
Pharmacists’ Role in Older Adults’ Medication Regimen Complexity: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
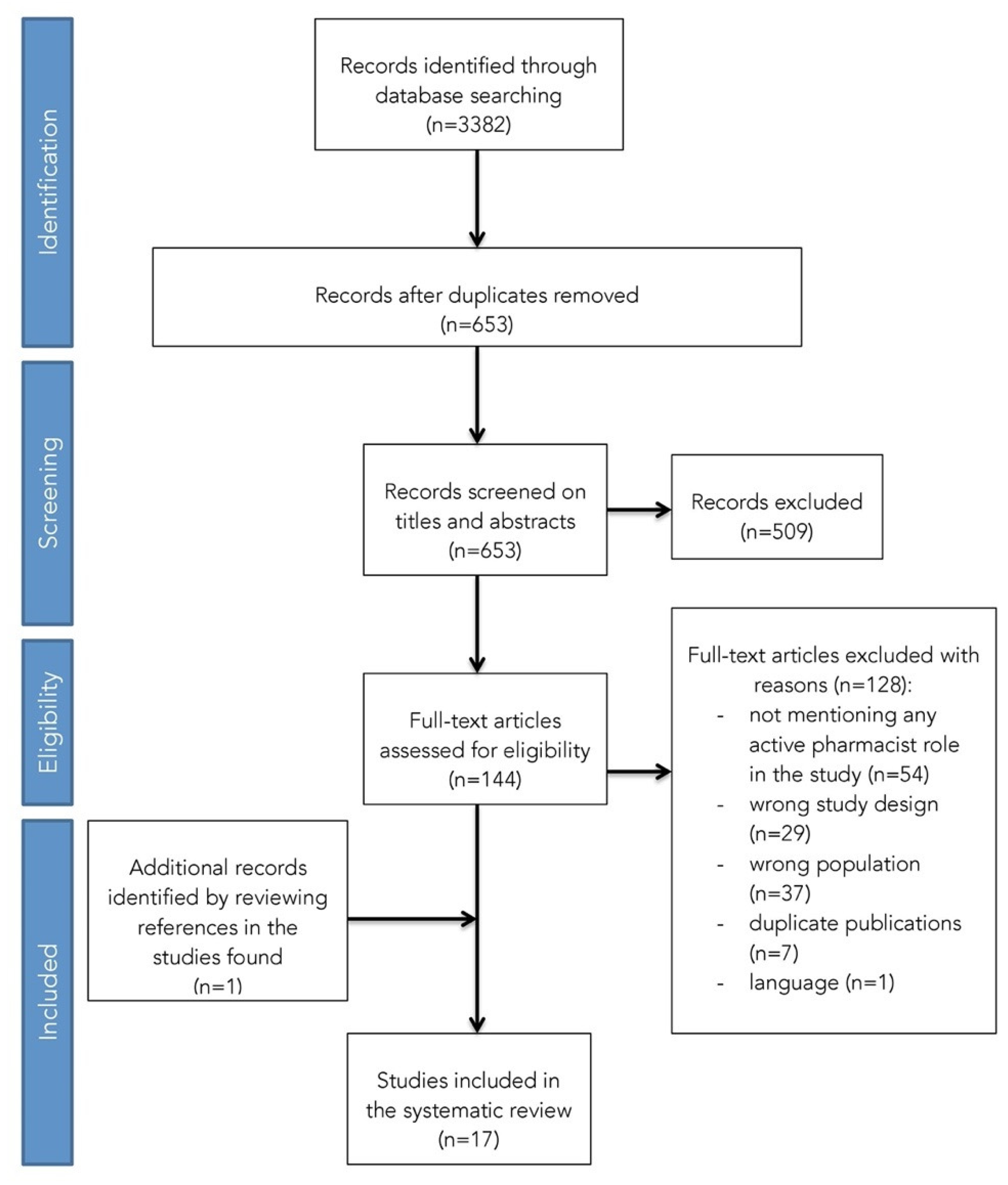
2.2. Study Selection
- all study participants had to be aged 60 or over, since, according to the World Health Organisation (WHO), the definition of older person “varies among countries but is often associated with the age of normal retirement” (60 or 65 years) [27];
- pharmacists’ role in MRC had to be mentioned in the article (for this purpose all pharmacists’ actions were regarded, beginning with simple data collection and ending with pharmacist intervention). Sabater’s et al. [28] definition of pharmacist intervention was considered: “pharmacist intervention is defined as the pharmacist’s activity consisting in a suggested action on the patient treatment and/or an action on the patient oriented towards finding a solution for or preventing a negative clinical outcome of the pharmacotherapy”;
- medication complexity had to be assessed, and for this purpose all tools were considered;
- be an original peer-reviewed observational study (i.e., cohort study, cross-sectional study, case study) or an experimental study (i.e., randomised controlled trial, quasi-experimental study);
- be written in English, Portuguese or German.
