment and Objective Measures of Sleep in the Multi-Ethnic Study of Atherosclerosis. Sleep 2017, 40. [Google Scholar] [CrossRef]
- Lang, I.A.; Llewellyn, D.J.; Langa, K.M.; Wallace, R.B.; Huppert, F.A.; Melzer, D. Neighborhood deprivation, individual socioeconomic status, and cognitive function in older people: Analyses from the English Longitudinal Study of Ageing. J. Am. Geriatr. Soc. 2008, 56, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Adams, M.A.; Sallis, J.F.; Conway, T.L.; Frank, L.D.; Saelens, B.E.; Kerr, J.; Cain, K.L.; King, A.C. Neighborhood environment profiles for physical activity among older adults. Am. J. Health Behav. 2012, 36, 757–769. [Google Scholar] [CrossRef]
- Chen-Edinboro, L.P.; Kaufmann, C.N.; Augustinavicius, J.L.; Mojtabai, R.; Parisi, J.M.; Wennberg, A.M.; Smith, M.T.; Spira, A.P. Neighborhood physical disorder, social cohesion, and insomnia: Results from participants over age 50 in the Health and Retirement Study. Int. Psychogeriatr. 2014. [Google Scholar] [CrossRef]
- Guilcher, S.J.T.; Kaufman-Shriqui, V.; Hwang, J.; O’Campo, P.; Matheson, F.I.; Glazier, R.H.; Booth, G.L. The association between social cohesion in the neighborhood and body mass index (BMI): An examination of gendered differences among urban-dwelling Canadians. Prev. Med. 2017, 99, 293–298. [Google Scholar] [CrossRef]
- Molinari, C.; Ahern, M.; Hendryx, M. Relationship of Community Quality to Health of Women and Men. Soc. Sci. Med. 1998, 47, 8. [Google Scholar] [CrossRef]
- Almeida, J.; Kawachi, I.; Molnar, B.E.; Subramanian, S.V. A multilevel analysis of social ties and social cohesion among Latinos and their neighborhoods: Results from Chicago. J. Urban Health 2009, 86, 745–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobson-Prater, T.; Leech, T.G.J. The Significance of Race for Neighborhood Social Cohesion: Perceived Difficulty of Collective Action in Majority Black Neighborhoods. J. Soc. Soc. Welfare 2012, 39, 22. [Google Scholar]
- LaVeist, T.A. On the study of race, racism and health: A shift from description to explanation. Int. J. Health Serv. 2000, 30, 3. [Google Scholar] [CrossRef] [PubMed]
- House, J.S. Understanding social factors and inequalities in health: 20th century progress and 21st century prospects. J. Health Soc. Behav. 2002, 43, 125–142. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.A.; Jackson, C.L.; Williams, N.J.; Alcantara, C. Are sleep patterns influenced by race/ethnicity—A marker of relative advantage or disadvantage? Evidence to date. Nat. Sci. Sleep 2019, 11, 79–95. [Google Scholar] [CrossRef] [Green Version]
- Slopen, N.; Williams, D.R. Discrimination, other psychosocial stressors, and self-reported sleep duration and difficulties. Sleep 2014, 37, 147–156. [Google Scholar] [CrossRef] [Green Version]
- IPUMS Health Surveys: National Health Interview Survey, Version 6.2. Available online: https://nhis.ipums.org/nhis/ (accessed on 15 April 2020).
- National Health Interview Survey Description; Division of Health Interview Statistics, National Center for Health Statistics, Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2016.
