Does Better Health-Related Knowledge Predict Favorable Health Behavior in Adolescents?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
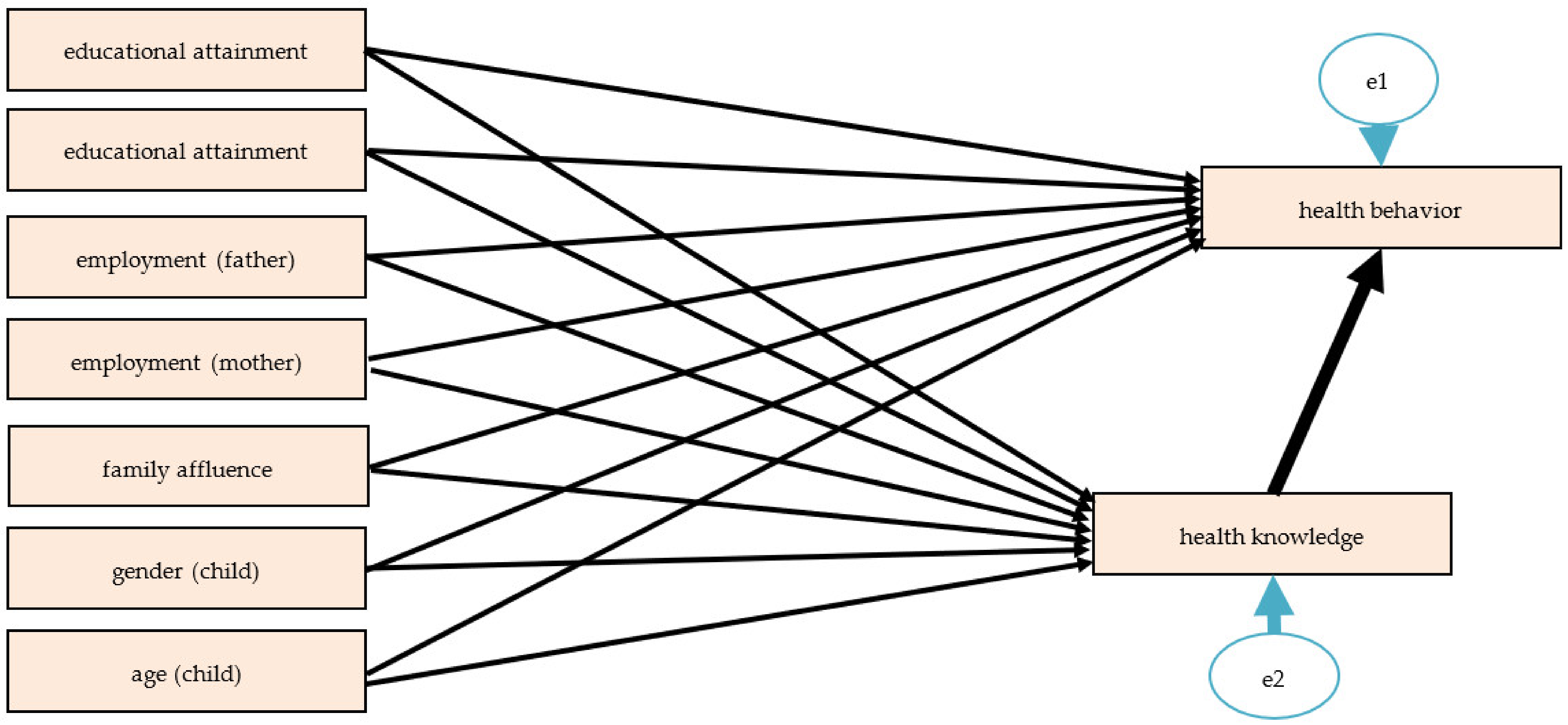
3.2. Association between Health Knowledge and Health Behavior Based upon Structural Equation Models
3.3. Models for Nutrition-Related Knowledge and Eating Habits
3.4. Models for Physical Activity-Related Knowledge and Physical Activity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dorn, L.D.; Hostinar, C.E.; Susman, E.J.; Pervanidou, P. Conceptualizing Puberty as a Window of Opportunity for Impacting Health and Well-Being Across the Life Span. J. Res. Adolesc. 2019, 29, 155–176. [Google Scholar] [CrossRef] [Green Version]
- Nutbeam, D. Health Education and Health Promotion Revisited. Health Educ. J. 2018. [Google Scholar] [CrossRef] [Green Version]
- Chung, L.M.Y.; Chung, J.W.Y.; Chan, A.P.C. Building Healthy Eating Knowledge and Behavior: An Evaluation of Nutrition Education in a Skill Training Course for Construction Apprentices. Int. J. Environ. Res. Public Health 2019, 16, 4852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Li, X.; Wang, X.; Shao, J.; Dou, J.A. Cross-Site Intervention in Chinese Rural Migrants Enhances HIV/AIDS Knowledge, Attitude and Behavior. Int. J. Environ. Res. Public Health 2014, 11, 4528–4543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Ji, H.; Chen, L.-J.; Jiang, R.; Wu, Y.-N. Food Safety Knowledge, Attitudes and Behavior among Dairy Plant Workers in Beijing, Northern China. Int. J. Environ. Res. Public Health 2018, 15, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharaibeh, H.; Haddad, L.; Alzyoud, S.; El-Shahawy, O.; Baker, N.A.; Umlauf, M. Knowledge, Attitudes, and Behavior in Avoiding Secondhand Smoke Exposure among Non-Smoking Employed Women with Higher Education in Jordan. Int. J. Environ. Res. Public Health 2011, 8, 4207–4219. [Google Scholar] [CrossRef] [PubMed]
- Knowles, S.; Lam, L.T.; McInnes, E.; Elliott, D.; Hardy, J.; Middleton, S. Knowledge, Attitudes, Beliefs and Behaviour Intentions for Three Bowel Management Practices in Intensive Care: Effects of a Targeted Protocol Implementation for Nursing and Medical Staff. BMC Nurs. 2015, 14, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, T.; Regehr, G.; Rosenfield, J.; Roberts, S.W.; Lingard, L. Exploring the Gap Between Knowledge and Behavior: A Qualitative Study of Clinician Action Following an Educational Intervention. Acad. Med. 2004, 79. [Google Scholar] [CrossRef] [Green Version]
- Németh, Á.; Költő, A. (Eds.) Health Behaviour in School-Aged Children (HBSC): A WHO-Collaborative Cross-National Study. National Report 2014; National Institute of Health Promotion: Budapest, Hungary, 2014. [Google Scholar]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C.; FAS Development Study Group. Psychometric Validation of the Revised Family Affluence Scale: A Latent Variable Approach. Child. Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef] [Green Version]