- were not performed exclusively on the older population;
- did not mention any role of pharmacists in MRC, or MRC assessment was not performed;
- were qualitative studies, reviews, protocols, congress abstracts, editorials, letters, dissertations, theses, feasibility or pilot studies;
- did not fulfil the language restrictions.
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Study Quality
3.3. Medication Regimen Complexity Assessment
3.4. Pharmacists’ Role on Older People’s Medication Regimen Complexity and Main Outcomes When Intervention Is Performed
4. Discussion
4.1. Medication Regimen Complexity Assessment
4.2. Measured Outcomes
4.3. Study Setting
4.4. Pharmacists’ Role
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; World Health Organization Press: Geneva, Switzerland, 2015. [Google Scholar]
- Advinha, A.M.; De Oliveira-Martins, S.; Mateus, V.; Pajote, S.G.; Lopes, M.J. Medication regimen complexity in institutionalized elderly people in an aging society. Int. J. Clin. Pharm. 2014, 36, 750–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, C.; Ramalho, C.; Luz, I.; Monteiro, J.; Fresco, P. Drug-related problems in institutionalized, polymedicated elderly patients: Opportunities for pharmacist intervention. Int. J. Clin. Pharm. 2015, 37, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Pantuzza, L.L.N.; Ceccato, M.D.G.B.; Silveira, M.R.; Junqueira, L.M.R.; Reis, A. Association between medication regimen complexity and pharmacotherapy adherence: A systematic review. Eur. J. Clin. Pharmacol. 2017, 73, 1475–1489. [Google Scholar] [CrossRef] [PubMed]
- Paquin, A.M.; Zimmerman, K.M.; Kostas, T.R.; Pelletier, L.; Hwang, A.; Simone, M.; Skarf, L.M.; Rudolph, J.L. Complexity perplexity: A systematic review to describe the measurement of medication regimen complexity. Expert Opin. Drug Saf. 2013, 12, 829–840. [Google Scholar] [CrossRef]
- Advinha, A.M.; Lopes, M.; De Oliveira-Martins, S. Assessment of the elderly’s functional ability to manage their medication: A systematic literature review. Int. J. Clin. Pharm. 2016, 39, 1–15. [Google Scholar] [CrossRef]
- Wimmer, B.C.; Johnell, K.; Fastbom, J.; Wiese, M.; Bell, J.S. Factors associated with medication regimen complexity in older people: A cross-sectional population-based study. Eur. J. Clin. Pharmacol. 2015, 71, 1099–1108. [Google Scholar] [CrossRef]
- Herson, M.; Bell, J.; Tan, E.; Emery, T.; Robson, L.; Wimmer, B. Factors associated with medication regimen complexity in residents of long-term care facilities. Eur. Geriatr. Med. 2015, 6, 561–564. [Google Scholar] [CrossRef]
- Ferreira, J.M.; Galato, D.; Melo, A.C. Medication regimen complexity in adults and the elderly in a primary healthcare setting: Determination of high and low complexities. Pharm. Pr. 2015, 13, 659. [Google Scholar] [CrossRef] [Green Version]
- Elliott, R.A.; O’Callaghan, C.J. Impact of Hospitalisation on the Complexity of Older Patients’ Medication Regimens and Potential for Regimen Simplification. J. Pharm. Pr. Res. 2011, 41, 21–25. [Google Scholar] [CrossRef]
- Witticke, D.; Seidling, H.M.; Lohmann, K.; Send, A.F.J.; Haefeli, W.E. Opportunities to Reduce Medication Regimen Complexity: A retrospective analysis of patients discharged from a university hospital in Germany. Drug Saf. 2012, 36, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.A.; O’Callaghan, C.; Paul, E.; George, J. Impact of an intervention to reduce medication regimen complexity for older hospital inpatients. Int. J. Clin. Pharm. 2013, 35, 217–224. [Google Scholar] [CrossRef]
