
Preterm Labor Using Tocolysis as a Possible Risk Factor for Postpartum Depression: A 14-Year Population-Based Study in Taiwan



Abstract
:1. Introduction
2. Materials and Methods
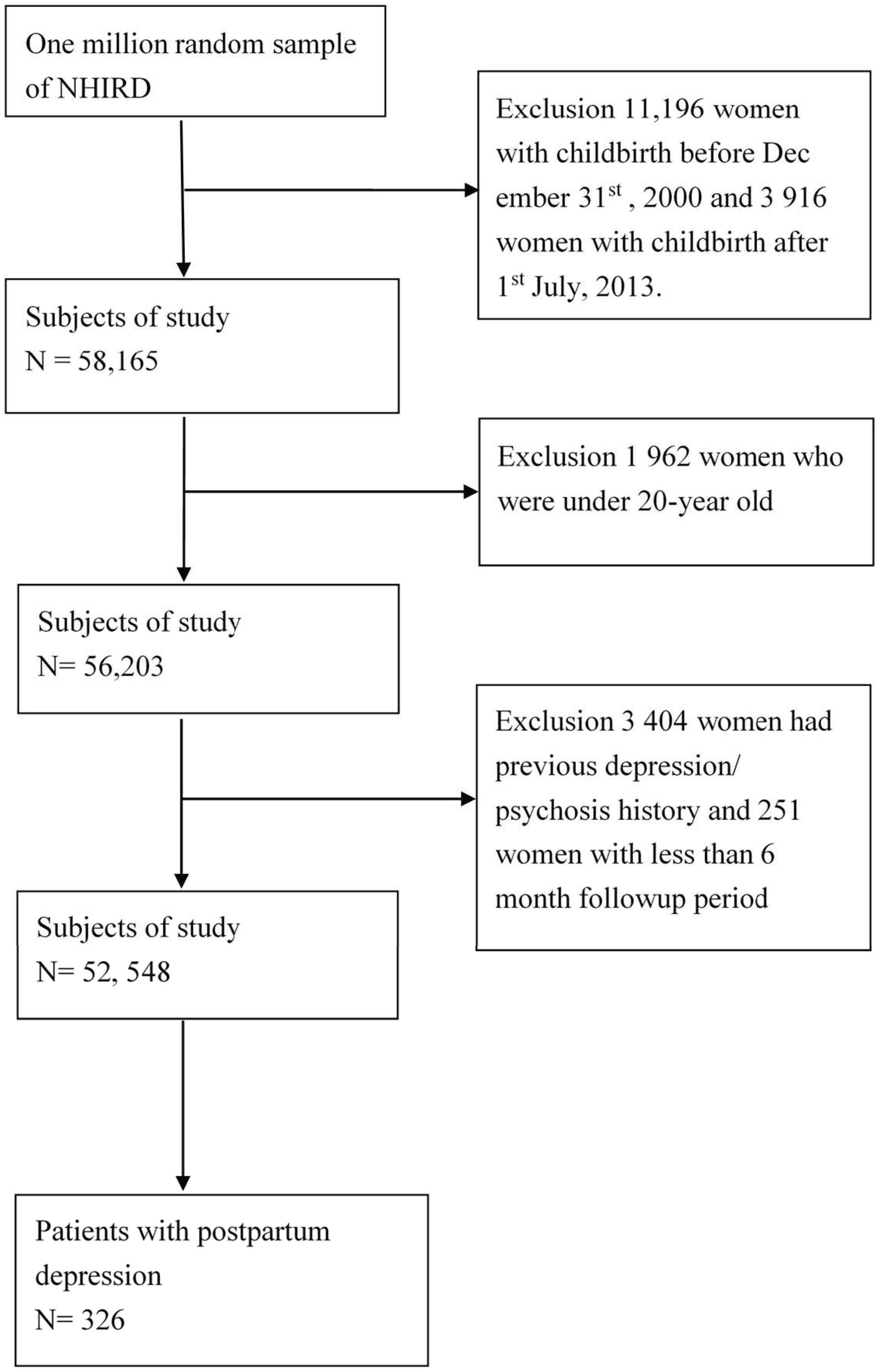
2.1. Data Source and Collection
2.2. Study Population
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Multivariable Analysis of Postpartum Depression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gaynes, B.N.; Gavin, N.; Meltzer-Brody, S.; Lohr, K.N.; Swinson, T.; Gartlehner, G.; Brody, S.; Miller, W.C. Perinatal depression: Prevalence, screening accuracy, and screening outcomes. In AHRQ Evidence Report Summaries; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2005; pp. 1–8. [Google Scholar]
- O’Hara, M.W.; McCabe, J.E. Postpartum depression: Current status and future directions. Annu. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [CrossRef]
- Wisner, K.L.; Sit, D.K.; McShea, M.C.; Rizzo, D.M.; Zoretich, R.A.; Hughes, C.L.; Eng, H.F.; Luther, J.F.; Wisniewski, S.R.; Costantino, M.L. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry 2013, 70, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Closa-Monasterolo, R.; Gispert-Llaurado, M.; Canals, J.; Luque, V.; Zaragoza-Jordana, M.; Koletzko, B.; Grote, V.; Weber, M.; Gruszfeld, D.; Szott, K.; et al. The Effect of Postpartum Depression and Current Mental Health Problems of the Mother on Child Behaviour at Eight Years. Matern. Child Health J. 2017, 21, 1563–1572. [Google Scholar] [CrossRef]
- First, M.B. Diagnostic and statistical manual of mental disorders, 5th edition, and clinical utility. J. Nerv. Ment. Dis. 2013, 201, 727–729. [Google Scholar] [CrossRef] [PubMed]
- Norhayati, M.N.; Hazlina, N.H.; Asrenee, A.R.; Emilin, W.M. Magnitude and risk factors for postpartum symptoms: A literature review. J. Affect. Disord. 2015, 175, 34–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, L.; Dunne, M.P.; Van Vo, T.; Anh, P.N.T.; Khawaja, N.G.; Cao, T.N. Postnatal depressive symptoms amongst women in Central Vietnam: A cross-sectional study investigating prevalence and associations with social, cultural and infant factors. BMC Pregnancy Childbirth 2015, 15, 234. [Google Scholar] [CrossRef]
