
A Comprehensive Descriptive Epidemiological and Clinical Analysis of SARS-CoV-2 in West-Mexico during COVID-19 Pandemic 2020

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Epidemiological Surveillance by RT-PCR for SARS-CoV-2 Detection
2.3. Statistical Analysis
3. Results
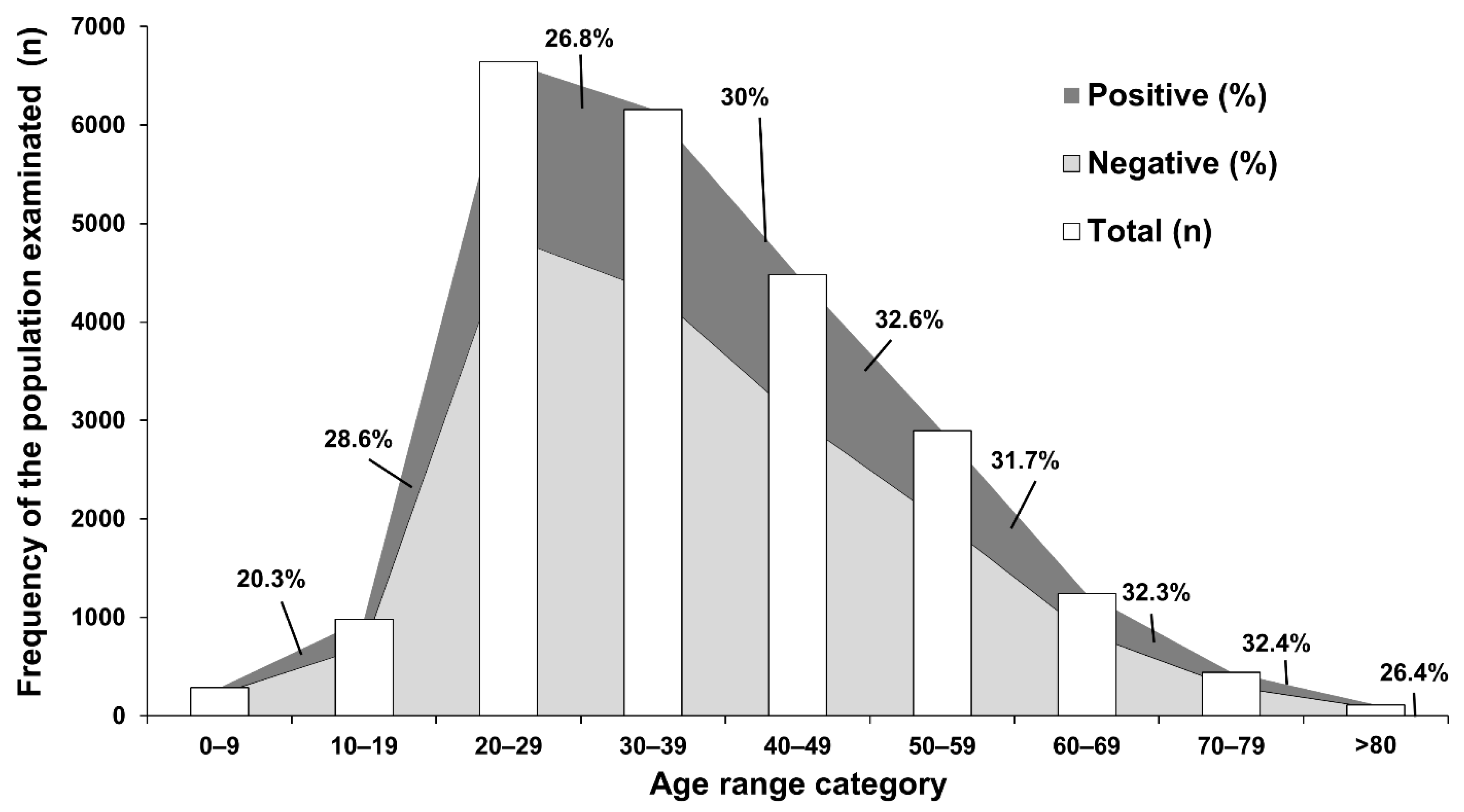
3.1. Demographic Information, Underlying Diseases and Travel History of the Overall Population
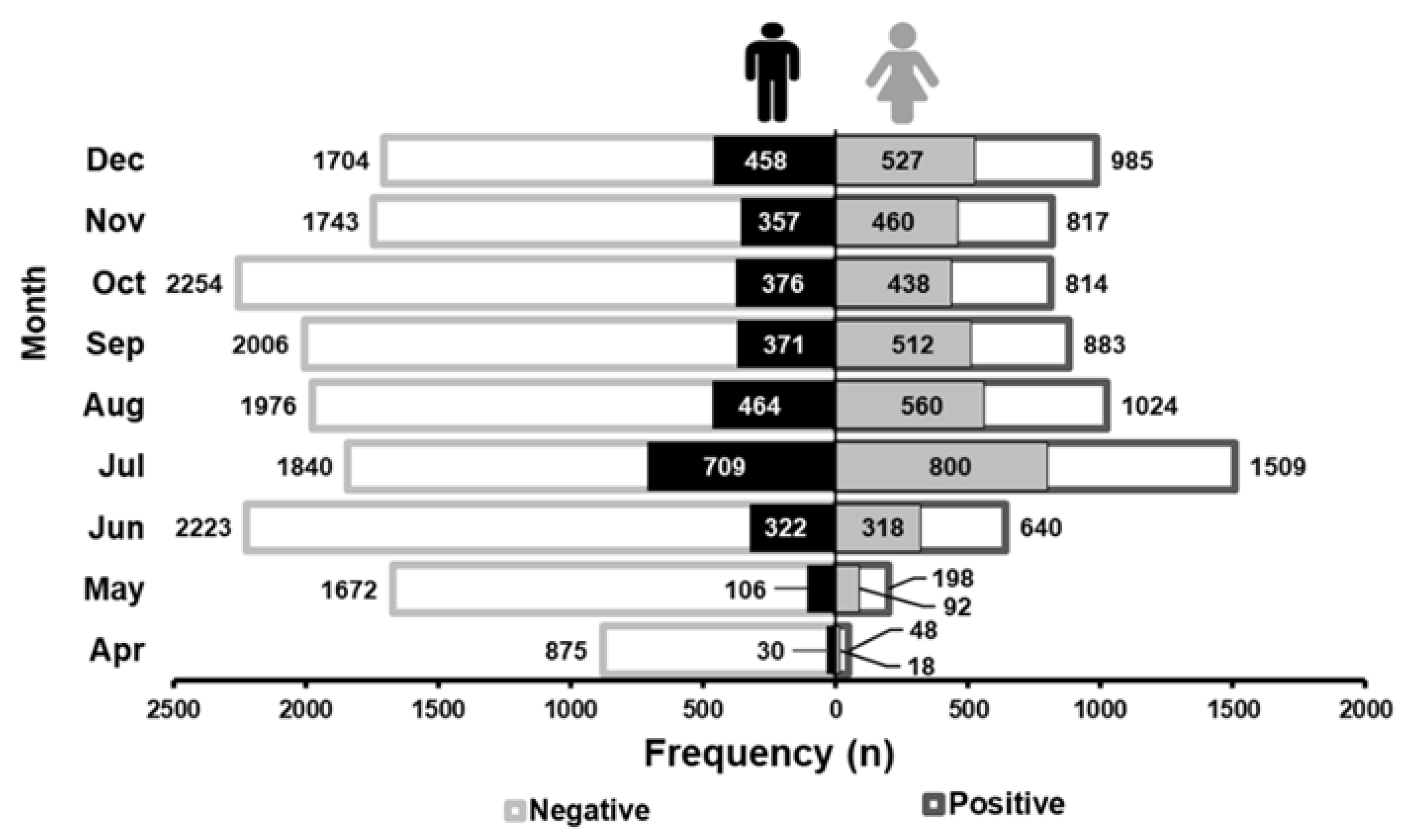
3.2. SARS-CoV-2 Distribution during 2020