- Stange, D.; Kriston, L.; Von-Wolff, A.; Baehr, M.; Dartsch, D.C. Reducing Cardiovascular Medication Complexity in a German University Hospital: Effects of a Structured Pharmaceutical Management Intervention on Adherence. J. Manag. Care Pharm. 2013, 19, 396–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rettig, S.M.; Wood, Y.; Hirsch, J.D. Medication regimen complexity in patients with uncontrolled hypertension and/or diabetes. J. Am. Pharm. Assoc. 2013, 53, 427–431. [Google Scholar] [CrossRef]
- George, J.; Phun, Y.-T.; Bailey, M.J.; Kong, D.C.; Stewart, K. Development and Validation of the Medication Regimen Complexity Index. Ann. Pharmacother. 2004, 38, 1369–1376. [Google Scholar] [CrossRef]
- Melchiors, A.C.; Correr, C.J.; Fernandez-Llimos, F. Tradução e validação para o português do Medication Regimen Complexity Index. Arq. Bras. Cardiol. 2007, 89, 210–218. [Google Scholar] [CrossRef]
- Stange, D.; Kriston, L.; Langebrake, C.; Cameron, L.K.; Wollacott, J.D.; Baehr, M.; Dartsch, D.C. Development and psychometric evaluation of the German version of the Medication Regimen Complexity Index (MRCI-D). J. Eval. Clin. Pr. 2011, 18, 515–522. [Google Scholar] [CrossRef]
- De La Fuente, J.S.; Díaz, A.S.; Cañamares, I.; Ramila, E.; Izquierdo-Garcia, E.; Esteban, C.; Escobar-Rodríguez, I. Cross-cultural Adaptation and Validation of the Medication Regimen Complexity Index Adapted to Spanish. Ann. Pharmacother. 2016, 50, 918–925. [Google Scholar] [CrossRef]
- Pantuzza, L.L.N.; Ceccato, M.D.G.B.; Silveira, M.R.; Pinto, I.V.; Reis, A. Validation and standardization of the Brazilian version of the Medication Regimen Complexity Index for older adults in primary care. Geriatr. Gerontol. Int. 2018, 18, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, B.C.; Cross, A.J.; Jokanovic, N.; Wiese, M.; George, J.; Johnell, K.; Diug, B.; Bell, J.S. Clinical Outcomes Associated with Medication Regimen Complexity in Older People: A Systematic Review. J. Am. Geriatr. Soc. 2016, 65, 747–753. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.T.; Keers, J.C.; Visser, R.; De Zeeuw, D.; Haaijer-Ruskamp, F.M.; Voorham, J.; Denig, P. Medication beliefs, treatment complexity, and non-adherence to different drug classes in patients with type 2 diabetes. J. Psychosom. Res. 2014, 76, 134–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wimmer, B.C.; Dent, E.; Visvanathan, R.; Wiese, M.; Johnell, K.; Chapman, I.; Bell, J.S. Polypharmacy and Medication Regimen Complexity as Factors Associated with Hospital Discharge Destination Among Older People: A Prospective Cohort Study. Drugs Aging 2014, 31, 623–630. [Google Scholar] [CrossRef]
- Fröhlich, S.E.; Zaccolo, A.V.; Da Silva, S.L.C.; Mengue, S.S. Association between drug prescribing and quality of life in primary care. Pharm. World Sci. 2010, 32, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Center for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; CRD University of York: York, UK, 2009. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization Centre for Health Development. A Glossary of Terms for Community Health Care and Services for Older Persons; WHO Centre for Health Development: Kobe, Japan, 2004; p. 42. Available online: https://apps.who.int/iris/handle/10665/68896 (accessed on 12 November 2019).
- Sabater, D.; Fernandez-Llimos, F.; Parras, M.; Faus, M.J. Tipos de intervenciones farmacéuticas en seguimiento farmacoterapéutico. Types of pharmacist intervention in pharmacotherapy follow-up. Seguim. Farmacoter. 2005, 3, 90–97. [Google Scholar]
- Effective Public Health Practice Project (EPHPP). Quality Assessment Tool for Quantitative Studies. Available online: http://www.ephpp.ca/tools.html (accessed on 20 October 2019).