- Sampson, R.J.; Raudenbush, S.; Earls, F. Neighborhoods and violent crime: A multielvel study of collective efficacy. Science 1997, 277, 7. [Google Scholar] [CrossRef]
- Young, M.C.; Gerber, M.W.; Ash, T.; Horan, C.M.; Taveras, E.M. Neighborhood social cohesion and sleep outcomes in the Native Hawaiian and Pacific Islander National Health Interview Survey. Sleep 2018, 41. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Adams Hillard, P.J.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripe, E.; Howes, M.J.; Normand, S.T.; Manderscheid, R.W.; Waltersm, E.E.; et al. Screenings for Serious Mental Illness in the General Population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassett, E.; Moore, S. Neighbourhood disadvantage, network capital and restless sleep: Is the association moderated by gender in urban-dwelling adults? Soc. Sci. Med. 2014, 108, 185–193. [Google Scholar] [CrossRef]
- Kavanagh, A.M.; Bentley, R.; Turrell, G.; Broom, D.H.; Subramanian, S.V. Does gender modify associations between self rated health and the social and economic characteristics of local environments? J. Epidemiol. Community Health 2006, 60, 490–495. [Google Scholar] [CrossRef] [Green Version]
- Stafford, M.A.I.; McMunn, A.; De Vogli, R. Neighbourhood social environment and depressive symptoms in mid-life and beyond. Ageing Soc. 2011, 31, 893–910. [Google Scholar] [CrossRef] [Green Version]
- Simonelli, G.; Patel, S.R.; Rodriguez-Espinola, S.; Perez-Chada, D.; Salvia, A.; Cardinali, D.P.; Vigo, D.E. The impact of home safety on sleep in a Latin American country. Sleep Health 2015, 1, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Q.; Hale, L. Neighborhood socioeconomic status, sleep duration, and napping in middle-to-old aged US men and women. Sleep 2018, 41. [Google Scholar] [CrossRef]
- Johnson, D.A.; Lisabeth, L.; Hickson, D.; Johnson-Lawrence, V.; Samdarshi, T.; Taylor, H.; Diez Roux, A.V. The Social Patterning of Sleep in African Americans: Associations of Socioeconomic Position and Neighborhood Characteristics with Sleep in the Jackson Heart Study. Sleep 2016, 39, 1749–1759. [Google Scholar] [CrossRef]
- Murillo, R.; Ayalew, L.; Hernandez, D.C. The association between neighborhood social cohesion and sleep duration in Latinos. Ethn. Health 2019. [Google Scholar] [CrossRef]
- Troxel, W.M.; DeSantis, A.; Richardson, A.S.; Beckman, R.; Ghosh-Dastidar, B.; Nugroho, A.; Hale, L.; Buysse, D.J.; Buman, M.P.; Dubowitz, T. Neighborhood disadvantage is associated with actigraphy-assessed sleep continuity and short sleep duration. Sleep 2018, 41. [Google Scholar] [CrossRef] [PubMed]