- Huang, Y.C.; Mathers, N. Postnatal depression—Biological or cultural? A comparative study of postnatal women in the UK and Taiwan. J. Adv. Nurs. 2001, 33, 279–287. [Google Scholar] [CrossRef]
- Chee, C.Y.; Lee, D.T.; Chong, Y.S.; Tan, L.K.; Ng, T.P.; Fones, C.S. Confinement and other psychosocial factors in perinatal depression: A transcultural study in Singapore. J. Affect. Disord. 2005, 89, 157–166. [Google Scholar] [CrossRef]
- Green, K.; Broome, H.; Mirabella, J. Postnatal depression among mothers in the United Arab Emirates: Socio-cultural and physical factors. Psychol. Health Med. 2006, 11, 425–431. [Google Scholar] [CrossRef]
- Kim, Y.K.; Hur, J.W.; Kim, K.H.; Oh, K.S.; Shin, Y.C. Prediction of postpartum depression by sociodemographic, obstetric and psychological factors: A prospective study. Psychiatry Clin. Neurosci. 2008, 62, 331–340. [Google Scholar] [CrossRef]
- Räisänen, S.; Lehto, S.M.; Nielsen, H.S.; Gissler, M.; Kramer, M.R.; Heinonen, S. Fear of childbirth predicts postpartum depression: A population-based analysis of 511 422 singleton births in Finland. BMJ Open 2013, 3, e004047. [Google Scholar] [CrossRef] [Green Version]
- Inandi, T.; Bugdayci, R.; Dundar, P.; Sumer, H.; Sasmaz, T. Risk factors for depression in the first postnatal year: A Turkish study. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 725–730. [Google Scholar] [CrossRef]
- Kretchy, I.A.; Owusu-Daaku, F.T.; Danquah, S.A. Mental health in hypertension: Assessing symptoms of anxiety, depression and stress on anti-hypertensive medication adherence. Int. J. Ment. Health Syst. 2014, 8, 25. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, B.E.; Martin, J.A.; Ventura, S.J. Births: Preliminary Data for 2012. Natl. Vital Stat. Rep. 2013, 62, 1–20. [Google Scholar]
- Lawn, J.E.; Cousens, S.N.; Darmstadt, G.L.; Bhutta, Z.A.; Martines, J.; Paul, V.; Knippenberg, R.; Fogstad, H. 1 year after The Lancet Neonatal Survival Series—Was the call for action heard? Lancet 2006, 367, 1541–1547. [Google Scholar] [CrossRef]
- Wang, L.K.; Chen, W.M.; Chen, C.P. Preterm birth trend in Taiwan from 2001 to 2009. J. Obstet. Gynaecol. Res. 2014, 40, 1547–1554. [Google Scholar] [CrossRef]