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Evaluation Clin. Pr. 2010, 18, 12–18. [Google Scholar] [CrossRef]
- Acurcio, F.A.; Silva, A.L.; Ribeiro, A.Q.; Rocha, N.P.; Silveira, M.R.; Klein, C.H.; Rozenfeld, S. Complexidade do regime terapêutico prescrito para idosos. Rev. Assoc. Med. Bras. 2009, 55, 468–474. [Google Scholar] [CrossRef] [Green Version]
- Bazargan, M.; Smith, J.; Yazdanshenas, H.; Movassaghi, M.; Martins, D.; Orum, G. Non-adherence to medication regimens among older African-American adults. BMC Geriatr. 2017, 17, 163. [Google Scholar] [CrossRef]
- Chang, W.T.; Kowalski, S.R.; Sorich, W.; Alderman, C.P. Medication regimen complexity and prevalence of potentially inappropriate medicines in older patients after hospitalisation. Int. J. Clin. Pharm. 2017, 39, 867–873. [Google Scholar] [CrossRef]
- Elliott, R.A. Reducing medication regimen complexity for older patients prior to discharge from hospital: Feasibility and barriers. J. Clin. Pharm. Ther. 2012, 37, 637–642. [Google Scholar] [CrossRef]
- Kroenke, K.; Pinholt, E.M. Reducing polypharmacy in the elderly. a controlled trial of physician feedback. J. Am. Geriatr. Soc. 1990, 38, 31–36. [Google Scholar] [CrossRef]
- Lakey, S.L.; Gray, S.L.; Borson, S. Assessment of Older Adults’ Knowledge of and Preferences for Medication Management Tools and Support Systems. Ann. Pharmacother. 2009, 43, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, L.A.; Lindquist, L.M.; Zickuhr, L.; Friesema, E.; Wolf, M.S. Unnecessary complexity of home medication regimens among seniors. Patient Educ. Couns. 2014, 96, 93–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linnebur, S.A.; Griend, J.P.V.; Metz, K.R.; Hosokawa, P.W.; Hirsch, J.D.; Libby, A.M. Patient-level Medication Regimen Complexity in Older Adults with Depression. Clin. Ther. 2014, 36, 1538–1546.e1. [Google Scholar] [CrossRef]
- Mansur, N.; Weiss, A.; Beloosesky, Y. Looking Beyond Polypharmacy: Quantification of Medication Regimen Complexity in the Elderly. Am. J. Geriatr. Pharmacother. 2012, 10, 223–229. [Google Scholar] [CrossRef]
- Moczygemba, L.R.; Barner, J.C.; Gabrillo, E.R. Outcomes of a Medicare Part D telephone medication therapy management program. J. Am. Pharm. Assoc. 2012, 52, e144–e152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, I.V.L.; Reis, A.; Almeida-Brasil, C.C.; Da Silveira, M.R.; Lima, M.G.; Ceccato, M.D.G.B. Avaliação da compreensão da farmacoterapia entre idosos atendidos na Atenção Primária à Saúde de Belo Horizonte, MG, Brasil. Cien. Saude Colet. 2016, 21, 3469–3481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouranayatihosseinabad, M.; Zaidi, S.T.R.; Peterson, G.; Nishtala, P.S.; Hannan, P.; Castelino, R. The impact of residential medication management reviews (RMMRs) on medication regimen complexity. Postgrad. Med. 2018, 130, 575–579. [Google Scholar] [CrossRef]
- Sevilla-Sánchez, D.; Molist-Brunet, N.; Amblàs-Novellas, J.; Espaulella-Panicot, J.; Codina-Jané, C. Potentially inappropriate medication at hospital admission in patients with palliative care needs. Int. J. Clin. Pharm. 2017, 39, 1018–1030. [Google Scholar] [CrossRef]
- Wimmer, B.C.; Dent, E.; Bell, J.S.; Wiese, M.D.; Chapman, I.; Johnell, K.; Visvanathan, R. Medication Regimen Complexity and Unplanned Hospital Readmissions in Older People. Ann. Pharmacother. 2014, 48, 1120–1128. [Google Scholar] [CrossRef]
- Hirsch, J.D.; Metz, K.R.; Hosokawa, P.W.; Libby, A. Validation of a Patient-Level Medication Regimen Complexity Index as a Possible Tool to Identify Patients for Medication Therapy Management Intervention. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2014, 34, 826–835. [Google Scholar] [CrossRef] [Green Version]
- Libby, A.M.; Fish, D.N.; Hosokawa, P.W.; Linnebur, S.A.; Metz, K.R.; Nair, K.V.; Saseen, J.; Griend, J.P.V.; Vu, S.P.; Hirsch, J.D. Patient-Level Medication Regimen Complexity Across Populations With Chronic Disease. Clin. Ther. 2013, 35, 385–398. [Google Scholar] [CrossRef] [Green Version]
- Alves-Conceição, V.; Rocha, K.S.S.; Silva, F.V.N.; Silva, R.O.S.; Da Silva, D.T.; De Lyra, D.P., Jr. Medication Regimen Complexity Measured by MRCI: A Systematic Review to Identify Health Outcomes. Ann. Pharmacother. 2018, 52, 1117–1134. [Google Scholar] [CrossRef]
- Conn, V.S.; Taylor, S.G.; Kelley, S. Medication Regimen Complexity and Adherence Among Older Adults. Image J. Nurs. Sch. 1991, 23, 231–236. [Google Scholar] [CrossRef]