- Neergheen, V.L.; Topel, M.; Van Dyke, M.E.; Sullivan, S.; Pemu, P.E.; Gibbons, G.H.; Vaccarino, V.; Quyyumi, A.A.; Lewis, T.T. Neighborhood social cohesion is associated with lower levels of interleukin-6 in African American women. Brain Behav. Immun. 2019, 76, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, S.; Matthews, K.A.; von Kanel, R.; Hall, M.H.; Thurston, R.C. Sleep characteristics and inflammatory biomarkers among midlife women. Sleep 2018, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S.V. Social environment and physical activity: A review of concepts and evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.; Whittemore, R.; Jung, S.; Latkin, C.; Kershaw, T.; Redeker, N.S. Physical neighborhood and social environment, beliefs about sleep, sleep hygiene behaviors, and sleep quality among African Americans. Sleep Health 2018, 4, 258–264. [Google Scholar] [CrossRef]
- Jackson, C.L.; Patel, S.R.; Jackson, W.B., 2nd; Lutsey, P.L.; Redline, S. Agreement between self-reported and objectively measured sleep duration among white, black, Hispanic, and Chinese adults in the United States: Multi-Ethnic Study of Atherosclerosis. Sleep 2018, 41. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C.L.; Ward, J.B.; Johnson, D.A.; Sims, M.; Wilson, J.; Redline, S. Concordance between self-reported and actigraphy-assessed sleep duration among African-American adults: Findings from the Jackson Heart Sleep Study. Sleep 2020, 43. [Google Scholar] [CrossRef] [Green Version]
- Weden, M.M.; Carpiano, R.M.; Robert, S.A. Subjective and objective neighborhood characteristics and adult health. Soc. Sci. Med. 2008, 66, 1256–1270. [Google Scholar] [CrossRef]
- Jackson, C.L.; Gaston, S.A. The impact of environmental exposures on sleep. In Sleep and Health; Elsevier BV: Amsterdam, The Netherlands, 2019; pp. 85–103. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Neighborhood Social Cohesion | ||||
|---|---|---|---|---|
| Low n = 53,364 (32%) | Medium n = 55,163 (33%) | High n = 58,626 (35%) | Overall n = 167,153 (100%) | |
| Sociodemographic | ||||
| Age, mean (S.D.), years | 44.0 (0.13) | 47.1 (0.13) | 50.7 (0.14) | 47.4 (0.10) |
| 18–30 | 18.7% | 16.2% | 13.7% | 16.3% |
| 31–50 | 21.0% | 23.5% | 26.0% | 23.3% |
| ≥50 | 60.3% | 60.3% | 60.3% | 60.3% |
| Sex/gender | ||||
| Women | 52.2% | 49.5% | 53.0% | 51.9% |
| Race/ethnicity | ||||
| NH-White | 61.7% | 68.1% | 77.0% | 69.2% |
| NH-Black | 14.1% | 11.7% | 7.9% | 11.1% |
| Hispanic/Latinx | 19.0% | 13.9% | 10.2% | 14.2% |
| Asian | 5.2% | 6.3% | 5.0% | 5.5% |
| Educational attainment | ||||
