How to Educate Pregnant Women about Endocrine Disruptors?



Abstract
:1. Introduction
2. Methods
2.1. PREVED Project
2.2. Perception of Professionals on Who, When, and How to Educate Pregnant Women
2.3. Construction of the Assessment Tool (PREVED© Questionnaire)
3. Results
3.1. Perception of Professionals on Who, When, and How to Educate Pregnant Women
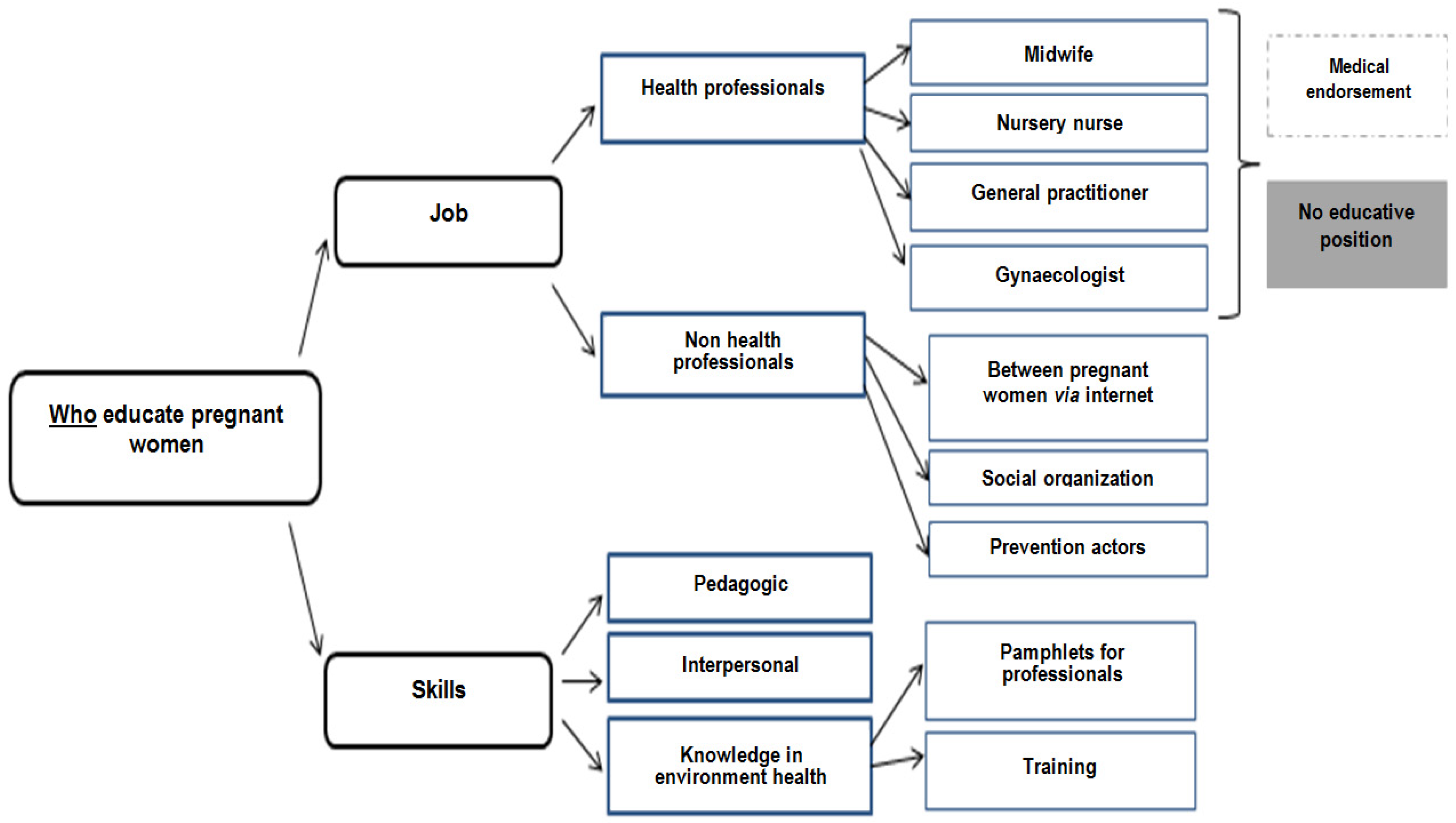
3.1.1. Who
- “In the encounter with these young women, the midwife who travels to homes, who sees her in the preparation of childbirth, can be the means.”
- “PMI professionals, midwives and prevention workers who are used to doing what is called secondary prevention.”
- “Would the attending physician perhaps be suitable, it is the physician who perhaps sees the patient most often, [silence] it is not necessarily on the perinatal subject.”