- He, Z.; Cheng, Z.; Shao, T.; Liu, C.; Shao, P.; Bishwajit, G.; Feng, D.; Feng, Z. Factors Influencing Health Knowledge and Behaviors among the Elderly in Rural China. Int. J. Environ. Res. Public Health 2016, 13, 975. [Google Scholar] [CrossRef] [Green Version]
- Fuady, A.; Pakasi, T.A.; Mansyur, M. The Social Determinants of Knowledge and Perception on Pulmonary Tuberculosis among Females in Jakarta, Indonesia. Med. J. Indones. 2014, 23. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.-H.; Yang, Y.; Gao, Y.-H.; Chen, S.-D.; Xu, Y. Status and Determinants of Health Literacy among Adolescents in Guangdong,China. Asian Pacific J. Cancer Prev. 2014, 15, 8735–8740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, R.B. Methodology in the Social Sciences, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Schmidt, C.O.; Fahland, R.A.; Franze, M.; Splieth, C.; Thyrian, J.R.; Plachta-Danielzik, S.; Hoffmann, W.; Kohlmann, T. Health-Related Behaviour, Knowledge, Attitudes, Communication and Social Status in School Children in Eastern Germany. Health Educ. Res. 2010, 25, 542–551. [Google Scholar] [CrossRef]
- Pirouznia, M. The Association between Nutrition Knowledge and Eating Behavior in Male and Female Adolescents in the US. Int. J. Food Sci. Nutr. 2001, 52, 127–132. [Google Scholar] [CrossRef]
- Mirmiran, P.; Azadbakht, L.; Azizi, F. Dietary Behaviour of Tehranian Adolescents Does Not Accord with Their Nutritional Knowledge. Public Health Nutr. 2007, 10, 897–901. [Google Scholar] [CrossRef] [Green Version]
- Tucker-Drob, E.M.; Briley, D.A. Socioeconomic Status Modifies Interest-Knowledge Associations among Adolescents. Pers. Individ. Dif. 2012, 53, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Mistretta, A.; Turconi, G.; Cena, H.; Roggi, C.; Galvano, F. Nutrition Knowledge and Other Determinants of Food Intake and Lifestyle Habits in Children and Young Adolescents Living in a Rural Area of Sicily, South Italy. Public Health Nutr. 2013, 16, 1827–1836. [Google Scholar] [CrossRef] [Green Version]
- Vaitkeviciute, R.; Ball, L.E.; Harris, N. The Relationship between Food Literacy and Dietary Intake in Adolescents: A Systematic Review. Public Health Nutr. 2015, 18, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Woods-Townsend, K.; Leat, H.; Bay, J.; Bagust, L.; Davey, H.; Lovelock, D.; Christodoulou, A.; Griffiths, J.; Grace, M.; Godfrey, K.; et al. LifeLab Southampton: A Programme to Engage Adolescents with DOHaD Concepts as a Tool for Increasing Health Literacy in Teenagers -a Pilot Cluster-Randomized Control Trial. J. Dev. Orig. Health Dis. 2018, 9, 475–480. [Google Scholar] [CrossRef] [Green Version]