- Arias, F.; Rodriquez, L.; Rayne, S.C.; Kraus, F.T. Maternal placental vasculopathy and infection: Two distinct subgroups among patients with preterm labor and preterm ruptured membranes. Am. J. Obstet. Gynecol. 1993, 168, 585–591. [Google Scholar] [CrossRef]
- Gilbert, W.M. The cost of preterm birth: The low cost versus high value of tocolysis. BJOG 2006, 113 (Suppl. 3), 4–9. [Google Scholar] [CrossRef] [PubMed]
- Spong, C.Y. Prediction and prevention of recurrent spontaneous preterm birth. Obstet. Gynecol. 2007, 110, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.S. Neuroendocrine perspectives on social attachment and love. Psychoneuroendocrinology 1998, 23, 779–818. [Google Scholar] [CrossRef]
- Feldman, R. Oxytocin and social affiliation in humans. Horm. Behav. 2012, 61, 380–391. [Google Scholar] [CrossRef]
- Neumann, I.D.; Landgraf, R. Balance of brain oxytocin and vasopressin: Implications for anxiety, depression, and social behaviors. Trends Neurosci. 2012, 35, 649–659. [Google Scholar] [CrossRef]
- Skrundz, M.; Bolten, M.; Nast, I.; Hellhammer, D.H.; Meinlschmidt, G. Plasma Oxytocin Concentration during Pregnancy is associated with Development of Postpartum Depression. Neuropsychopharmacology 2011, 36, 1886–1893. [Google Scholar] [CrossRef] [Green Version]
- Stuebe, A.M.; Grewen, K.; Meltzer-Brody, S. Association between maternal mood and oxytocin response to breastfeeding. J. Womens Health 2013, 22, 352–361. [Google Scholar] [CrossRef]
- Gu, V.; Feeley, N.; Gold, I.; Hayton, B.; Robins, S.; MacKinnon, A.; Samuel, S.; Carter, C.S.; Zelkowitz, P. Intrapartum Synthetic Oxytocin and Its Effects on Maternal Well-Being at 2 Months Postpartum. Birth 2015, 43, 28–35. [Google Scholar] [CrossRef]
- Kang, J.H.; Ho, J.D.; Chen, Y.H.; Lin, H.C. Increased risk of stroke after a herpes zoster attack: A population-based follow-up study. Stroke 2009, 40, 3443–3448. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.H.; Chen, Y.H.; Lin, H.C. Comorbidities amongst patients with multiple sclerosis: A population-based controlled study. Eur. J. Neurol. 2010, 17, 1215–1219. [Google Scholar] [CrossRef]
- National Health Insurance Research Database. Available online: http://nhird.nhri.org.tw/date_01.html (accessed on 7 May 2021).