- “Rather educate professionals who intervene before [pregnancy], especially gynecologists”
- “Information distributed by health professionals is highly listened to.”
- “It is true that health professionals are not necessarily equipped, so it would be a platelet almost for health professionals, to get in touch with people.”
- “In front of a professional they won’t dare ask questions…”
- “The gynecologist can provide a medical guarantee but I’m afraid that as it is not his role, that he delivers the information with all the weight of a doctor but without accompaniment.”
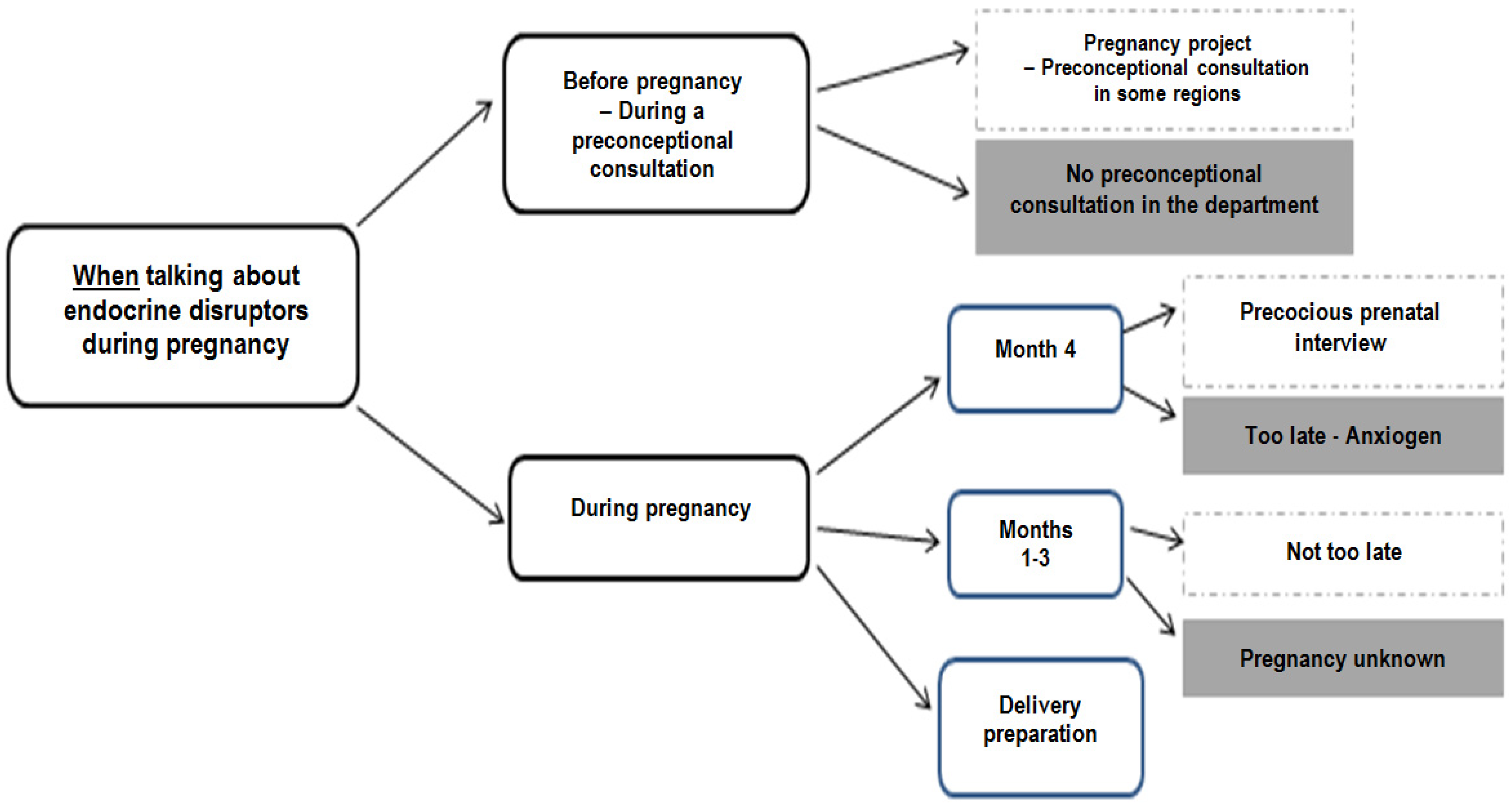
3.1.2. When
- “The time would be even before pregnancy, not necessarily when people are concerned about the issue, but the issue would be before.”
- “First introduce this topic, when women are planning pregnancy, perhaps more …because the goal is to prevent as soon as possible.”
- “I think the 4th month maintenance might be interesting, it’s a time when you really address the patient’s entire environment, you address her daily life, the environment in which she lives, her habitat, This could be a good time to talk about endocrine disrupters, they are quite open and we really talk about their whole environment at that time.”