| <High school | 13.6% | 9.4% | 8.2% | 10.3% |
| High school graduate | 29.8% | 26.5% | 26.1% | 27.4% |
| Some college | 31.1% | 29.7% | 29.7% | 30.2% |
| ≥College | 25.5% | 34.4% | 36.0% | 32.2% |
| Annual household income | ||||
| <$35,000 | 37.3% | 26.4% | 22.8% | 28.6% |
| $35–$74,999 | 32.1% | 30.0% | 28.0% | 30.1% |
| ≥$75,000 | 30.6% | 43.5% | 49.2% | 41.3% |
| Unemployed/not in labor force | 43.6% | 39.8% | 39.6% | 40.9% |
| Occupation class | ||||
| Professional/management | 17.6% | 22.8% | 23.6% | 21.5% |
| Support services | 44.1% | 44.4% | 46.5% | 45.2% |
| Laborers | 38.3% | 32.8% | 29.9% | 33.4% |
| Marital status | ||||
| Married/living with partner/co-habited | 55.3% | 62.3% | 66.7% | 61.7% |
| Divorced/widowed | 24.0% | 19.8% | 18.4% | 20.4% |
| Single/no live-in partner | 20.7% | 17.9% | 14.9% | 17.9% |
| Region of residence | ||||
| Northeast | 18.0% | 18.9% | 18.0% | 18.2% |
| Midwest | 21.2% | 22.6% | 23.7% | 22.5% |
| South | 36.3% | 35.6% | 37.9% | 36.7% |
| West | 24.5% | 22.9% | 20.4% | 22.6% |
| Health Behaviors | Low | Medium | High | Overall |
| Sleep duration | ||||
| <6 h (very short) | 11.8% | 7.9% | 7.5% | 8.9% |
| <7 h (short) | 36.2% | 30.5% | 27.9% | 31.3% |
| 7–9 h (recommended) | 59.3% | 65.9% | 68.2% | 64.7% |
| >9 h (long) | 4.5% | 3.6% | 3.9% | 4.0% |
| Trouble falling asleep (≥3 times/week) | 25.4% | 18.6% | 16.6% | 19.9% |
| Trouble staying asleep (≥3 times/week) | 32.2% | 26.3% | 24.4% | 27.4% |
| Insomnia symptoms b | 39.0% | 31.6% | 29.3% | 33.0% |
| Woke up feeling unrested (≥3 days/week) | 50.5% | 42.1% | 36.9% | 42.8% |
| Sleep medication (≥3 times/week) | 11.5% | 9.0% | 9.1% | 9.8% |
| Smoking status | ||||
| Never/quit > 12 months prior | 80.4% | 84.7% | 85.7% | 83.7% |
| Former | 1.5% | 1.3% | 1.2% | 1.3% |
| Current | 18.1% | 14.0% | 13.2% | 15.0% |
| Alcohol status | ||||
| Never | 20.3% | 18.6% | 19.3% | 19.4% |
| Former | 17.5% | 14.6% | 14.0% | 15.1% |
| Current | 62.2% | 66.9% | 66.7% | 65.5% |
| Leisure-time physical activity | ||||
| Never/unable | 37.9% | 30.5% | 28.5% | 32.0% |
| Does not meet PA guidelines | 19.4% | 19.1% | 18.2% | 18.9% |
| Meets PA guidelines c | 42.7% | 50.4% | 53.3% | 49.1% |
| Clinical Characteristics | Low | Medium | High | Overall |
| Health status | ||||
| Excellent/very good | 49.8% | 59.6% | 65.4% | 58.7% |
| Good | 30.5% | 27.6% | 23.9% | 27.2% |
| Fair/poor | 19.7% | 12.8% | 10.8% | 14.0% |
| Mental illness d | 5.7% | 2.6% | 2.2% | 3.4% |
| Body Mass Index (BMI) | ||||
| Recommended (18.5–< 25 km/m2) | 30.9% | 33.1% | 34.8% | 33.1% |
| Overweight (25–29.9 km/m2) | 34.6% | 36.6% | 36.5% | 36.0% |