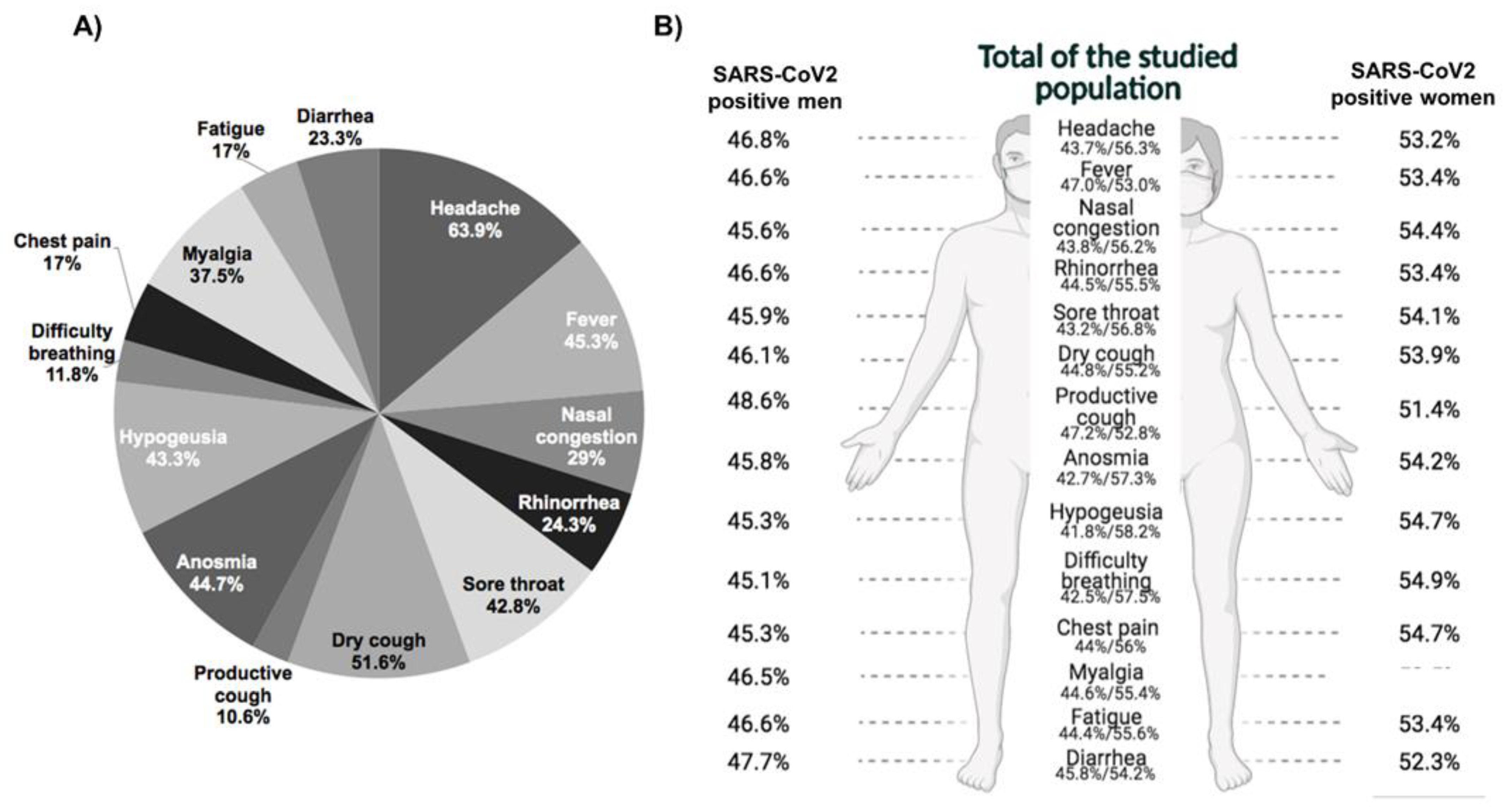
3.3. Symptoms Frequency Description in the Studied Population
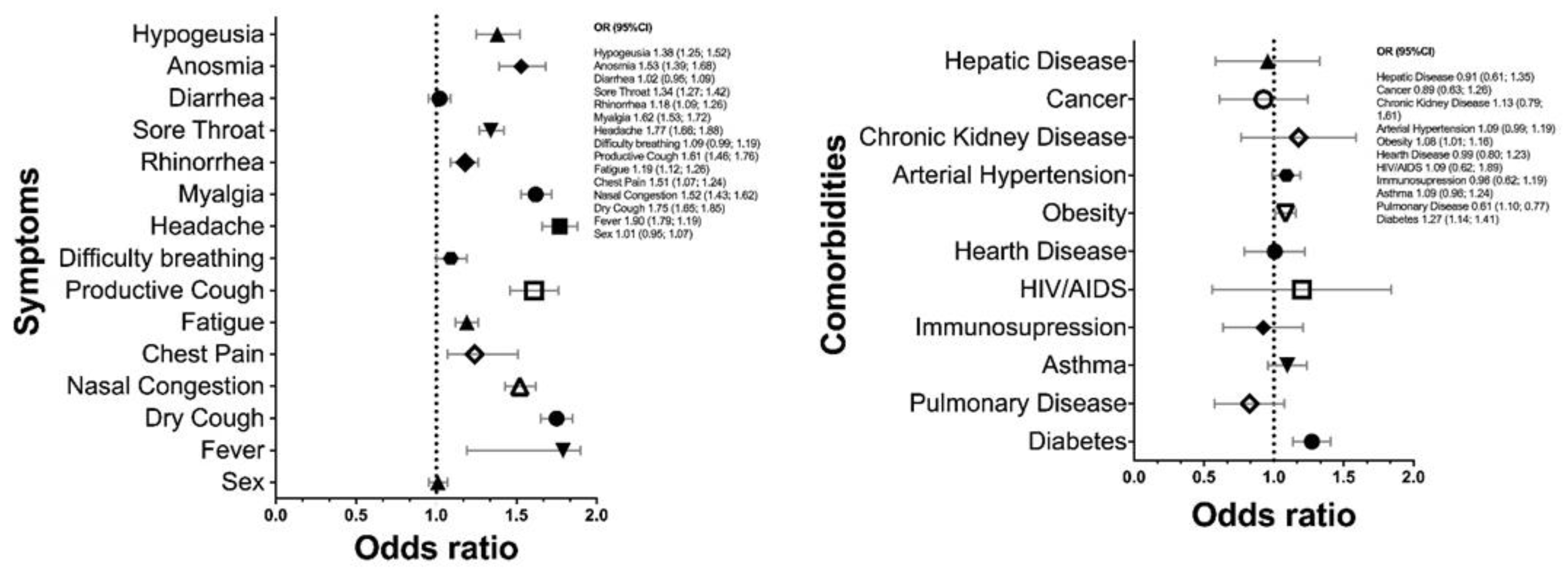
3.4. Association of Demographic Data, Underlying Diseases and SARS-CoV-2 Positive Diagnosis with Symptomatology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Map. Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 3 September 2021).
- Garcés-Ayala, F.; Araiza-Rodríguez, A.; Mendieta-Condado, E.; Rodríguez-Maldonado, A.P.; Wong-Arámbula, C.; Landa-Flores, M.; Mazo-López, J.C.; González-Villa, M.; Escobar-Escamilla, N.; Fragoso-Fonsecaet, D.E.; et al. Full genome sequence of the first SARS-CoV-2 detected in Mexico. Arch. Virol. 2020, 165, 2095–2098. [Google Scholar] [CrossRef]
- Confirma Jalisco los Primeros dos Casos de COVID-19. Secretaría de Salud. Available online: https://ssj.jalisco.gob.mx/prensa/noticia/8920 (accessed on 15 May 2021).
- CDC. Coronavirus Disease 2019 (COVID-19)—Symptoms. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 8 June 2021).
- Dolan, M.E.; Hill, D.P.; Mukherjee, G.; McAndrews, M.S.; Chesler, E.J.; Blake, J.A. Investigation of COVID-19 comorbidities reveals genes and pathways coincident with the SARS-CoV-2 viral disease. Sci. Rep. 2020, 10, 20848. [Google Scholar] [CrossRef]
- Encuesta Nacional de Salud y Nutrición. ENSANUT. Available online: https://ensanut.insp.mx/encuestas/ensanut2018/index.php (accessed on 9 April 2021).