- “The risk when you start, when you give this information at the fourth month, it’s true to say, well, all I’ve done before, that’s the limit” which can then cause ‘anguish’.”
- “The issue would be earlier, or at least in the first 3 months.”
- “Often the first three months are the time when there are no periods, the first ultrasound is the time when you don’t know too much, they don’t know if they are pregnant, it’s true it’s a bit complicated.”
- “The first 2-3 months, well, it’s true that this is a time when people are a little lost.”
- “There are prep classes at the hospital, and it’s true that we’re talking a little bit about bisphenol A, so we’re talking about glass baby bottles, all those things, after that it’s still little tips like that but it’s really not dedicated to that yet.”
- “They have time, they are on maternity leave.”
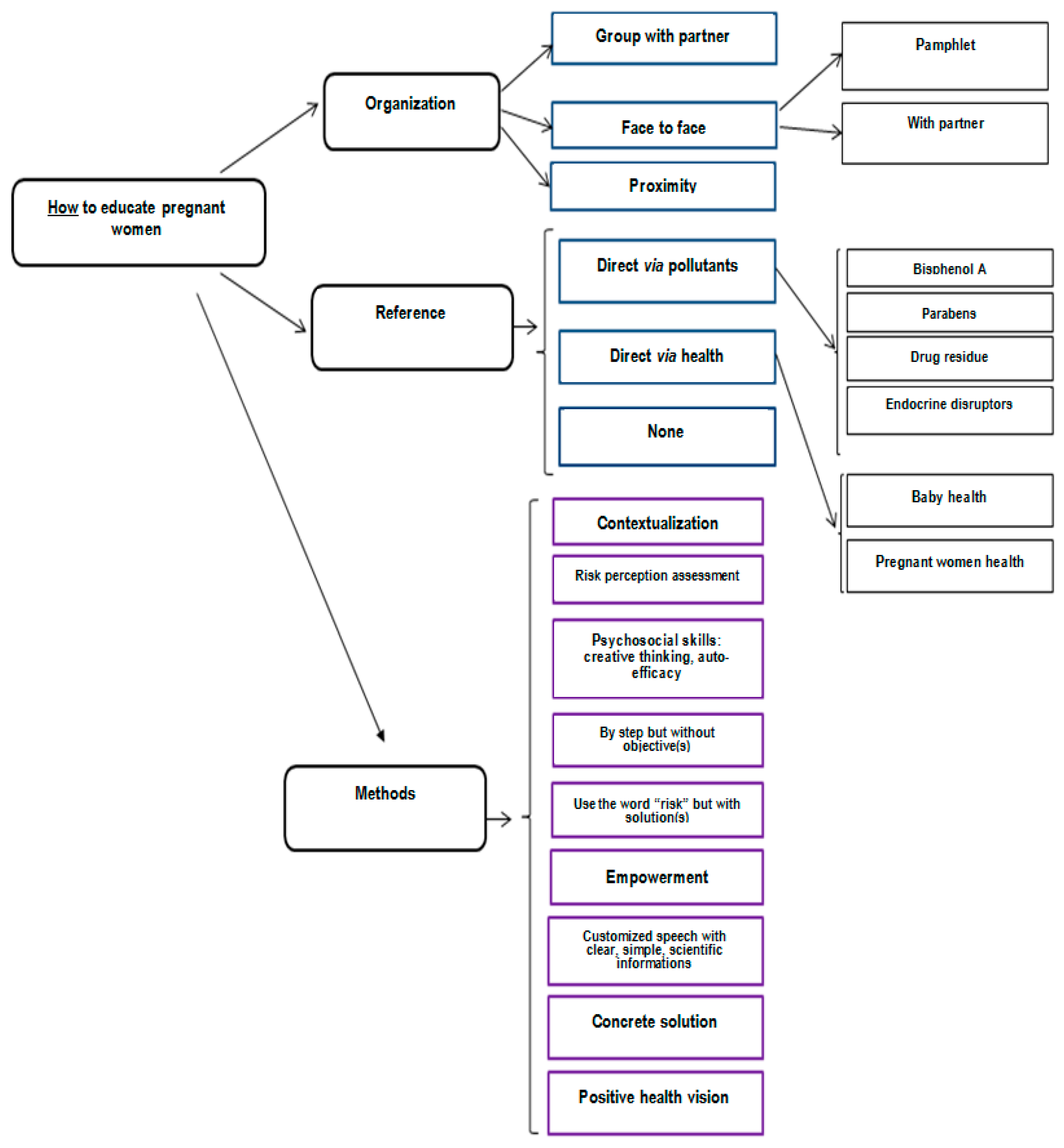
3.1.3. How
3.2. Construction of the Evaluation Tool (PREVED© Questionnaire)
- -
- Knowledge about ED, composed of four questions about routes and sources of exposure, ability to name some ED molecules or families of molecules, and a definition of an ED. A catalogue of pictures illustrating sources of exposure helped the interviewer to ask questions.