- Wimmer, B.C.; Bell, J.S.; Fastbom, J.; Wiese, M.; Johnell, K. Medication Regimen Complexity and Polypharmacy as Factors Associated With All-Cause Mortality in Older People: A population-based cohort study. Ann. Pharmacother. 2015, 50, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Kozma, C.M.; Reeder, C.E.; Schultz, R.M. Economic, clinical, and humanistic outcomes: A planning model for pharmacoeconomic research. Clin. Ther. 1993, 15, 1121–1132. [Google Scholar]
- Charrois, T.L.; Durec, T.; Tsuyuki, R.T. Systematic Reviews of Pharmacy Practice Research: Methodologic Issues in Searching, Evaluating, Interpreting, and Disseminating Results. Ann. Pharmacother. 2009, 43, 118–122. [Google Scholar] [CrossRef] [PubMed]
- American Geriatrics Society. American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2014, 44, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, S. The state of the world’s pharmacy: A portrait of the pharmacy profession. J. Interprofessional Care 2002, 16, 391–404. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Country | Study Design | Participants’ Demographics | Setting | Study Aim | ||
|---|---|---|---|---|---|---|---|
| No. of Participants (n) | Mean Age, Years (SD) [Range] | Female | |||||
| Acurcio et al. [31], 2009 | Brazil | Epidemiological cross-sectional | 377 | 72.4 (61–102) | 69.2% | Home visits. | To examine factors associated with therapeutic regimen complexity of drug prescriptions for elderly people. |
| Bazargan et al. [32], 2017 | USA | Cross-sectional study | 400 | 73.5 (7) (65–94) | 65% | Sixteen predominantly African-American churches in SPA6 of Los Angeles County. | To examine the association between adherence to drug regimens and a spectrum of medication-related factors, including polypharmacy, medication regimen complexity, use of PIMs, knowledge about their therapeutic purpose and instructions of proper medication use. |
| Chang et al. [33], 2017 | Australia | Retrospective cohort study | 100 | 82 (9.15) | 60% | General medical units of a tertiary care hospital. | To assess the changes in the MRCI before and after hospitalisation. To examine the prevalence of prescribing PIMs at the time of hospital discharge, using the 2015 Beers Criteria. |
| Elliot [34], 2012 | Australia | Cohort study | 205 | 81.3 (8.0) | 58% | Two acute general medicine wards and two subacute aged care wards at a major metropolitan public hospital. | To explore the feasibility of incorporating medication regimen simplifications into routine clinical pharmacists’ care for older hospital inpatients, and to identify barriers to regimen simplification. |
| Elliot et al. [10], 2011 | Australia | Cohort study | 186 Acute wards: 115 Subacute wards: 71 | Acute wards: 79 (77–80) Subacute wards: 81 (80–83) | Acute wards: 59% Subacute wards: 55% | Two acute general medicine wards and two subacute aged care wards at a large public hospital. | To investigate the impact of hospitalisation on the complexity of older patients’ medication regimens, and to determine whether discharge medication regimens could be simplified. |
| Elliot et al. [12], 2013 | Australia | Cohort study | 391 Pre-intervention: 186 Intervention: 205 | Pre-intervention: 79.7 (8.2) Intervention: 81.3 (8.0) | 57.8% Pre-intervention: 57.5% Intervention: 58.% | Two acute general medicine wards and two subacute aged care wards at a major metropolitan public hospital. | To investigate the impact of pharmacists’ medication reviews, together with an educational intervention targeting inpatient clinical pharmacists and junior medical officers on the increase in medication regimen complexity during hospitalisation. |
| Kroenke et al. [35], 1990 | USA | Prospective controlled trial | 79 Intervention: 38 Control: 41 | Intervention: 72.3 Control: 71.4 | 40.5% Intervention: 39.5% Control: 41.5% | Internal Medicine Clinic at Brooke Army Medical Center. | To determine the effectiveness of specific feedback to prescribing physicians in reducing polypharmacy in elderly outpatients. |
| Lakey et al. [36], 2009 | USA | Cross-sectional | 109 | 85.9 (5.1) (73–98) | 79.8% | Continuing care retirement community in Seattle. | To assess older adults’ current use of, knowledge of and preferences for medication management tools and supports. |
| Lindquist et al. [37], 2014 | USA | Cross-sectional | 200 | 79.6 (6.4) (70–100) | 58% | Home visits after discharge from Northwestern Memorial Hospital. | To determine whether seniors consolidate their home medications or if there is evidence of unnecessary regimen complexity. |