| Obese (≥30 kg/m2) | 34.5% | 30.3% | 28.7% | 30.9% |
| Dyslipidemia e | 51.0% | 48.5% | 50.1% | 49.7% |
| Hypertension f | 38.6% | 35.3% | 33.8% | 35.7% |
| Prediabetes/diabetes g | 20.9% | 17.3% | 15.4% | 17.6% |
| “Ideal” cardiovascular health h | 7.5% | 10.2% | 11.5% | 9.8% |
| Sleep Health Dimensions | ||||||||
|---|---|---|---|---|---|---|---|---|
| Low Neighborhood Social Cohesion | Very short <6 vs. 7–9 h | Short <7 vs. 7–9 h | Long >9 vs. 7–9 h | Trouble falling asleep (≥3 times/week) | Trouble staying asleep (≥3 times/week) | Insomnia symptoms a | Woke up feeling unrested (≥3 days/week) | Sleep medication (≥3 times/week) |
| Women | ||||||||
| NH-White 18–30 | 1.15 (0.91, 1.46) | 1.07 (0.95, 1.20) | 1.02 (0.70, 1.50) | 1.21 (1.07, 1.38) | 1.3 (1.15, 1.49) | 1.23 (1.11, 1.36) | 1.26 (1.16, 1.36) | 1.31 (1.01, 1.71) |
| NH-White 31–49 | 1.39 (1.21, 1.61) | 1.19 (1.11, 1.28) | 1.24 (0.89, 1.73) | 1.19 (1.09, 1.30) | 1.26 (1.17, 1.35) | 1.21 (1.14, 1.29) | 1.16 (1.11, 1.21) | 1.03 (0.89, 1.20) |
| NH-White ≥50 | 1.40 (1.25, 1.56) | 1.28 (1.21, 1.35) | 1.04 (0.88, 1.23) | 1.35 (1.27, 1.43) | 1.22 (1.17, 1.28) | 1.23 (1.18, 1.28) | 1.30 (1.25, 1.36) | 1.08 (0.99, 1.18) |
| NH-Black 18–30 | 1.79 (1.15, 2.79) | 1.29 (1.06, 1.58) | 0.64 (0.34, 1.19) | 1.29 (0.95, 1.75) | 0.94 (0.70, 1.26) | 1.22 (0.96, 1.56) | 1.23 (1.03, 1.46) | 0.90 (0.40, 2.03) |
| NH-Black 31–49 | 1.37 (1.03, 1.83) | 1.16 (1.01, 1.33) | 1.37 (0.71, 2.63) | 1.18 (0.95, 1.45) | 1.21 (1.00, 1.47) | 1.18 (0.99, 1.40) | 1.28 (1.14, 1.43) | 1.01 (0.70, 1.46) |
| NH-Black ≥50 | 1.01 (0.83, 1.24) | 1.00 (0.89, 1.11) | 1.16 (0.84, 1.60) | 1.26 (1.06, 1.48) | 1.17 (1.02, 1.34) | 1.20 (1.07, 1.36) | 1.18 (1.06, 1.33) | 1.26 (0.98, 1.63) |
| Latinx 18–30 | 1.36 (0.84, 2.19) | 1.31 (1.02, 1.69) | 0.89 (0.48, 1.64) | 1.42 (1.03, 1.94) | 1.34 (0.99, 1.83) | 1.37 (1.06, 1.78) | 1.24 (1.08, 1.43) | 5.51 (2.02, 15.03) |
| Latinx 31–49 | 1.53 (1.13, 2.06) | 1.34 (1.16, 1.55) | 1.05 (0.54, 2.05) | 1.25 (1.04, 1.50) | 1.31 (1.08, 1.60) | 1.26 (1.07, 1.47) | 1.30 (1.17, 1.44) | 0.95 (0.64, 1.42) |
| Latinx ≥ 50 | 1.53 (1.19, 1.97) | 1.35 (1.16, 1.57) | 0.97 (0.60, 1.55) | 1.29 (1.07, 1.56) | 1.24 (1.05, 1.47) | 1.26 (1.08, 1.45) | 1.40 (1.24, 1.59) | 1.28 (0.95, 1.74) |
| Asian 18–30 | 1.57 (0.57, 4.31) | 1.24 (0.84, 1.84) | NE | NE | NE | NE | 1.37 (1.04, 1.81) | NE |
| Asian 31–49 | 1.60 (0.94, 2.72) | 1.29 (1.02, 1.62) | NE | 1.60 (1.03, 2.48) | 2.20 (1.45, 3.34) | 2.09 (1.49, 2.94) | 1.25 (1.04, 1.51) | 0.92 (0.39, 2.19) |
| Asian ≥50 | 1.81 (1.15, 2.85) | 1.17 (0.96, 1.44) | 1.09 (0.49, 2.41) | 1.00 (0.71, 1.42) | 1.00 (0.75, 1.31) | 1.04 (0.81, 1.32) | 1.40 (1.12, 1.74) | 1.16 (0.57, 2.37) |