- -
- Attitudes as perception of risk with two components: Perceived severity and vulnerability. The created score is based on and adapted from the Perception of Pregnancy Risk Questionnaire [16]. It is composed of three questions with a binary and/or visual analogic scale.
- -
- Practices as the perceived ability to reduce one’s exposure to EDs with a visual analogic scale.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barouki, R.; Gluckman, P.D.; Grandjean, P.; Hanson, M.; Heindel, J.J. Developmental origins of non-communicable disease: Implications for research and public health. Environ. Health Glob. Access Sci. Source 2012, 11, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veiga-Lopez, A.; Kannan, K.; Liao, C.; Ye, W.; Domino, S.E.; Padmanabhan, V. Gender-Specific Effects on Gestational Length and Birth Weight by Early Pregnancy BPA Exposure. J. Clin. Endocrinol. Metab. 2015, 100, E1394–E1403. [Google Scholar] [CrossRef] [PubMed]
- Troisi, J.; Mikelson, C.; Richards, S.; Symes, S.; Adair, D.; Zullo, F.; Guida, M. Placental concentrations of bisphenol A and birth weight from births in the Southeastern U.S. Placenta 2014, 35, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, B.; Vetrano, A.M.; Archer, F.E.; Marcella, S.W.; Buckley, B.; Wartenberg, D.; Robson, M.G.; Klim, J.; Azhar, S.; Cavin, S.; et al. Effects of maternal exposure to phthalates and bisphenol A during pregnancy on gestational age. J. Matern.-Fetal Neonatal Med. 2014, 27, 323–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, K.K.; McElrath, T.F.; Meeker, J.D. Environmental phthalate exposure and preterm birth. JAMA Pediatr. 2014, 168, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Gascon, M.; Casas, M.; Morales, E.; Valvi, D.; Ballesteros-Gómez, A.; Luque, N.; Rubio, S.; Monfort, N.; Ventura, R.; Martínez, D.; et al. Prenatal exposure to bisphenol A and phthalates and childhood respiratory tract infections and allergy. J. Allergy Clin. Immunol. 2015, 135, 370–378. [Google Scholar] [CrossRef]
- Ferguson, K.K.; Peterson, K.E.; Lee, J.M.; Mercado-García, A.; Blank-Goldenberg, C.; Téllez-Rojo, M.M.; Meeker, J.D. Prenatal and peripubertal phthalates and bisphenol A in relation to sex hormones and puberty in boys. Reprod. Toxicol. Elmsford N 2014, 47, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Kalkbrenner, A.E.; Schmidt, R.J.; Penlesky, A.C. Environmental chemical exposures and autism spectrum disorders: A review of the epidemiological evidence. Curr. Probl. Pediatr. Adolesc. Health Care 2014, 44, 277–318. [Google Scholar] [CrossRef] [Green Version]
- Braun, J.M.; Kalkbrenner, A.E.; Just, A.C.; Yolton, K.; Calafat, A.M.; Sjödin, A.; Hauser, R.; Webster, G.M.; Chen, A.; Lanphear, B.P. Gestational Exposure to Endocrine-Disrupting Chemicals and Reciprocal Social, Repetitive, and Stereotypic Behaviors in 4- and 5-Year-Old Children: The HOME Study. Environ. Health Perspect. 2014, 122, 513–520. [Google Scholar] [CrossRef]
- Cohn, B.A.; La Merrill, M.; Krigbaum, N.Y.; Yeh, G.; Park, J.-S.; Zimmermann, L.; Cirillo, P.M. DDT Exposure in Utero and Breast Cancer. J. Clin. Endocrinol. Metab. 2015, 100, 2865–2872. [Google Scholar] [CrossRef]
- Lane, A.; Goodyer, C.G.; Rab, F.; Ashley, J.M.; Sharma, S.; Hodgson, A.; Nisker, J. Pregnant Women’s perceptions of exposure to brominated flame retardants. Reprod. Health 2016, 13, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chabert, M.-C.; Perrin, J.; Berbis, J.; Bretelle, F.; Adnot, S.; Courbiere, B. Lack of information received by a French female cohort regarding prevention against exposure to reprotoxic agents during pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 205, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Marie, C.; Lémery, D.; Vendittelli, F.; Sauvant-Rochat, M.-P. Perception of Environmental Risks and Health Promotion Attitudes of French Perinatal Health Professionals. Int. J. Environ. Res. Public. Health 2016, 13, 1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouillon, S.; Deshayes-Morgand, C.; Enjalbert, L.; Rabouan, S.; Hardouin, J.-B.; Group DisProSE; Migeot, V.; Albouy-Llaty, M. Endocrine Disruptors and Pregnancy: Knowledge, Attitudes and Prevention Behaviors of French Women. Int. J. Environ. Res. Public. Health 2017, 14, 1021. [Google Scholar] [CrossRef] [Green Version]
