
Health Impact and Risk Factors Affecting South and Southeast Asian Women Following Natural Disasters: A Systematic Review


Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. Protocol and Registration
2.2. Inclusion Criteria
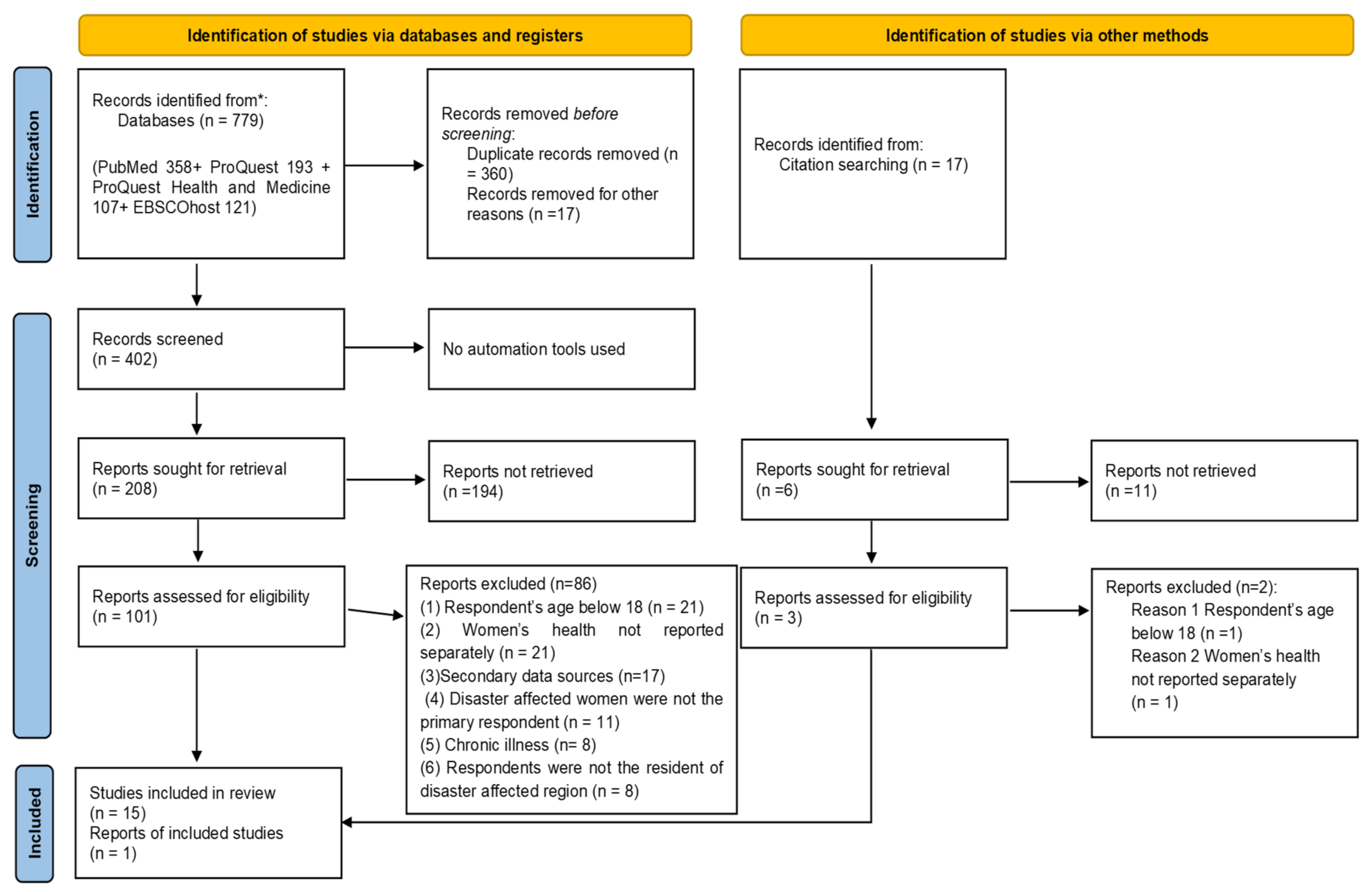
2.3. Search Strategy
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis
3. Systematic Review Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Mixed Method Synthesis
3.4. Health Impact of Natural Disasters on Women
3.4.1. Physical Health Outcomes
3.4.2. Mental Health Outcomes
3.4.3. Post-Traumatic Stress Disorder (PTSD)
3.5. Risk Factors Affecting Women’s Health Following Natural Disasters
3.5.1. Socio-Demographic Risk Factors
3.5.2. Disaster Exposure
3.5.3. Post-Disaster Risk Factors
3.5.4. Pre-Existing Risk Factors
3.6. Association between Physical and Mental Health
4. Discussion
4.1. Policy Implication
4.2. Clinical Implications
5. Conclusions
5.1. Limitations
5.2. Recommendation for Future Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Altmaier, E.M. Promoting Positive Processes After Trauma; Academic Press: Cambridge, UK, 2019. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Gender and Health in Natural Disasters. 2005. Available online: http://www.who.int/gender/gwhgendernd2.pdf (accessed on 15 March 2021).