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Regier, D.A.; Kuhl, E.A.; Kupfer, D.J. The DSM-5, Classification and criteria changes. World Psychiatry 2013, 12, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigod, S.N.; Villegas, L.; Dennis, C.L.; Ross, L.E. Prevalence and risk factors for postpartum depression among women with preterm and low-birth-weight infants: A systematic review. BJOG 2010, 117, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Handelzalts, J.E.; Krissi, H.; Levy, S.; Freund, Y.; Carmiel, N.; Ashwal, E.; Peled, Y. Personality, preterm labor contractions, and psychological consequences. Arch. Gynecol. Obstet. 2015, 293, 575–582. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Fatoye, F.O.; Ola, B.A.; Ijaodola, O.R.; Ibigbami, S.M. Sociodemographic and obstetric risk factors for postpartum depressive symptoms in Nigerian women. J. Psychiatr. Pract. 2005, 11, 353–358. [Google Scholar] [CrossRef]
- Drewett, R.; Blair, P.; Emmett, P.; Emond, A.; the ALSPAC Study Team. Failure to thrive in the term and preterm infants of mothers depressed in the postnatal period: A population-based birth cohort study. J. Child Psychol. Psychiatry 2004, 45, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.N.; Shen, L.J.; Ping, T.; Wang, Y.C.; Chien, C.W. The delivery mode and seasonal variation are associated with the development of postpartum depression. J. Affect. Disord. 2011, 132, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Ding, Y.; Ma, Y.; Xin, X.; Zhang, D. Cesarean section and risk of postpartum depression: A meta-analysis. J. Psychosom. Res. 2017, 97, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Koutra, K.; Vassilaki, M.; Georgiou, V.; Koutis, A.; Bitsios, P.; Chatzi, L.; Kogevinas, M. Antenatal maternal mental health as determinant of postpartum depression in a population based mother-child cohort (Rhea Study) in Crete, Greece. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.Y.; Choi, Y.; Kim, J.; Cho, K.H.; Park, E.C. The synergistic effect of breastfeeding discontinuation and cesarean section delivery on postpartum depression: A nationwide population-based cohort study in Korea. J. Affect. Disord. 2017, 218, 53–58. [Google Scholar] [CrossRef]
- Andersson, L.; Poromaa, I.S.; Wulff, M.; Åström, M.; Bixo, M. Implications of Antenatal Depression and Anxiety for Obstetric Outcome. Obstet. Gynecol. 2004, 104, 467–476. [Google Scholar] [CrossRef]
- Rydahl, E.; Eriksen, L.; Juhl, M. Effects of induction of labor prior to post-term in low-risk pregnancies: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 170–208. [Google Scholar] [CrossRef]
- Chung, T.K.; Lau, T.K.; Yip, A.S.; Chiu, H.F.; Lee, D.T. Antepartum depressive symptomatology is associated with adverse obstetric and neonatal outcomes. Psychosom. Med. 2001, 63, 830–834. [Google Scholar] [CrossRef]
- Hansotte, E.; Payne, S.I.; Babich, S.M. Positive postpartum depression screening practices and subsequent mental health treatment for low-income women in Western countries: A systematic literature review. Public Health Rev. 2017, 38, 3. [Google Scholar] [CrossRef] [Green Version]
- Mundorf, C.; Shankar, A.; Moran, T.; Heller, S.; Hassan, A.; Harville, E.; Lichtveld, M. Reducing the Risk of Postpartum Depression in a Low-Income Community Through a Community Health Worker Intervention. Matern. Child Health J. 2018, 22, 520–528. [Google Scholar] [CrossRef]