- Teysseire, R.; Lecourt, M.; Canet, J.; Manangama, G.; Sentilhes, L.; Delva, F. Perception of Environmental Risks and Behavioral Changes during Pregnancy: A Cross-Sectional Study of French Postpartum Women. Int. J. Environ. Res. Public. Health 2019, 16, 565. [Google Scholar] [CrossRef] [Green Version]
- Ashley, J.M.; Hodgson, A.; Sharma, S.; Nisker, J. Pregnant women’s navigation of information on everyday household chemicals: Phthalates as a case study. BMC Pregnancy Childbirth 2015, 15, 312. [Google Scholar] [CrossRef] [Green Version]
- Stotland, N.E.; Sutton, P.; Trowbridge, J.; Atchley, D.S.; Conry, J.; Trasande, L.; Gerbert, B.; Charlesworth, A.; Woodruff, T.J. Counseling Patients on Preventing Prenatal Environmental Exposures—A Mixed-Methods Study of Obstetricians. PLoS ONE 2014, 9, e98771. [Google Scholar] [CrossRef]
- Ferrari, R.M.; Siega-Riz, A.M.; Evenson, K.R.; Moos, M.-K.; Carrier, K.S. A qualitative study of women’s perceptions of provider advice about diet and physical activity during pregnancy. Patient Educ. Couns. 2013, 91, 372–377. [Google Scholar] [CrossRef] [Green Version]
- Barrett, E.S.; Sathyanarayana, S.; Janssen, S.; Redmon, J.B.; Nguyen, R.H.N.; Kobrosly, R.; Swan, S.H. TIDES Study Team Environmental health attitudes and behaviors: Findings from a large pregnancy cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 176, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Pasinlioğlu, T. Health education for pregnant women: The role of background characteristics. Patient Educ. Couns. 2004, 53, 101–106. [Google Scholar] [CrossRef]
- Che, S.-R.; Barrett, E.S.; Velez, M.; Conn, K.; Heinert, S.; Qiu, X. Using the Health Belief Model to Illustrate Factors That Influence Risk Assessment during Pregnancy and Implications for Prenatal Education about Endocrine Disruptors. Policy Futur. Educ. 2014, 12, 961–974. [Google Scholar] [CrossRef] [Green Version]
- Rouillon, S.; El Ouazzani, H.; Rabouan, S.; Migeot, V.; Albouy-Llaty, M. Determinants of Risk Perception Related to Exposure to Endocrine Disruptors during Pregnancy: A Qualitative and Quantitative Study on French Women. Int. J. Environ. Res. Public. Health 2018, 15, 2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaquoi, L.; Edwards, N. A Scoping Review of Maternal and Child Health Clinicians Attitudes, Beliefs, Practice, Training and Perceived Self-Competence in Environmental Health. Int. J. Environ. Res. Public. Health 2015, 12, 15769–15781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathyanarayana, S.; Focareta, J.; Dailey, T.; Buchanan, S. Environmental exposures: How to counsel preconception and prenatal patients in the clinical setting. Am. J. Obstet. Gynecol. 2012, 207, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Haruty, B.; Friedman, J.; Hopp, S.; Daniels, R.; Pregler, J. Reproductive health and the environment: Counseling patients about risks. Clevel. Clin. J. Med. 2016, 83, 367–372. [Google Scholar] [CrossRef]
- Küllenberg de Gaudry, D.; Grede, N.; Motschall, E.; Lins, S. Analysis of German nutrition brochures for pregnant women with evidence-based patient information criteria. Patient Educ. Couns. 2015, 98, 207–212. [Google Scholar] [CrossRef]
- Rosas, L.G.; Trujillo, C.; Camacho, J.; Madrigal, D.; Bradman, A.; Eskenazi, B. Acceptability of health information technology aimed at environmental health education in a prenatal clinic. Patient Educ. Couns. 2014, 97, 244–247. [Google Scholar] [CrossRef] [Green Version]
- Jackson, R.A.; Stotland, N.E.; Caughey, A.B.; Gerbert, B. Improving diet and exercise in pregnancy with Video Doctor counseling: A randomized trial. Patient Educ. Couns. 2011, 83, 203–209. [Google Scholar] [CrossRef]
- Nisbeth Jensen, M.; Fage-Butler, A.M. Antenatal group consultations: Facilitating patient-patient education. Patient Educ. Couns. 2016, 99, 1999–2004. [Google Scholar] [CrossRef]
- Albouy-Llaty, M.; Rouillon, S.; El Ouazzani, H.; Group DisProSE; Rabouan, S.; Migeot, V. Environmental Health Knowledge, Attitudes, and Practices of French Prenatal Professionals Working with a Socially Underprivileged Population: A Qualitative Study. Int. J. Environ. Res. Public. Health 2019, 16, 2544. [Google Scholar] [CrossRef] [Green Version]
- El Ouazzani, H.; Rouillon, S.; Sifer-Rivière, L.; Dupuis, A.; Venisse, N.; Gourgues, A.-S.; Pierre, F.; Rabouan, S.; Migeot, V.; Albouy-Llaty, M. Impact of a perinatal environmental health education intervention on exposure to endocrine disruptors—PREVED study: Protocol for a randomized controlled trial. In Press.