- Haible, S.; Volk, C.; Demetriou, Y.; Höner, O.; Thiel, A.; Sudeck, G. Physical Activity-Related Health Competence, Physical Activity, and Physical Fitness: Analysis of Control Competence for the Self-Directed Exercise of Adolescents. Int. J. Environ. Res. Public Health 2019, 17, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, W.M.P.; Grenen, E.G.; O’Connell, M.; Blanch-Hartigan, D.; Chou, W.-Y.S.; Hall, K.L.; Taber, J.M.; Vogel, A.L. Integrating Knowledge across Domains to Advance the Science of Health Behavior: Overcoming Challenges and Facilitating Success. Transl. Behav. Med. 2017, 7, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turconi, G.; Celsa, M.; Rezzani, C.; Biino, G.; Sartirana, M.A.; Roggi, C. Reliability of a Dietary Questionnaire on Food Habits, Eating Behaviour and Nutritional Knowledge of Adolescents. Eur. J. Clin. Nutr. 2003, 57, 753–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tortolero, S.R.; Markham, C.M.; Peskin, M.F.; Shegog, R.; Addy, R.C.; Escobar-Chaves, S.L.; Baumler, E.R. It’s Your Game: Keep It Real: Delaying Sexual Behavior with an Effective Middle School Program. J. Adolesc. Health 2010, 46, 169–179. [Google Scholar] [CrossRef] [Green Version]
- Peleg, A.; Neumann, L.; Friger, M.; Peleg, R.; Sperber, A.D. Outcomes of a Brief Alcohol Abuse Prevention Program for Israeli High School Students. J. Adolesc. Health 2001, 28, 263–269. [Google Scholar] [CrossRef]
- Tucker, P.; van Zandvoort, M.M.; Burke, S.M.; Irwin, J.D. The Influence of Parents and the Home Environment on Preschoolers’ Physical Activity Behaviours: A Qualitative Investigation of Childcare Providers’ Perspectives. BMC Public Health 2011, 11, 168. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Demographic Indicators | N (%) | |
|---|---|---|
| Gender of students | male | 128 (49.6%) |
| female | 130 (50.4%) | |
| Educational attainment of father | primary school or less | 52 (20.2%) |
| vocational school | 113 (43.8%) | |
| secondary school | 46 (17.8%) | |
| university/college | 12 (4.7%) | |
| not known, missing | 35 (13.6%) | |
| Educational attainment of mother | primary school or less | 65 (25.2%) |
| vocational school | 71 (27.5%) | |
| secondary school | 72 (27.9%) | |
| university/college | 20 (7.8%) | |
| not known, missing | 30 (11.6%) | |
| Employment status of father | unemployed | 8 (3.1%) |
| employed | 230 (89.1%) | |
| not known, missing | 20 (7.8%) | |
| Employment status of mother | unemployed | 40 (15.5%) |
| employed | 207 (80.2%) | |
| not known, missing | 11 (4.3%) | |
| Age | mean (±SD) | 14.9 (0.61) |
| Family affluence | mean (±SD) | 5.68 (2.14) |