| Linnebur et al. [38], 2014 | USA | Retrospective cross-sectional | 200 CA: 100 CO: 100 | CA: 74.3 (7.4) CO: 79.7 (6.1) | 78.5% CA: 76% CO: 81% | Ambulatory clinics at the University of CA and the University of CO. | To evaluate the entire medication regimen of older adults with depression, and determine potential targets to simplify the regimen and improve adherence. |
| Mansur et al. [39], 2012 | Israel | Cohort study | 212 | 81.1 (7.3) (66–103) | 61.8% | Acute Geriatric Ward at the Beilinson Hospital, Rabin Medical Center. | To test the convergent, discriminant and predictive validity of the MRCI in older hospitalised patients with varying functional and cognitive levels. |
| Moczygemba et al. [40], 2012 | USA | Quasi-experimental | 120 Intervention: 60 Control: 60 | Intervention: 71.2 (7.5) Control: 73.9 (8.0) | 60% Intervention: 48.3% Control: 71.7% | Telephone consultation. | To determine the impact of telephone MTM on MHRPs, medication adherence and total drug costs for Medicare Part D participants. |
| Pinto et al. [41], 2016 | Brazil | Cross-sectional | 227 | 71.4 | 70.9% | Two PHUs in the municipality of Belo Horizonte. | To evaluate the level of understanding of pharmacotherapy and the associated factors amongst older people in two PHUs. |
| Pouranayatihosseinabad et al. [42], 2018 | Australia | Retrospective observational study | 285 | 85.5 (7.7) | 68% | Residential ACFs. | To investigate the impact of RMMRs on simplifying medication regimen complexity in Australian ACF residents using the MRCI. |
| Sevilla-Sánchez et al. [43], 2017 | Spain | Prospective cross-sectional study | 235 | 86.80 (5.37) | 65.50% | AGU in a second-level hospital. | To determine the prevalence of PIMs among patients with advanced chronic conditions and palliative care needs, and to analyse the associated risk factors and resulting clinical consequences. |
| Wimmer et al. [44], 2014 | Australia | Prospective cohort | 163 Readmitted: 99 Not readmitted: 64 | Readmitted: 84.9 (6.2) Not readmitted: 85.6 (6.74) | 72.4% Readmitted: 68.7% Not readmitted: 78.1% | GEM unit of a public hospital in Adelaide. | To investigate the association between discharge medication regimen complexity and unplanned re-hospitalisation over 12 months. |
| Wimmer et al. [22], 2014 | Australia | Prospective cohort | 163 DD home: 87 DD NCS: 76 | 85.2 (6.4) (71–101) DD home: 84.6 (6.9) DD NCS: 85.8 (5.8) | 72.4% DD home: 68.7% DD NCS: 77.6% | GEM unit at the Queen Elizabeth Hospital. | To investigate the association between polypharmacy and medication regimen complexity with hospital discharge destination among older people. |
| Author, Year | Medication Data | Pharmacists’ Role in MRC | Main Outcomes | ||
|---|---|---|---|---|---|
| Source | Type of Medication Included | Instrument to Assess MRC | |||
| Acurcio et al. [31], 2009 | Medical prescription | Prescription medication | MCI | Household data collection, after previous training. | MCI ranged from 1 to 24 (mean = 6.1; median = 5.0). Nr. of drugs prescribed (> 2), less schooling, worse perception of health and lower benefit payment associated positively with greater complexity (p < 0.05). An association was observed between RC and failure to use some drugs in the preceding 15 days (p = 0.34). |
| Bazargan et al. [32], 2017 | The brown bag method | Prescription medication | MRCI | Evaluation of any medication duplication; application of the Beers Criteria to document the number of PIM use; and comparison of subjects perceived purpose of each prescription drug with all therapeutic indications used in clinical practice. | The mean value of the MRCI was 15.1 (SD = 8.2; minimum = 2.5; and maximum = 55.5). Of the participants, 70% (278) engaged in PIM use and used at least one medication that was classified as “Avoid” (27%) and “Use Conditionally” (43%) through the Beers Criteria. Participants with increased knowledge about the therapeutic purpose of the dosage regimen were almost seven times more likely to adhere to their medication. |
| Chang et al. [33], 2017 | Hospital electronic medical record system | Prescription medication | MRCI | Medication history record. | The mean MRCI increased from 28.70 at the time of admission to 32.46 at discharge (p = 0.007). Hospitalisation resulted in a statistically significant reduction in the prevalence of the use of PIMs. |