- Jarman, M.; Adam, L.; Lawrence, W.; Barker, M.; Bell, R.C. Healthy conversation skills as an intervention to support healthy gestational weight gain: Experience and perceptions from intervention deliverers and participants. Patient Educ. Couns. 2019, 102, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Postlethwaite, D. Preconception Health Counseling for Women Exposed to Teratogens: The Role of the Nurse. J. Obstet. Gynecol. Neonatal Nurs. 2003, 32, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Belfrage, A.S.V.; Grotmol, K.S.; Tyssen, R.; Moum, T.; Finset, A.; Isaksson Rø, K.; Lien, L. Factors influencing doctors’ counselling on patients’ lifestyle habits: A cohort study. BJGP Open 2018, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, D. Which educational interventions improve healthcare professionals’ resilience? Med. Teach. 2016, 38, 1236–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saravelos, S.; Regan, L. The Importance of Preconception Counseling and Early Pregnancy Monitoring. Semin. Reprod. Med. 2011, 29, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.; de Normanville, C.; Payne, K.; Kelly, M.P. Making every contact count: An evaluation. Public Health 2013, 127, 653–660. [Google Scholar] [CrossRef] [PubMed]
- de Vries, H.; Bakker, M.; Mullen, P.D.; van Breukelen, G. The effects of smoking cessation counseling by midwives on Dutch pregnant women and their partners. Patient Educ. Couns. 2006, 63, 177–187. [Google Scholar] [CrossRef]
- Sutton, C.D.; Carvalho, B. What’s trending now? An analysis of trends in internet searches for labor epidurals. Int. J. Obstet. Anesth. 2017, 30, 52–57. [Google Scholar] [CrossRef]
- Brixi, O. Eduquer pour La Santé Autrement; Le Manuscrit: Paris, France, 2008; ISBN 978-2-304-01382-5. [Google Scholar]
- Forbech Vinje, H.; Hanson Ausland, L.; Langeland, E. The Application of Salutogenesis in the Training of Health Professionals. In Handbook of Salutogenesis; Springer: Sham, Switzerland, 2016; pp. 307–318. [Google Scholar]
- Tinney, V.A.; Paulson, J.A.; Bathgate, S.L.; Larsen, J.W. Medical education for obstetricians and gynecologists should incorporate environmental health. Am. J. Obstet. Gynecol. 2015, 212, 163–166.e1. [Google Scholar] [CrossRef]
- Khoramabadi, M.; Dolatian, M.; Hajian, S.; Zamanian, M.; Taheripanah, R.; Sheikhan, Z.; Mahmoodi, Z.; Seyedi-Moghadam, A. Effects of Education Based on Health Belief Model on Dietary Behaviors of Iranian Pregnant Women. Glob. J. Health Sci. 2015, 8, 46495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahnazi, H.; Sabooteh, S.; Sharifirad, G.; Mirkarimi, K.; Hassanzadeh, A. The impact of education intervention on the Health Belief Model constructs regarding anxiety of nulliparous pregnant women. J. Educ. Health Promot. 2015, 4, 27. [Google Scholar] [PubMed]
- Renner, B.; Schupp, H.T.; Vollmann, M.; Hartung, F.-M.; Schmälzle, R.; Panzer, M. Risk perception, risk communication and health behavior change. Z. Für Gesundheitspsychologie 2008, 16, 150–153. [Google Scholar] [CrossRef]
- Schmälzle, R.; Renner, B.; Schupp, H.T. Health Risk Perception and Risk Communication. Policy Insights Behav. Brain Sci. 2017, 4, 163–169. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Phases of PREVED Project | Aims | Period | References |
|---|---|---|---|
| Constitution of consortium | to involve researchers, prevention actors and deciders on the project | 2014 | |
| Review of the literature | to choose a behavior change model | 2014–2015 | |
| Interviews of 12 pregnant women | to explore dimensions for constructing the program | 2015 | [14] |
| Focus group of 7 health professionals | aim 1: to discuss how to educate pregnant women for construction of the program aim 2: to explore how to assess the program | 03/2015 | aim 1: result section aim 2: [30] |
| Focus group of 11 perinatal health professionals working with underprivileged population | aim 1: to describe knowledge and attitudes of professionals aim 2: to describe practices of professionals = to discuss how to educate pregnant women for construction of the program | 09/2015 | [30] |
| Cross-sectional study on 30 women | to pre-test of the questionnaire | 07/2015 | |
| Cross-sectional study on 300 women | aim 1: to describe KAP of pregnant women aim 2: to validate the questionnaire | 08/2015-> 04/2016 | aim 1: [14] aim 2: result section |
| Randomized controlled trial on 268 women | to test the efficacy and effectiveness of the program | 04/2017-> 10/2020 | Protocol: [31] Results: ongoing |