| Breakfast Consumption | Fruits Consumption | Vegetables Consumption | Sweets Consumption | Soft Drinks Consumption | Moderate-to-Vigorous Physical Activity | Vigorous Physical Activity | ||
|---|---|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||
| Gender of students | male | 89 (46.6%) | 88 (46.6%) | 88 (46.6%) | 88 (46.3%) | 89 (46.8%) | 83 (46.1%) | 79 (48.2%) |
| female | 102 (53.4%) | 101 (53.4%) | 101 (53.4%) | 102 (53.7%) | 101 (53.2%) | 97 (53.9%) | 85 (51.8%) | |
| Age | 14 years old | 31 (16.2%) | 30 (15.9%) | 30 (15.9%) | 31 (16.3%) | 30 (15.8%) | 30 (16.7%) | 28 (17.1%) |
| 15 years old | 137 (71.7%) | 136 (71.9%) | 136 (71.9%) | 136 (71.6%) | 137 (72.1%) | 129 (71.7%) | 117 (71.3%) | |
| 16 years old | 23 (12.0%) | 23 (12.2%) | 23 (12.2%) | 23 (12.1%) | 23 (12.1%) | 21 (11.7%) | 19 (11.6%) | |
| Educational attainment of father | primary school or less | 41 (21.5%) | 40 (21.2%) | 40 (21.2%) | 41 (21.6%) | 41 (21.6%) | 35 (19.4%) | 35 (21.3%) |
| vocational school | 99 (51.8%) | 98 (51.9%) | 98 (51.9%) | 98 (51.6%) | 98 (51.6%) | 96 (53.3%) | 84 (51.2%) | |
| secondary school | 39 (20.4%) | 39 (20.6%) | 39 (20.6%) | 39 (20.5%) | 39 (20.5%) | 38 (21.1%) | 34 (20.7%) | |
| university/college | 12 (6.3%) | 12 (6.4%) | 12 (6.4%) | 12 (6.3%) | 12 (6.3%) | 11 (6.1%) | 11 (6.7%) | |
| Educational attainment of mother | primary school or less | 48 (25.1%) | 47 (24.9%) | 47 (24.9%) | 48 (25.3%) | 48 (25.3%) | 45 (25.0%) | 43 (26.2%) |
| vocational school | 60 (31.4%) | 59 (31.2%) | 59 (31.2%) | 59 (31.1%) | 60 (31.6%) | 57 (31.7%) | 50 (30.5%) | |
| secondary school | 65 (34.0%) | 65 (34.4%) | 65 (34.4%) | 65 (34.2%) | 64 (33.7%) | 60 (33.3%) | 53 (32.3%) | |
| university/college | 18 (9.4%) | 18 (9.5%) | 18 (9.5%) | 18 (9.5%) | 18 (9.5%) | 18 (10.0%) | 18 (10.9%) | |
| Employment status of father | unemployed | 6 (3.1%) | 6 (3.8%) | 6 (3.2%) | 6 (3.2%) | 6 (3.2%) | 6 (3.3%) | 5 (3.1%) |
| employed | 185 (96.9%) | 183 (96.8%) | 183 (96.8%) | 184 (96.8%) | 184 (96.8%) | 174 (96.7%) | 159 (96.9%) | |
| Employment status of mother | unemployed | 30 (15.7%) | 30 (15.9%) | 30 (15.9%) | 30 (15.8%) | 29 (15.3%) | 26 (14.4%) | 25 (15.2%) |
| employed | 161 (84.3%) | 159 (84.1%) | 159 (84.1%) | 160 (84.2%) | 161 (84.7%) | 154 (85.6%) | 139 (84.8%) | |
| Total | 191 (100.0%) | 189 (100.0%) | 189 (100.0%) | 190 (100.0%) | 190 (100.0%) | 180 (100.0%) | 164 (100.0%) | |
| Family affluence | mean (±SD) | 5.80 (2.18) | 5.81 (2.18) | 5.81 (2.18) | 5.79 (2.19) | 5.79 (2.19) | 5.79 (2.16) | 5.73 (2.13) |
| Health knowledge (nutrition or physical activity) | mean (±SD) | 15.00 (4.66) | 15.74 (4.68) | 15.74 (4.68) | 15.78 (4.64) | 15.77 (4.66) | 15.49 (3.26) | 15.49 (3.31) |
| Proportion of missing answers | 25.9% | 26.7% | 26.7% | 26.4% | 26.4% | 30.2% | 36.4% | |
