Application and Perceived Effectiveness of Complementary and Alternative Intervention Strategies for Attention-Deficit/Hyperactivity Disorder: Relationships with Affiliate Stigma



Abstract
:1. Introduction
1.1. Necessity of Treatment for Attention-Deficit/Hyperactivity Disorder
1.2. Complementary and Alternative Intervention Strategies (CAIS) for ADHD
1.3. Role of Affiliate Stigma for the Treatment of ADHD
1.4. Aims of the Present Study
2. Methods
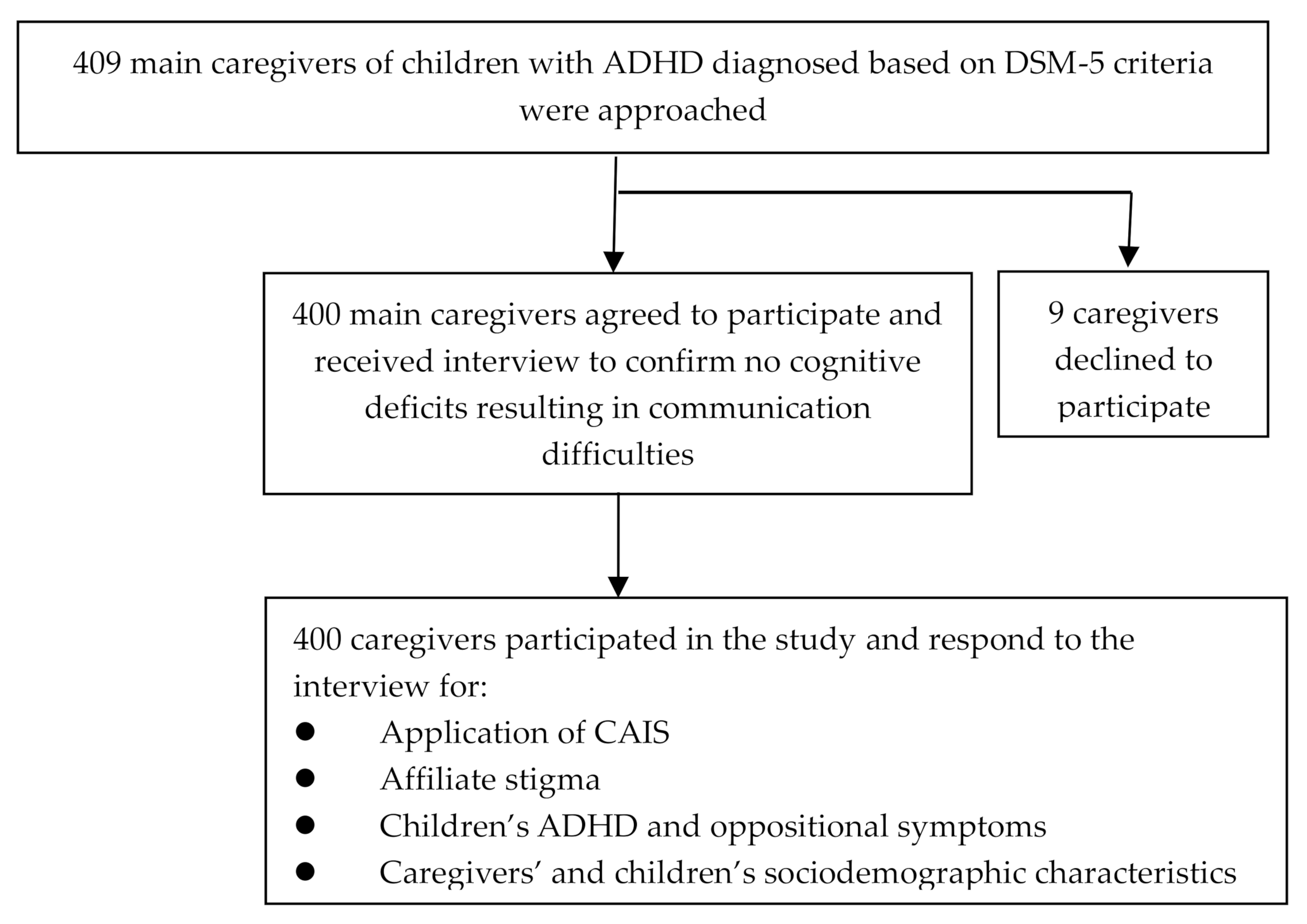
2.1. Participants and Procedure
2.2. Measures
2.2.1. CAIS for ADHD
2.2.2. Caregivers’ and Children’s Factors
2.3. Procedure and Statistical Analysis
2.4. Ethics
3. Results
3.1. Employment and Effectiveness of CAIS
3.2. Affiliate Stigma and Application of CAIS
3.3. Affiliate Stigma and Effectiveness of CAIS
3.4. Current Psychiatric Treatment, CAIS, and Affiliate Stigma
4. Discussion
4.1. Affiliate Stigma and Employment of CAIS
4.2. Affiliate Stigma and the Effectiveness of CAIS
4.3. Current Psychiatric Treatment, CAIS, and Affiliate Stigma
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Chen, Y.L.; Chen, W.J.; Lin, K.C.; Shen, L.J.; Gau, S.S. Prevalence of DSM-5 mental disorders in a nationally representative sample of children in Taiwan: Methodology and main findings. Epidemiol. Psychiatr. Sci. 2019, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R. Attention Deficit Hyperactivity Disorder; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Huang, K.L.; Wei, H.T.; Hsu, J.W.; Bai, Y.M.; Su, T.P.; Li, C.T.; Lin, W.C.; Tsai, S.J.; Chang, W.H.; Chen, T.J.; et al. Risk of suicide attempts in adolescents and young adults with attention-deficit hyperactivity disorder: A nationwide longitudinal study. Br. J. Psychiatry 2018, 212, 234–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liou, Y.J.; Wei, H.T.; Chen, M.H.; Hsu, J.W.; Huang, K.L.; Bai, Y.M.; Su, T.P.; Li, C.T.; Yang, A.C.; Tsai, S.J.; et