- Enfermedades Cardiovasculares, Principal Causa de Muerte Entre los Mexicanos|Asociación Ale. Available online: https://asociacionale.org.mx/enfermedades-cardiovasculares-principal-causa-de-muerte-entre-los-mexicanos/ (accessed on 9 April 2021).
- Muralidar, S.; Ambi, S.V.; Sekaran, S.; Krishnan, U.M. The emergence of COVID-19 as a global pandemic: Understanding the epidemiology, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie 2020, 179, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus. Conoce Todo lo Que Debes Saber. Available online: https://coronavirus.jalisco.gob.mx/ (accessed on 10 June 2021).
- INEGI. Available online: https://www.inegi.org.mx/ (accessed on 12 June 2021).
- COVID-19 Tablero. CONACyT. Available online: https://datos.covid-19.conacyt.mx/index.php (accessed on 3 September 2021).
- Informes de Movilidad Local Sobre el COVID-19. GOOGLE. Available online: https://www.google.com/covid19/mobility/ (accessed on 31 August 2021).
- The COVID-19 Sex-Disaggregated Data Tracker. Global Health 50/50. Available online: https://globalhealth5050.org/the-sex-gender-and-covid-19-project/the-data-tracker/ (accessed on 21 June 2021).
- Rashedi, J.; Poor, B.M.; Asgharzadeh, V.; Pourostadi, M.; Kafil, H.S.; Vegari, A.; Tayebi-Khosroshahi, H.; Asgharzadeh, M. Risk Factors for COVID-19. Infez Med. 2020, 28, 469–474. [Google Scholar]
- IMCO. Evidencia de las Afectaciones Económicas del COVID-19 en la Mujer. Available online: https://imco.org.mx/evidencia-de-las-afectaciones-economicas-del-covid-19-en-la-mujer/ (accessed on 30 April 2021).
- Jalisco Registra Baja en Empleos en Mujeres Tras COVID-19. Available online: https://www.milenio.com/politica/comunidad/jalisco-registra-baja-empleos-mujeres-covid-19 (accessed on 30 April 2021).
- COVID-19 Impact on Women and Gender Equality. Available online: https://www.mckinsey.com/featured-insights/future-of-work/covid-19-and-gender-equality-countering-the-regressive-effects# (accessed on 30 April 2021).
- Suárez, V.; Suarez-Quezada, M.; Oros-Ruiz, S.; Ronquillo De Jesús, E. Epidemiology of COVID-19 in Mexico: From the 27th of February to the 30th of April 2020. Rev. Clin. Esp. 2020, 220, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Rojas, M.A.; Luna-Ruiz Esparza, M.A.; Campos-Romero, A.; Calva-Espinosa, D.Y.; Moreno-Camacho, J.L.; Langle-Martínez, A.P.; García-Gil, A.; Solís-González, C.J.; Canizalez-Román, A.; León-Scairos, N.; et al. Epidemiology of COVID-19 in Mexico: Symptomatic profiles and presymptomatic people. Int. J. Infect. Dis. 2021, 104, 572–579. [Google Scholar] [CrossRef]
- Salinas-Escudero, G.; Carrillo-Vega, M.F.; Granados-García, V.; Martínez-Valverde, S.; Toledano-Toledano, F.; Garduño-Espinosa, J. A survival analysis of COVID-19 in the Mexican population. BMC Public Health 2020, 20, 1616. [Google Scholar] [CrossRef]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; CMMID COVID-19 Working Group; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus. Available online: https://www.who.int/westernpacific/health-topics/coronavirus (accessed on 11 March 2021).