- Liu, J.-M.; Chiu, F.-H.; Liu, Y.-P.; Chen, S.-P.; Chan, H.-H.; Yang, J.-J.; Chang, F.-W.; Hsu, R.-J. Antepartum urinary tract infection and postpartum depression in Taiwan—A nationwide population-based study. BMC Pregnancy Childbirth 2018, 18, 79. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Demographic Factor | Total Pregnant Women (%) | Women without PPD (%) | Women with PPD (%) | p Value a |
|---|---|---|---|---|
| No. of patients | 52,548 | 52,222 | 326 | |
| Mean age (standard deviation) Age (mean ± SD, years) | 29.6 ± 4.6 | 29.6 ± 4.6 | 29.5 ± 4.6 | 0.853 |
| 20–24 | 8747 (16.6) | 8688(16.6) | 59(18.1) | |
| 25–29 | 20,149(38.4) | 20,027(38.4) | 122(37.5) | |
| 30–34 | 17,205(32.7) | 17,101(32.7) | 104(31.9) | |
| 35–39 | 5513(10.5) | 5479(10.5) | 34(10.4) | |
| ≥40 | 934(1.8) | 927(1.8) | 7(2.1) | |
| Charlson comorbidity index | 0.1 ± 0.4 | 0.1 ± 0.4 | 0.2 ± 0.5 | 0.031 |
| 0 | 47,243(89.9) | 46,963(89.9) | 280(85.9) | |
| 1 | 4597(8.7) | 4560(8.7) | 37(11.4) | |
| 2 | 562(1.1) | 555(1.1) | 7(2.1) | |
| ≥3 | 146(0.3) | 144(0.3) | 2(0.6) | |
| Comorbidity disease | ||||
| Chronic pulmonary disease | 1507(2.9) | 1495(2.9) | 12(3.7) | 0.401 |
| Hypertension | 475(0.9) | 467(0.9) | 8(2.5) | 0.010 |
| Hypertension-complicated pregnancy | 811(1.5) | 802(1.5) | 9(2.8) | 0.106 |
| Diabetes complicating pregnancy childbirth | 2542(4.8) | 2527(4.8) | 15(4.6) | 0.999 |
| Hyperlipidemia | 135(0.3) | 134(0.3) | 1(0.3) | 0.569 |
| Heart disease | 976(1.9) | 960(1.8) | 16(4.9) | <0.001 |
| Anemia | 3644(6.2) | 3624(6.2) | 20(6.1) | 0.987 |
| Peptic ulcer disease | 1743(3.3) | 1723(3.3) | 20(6.1) | 0.008 |
| Cerebrovascular disease | 55(0.1) | 55(0.1) | 0 (0) | 1.00 |
| Parkinson’s disease | 2(0.1) | 2(0.1) | 2(0) | 1.00 |
| Epilepsy | 62(0.1) | 62(0.1) | 0(0) | 1.000 |
| Tuberculosis | 33(0.1) | 33(0.1) | 0(0) | 1.00 |
| Asthma | 605(1.2) | 602(1.2) | 3(0.9) | 0.998 |
| Liver cirrhosis | 822(1.6) | 814(1.6) | 8(2.5) | 0.178 |
| Chronic kidney disease | 51(0.1) | 48(0.1) | 3(0.9) | 0.004 |
| Herpes | 853(1.6) | 845(1.6) | 8(2.5) | 0.263 |
| Syphilis | 75(0.1) | 74(0.1) | 1(0.3) | 0.373 |
| Antepartum hemorrhage | 3739(7.1) | 3712(7.1) | 27(8.3) | 0.392 |
| Premature separation of placenta | 153(0.3) | 151(0.3) | 2(0.6) | 0.245 |
| Placenta previa | 1017(1.9) | 1008(1.9) | 9(2.8) | 0.306 |
| Eclampsia or pre-eclampsia | 539(1.0) | 533(1.0) | 6(1.8) | 0.155 |
| Unspecified disorder of the thyroid | 2(0.1) | 2(0.1) | 0(0) | 1.000 |
| Unstable lie | 2296(4.4) | 2271(4.3) | 65(7.7) | 0.006 |
| Polyhydramnios | 214(0.4) | 214(0.4) | 0(0) | 1.000 |
| Oligohydramnios | 1326(2.5) | 1314(2.5) | 14(3.7) | 0.209 |
| Poor fetal growth | 1905(3.6) | 1899(3.6) | 16(4.9) | 0.231 |
| Excessive fetal growth | 985(2.9) | 980(2.9) | 5(3.7) | 0.838 |
| Other known or suspected fetal abnormality | 147(0.3) | 145(0.3) | 2(0.6) | 0.232 |
| Cervical incompetence | 127(0.2) | 125(0.2) | 2(0.6) | 0.187 |
| Early delivery onset | 12,959 (24.7) | 12,846 (24.6) | 113(34.7) | <0.001 |
| Hospital stay (mean ± SD, days) | 3.6 ± 1.6 | 3.6 ± 1.6 | 3.8 ± 2.6 | 0.128 |
| Monthly income (TWD b) | 0.001 | |||
| <20,000 | 17,012(32.4) | 16,873(32.4) | 139(42.6) | |
| 20,000–40,000 | 24,733(47.1) | 24,598(47.1) | 135(42.4) | |