al. Risk of traumatic brain injury among children, adolescents, and young adults with attention-deficit hyperactivity disorder in Taiwan. J. Adolesc. Health 2018, 63, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.W.; Lin, C.L.; Lin, C.W.; Huang, M.T.; Chang, W.L.; Lu, T.H.; Lin, C.J. Fracture risk and correlating factors of a pediatric population with attention deficit hyperactivity disorder: A nationwide matched study. J. Pediatr. Orthop. B 2016, 25, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.H.; Hsu, J.W.; Huang, K.L.; Bai, Y.M.; Ko, N.Y.; Su, T.P.; Li, C.T.; Lin, W.C.; Tsai, S.J.; Pan, T.L.; et al. Sexually transmitted infection among adolescents and young adults with attention-deficit/hyperactivity disorder: A nationwide longitudinal study. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 48–53. [Google Scholar] [CrossRef]
- Lee, M.J.; Yang, K.C.; Shyu, Y.C.; Yuan, S.S.; Yang, C.J.; Lee, S.Y.; Lee, T.L.; Wang, L.J. Attention-deficit hyperactivity disorder, its treatment with medication and the probability of developing a depressive disorder: A nationwide population-based study in Taiwan. J. Affect. Disord. 2016, 189, 110–117. [Google Scholar] [CrossRef]
- Zulauf, C.A.; Sprich, S.E.; Safren, S.A.; Wilens, T.E. The complicated relationship between attention deficit/hyperactivity disorder and substance use disorders. Curr. Psychiatry Rep. 2014, 16, 436. [Google Scholar] [CrossRef]
- Charach, A.; Dashti, B.; Carson, P.; Booker, L.; Lim, C.G.; Lillie, E.; Yeung, E.; Ma, J.; Raina, P.; Schachar, R. Attention Deficit Hyperactivity Disorder: Effectiveness of Treatment in At-rRisk Preschoolers; Long-Term Effectiveness in all, aAges and Variability in Prevalence, Diagnosis, and Treatment; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011; Available online: https://www.ncbi.nlm.nih.gov/books/NBK82368/ (accessed on 23 December 2019).