| Elliot [34], 2012 | Hospital medical record | Long-term, short-term and “when required” medication | Not mentioned | Pharmacists were encouraged to minimise RC and discuss simplifications with hospital doctors and patients. Afterwards, they were asked to indicate if they reviewed the patient’s RC (and why not) and whether regimen changes were considered or attempted. Changes had to be recorded and whether they were successfully implemented (and if not why). | Pharmacists reviewed medication RC for 173/205 (84.4%) patients and identified 149 potential changes to reduce RC for 79/173 (45.7%) reviewed patients. Ninety-four (63.1%) changes were successfully implemented in 54/205 (26.3%) patients. |
| Elliot et al. [10], 2011 | Pre-admission: medication history on admission within the patient’s hospital medical record Discharge: discharge prescription | Long-term, short-term and “when required” medication | MRCI | Review of discharge medication regimens and identification of any potential change that could make the regimen simpler. | MRCI scores increased by 22% (18 to 22; p < 0.0001) for regularly scheduled long-term medications and 32% (21 to 27; p < 0.001) for all medications. Ninety simplifications to regularly long-term medications were proposed and 84 (93%) were rated as feasible and likely to have the same or similar outcome. |
| Elliot et al. [12], 2013 | Pre-admission: hospital medical record Discharge: discharge prescription | Long-term, short-term and “when required” medication | MRCI | Clinical pharmacists were encouraged to review RC and make recommendations to hospital medical officers to simplify medication regimens when clinically appropriate. | MRCI score for all medications: pre-intervention patients = 20.7 (SD = 12.5); intervention patients = 21.7 (SD = 11.6). MRCI score for all regularly scheduled long-term medication: pre-intervention patients = 18.2 (SD = 11.2); intervention patients = 19.1 (SD = 10.3). The mean increase in MRCI score between admission and discharge was significantly smaller in the intervention patients than in the usual care patients (2.5 vs. 4.0; p = 0.02, adjusted difference 1.6; 95% CI 0.3, 2.9). |
| Kroenke et al. [35], 1990 | Patients were asked to bring all prescription bottles to the interview, where medications were used regularly and the dosage schedules were confirmed | Prescription medication | A complexity score was calculated by summing the different dosage intervals, weighted for frequency | A clinical pharmacist interviewed patients to determine the precise drug regimen. Investigating physicians discussed and agreed upon recommendations that might reduce polypharmacy. | All four indices of polypharmacy improved in the intervention group (7.2 vs. 6.6; p = 0.007). Physicians complied 100% with recommendations to simplify a dosage schedule, 62% to substitute a new drug for the old one and only 40% with recommendations to stop a medication (p = 0.04). |
| Lakey et al. [36], 2009 | Participants were asked to show containers for all medication taken in the week before | Prescription medication, non-prescription medication and herbal products | The frequency of dosing for each medication was summed to calculate a complexity score | The investigating pharmacist performed data collection. | Medication complexity score: only for prescription drugs = 5.0 ± 3.8; total = 8.3 ± 4.4. |
| Lindquist et al. [37], 2014 | Subjects were asked to show how they take their medication on a typical day and all medications were registered and compared to discharge instructions | Medication subjects take a day | The number of times medications were taken in a 24 h period for each subject was calculated | A pharmacist acted as one of two coders, determining the fewest number of times a day that a patient could take the regimen. | Home medication regimens could be simplified for 85 (42.5%) subjects. |
| Linnebur et al. [38], 2014 | Electronic health record | Depression medications, other prescription medications and over-the-counter (OTC) medications | MRCI/patient-level MRCI (pMRCI) | A clinical pharmacist coded the pMRCI using an electronic data capture tool that calculated three subscores. | Individual pMRCI scores average: 17.62 (CA) and 19.36 (CO). Dosing frequency contributed to 57–58% of the MRCI score, with patients facing an average of 7–8 unique dosing frequencies in their regimen. |