| Methods | Biomedical Position | Educative Position |
|---|---|---|
| To customize speech taking representations of pregnant women into account | “EDs are chemical products where exposure is associated with diseases” | “what are EDs for you?” |
| To present risk and solution in the same time | “As EDs are present in plastics, you should avoid plastics” | “you told me there are EDs in plastics, what could you do to avoid it?” |
| To use the word risk but in a positive vision | “You must avoid this product” | “what could you do about ED exposure to improve health?” |
| To highlight solutions that the pregnant women can use to decrease this exposure | “It is a very good idea to have chosen a glass bottle!” | |
| To empower, to motivate that it is possible to change | “You told me you wanted the best for your baby, what about doing as well outside the house as you do inside the house?” [cooking] | |
| To have concrete speech | “In your house….” | |
| To respect steps | “You should throw away all your plastic boxes” | “You can do that this week and think about another way to do better the following week” |
| Dimension/Questions | Possible Spontaneous Answers | Score |
|---|---|---|
| KNOWLEDGE [40,5 points] -> to multiplicate by 2.4691 to obtain a score on 100 | ||
| 1. How could you imagine that chemical products which could degrade your health enter in your body or in your baby’s body? | Skin, Breathing, Eating, Drinking water, Through the placenta | 0–5 points |
| 2. According to you, what are the sources of exposure to ED that could degrade your health? | ||
| Outside wrapping | Mineral water, Tap water, Fresh fruits and vegetables, Shower gel, deodorant, perfume, Day cream, makeup, Baby cream, Diaper-wipe, Drug, Household domestic, Home improvement products, Air ambient, Furniture, Toys, Candle, Incense, Interior perfume | 0–22 points |
| In wrapping | Plastic bottle, Card bottle, Cans for drinks, Cans for food, Vacuum pack, Shrink-wrapped tray, Glass bottle | |
| 3. If you have heard about EDs, could you name some? | Bisphenol A, Parabens, Phthalates, Pesticides, PCB, Flame retardant, Alkyl phenol, Nitrate, Phytoestrogen, Heavy metal, Phenoxyethanol (1 point for bisphenol A and parabens; 0.5 for another proposition) | 0–6.5 points |
| 4. How could you define an ED? | Hormonal molecule, Chemical molecule, Molecule produced by body, Molecule which alters body functioning, bacteria, Drug, Natural molecule | 0–7 points |
| RISK PERCEPTION [SEVERITY: 400 POINTS—VULNERABILITY: 1400 POINTS] | ||
| SEVERITY: 5. In general terms, the risk of endocrine disruptor exposure for pregnant women health is: | Nul (0 points)-Light (33 points)-High (100 points) | 0–100 points |
| 6. In general terms, how do you evaluate the risk of endocrine disruptor exposure during your pregnancy for… | A baby, An adolescent, An adult Nul……………………………….very high * | 3 times 0–100 points |
| VULNERABILITY: 7. For each scale, make a mark for your vision of the risk about ED | ||
| For your health | Nonexistent……………………………….very high * | 0–100 points |
| For your baby to be born prematurely | Nonexistent……………………………….very high * | 0–100 points |
| For your baby to have a congenital malformation | Nonexistent……………………………….very high * | 0–100 points |
| For your baby to be small for gestational age | Nonexistent……………………………….very high * | 0–100 points |
| For your future adolescent to be obese | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have asthma | Nonexistent……………………………….very high * | 0–100 points |
| For your children to develop an allergy | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have immunity problems | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have premature puberty | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have problems making babies | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have autism | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have behavioral problems | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have problems walking | Nonexistent……………………………….very high * | 0–100 points |
| For your children to have cancer when adult | Nonexistent……………………………….very high * | 0–100 points |
| BEHAVIOR [100 POINTS] | ||
| PERCEIVED ABILITY 8. Do you think you are able to avoid chemical products like ED which disturb your health? | No………………………….……….A lot * | 0–100 points |
| Dimension | Test Phase | Adjustment Phase | ||