| MODEL I. | MODEL II. | MODEL III. | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Health Knowledge (Nutrition) | Breakfast Consumption | Health Knowledge (Nutrition) | Fruits Consumption | Health Knowledge (Nutrition) | Vegetables Consumption | ||||
| Employment of mother (ref.: employed) | −0.03 [p = 0.523] | 0.06 [p = 0.493] | −0.10 [p = 0.124] | 0.01 [p = 0.864] | −0.05 [p = 0.505] | −0.03 [p = 0.478] | |||
| Employment of father (ref.: employed) | −0.05 [p = 0.083] | −0.02 [p = 0.801] | −0.04 [p = 0.605] | 0.01 [p = 0.852] | −0.10 [p = 0.169] | −0.02 [p = 0.722] | |||
| Family affluence | −0.08 [p = 0.031] | 0.03 [p = 0.720] | −0.17 [p = 0.030] | 0.08 [p = 0.159] | −0.17 [p = 0.025] | 0.12 [p = 0.082] | |||
| Educational attainment of mother (ref.: primary or less) | −0.10 [p = 0.085] | −0.12 [p = 0.262] | −0.15 [p = 0.162] | 0.02 [p = 0.797] | −0.16 [p = 0.081] | −0.04 [p = 0.775] | |||
| Educational attainment of father (ref.: primary or less) | 0.21 [p = 0.002] | −0.06 [p = 0.583] | 0.38 [p = 0.012] | −0.01 [p = 0.892] | 0.38 [p = 0.008] | −0.05 [p = 0.495] | |||
| Age (child) | −0.21 [p = 0.009] | −0.09 [p = 0.460] | −0.42 [p = 0.004] | −0.01 [p = 0.955] | −0.42 [p = 0.034] | −0.24 [p = 0.009] | |||
| Gender (child, ref.: boy) | 0.24 [p = 0.008] | −0.41 [p = 0.027] | 0.48 [p = 0.003] | −0.10 [p = 0.329] | 0.49 [p = 0.030] | 0.11 [p = 0.334] | |||
| Health knowledge (nutrition) | −0.09 [p = 0.529] | . | 0.05 [p = 0.179] | . | 0.06 [p = 0.065] | ||||
| Fit statistics of the model | χ2(df) = 10.390 (7); χ2(p−value) = 0.168; CFI = 0.979; RMSEA = 0.050; PCLOSE = 0.431 | χ2(df) = 10.319 (7); χ2(p−value) = 0.171; CFI = 0.979; RMSEA = 0.050; PCLOSE = 0.434 | χ2(df) = 10.340 (7); χ2(p−value) = 0.170; CFI = 0.980; RMSEA = 0.050; PCLOSE = 0.432 | ||||||
| MODEL IV. | MODEL V. | ||||||||
| Health Knowledge (Nutrition) | Sweets Consumption | Health Knowledge (Nutrition) | Soft Drinks Consumption | ||||||
| Employment of mother (ref.: employed) | −0.05 [p = 0.534] | 0.07 [p = 0.358] | −0.02 [p = 0.771] | 0.01 [p = 0.979] | |||||
| Employment of father (ref.: employed) | −0.11 [p = 0.103] | 0.10 [p = 0.333] | −0.11 [p = 0.082] | 0.10 [p = 0.377] | |||||
| Family affluence | −0.17 [p = 0.037] | −0.04 [p = 0.460] | −0.16 [p = 0.043] | −0.07 [p = 0.368] | |||||
| Educational attainment of mother (ref.: primary or less) | −0.16 [p = 0.179] | −0.17 [p = 0.019] | −0.14 [p = 0.226] | −0.18 [p = 0.029] | |||||
| Educational attainment of father (ref.: primary or less) | 0.38 [p = 0.004] | 0.04 [p = 0.602] | 0.37 [p = 0.012] | −0.13 [p = 0.168] | |||||
| Age (child) | −0.42 [p = 0.013] | 0.07 [p = 0.474] | −0.45 [p = 0.003] | 0.27 [p = 0.038] | |||||
| Gender (child, ref.: boy) | 0.47 [p = 0.002] | 0.08 [p = 0.495] | 0.51 [p = 0.004] | 0.06 [p = 0.643] | |||||