| 40,000–60,000 | 6504(12.4) | 6469(12.4) | 35(10.7) | |
| ≥60,000 | 4299(8.1) | 4282(8.1) | 17(5.3) | |
| Tocolytic drugs | 0.002 | |||
| Yes | 3266(6.2) | 3232(6.2) | 34(10.4) | |
| Only oral form | 2220(4.2) | 2197(4.2) | 23(7.1) | 0.018 |
| Only injection form | 500(1.0) | 491(1.0) | 9(2.7) | 0.004 |
| Both oral and injection forms | 546(1.0) | 544(1.0) | 2(0.6) | 0.780 |
| No | 492,824(93.8) | 48,990(93.8) | 292(89.6) | |
| Uterotonic drugs | 0.178 | |||
| Yes | 37,228(70.8) | 37,008(70.9) | 220(67.5) | |
| No | 15,320(29.2) | 15,214(79.1) | 106(32.5) |
| Estimate | Standard Error | Wals Chi-Square | Adjusted Odds Ratio | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|---|
| Charlson comorbidity index (reference: 0) | ||||||
| 1 | 0.047 | 0.224 | 0.044 | 1.048 | (0.676–1.626) | 0.834 |
| 2 | 0.117 | 0.470 | 0.062 | 1.124 | (0.447–2.827) | 0.804 |
| ≥3 | −0.225 | 0.827 | 0.074 | 0.798 | (0.158–4.040) | 0.786 |
| Hypertension | 0.692 | 0.378 | 3.345 | 1.998 | (0.952–4.194) | 0.067 |
| Peptic ulcer disease | 0.547 | 0.307 | 3.183 | 1.728 | (0.947–3.153) | 0.074 |
| Chronic kidney disease | 2.037 | 0.754 | 7.298 | 7.665 | (1.749–33.595) | 0.007 |
| Heart disease | 0.834 | 0.268 | 9.665 | 2.302 | (1.361–3.895) | 0.002 |
| Unstable lie | 0.545 | 0.211 | 6.676 | 1.724 | (1.141–2.605) | 0.010 |
| Early delivery onset | 0.253 | 0.454 | 0.311 | 1.288 | (0.529–3.138) | 0.577 |
| Monthly income (reference: <20,000) | ||||||
| 20,000–40,000 | −0.409 | 0.121 | 11.343 | 0.664 | (0.524–0.843) | 0.001 |
| 40,000–60,000 | −0.416 | 0.190 | 4.785 | 0.659 | (0.454–0.958) | 0.029 |
| ≥60,000 | −0.713 | 0.258 | 7.624 | 0.490 | (0.295–0.813) | 0.006 |
| Premature birth | 0.141 | 0.455 | 0.096 | 1.151 | (0.471–2.881) | 0.757 |
| Tocolytic drugs (reference: no) | ||||||
| Only oral form | 0.340 | 0.228 | 2.235 | 1.405 | (0.900–2.196) | 0.135 |
| Only injection form | 0.806 | 0.352 | 5.232 | 2.238 | (1.122–4.463) | 0.022 |
| Both oral and injection forms | −0.779 | 0.717 | 1.181 | 0.459 | (0.113–1.870) | 0.277 |
| Uterotonic drugs | −0.180 | 0.120 | 2.260 | 0.835 | (0.660–1.056) | 0.133 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.-M.; Liu, C.-Y.; Hsu, R.-J.; Chang, F.-W. Preterm Labor Using Tocolysis as a Possible Risk Factor for Postpartum Depression: A 14-Year Population-Based Study in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 7211. https://doi.org/10.3390/ijerph18137211
Liu J-M, Liu C-Y, Hsu R-J, Chang F-W. Preterm Labor Using Tocolysis as a Possible Risk Factor for Postpartum Depression: A 14-Year Population-Based Study in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(13):7211. https://doi.org/10.3390/ijerph18137211
Chicago/Turabian StyleLiu, Jui-Ming, Chien-Yu Liu, Ren-Jun Hsu, and Fung-Wei Chang. 2021. "Preterm Labor Using Tocolysis as a Possible Risk Factor for Postpartum Depression: A 14-Year Population-Based Study in Taiwan" International Journal of Environmental Research and Public Health 18, no. 13: 7211. https://doi.org/10.3390/ijerph18137211
APA StyleLiu, J. -M., Liu, C. -Y., Hsu, R. -J., & Chang, F. -W. (2021). Preterm Labor Using Tocolysis as a Possible Risk Factor for Postpartum Depression: A 14-Year Population-Based Study in Taiwan. International Journal of Environmental Research and Public Health, 18(13), 7211. https://doi.org/10.3390/ijerph18137211