|---|---|---|---|---|
| α-Cronbach | H Loevinger | α-Cronbach | H Loevinger | |
| Route of exposure | 0.54 | 0.38 | Questions were not modified | |
| Source of exposure | 0.61 | 0.16 | ||
| Knowledge of name | 0.13 | 0.30 | ||
| ED Definition | 0.72 | 0.32 | ||
| Perceived severity | 0.84 | 0.35 | 0.97 | NA (VAS) |
| Perceived vulnerability | 0.95 | NA (VAS) | 0.84 | NA (VAS) |
| General Lifestyle | Diet | Cosmetics and Hobbies | Hygiene |
|---|---|---|---|
| To have a healthy lifestyle | To choose a balanced diet | Do not use pesticides/fertilizers in your garden- To wear gloves when gardening | To regularly clean fridge |
| Do not smoke, to not use drugs, not drink alcohol-To avoid self-medication | To consume foods from organic farming or one’s garden or fresh unprocessed foods-To be careful of the origin of the products you buy | To avoid exposure to paints and products for work/do it yourself | To wash clothes before wearing for the first time |
| To regularly walk-To reduce the use of the vehicle-To live in the country | To breastfeed | To avoid makeup, coloring hair, nail polish/To reduce or stop consumption of cosmetics-To avoid scented cosmetics | To have good hand hygiene |
| To avoid walking near treated fields-To avoid polluted areas/living in an unpolluted environment | To Homemade prepare-To cook well the food | To prefer home-made, organic or natural cosmetics without paraben | To protect yourself when using chemicals household products (gloves, mask, etc.) |
| To aerate its habitat/Clean air vents in habitat-To avoid dusty atmospheres | To use caterer preparation | To prefer the purchase of cosmetics- personal hygiene products in (para)pharmacy | To reduce the use of chemical cleaning products |
| To prefer local products | To reduce the consumption of the canned foods or industrial foods or food additives or food containing GMOs | To prefer the liniment for children | To avoid using indoor perfumes, scented candles or incense, essential oils, sprays and aerosols or inhaling cleaning products or maintenance products without odor/fragrance |
| To protect against chemicals at work-To keep dangerous products out of children | To avoid eating foods that have been frozen | To use biological diapers | To prefer home-made or hypoallergenic cleaning products or detergents, or natural cleaning products (e.g., white vinegar) or products without bleach or ecological cleaning products |
| To check the labelling of cosmetic products, foods, processed drinks and medicines -To prefer all products with a label | To reduce consumption of meat or fish | To avoid synthetic fluff | To avoid wipes for children |
| To learn, read, learn about exposure sources | To consume filtered tap water | To avoid plywood furniture | |
| To reduce the use of plastic dishes, To Recycle, collect waste, To prefer selective sorting | To wash or peel fruits and vegetables | ||
| To limit exposure to waves (phones, wi-fi) | To use set of glasses, glass containers- baby bottles glass-made or plastic containers without ED/To avoid food in plastic containers | ||
| To pay attention to quality water | Do not use -To reduce the use of aluminum foil | ||
| To harvest rainwater | |||
| To avoid products containing bisphenols |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouillon, S.; El Ouazzani, H.; Hardouin, J.-B.; Enjalbert, L.; Rabouan, S.; Migeot, V.; Albouy-Llaty, M. How to Educate Pregnant Women about Endocrine Disruptors? Int. J. Environ. Res. Public Health 2020, 17, 2156. https://doi.org/10.3390/ijerph17062156
Rouillon S, El Ouazzani H, Hardouin J-B, Enjalbert L, Rabouan S, Migeot V, Albouy-Llaty M. How to Educate Pregnant Women about Endocrine Disruptors? International Journal of Environmental Research and Public Health. 2020; 17(6):2156. https://doi.org/10.3390/ijerph17062156
Chicago/Turabian StyleRouillon, Steeve, Houria El Ouazzani, Jean-Benoit Hardouin, Line Enjalbert, Sylvie Rabouan, Virginie Migeot, and Marion Albouy-Llaty. 2020. "How to Educate Pregnant Women about Endocrine Disruptors?" International Journal of Environmental Research and Public Health 17, no. 6: 2156. https://doi.org/10.3390/ijerph17062156
APA StyleRouillon, S., El Ouazzani, H., Hardouin, J. -B., Enjalbert, L., Rabouan, S., Migeot, V., & Albouy-Llaty, M. (2020). How to Educate Pregnant Women about Endocrine Disruptors? International Journal of Environmental Research and Public Health, 17(6), 2156. https://doi.org/10.3390/ijerph17062156