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- da Rosa-Mesquita, R.; Francelino-Silva, J.L.C.; Santos-Santana, F.M.; Farias de Oliveira, T.; Campos-Alcántara, R.; Monteiro-Arnozo, G.; da Silva-Filho, E.R.; Galdino-dos Santos, A.G.; Oliveira-da Cunha, E.J.; Salgueiro-de Aquino, S.H.; et al. Clinical manifestations of COVID-19 in the general population: Systematic review. Wien. Klin. Wochenschr. 2020, 133, 1–6. [Google Scholar]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.; Chai, P.S.; Chong, M.Y.; Tohit, E.R.M.; Ramasamy, R.; Pei, C.P.; Vidyadaran, S. Gender effect on in vitro lymphocyte subset levels of healthy individuals. Cell Immunol. 2012, 272, 214–219. [Google Scholar] [CrossRef]
- Berghöfer, B.; Frommer, T.; Haley, G.; Fink, L.; Bein, G.; Hackstein, H. TLR7 Ligands Induce Higher IFN-α Production in Females. J. Immunol. 2006, 177, 2088–2096. [Google Scholar] [CrossRef] [Green Version]
- Laffont, S.; Rouquié, N.; Azar, P.; Seillet, C.; Plumas, J.; Aspord, C.; Guéry, J.C. X-Chromosome complement and estrogen receptor signaling independently contribute to the enhanced TLR7-mediated IFN-α production of plasmacytoid dendritic cells from women. J. Immunol. 2014, 193, 5444–5452. [Google Scholar] [CrossRef] [Green Version]
- Hewagama, A.; Patel, D.; Yarlagadda, S.; Strickland, F.M.; Richardson, B.C. Stronger inflammatory/cytotoxic T-cell response in women identified by microarray analysis. Genes Immun. 2009, 10, 509–516. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Federación Mexicana de Diabetes. Available online: http://fmdiabetes.org/ (accessed on 30 April 2021).
- Ng, W.H.; Tipih, T.; Makoah, N.A.; Vermeulen, J.G.; Goedhals, D.; Sempa, J.B.; Burt, F.J.; Taylor, A.; Mahalingam, S. Comorbidities in SARS-CoV-2 Patients: A Systematic Review and Meta-Analysis. mBio 2021, 12, e03647-20. [Google Scholar] [CrossRef]
- Callender, L.A.; Curran, M.; Bates, S.M.; Mairesse, M.; Weigandt, J.; Betts, C.J. The Impact of Pre-existing Comorbidities and Therapeutic Interventions on COVID-19. Front. Immunol. 2020, 11, 1991. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n (%) | SARS-CoV-2 Negative n (%) | SARS-CoV-2 Positive n (%) | p-Value | |
|---|---|---|---|---|
| n (%) | 23,211 | 16,293 (70.2%) | 6918 (29.8%) | <0.001 |
| Age (mean ± SD) | 37.4 ± 14.2 | 37.0 ± 14.2 | 38.4 ± 13.9 | NS |
| Sex | NS | |||
| Male | 10,761 (46.4%) | 7568 (70.3%) | 3193 (29.7%) | <0.001 |
| Female | 12,450 (53.6%) | 8725 (70.1%) | 3725 (29.9%) | <0.001 |
| Economic Activity | <0.001 | |||
| No data | 12,515 (53.7%) | 8520 (68.1%) | 3995 (31.9%) | <0.001 |
| Primary | 17 (0.1%) | 13 (76.5%) | 4 (23.5%) | 0.029 |
| Secondary | 149 (0.8%) | 110 (73.8%) | 39 (26.2%) | <0.001 |
| Tertiary | 10,530 (45.4%) | 7650 (72.7%) | 2880 (27.4%) | <0.001 |
| Underlying Disease | 10,220 (52.4%) | 7376 (72.2%) | 2844 (27.8%) | <0.001 |