| Men | ||||||||
| NH-White 18–30 | 1.02 (0.80, 1.30) | 1.11 (0.99, 1.26) | 1.11 (0.65, 1.91) | 1.39 (1.16, 1.65) | 1.50 (1.22, 1.83) | 1.42 (1.22, 1.64) | 1.24 (1.12, 1.36) | 1.68 (1.15, 2.44) |
| NH-White 31–49 | 1.16 (0.99, 1.36) | 1.16 (1.08, 1.25) | 1.19 (0.72, 1.95) | 1.24 (1.11, 1.39) | 1.16 (1.05, 1.28) | 1.22 (1.13, 1.33) | 1.27 (1.20, 1.34) | 1.09 (0.90, 1.34) |
| NH-White ≥50 | 1.48 (1.28, 1.70) | 1.18 (1.10, 1.26) | 0.82 (0.69, 0.97) | 1.29 (1.18, 1.40) | 1.27 (1.20, 1.35) | 1.26 (1.20, 1.34) | 1.40 (1.33, 1.48) | 1.12 (1.00, 1.26) |
| NH-Black 18–30 | 1.70 (0.99, 2.91) | 1.61 (1.19, 2.17) | 2.14 (0.80, 5.77) | 3.77 (1.97, 7.22) | 3.16 (1.83, 5.47) | 2.61 (1.59, 4.31) | 1.48 (1.08, 2.02) | 1.17 (0.36, 3.83) |
| NH-Black 31–49 | 0.81 (0.58, 1.12) | 1.05 (0.90, 1.22) | 0.56 (0.27, 1.17) | 1.40 (0.99, 1.98) | 1.11 (0.85, 1.46) | 1.19 (0.93, 1.53) | 1.32 (1.11, 1.57) | 1.33 (0.67, 2.64) |
| NH-Black ≥50 | 1.00 (0.78, 1.28) | 1.08 (0.94, 1.23) | 1.08 (0.76, 1.54) | 1.37 (1.08, 1.72) | 1.14 (0.94, 1.37) | 1.18 (1.00, 1.40) | 1.30 (1.11, 1.51) | 1.31 (0.92, 1.85) |
| Latinx 18–30 | 1.23 (0.69, 2.19) | 1.13 (0.87, 1.46) | 1.73 (0.79, 3.78) | 1.45 (0.99, 2.13) | 1.54 (0.98, 2.44) | 1.49 (1.06, 2.09) | 1.26 (1.05, 1.51) | 1.74 (0.54, 5.60) |
| Latinx 31–49 | 1.04 (0.74, 1.45) | 1.13 (0.97, 1.32) | 0.94 (0.49, 1.79) | 1.40 (1.07, 1.84) | 1.23 (0.95, 1.60) | 1.41 (1.13, 1.74) | 1.19 (1.05, 1.34) | 0.57 (0.34, 0.96) |
| Latinx ≥50 | 1.06 (0.76, 1.47) | 1.07 (0.91, 1.27) | 0.82 (0.50, 1.36) | 1.22 (0.98, 1.50) | 1.07 (0.86, 1.34) | 1.21 (1.01, 1.45) | 1.22 (1.05, 1.42) | 1.24 (0.86, 1.79) |
| Asian 18–30 | NE | 1.14 (0.77, 1.67) | NE | 1.37 (0.70, 2.66) | NE | 1.45 (0.77, 2.71) | 1.47 (1.07, 2.01) | NE |
| Asian 31–49 | 0.57 (0.30, 1.11) | 1.05 (0.81, 1.37) | NE | 1.19 (0.68, 2.08) | 1.43 (0.85, 2.39) | 1.33 (0.85, 2.07) | 1.40 (1.11, 1.76) | NE |
| Asian ≥50 | 1.17 (0.72, 1.91) | 1.31 (1.04, 1.66) | NE | 1.57 (0.94, 2.61) | 1.74 (1.16, 2.63) | 1.51 (1.05, 2.17) | 1.42 (0.99, 1.63) | 1.08 (0.52, 2.24) |
| Medium Neighborhood Social Cohesion | Very short <6 vs. 7–9 h | Short <7 vs. 7–9 h | Long >9 vs. 7–9 h | Trouble falling asleep (≥3 times/week) | Trouble staying asleep (≥3 times/week) | Insomnia symptoms a | Woke up feeling unrested (≥3 days/week) | Sleep medication (≥3 times/week) |
| Women | ||||||||
| NH-White 18–30 | 0.95 (0.73, 1.24) | 1.01 (0.90, 1.14) | 0.81 (0.52, 1.25) | 1.11 (0.98, 1.27) | 1.18 (1.03, 1.35) | 1.17 (1.05, 1.30) | 1.16 (1.07, 1.25) | 0.77 (0.57, 1.04) |