| Health knowledge (nutrition) | . | −0.04 [p = 0.393] | . | −0.08 [p = 0.165] | |||||
| Fit statistics of the model | χ2(df) = 10.146 (7); χ2(p−value) = 0.180; CFI = 0.982; RMSEA = 0.049; PCLOSE = 0.448 | χ2(df) = 10.484 (7); χ2(p−value) = 0.163; CFI = 0.982; RMSEA = 0.051; PCLOSE = 0.423 | |||||||
| MODEL VI. | MODEL VII. | ||||||||
| Health Knowledge (Physical Activity) | Moderate−to−Vigorous Physical Activity | Health Knowledge (Physical Activity) | Vigorous Physical Activity | ||||||
| Employment of mother (ref.: employed) | −0.03 [p = 0.670] | −0.05 [p = 0.500] | −0.08 [p = 0.226] | −0.21 [p = 0.036] | |||||
| Employment of father (ref.: employed) | −0.02 [p = 0.725] | −0.14 [p = 0.143] | −0.06 [p = 0.410] | −0.21 [p = 0.057] | |||||
| Family affluence | 0.05 [p = 0.331] | 0.18 [p = 0.044] | 0.09 [p = 0.122] | 0.16 [p = 0.023] | |||||
| Educational attainment of mother (ref.: primary or less) | 0.01 [p = 0.926] | −0.04 [p = 0.692] | 0.00 [p = 0.984] | −0.05 [p = 0.602] | |||||
| Educational attainment of father (ref.: primary or less) | 0.24 [p = 0.028] | 0.06 [p = 0.604] | 0.25 [p = 0.013] | 0.07 [p = 0.476] | |||||
| Age (child) | −0.08 [p = 0.470] | −0.22 [p = 0.083] | −0.09 [p = 0.431] | 0.02 [p = 0.889] | |||||
| Gender (child, ref.: boy) | 0.28 [p = 0.030] | −0.54 [p = 0.002] | 0.27 [p = 0.047] | −0.50 [p = 0.001] | |||||
| Health knowledge (physical activity) | 0.20 [p = 0.025] | 0.13 [p = 0.111] | |||||||
| Fit statistics of the model | χ2(df) = 12.531 (7); χ2(p−value) = 0.084; CFI = 0.969; RMSEA = 0.066; PCLOSE = 0.277 | χ2(df) = 11.972 (7); χ2(p−value) = 0.101; CFI = 0.972; RMSEA = 0.066; PCLOSE = 0.290 | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy-Pénzes, G.; Vincze, F.; Sándor, J.; Bíró, É. Does Better Health-Related Knowledge Predict Favorable Health Behavior in Adolescents? Int. J. Environ. Res. Public Health 2020, 17, 1680. https://doi.org/10.3390/ijerph17051680
Nagy-Pénzes G, Vincze F, Sándor J, Bíró É. Does Better Health-Related Knowledge Predict Favorable Health Behavior in Adolescents? International Journal of Environmental Research and Public Health. 2020; 17(5):1680. https://doi.org/10.3390/ijerph17051680
Chicago/Turabian StyleNagy-Pénzes, Gabriella, Ferenc Vincze, János Sándor, and Éva Bíró. 2020. "Does Better Health-Related Knowledge Predict Favorable Health Behavior in Adolescents?" International Journal of Environmental Research and Public Health 17, no. 5: 1680. https://doi.org/10.3390/ijerph17051680
APA StyleNagy-Pénzes, G., Vincze, F., Sándor, J., & Bíró, É. (2020). Does Better Health-Related Knowledge Predict Favorable Health Behavior in Adolescents? International Journal of Environmental Research and Public Health, 17(5), 1680. https://doi.org/10.3390/ijerph17051680