| Mansur et al. [39], 2012 | Patient interview on admission. Retrospectively, patients’ medical files were reviewed to calculate their MRCI score for discharge medication regimens | Long-term discharge medication | MRCI | The pharmacist interviewed the patients to collect clinical and demographical data as well as patients’ medication on admission. | Mean (SD) MRCI at discharge: 30.27 (13.95). The MRCI score was strongly correlated with the number of medications (r = 0.94; p < 0.001) and the number of daily doses (r = 0.87; p < 0.001), and increased as the number of medications taken ≥ 3 times a day increased (27.35; 34.45 and 43.00 for none, 1 and 2 drugs; p < 0.001). |
| Moczygemba et al. [40], 2012 | Electronic medical records and prescription claims | Prescription medication | MRCI | Pharmacists reviewed the patient’s electronic medical records to identify potential MHRPs. Furtherly, in the intervention group, an MTM telephone consultation was made and recommendations were given to the patient to resolve MHRPs. | MRCI intervention group: 21.5 ± 7.8. MRCI control group: 22.8 ± 6.9. |
| Pinto et al. [41], 2016 | Prescribed medication that each individual had in his hand at the time of the interview | Prescription medication | MRCI | Resident pharmacists and academics studying pharmacy were part of the team carrying out data collection. | Mean value of the rate of complexity: 22.7 (DP = 10.9; CV = 48.0%), with a minimum of 4.0 and a maximum of 65.5. |
| Pouranayatihosseinabad et al. [42], 2018 | RMMR report | Prescription medication | MRCI | Accredited pharmacists compiled RMMR reports, which included pharmacists’ findings and recommendations. | The median MRCI at baseline was 25.5 (19.0–32.5). The main contributing factor to the MRCI score was dosing frequency. Pharmacists made 764 recommendations, of which GPs accepted 74.5%. There were no significant differences in the MRCI scores after pharmacists’ recommendations (p = 0.53) or after GPs’ acceptance of these recommendations (p = 0.07) compared to baseline. |
| Sevilla-Sánchez et al. [43], 2017 | Not mentioned | Routine chronic medication | MRCI | A multidisciplinary team consisting of a pharmacist and two physicians determined the PIMs. | MRCI (mean; SD) = 38.00 (16.54). Of the population, 88.50% had at least one STOPP criterion and 97.40% had some criterion according to the MAI criteria. The identified risk factors for the existence of PIMs were: insomnia, anxiety–depressive disorders, falls, pain, excessive polypharmacy and therapeutic complexity. |
| Wimmer et al. [44], 2014 | Hospital separation summary recorded in the OACIS | All prescription and non-prescription medications, nutritional supplements, health products, dermatological preparations and short-term medications were considered | MRCI | The same pharmacist researcher extracted all medication data. | Mean MRCI for: - discharged patients: 27.86 (SD = 11.63) - readmitted: 28.01 (SD = 12.48) - not readmitted: 27.62 (SD = 10.26). The MRCI was not significantly different in patients who were readmitted and not readmitted over 12 months (mean difference = −0.39; 95% CI = −4.09 to 3.30). |
| Wimmer et al. [22], 2014 | Hospital separation summary recorded in OACIS | Prescription, non-prescription and CAMs | MRCI | The same pharmacist researcher extracted all medication data. | Patients discharged directly to home: mean MRCI = 26.1; SD 9.7. Patients discharged to NCSs: mean MRCI = 29.9; SD 9.7. High medication RC (MRCI > 35) inversely associated with discharge directly to home (RR 0.39; 95% CI 0.20–0.73). Polypharmacy (≥ 9 medications) not significantly associated with discharge directly to home (RR 0.97; 95% CI 0.53–1.58). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falch, C.; Alves, G. Pharmacists’ Role in Older Adults’ Medication Regimen Complexity: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8824. https://doi.org/10.3390/ijerph18168824
Falch C, Alves G. Pharmacists’ Role in Older Adults’ Medication Regimen Complexity: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8824. https://doi.org/10.3390/ijerph18168824
Chicago/Turabian StyleFalch, Catharine, and Gilberto Alves. 2021. "Pharmacists’ Role in Older Adults’ Medication Regimen Complexity: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8824. https://doi.org/10.3390/ijerph18168824
APA StyleFalch, C., & Alves, G. (2021). Pharmacists’ Role in Older Adults’ Medication Regimen Complexity: A Systematic Review. International Journal of Environmental Research and Public Health, 18(16), 8824. https://doi.org/10.3390/ijerph18168824