| NH-White 31–49 | 1.03 (0.87, 1.22) | 1.05 (0.97, 1.13) | 0.91 (0.64, 1.31) | 1.06 (0.97, 1.15) | 1.17 (1.09, 1.26) | 1.14 (1.07, 1.22) | 1.08 (1.03, 1.13) | 0.96 (0.83, 1.12) |
| NH-White ≥50 | 0.99 (0.87, 1.11) | 1.11 (1.05, 1.18) | 0.86 (0.74, 0.99) | 1.14 (1.07, 1.21) | 1.08 (1.03, 1.13) | 1.08 (1.04, 1.12) | 1.12 (1.07, 1.17) | 0.97 (0.90, 1.05) |
| NH-Black 18–30 | 1.54 (0.89, 2.64) | 1.27 (1.00, 1.60) | 0.90 (0.48, 1.70) | 1.15 (0.79, 1.67) | 0.88 (0.62, 1.26) | 1.10 (0.81, 1.49) | 1.07 (0.88, 1.31) | 0.76 (0.31, 1.87) |
| NH-Black 31–49 | 1.06 (0.78, 1.44) | 1.02 (0.89, 1.18) | 1.25 (0.62, 2.51) | 0.94 (0.73, 1.20) | 0.97 (0.79, 1.19) | 0.96 (0.80, 1.16) | 1.15 (1.01, 1.30) | 0.88 (0.59, 1.31) |
| NH-Black ≥50 | 0.80 (0.64, 1.01) | 0.90 (0.80, 1.00) | 1.14 (0.86, 1.53) | 1.11 (0.94, 1.30) | 1.06 (0.92, 1.21) | 1.07 (0.94, 1.20) | 1.07 (0.96, 1.19) | 1.27 (0.98, 1.63) |
| Latinx 18–30 | 1.04 (0.62, 1.76) | 1.14 (0.86, 1.51) | 0.81 (0.41, 1.61) | 0.95 (0.68, 1.35) | 0.95 (0.67, 1.34) | 1.01 (0.76, 1.34) | 1.07 (0.91, 1.26) | 2.94 (1.03, 8.40) |
| Latinx 31–49 | 1.15 (0.81, 1.63) | 1.16 (0.99, 1.36) | 0.75 (0.37, 1.50) | 1.08 (0.88, 1.33) | 1.15 (0.93, 1.42) | 1.10 (0.93, 1.31) | 1.19 (1.06, 1.33) | 0.66 (0.43, 1.01) |
| Latinx ≥50 | 1.05 (0.79, 1.40) | 1.12 (0.95, 1.32) | 0.69 (0.38, 1.23) | 1.12 (0.91, 1.38) | 1.08 (0.90, 1.31) | 1.11 (0.94, 1.31) | 1.34 (1.18, 1.54) | 1.26 (0.93, 1.70) |
| Asian 18–30 | 1.44 (0.53, 3.94) | 0.75 (0.48, 1.17) | NE | NE | NE | NE | 1.03 (0.78, 1.37) | NE |
| Asian 31–49 | 0.65 (0.36, 1.16) | 1.04 (0.81, 1.33) | NE | 1.24 (0.81, 1.91) | 1.27 (0.82, 1.95) | 1.27 (0.90, 1.78) | 1.02 (0.85, 1.21) | 0.46 (0.21, 1.01) |
| Asian ≥50 | 1.12 (0.71, 1.78) | 0.89 (0.73, 1.10) | 0.70 (0.34, 1.42) | 0.86 (0.60, 1.22) | 0.77 (0.56, 1.07) | 0.78 (0.60, 1.02) | 1.03 (0.83, 1.28) | 1.22 (0.66, 2.25) |
| Men | ||||||||
| NH-White 18–30 | 0.75 (0.56, 1.00) | 1.04 (0.92, 1.17) | 1.47 (0.89, 2.41) | 1.07 (0.88, 1.31) | 1.22 (0.97, 1.54) | 1.10 (0.92, 1.30) | 1.11 (1.00, 1.23) | 1.37 (0.90, 2.09) |
| NH-White 31–49 | 1.15 (0.98, 1.34) | 1.07 (1.00, 1.14) | 1.50 (0.93, 2.41) | 1.20 (1.07, 1.35) | 1.10 (0.99, 1.21) | 1.11 (1.02, 1.20) | 1.14 (1.08, 1.21) | 1.34 (1.11, 1.61) |
| NH-White ≥50 | 1.18 (1.03, 1.35) | 1.07 (1.00, 1.14) | 0.90 (0.77, 1.05) | 1.11 (1.01, 1.21) | 1.12 (1.06, 1.19) | 1.11 (1.06, 1.17) | 1.24 (1.18, 1.30) | 1.04 (0.93, 1.16) |
| NH-Black 18–30 | 1.28 (0.71, 2.31) | 1.28 (0.93, 1.77) | 1.49 (0.42, 5.34) | 2.82 (1.43, 5.58) | 2.35 (1.28, 4.31) | 2.04 (1.19, 3.50) | 1.29 (0.94, 1.77) | 0.40 (0.08, 1.94) |