- Goode, A.P.; Coeytaux, R.R.; Maslow, G.R.; Davis, N.; Hill, S.; Namdari, B.; LaPointe, N.M.A.; Befus, D.; Lallinger, K.R.; Bowen, S.E.; et al. Nonpharmacologic treatments for attention-deficit/hyperactivity disorder: A systematic review. Pediatrics 2018, 141, e20180094. [Google Scholar] [CrossRef] [Green Version]
- Schatz, N.K.; Fabiano, G.A.; Cunningham, C.E.; dosReis, S.; Waschbusch, D.A.; Jerome, S.; Lupas, K.; Morris, K.L. Systematic review of patients’ and parents’ preferences for ADHD treatment options and processes of care. Patient 2015, 8, 483–497. [Google Scholar] [CrossRef]
- Bussing, R.; Zima, B.T.; Gary, F.A.; Garvan, C.W. Use of complementary and alternative medicine for symptoms of attention-deficit hyperactivity disorder. Psychiatr. Serv. 2002, 53, 1096–1102. [Google Scholar] [CrossRef]
- National Center for Complementary and Integrative Health. Complementary, Alternative, or Integrative Health: What’s In a Name? Available online: https://nccih.nih.gov/health/integrative-health#hed1 (accessed on 31 January 2020).
- Section On Complementary And Integrative Medicine; Council on Children with Disabilities; American Academy of Pediatrics; Zimmer, M.; Desch, L. Sensory integration therapies for children with developmental and behavioral disorders. Pediatrics 2012, 129, 1186–1189. [Google Scholar] [CrossRef] [Green Version]
- Tzang, R.F.; Chang, Y.C.; Kao, K.L.; Huang, Y.H.; Huang, H.C.; Wang, Y.C.; Muo, C.H.; Wu, S.I.; Sung, F.C.; Stewart, R. Increased risk of developing psychiatric disorders in children with attention deficit and hyperactivity disorder (ADHD) receiving sensory integration therapy: A population-based cohort study. Eur. Child Adolesc. Psychiatry 2019, 28, 247–255. [Google Scholar] [CrossRef]
- Colvin, M.K.; Stern, T.A. Diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2015, 76, e1148. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Massachusetts, MA, USA, 1979. [Google Scholar]
- Mueller, A.K.; Fuermaier, A.B.M.; Koerts, J.; Tucha, L. Stigma in attention deficit hyperactivity disorder. ADHD Atten. Def. Hyperact. Disord. 2012, 4, 101–114. [Google Scholar] [CrossRef] [Green Version]
- Sciutto, M.J. ADHD knowledge, misconceptions, and treatment acceptability. J. Atten. Disord. 2015, 19, 91–98. [Google Scholar] [CrossRef]
- Johnston, C.; Seipp, C.; Hommersen, P.; Hoza, B.; Fine, S. Treatment choices and experiences in attention deficit and hyperactivity disorder: Relations to parents’ beliefs and attributions. Child Care Health Dev. 2005, 31, 669–677. [Google Scholar] [CrossRef]
- Mak, W.W.; Cheung, R.Y.M. Affiliate stigma among caregivers of people with intellectual disability or mental illness. J. Appl. Res. Intellect. Disabil. 2008, 21, 532–545. [Google Scholar] [CrossRef]
- Mikami, A.Y.; Chong, G.K.; Saporito, J.M.; Na, J.J. Implications of parental affiliate stigma in families of children with ADHD. J. Clin. Child Adolesc. Psychol. 2015, 44, 595–603. [Google Scholar] [CrossRef] [Green Version]
- Charbonnier, E.; Caparos, S.; Trémolière, B. The role of mothers’ affiliate stigma and child’s symptoms on the distress of mothers with ADHD children. J. Ment. Health 2019, 28, 282–288. [Google Scholar] [CrossRef]
- Triandis, H.C. Individualism-collectivism and personality. J. Personal. 2001, 69, 907–924. [Google Scholar] [CrossRef]