| Diabetes | 1622 (7%) | 1059 (65.3%) | 563 (34.7%) | <0.001 |
| Pulmonary disease | 135 (0.6%) | 92 (68.2%) | 43 (31.9%) | <0.001 |
| Asthma | 1209 (5.2%) | 819 (67.7%) | 390 (32.3%) | <0.001 |
| Immunosuppression | 183 (0.8%) | 132 (72.1%) | 51 (27.9%) | <0.001 |
| HIV/AIDS | 57 (0.2%) | 39 (68.42%) | 18 (31.6%) | <0.001 |
| Hearth disease | 417 (1.8%) | 296 (71%) | 121 (29.0%) | <0.001 |
| Obesity | 4495 (19.4%) | 3095 (68.9%) | 1400 (31.2%) | <0.001 |
| Arterial hypertension | 2452 (10.6%) | 1673 (68.2%) | 779 (31.8%) | <0.001 |
| Chronic kidney disease | 136 (0.6%) | 92 (67.7%) | 44 (32.4%) | <0.001 |
| Cancer | 155 (0.8%) | 110 (71%) | 45 (29%) | <0.001 |
| Hepatic disease | 122 (0.5%) | 89 (73%) | 33 (27%) | <0.001 |
| Travel history | 1567 (6.7%) | |||
| National | 1493 (95.3%) | 1471 (98.5%) | 22 (1.5%) | <0.001 |
| International | 74 (4.7%) | 74 (100.00%) | - | |
| North America | 56 (3.6%) | 56 (100.00%) | - | |
| South America | 1 (0.1%) | 1 (100.00%) | - | |
| Europe | 14 (0.9%) | 14 (100.00%) | - | |
| Asia | 2 (0.1%) | 2 (100.00%) | - | |
| Oceania | 1 (0.1%) | 1 (100.00%) | - |
| Total (n = 23,211) n (%) | SARS-CoV-2 Negative n (%) | SARS-CoV-2 Positive n (%) | p-Value | |
|---|---|---|---|---|
| Asymptomatic | 4051 (17.5%) | 3515 (86.8%) | 536 (13.2%) | <0.001 |
| Headache | 14,825 (63.9%) | 9811 (66.2%) | 5014 (33.8%) | <0.001 |
| Fever | 10,513 (45.3%) | 6630 (63.1%) | 3883 (36.9%) | <0.001 |
| Nasal congestion | 6722 (29%) | 4301 (64%) | 2421 (36%) | <0.001 |
| Rhinorrhea | 4729 (24.3%) | 3118 (65.9%) | 1611 (34.1%) | <0.001 |
| Sore throat | 9936 (42.8%) | 6623 (66.7%) | 3313 (33.3%) | <0.001 |
| Dry cough | 11,986 (51.6%) | 7751 (64.7%) | 4235 (35.3%) | <0.001 |
| Productive cough | 2061 (10.6%) | 1214 (58.9%) | 847 (41.1%) | <0.001 |
| Anosmia | 3467 (44.7%) | 2131 (61.5%) | 1336 (38.5%) | <0.001 |
| Dysgeusia | 3361 (43.3%) | 2104 (62.6%) | 1257 (37.4%) | <0.001 |
| Difficulty breathing | 2731 (11.8%) | 1876 (68.7%) | 855 (31.3%) | <0.001 |
| Chest pain | 3941 (17%) | 2677 (67.9%) | 1264 (32.1%) | <0.001 |
| Muscle pain | 8703 (37.5%) | 5555 (63.8%) | 3148 (36.2%) | <0.001 |
| Fatigue | 10,983 (56.5%) | 7361 (67.1%) | 3622 (33%) | <0.001 |
| Diarrhea | 5402 (23.3%) | 3795 (70.3%) | 1607 (29.8%) | <0.001 |
| Asymptomatic n (%) | 1–3 Symptoms n (%) | 4–5 Symptoms n (%) | >6 Symptoms n (%) | p-Value | OR (IC 95%) | |
|---|---|---|---|---|---|---|
| Age (>60) | 14 (2.6%) | 144 (10.1%) | 242 (9.5%) | 174 (7.3%) | <0.001 | 3.59 (2.10–6.14) |
| Age range | <0.001 | 1.10 (1.04–1.18) | ||||
| 0–9 | 73 (1.8%) | 90 (1.8%) | 76 (1.0%) | 47 (0.7%) | ||
| 10–19 | 137 (3.4%) | 216 (4.4%) | 343 (4.7%) | 283 (4.2%) | <0.001 | 4.92 (2.27–10.70) |
| 20–29 | 1164 (28.7%) | 1378 (27.7%) | 2099 (28.5%) | 1995 (29.3%) | <0.001 | 4.48 (2.39–8.41) |
| 30–39 | 1331 (32.7%) | 1222 (24.6%) | 1853 (25.1%) | 1740 (25.5%) | <0.001 | 2.96 (1.59–5.52) |