| NH-Black 31–49 | 0.94 (0.68, 1.31) | 1.03 (0.89, 1.20) | 0.36 (0.16, 0.78) | 1.15 (0.81, 1.64) | 0.84 (0.64, 1.10) | 0.92 (0.72, 1.19) | 1.23 (1.04, 1.46) | 0.99 (0.50, 1.97) |
| NH-Black ≥50 | 0.83 (0.63, 1.09) | 1.03 (0.90, 1.17) | 0.80 (0.57, 1.13) | 1.39 (1.10, 1.77) | 1.19 (1.00, 1.42) | 1.19 (1.01, 1.40) | 1.22 (1.05, 1.41) | 0.89 (0.61, 1.31) |
| Latinx 18–30 | 1.22 (0.68, 2.22) | 1.09 (0.83, 1.42) | 1.39 (0.61, 3.19) | 1.20 (0.81, 1.79) | 1.18 (0.74, 1.88) | 1.27 (0.90, 1.80) | 1.10 (0.91, 1.33) | 2.55 (0.96, 6.76) |
| Latinx 31–49 | 0.91 (0.64, 1.28) | 1.08 (0.92, 1.26) | 0.38 (0.18, 0.82) | 1.07 (0.80, 1.43) | 0.85 (0.63, 1.15) | 1.02 (0.80, 1.31) | 1.03 (0.89, 1.18) | 0.32 (0.17, 0.60) |
| Latinx ≥50 | 0.77 (0.55, 1.09) | 0.91 (0.76, 1.08) | 0.76 (0.47, 1.21) | 0.83 (0.64, 1.07) | 0.94 (0.75, 1.17) | 0.94 (0.76, 1.15) | 1.01 (0.85, 1.20) | 0.88 (0.60, 1.29) |
| Asian 18–30 | NE | 0.73 (0.48, 1.11) | NE | 0.73 (0.35, 1.52) | NE | 0.68 (0.33, 1.38) | 1.13 (0.81, 1.58) | NE |
| Asian 31–49 | 0.84 (0.44, 1.61) | 0.92 (0.72, 1.17) | NE | 1.16 (0.67, 2.02) | 0.78 (0.49, 1.26) | 1.00 (0.66, 1.52) | 1.29 (1.04, 1.61) | NE |
| Asian ≥50 | 1.28 (0.77, 2.13) | 1.31 (1.05, 1.62) | NE | 1.22 (0.73, 2.04) | 1.64 (1.08, 2.49) | 1.34 (0.92, 1.96) | 1.27 (0.99, 1.63) | 1.15 (0.56, 2.33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhasan, D.M.; Gaston, S.A.; Jackson, W.B., II; Williams, P.C.; Kawachi, I.; Jackson, C.L. Neighborhood Social Cohesion and Sleep Health by Age, Sex/Gender, and Race/Ethnicity in the United States. Int. J. Environ. Res. Public Health 2020, 17, 9475. https://doi.org/10.3390/ijerph17249475
Alhasan DM, Gaston SA, Jackson WB II, Williams PC, Kawachi I, Jackson CL. Neighborhood Social Cohesion and Sleep Health by Age, Sex/Gender, and Race/Ethnicity in the United States. International Journal of Environmental Research and Public Health. 2020; 17(24):9475. https://doi.org/10.3390/ijerph17249475
Chicago/Turabian StyleAlhasan, Dana M., Symielle A. Gaston, W. Braxton Jackson, II, Patrice C. Williams, Ichiro Kawachi, and Chandra L. Jackson. 2020. "Neighborhood Social Cohesion and Sleep Health by Age, Sex/Gender, and Race/Ethnicity in the United States" International Journal of Environmental Research and Public Health 17, no. 24: 9475. https://doi.org/10.3390/ijerph17249475
APA StyleAlhasan, D. M., Gaston, S. A., Jackson, W. B., II, Williams, P. C., Kawachi, I., & Jackson, C. L. (2020). Neighborhood Social Cohesion and Sleep Health by Age, Sex/Gender, and Race/Ethnicity in the United States. International Journal of Environmental Research and Public Health, 17(24), 9475. https://doi.org/10.3390/ijerph17249475