- Han, K.H. The feeling of “face” in Confucian society: From a perspective of psychosocial equilibrium. Front. Psychol. 2016, 7, 1055. [Google Scholar] [CrossRef] [Green Version]
- Gau, S.S.; Shang, C.Y.; Liu, S.K. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, version IV scale-parent form. Int. J. Methods Psychiatr. Res. 2008, 17, 35–44. [Google Scholar] [CrossRef]
- Swanson, J.M.; Kraemer, H.C.; Hinshaw, S.P.; Arnold, L.E.; Conners, C.K.; Abikoff, H.B.; Clevenger, W.; Davies, M.; Elliott, G.R.; Greenhill, L.L.; et al. Clinical relevance of the primary findings of the MTA: Success rates based on severity of ADHD and ODD symptoms at the end of treatment. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 168–179. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, F.Y. Sample size tables for logistic regression. Stat. Med. 1989, 8, 795–802. [Google Scholar] [CrossRef]
- Chang, C.C.; Su, J.A.; Tsai, C.S.; Yen, C.F.; Liu, J.H.; Lin, C.Y. Rasch analysis suggested three unidimensional domains for Affiliate Stigma Scale: Additional psychometric evaluation. J. Clin. Epidemiol. 2015, 68, 674–683. [Google Scholar] [CrossRef]
- Hwang, Y.J. An analysis of the reliability and validity of the close-ended questionnaire of the occupational survey in the educational research. Bull. Educ. Res. 2005, 51, 43–71. [Google Scholar]
- Liu, Y.C.; Liu, S.K.; Shang, C.Y.; Lin, C.H.; Tu, C.L.; Gau, S.S. Norm of the Chinese Version of the Swanson, Nolan and Pelham, Version IV Scale for ADHD. Taiwan. J. Psychiatry (Taipei) 2006, 20, 290–304. [Google Scholar] [CrossRef]
- Bussing, R.; Gary, F.A.; Mills, T.L.; Garvan, C.W. Parental explanatory models of ADHD: Gender and cultural variations. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 563–575. [Google Scholar] [CrossRef]
- Bussing, R.; Meyer, J.; Zima, B.T.; Mason, D.M.; Gary, F.A.; Garvan, C.W. Childhood ADHD symptoms: Association with parental social networks and mental health service use during adolescence. Int. J. Environ. Res. Public Health 2015, 12, 11893–11909. [Google Scholar] [CrossRef] [Green Version]
- DosReis, S.; Barksdale, C.L.; Sherman, A.; Maloney, K.; Charach, A. Stigmatizing experiences of parents of children with a new diagnosis of ADHD. Psychiatr. Serv. 2010, 61, 811–816. [Google Scholar] [CrossRef]
- Koro-Ljungberg, M.; Bussing, R. The management of courtesy stigma in the lives of families with teenagers with ADHD. J. Fam. Issues 2009, 30, 1175–1200. [Google Scholar] [CrossRef]
- Fegert, J.M.; Slawik, L.; Wermelskirchen, D.; Nübling, M.; Mühlbacher, A. Assessment of parents’ preferences for the treatment of school-age children with ADHD: A discrete choice experiment. Expert Rev. Pharm. Outcomes Res. 2011, 11, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Szumilas, M. Explaining odds ratios. Can. Acad. Child Adolesc. Psychiatry 2010, 19, 227–229. [Google Scholar]
- Wang, L.J.; Lee, S.Y.; Yuan, S.S.; Yang, C.J.; Yang, K.C.; Huang, T.S.; Chou, W.J.; Chou, M.C.; Lee, M.J.; Lee, T.L.; et al. Prevalence rates of youths diagnosed with and medicated for ADHD in a nationwide survey in Taiwan from 2000 to 2011. Epidemiol. Psychiatr. Sci. 2017, 26, 624–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, E.S.F.; Ma, J.L.C.; Lai, K.Y.C.; Lo, J.W.K. The subjective experiences of attention-deficit/hyperactivity disorder of Chinese families in Hong Kong: Co-construction