| 40–49 | 818 (20.2%) | 924 (18.6%) | 1384 (18.8%) | 1350 (19.8%) | <0.001 | 3.34 (1.78–6.26) |
| 50–59 | 375 (9.3%) | 633 (12.7%) | 972 (13.2%) | 914 (13.4%) | <0.001 | 4.04 (2.11–7.75) |
| 60–69 | 113 (2.8%) | 346 (7%) | 437 (5.9%) | 343 (5%) | <0.001 | 11.25 (4.81–26.30) |
| 70–79 | 30 (0.7%) | 121 (2.4%) | 173 (2.4%) | 121 (1.8%) | <0.001 | 22.75 (4.98–103.98) |
| >80 | 10 (0.2%) | 37 (0.7%) | 37 (0.5%) | 26 (0.4%) | <0.001 | 8.91 (1.11–71.55) |
| Sex | 536 (7.75%) | – | – | – | 0.194 | 0.89 (0.74–1.06) |
| No. of comorbidities | 0.619 | 1.08 (0.079–1.46) | ||||
| 0 | 103 (19.2%) | 748 (52.5%) | 1363 (53.2%) | 1310 (54.7%) | ||
| 1–3 | 54 (10.1%) | 519 (36.4%) | 1025 (40%) | 958 (40%) | 0.12 | 1.396 (0.85–1.95) |
| >4 | 379 (70.7%) | 158 (11.1%) | 173 (6.8%) | 128 (5.3%) | 0.16 | 0.36 (0.029–1.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viera-Segura, O.; Vega-Magaña, N.; García-Chagollán, M.; Peña-Rodríguez, M.; Muñoz-Sánchez, G.; Carranza-Aranda, A.S.; Llamas-Covarrubias, I.M.; Ramos-Solano, M.; Mora-Mora, J.; Díaz-Palomera, C.D.; et al. A Comprehensive Descriptive Epidemiological and Clinical Analysis of SARS-CoV-2 in West-Mexico during COVID-19 Pandemic 2020. Int. J. Environ. Res. Public Health 2021, 18, 10644. https://doi.org/10.3390/ijerph182010644
Viera-Segura O, Vega-Magaña N, García-Chagollán M, Peña-Rodríguez M, Muñoz-Sánchez G, Carranza-Aranda AS, Llamas-Covarrubias IM, Ramos-Solano M, Mora-Mora J, Díaz-Palomera CD, et al. A Comprehensive Descriptive Epidemiological and Clinical Analysis of SARS-CoV-2 in West-Mexico during COVID-19 Pandemic 2020. International Journal of Environmental Research and Public Health. 2021; 18(20):10644. https://doi.org/10.3390/ijerph182010644
Chicago/Turabian StyleViera-Segura, Oliver, Natali Vega-Magaña, Mariel García-Chagollán, Marcela Peña-Rodríguez, Germán Muñoz-Sánchez, Ahtziri Socorro Carranza-Aranda, Iris Monserrat Llamas-Covarrubias, Moisés Ramos-Solano, Jesús Mora-Mora, Carlos Daniel Díaz-Palomera, and et al. 2021. "A Comprehensive Descriptive Epidemiological and Clinical Analysis of SARS-CoV-2 in West-Mexico during COVID-19 Pandemic 2020" International Journal of Environmental Research and Public Health 18, no. 20: 10644. https://doi.org/10.3390/ijerph182010644
APA StyleViera-Segura, O., Vega-Magaña, N., García-Chagollán, M., Peña-Rodríguez, M., Muñoz-Sánchez, G., Carranza-Aranda, A. S., Llamas-Covarrubias, I. M., Ramos-Solano, M., Mora-Mora, J., Díaz-Palomera, C. D., León, G. E. -D., Zepeda-Nuño, J. S., Santillán-López, E., García-Arellano, S., Hernández-Silva, C. D., Zerpa-Hernandez, D. A., Muñoz-Rios, G., Rodríguez-Sanabria, J. S., & Muñoz-Valle, J. F. (2021). A Comprehensive Descriptive Epidemiological and Clinical Analysis of SARS-CoV-2 in West-Mexico during COVID-19 Pandemic 2020. International Journal of Environmental Research and Public Health, 18(20), 10644. https://doi.org/10.3390/ijerph182010644