of meanings in multiple family groups. Health Soc. Work 2016, 41, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Singh, I.; Filipe, A.M.; Bard, I.; Bergey, M.; Baker, L. Globalization and cognitive enhancement: Emerging social and ethical challenges for ADHD clinicians. Curr. Psychiatry Rep. 2013, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bussing, R.; Zima, B.T.; Mason, D.M.; Meyer, J.M.; White, K.; Garvan, C.W. ADHD knowledge, perceptions, and information sources: Perspectives from a community sample of adolescents and their parents. J. Adolesc. Health 2012, 51, 593–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | n (%) | Mean (SD) | Range |
|---|---|---|---|
| Caregivers | |||
| Relationship with the child | |||
| Mother | 287 (71.8) | ||
| Father | 90 (22.5) | ||
| Others | 23 (5.8) | ||
| Age (years) | 43.4 (6.8) | 25–70 | |
| Sex | |||
| Female | 304 (76.0) | ||
| Male | 96 (24.0) | ||
| Education (years) | 13.8 (2.9) | 3–23 | |
| Parental marriage status | |||
| Intact | 320 (80) | ||
| Disruptive | 80 (20) | ||
| Occupational socioeconomic status | |||
| High | 155 (38.8) | ||
| Low | 245 (61.2) | ||
| Affiliate stigma | 38.7 (11.3) | 22–75 | |
| Children | |||
| Age (years) | 10.7 (3.2) | 4–18 | |
| Sex | |||
| Girls | 64 (16.0) | ||
| Boys | 336 (84.0) | ||
| Education | |||
| Primary school or kindergarten | 355 (88.8) | ||
| High school | 45 (11.3) | ||
| ADHD symptoms on the SNAP-IV | |||
| Inattention | 13.4 (3.6) | 0–27 | |
| Hyperactivity/impulsivity | 9.8 (6.0) | 0–27 | |
| Opposition defiance | 10.1 (6.0) | 0–24 |
| Variables | n (%) | Age of Children at the First Visit (Years) Mean (SD) | Effect | |
|---|---|---|---|---|
| No Effect n (%) | Have Effect n (%) | |||
| Sensory integration | 121 (30.3) | 5.3 (2.3) | 35 (28.9) | 86 (71.1) |
| Exercise training | 117 (29.3) | 6.5 (2.6) | 23 (19.7) | 94 (80.3) |
| Sugar restriction | 82 (20.5) | 6.0 (2.3) | 26 (31.7) | 56 (68.3) |
| Omega fatty acids supplement | 45 (11.3) | 7.1 (3.5) | 28 (62.2) | 17 (37.8) |
| Treatment for allergy | 35 (8.8) | 6.7 (2.9) | 19 (54.3) | 16 (45.7) |
| Music therapy | 32 (8.0) | 6.5 (2.9) | 10 (31.3) | 22 (68.7) |
| Chinese herbal medicine | 21 (5.3) | 7.9 (3.3) | 12 (57.1) | 9 (42.9) |
| Meditation or mindfulness | 10 (2.5) | 7.2 (3.6) | 1 (10) | 9 (90) |
| Chiropractic | 10 (2.5) | 5.9 (3.1) | 2 (20) | 8 (80) |
| Acupuncture | 9 (2.3) | 7.0 (3.9) | 4 (44.4) | 5 (55.6) |
| Homeopathy | 9 (2.3) | 5.1 (3.1) | 5 (55.6) | 4 (44.4) |
| Folk therapy | 7 (1.8) | 5.4 (4.0) | 2 (28.6) | 5 (71.4) |
| Mind growth programs by religious groups | 7 (1.8) | 7.0 (4.3) | 2 (28.6) | 5 (71.4) |
| Neurofeedback | 1 (0.3) | 10 (n/a) | 0 | 1 (100) |
| Chelating agent for removing heavy metals | 1 (0.3) | 3 (n/a) | 1 (100) | 0 |
| Variables | Sensory Integration | Exercise Training | Sugar Restriction | Omega Fatty Acids Supplement | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Caregivers | ||||||||
| Males a | 0.405 (0.220–0.746) | 0.004 | 0.703 (0.401–1.235) | 0.221 | 0.440 (0.215–0.902) | 0.025 | 0.432 (0.160–1.168) | 0.098 |
| Age | 0.987 (0.953–1.023) | 0.485 | 0.986 (0.952–1.021) | 0.424 | 0.986 (0.944–1.029) | 0.516 | 0.976 (0.923–1.031) | 0.387 |
| Education level | 1.072 (0.985–1.167) | 0.108 | 1.036 (0.952–1.126) | 0.412 | 1.100 (0.998–1.211) | 0.054 | 1.034 (0.914–1.170) | 0.592 |
| Disruptive marriage status b | 0.897 (0.512–1.574) | 0.706 | 1.046 (0.603–1.815) | 0.873 | 0.586 (0.289–1.187) | 0.138 | 0.496 (0.187–1.317) | 0.159 |
| Low occupational SES c | 0.878 (0.537–1.436) | 0.605 | 1.207 (0.734–1.984) | 0.458 | 0.701 (0.404–1.218) | 0.207 | 1.038 (0.506–2.132) | 0.918 |
| Affiliate stigma | 1.020 (1.000–1.040) | 0.049 | 1.023 (1.003–1.043) | 0.022 | 1.015 (0.993–1.038) | 0.184 | 1.042 (1.013–1.071) | 0.004 |
| Children | ||||||||
| Boys d | 1.405 (0.749–2.634) | 0.290 | 0.926 (0.512–1.675) | 0.799 | 0.790 (0.410–1.524) | 0.483 | 1.700 (0.664–4.354) | 0.269 |
| Variables | Sensory Integration | Exercise Training | Sugar Restriction | Omega Fatty Acids Supplement | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Caregivers | ||||||||
| Males a | 1.077 (0.297–3.897) | 0.911 | 0.520 (0.141–1.916) | 0.326 | 1.304 (0.287–5.928) | 0.731 | 0.105 (0.007–1.632) | 0.107 |
| Age | 0.930 (0.864–1.002) | 0.055 | 0.944 (0.876–1.017) | 0.131 | 0.982 (0.911–1.058) | 0.634 | 0.922 (0.789–1.079) | 0.311 |
| Education level | 1.093 (0.925–1.291) | 0.296 | 1.107 (0.919–1.332) | 0.285 | 1.010 (0.843–1.210) | 0.915 | 0.758 (0.516–1.114) | 0.158 |
| Disruptive marriage status b | 0.994 (0.300–3.288) | 0.992 | 3.054 (0.608–15.336) | 0.175 | 1.074 (0.243–4.744) | 0.925 | 7.863 (0.260–237.923) | 0.236 |
| Low occupational SES c | 0.679 (0.262–1.761) | 0.426 | 0.546 (0.153–1.946) | 0.350 | 0.567 (0.199–1.617) | 0.288 | 0.690 (0.1144–0.169) | 0.686 |
| Affiliate stigma | 0.945 (0.908–0.984) | 0.006 | 0.955 (0.913–0.999) | 0.043 | 0.976 (0.936–1.018) | 0.261 | 0.909 (0.844–0.980) | 0.013 |
| Children | ||||||||
| Boys d | 0.170 (0.031–0.939) | 0.042 | 1.829 (0.526–6.358) | 0.342 | 1.356 (0.401–4.586) | 0.624 | 0.284 (0.023–3.527) | 0.327 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, W.-J.; Liu, T.-L.; Hsiao, R.C.; Chen, Y.-M.; Chang, C.-C.; Yen, C.-F. Application and Perceived Effectiveness of Complementary and Alternative Intervention Strategies for Attention-Deficit/Hyperactivity Disorder: Relationships with Affiliate Stigma. Int. J. Environ. Res. Public Health 2020, 17, 1505. https://doi.org/10.3390/ijerph17051505
Chou W-J, Liu T-L, Hsiao RC, Chen Y-M, Chang C-C, Yen C-F. Application and Perceived Effectiveness of Complementary and Alternative Intervention Strategies for Attention-Deficit/Hyperactivity Disorder: Relationships with Affiliate Stigma. International Journal of Environmental Research and Public Health. 2020; 17(5):1505. https://doi.org/10.3390/ijerph17051505
Chicago/Turabian StyleChou, Wen-Jiun, Tai-Ling Liu, Ray C. Hsiao, Yu-Min Chen, Chih-Cheng Chang, and Cheng-Fang Yen. 2020. "Application and Perceived Effectiveness of Complementary and Alternative Intervention Strategies for Attention-Deficit/Hyperactivity Disorder: Relationships with Affiliate Stigma" International Journal of Environmental Research and Public Health 17, no. 5: 1505. https://doi.org/10.3390/ijerph17051505
APA StyleChou, W. -J., Liu, T. -L., Hsiao, R. C., Chen, Y. -M., Chang, C. -C., & Yen, C. -F. (2020). Application and Perceived Effectiveness of Complementary and Alternative Intervention Strategies for Attention-Deficit/Hyperactivity Disorder: Relationships with Affiliate Stigma. International Journal of Environmental Research and Public Health, 17(5), 1505. https://doi.org/10.3390/ijerph17051505