- Centre for Research on the Epidemiology of Disasters (CRED), UN Office for Disaster Risk Reduction. Human Cost of Disasters: An Overview of the Last 20 Years 2000–2019. 2020. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/Human%20Cost%20of%20Disasters%202000-2019%20Report%20-%20UN%20Office%20for%20Disaster%20Risk%20Reduction.pdf (accessed on 19 May 2021).
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Capstick, S.; et al. The 2019 report of The Lancet Countdown on health and climate change: Ensuring that the health of a child born today is not defined by a changing climate. Lancet 2019, 394, 1836–1878. [Google Scholar] [CrossRef] [Green Version]
- Thurston, A.M.; Stöckl, H.; Ranganathan, M. Natural hazards, disasters and violence against women and girls: A global mixed-methods systematic review. BMJ Glob. Health 2021, 6, e004377. [Google Scholar] [CrossRef] [PubMed]
- United Nations Development Programme (UNDP). Gender and Disaster Risk Reduction; UNDP: New York, NY, USA, 2013. [Google Scholar]
- Neumayer, E.; Plümper, T. The Gendered Nature of Natural Disasters: The Impact of Catastrophic Events on the Gender Gap in Life Expectancy, 1981–2002. Ann. Assoc. Am. Geogr. 2007, 97, 551–566. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.S. Climate change, disaster and gender vulnerability: A study on two divisions of Bangladesh. Am. J. Hum. Ecol. 2013, 2, 72–82. [Google Scholar] [CrossRef] [Green Version]
- Alam, K.; Rahman, M.H. Women in natural disasters: A case study from southern coastal region of Bangladesh. Int J. Disaster Risk. Reduct. 2014, 8, 68–82. [Google Scholar] [CrossRef]
- Goodman, A. In the Aftermath of Disasters: The Impact on Women’s Health. Crit. Care Obstet. Gynecol. 2016, 2, 29. [Google Scholar] [CrossRef] [Green Version]
- Sohrabizadeh, S.; Tourani, S.; Khankeh, H.R. Women and health consequences of natural disasters: Challenge or opportunity? Women Health 2016, 56, 977–993. [Google Scholar] [CrossRef] [PubMed]
- Fatema, S.R. Women’s health-related vulnerabilities in natural disaster-affected areas of Bangladesh: A mixed-methods study protocol. BMJ Open 2020, 10, e039772. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Definition of Health. In Official Records of the World Health Organization; WHO: Geneva, Switzerland, 1948. [Google Scholar]
- World Health Organization. Mental Health: Strengthening Mental Health Promotion; Fact Sheet No 220; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice; Summary Report; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Yazd, S.D.; Wheeler, S.A.; Zuo, A. Key Risk Factors Affecting Farmers’ Mental Health: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4849. [Google Scholar] [CrossRef] [Green Version]
- Kun, P.; Tong, X.; Liu, Y.; Pei, X.; Luo, H. What are the determinants of post-traumatic stress disorder: Age, gender, ethnicity or other? Evidence from 2008 Wenchuan earthquake. Public Health 2013, 127, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Cénat, J.M.; Derivois, D. Assessment of prevalence and determinants of posttraumatic stress disorder and depression symptoms in adults survivors of earthquake in Haiti after 30 months. J. Affect. Disord. 2014, 159, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Cofini, V.; Carbonelli, A.; Cecilia, M.; Binkin, N.; di Orio, F. Post traumatic stress disorder and coping in a sample of adult survivors of the Italian earthquake. Psychiatry Res. 2015, 229, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Forbes, D.; Alkemade, N.; Waters, E.; Gibbs, L.; Gallagher, H.C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; et al. The role of anger and ongoing stressors in mental health following a natural disaster. Aust. N. Z. J. Psychiatry 2015, 49, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Cannon, T. Gender and climate hazards in Bangladesh. Gend. Dev. 2002, 10, 45–50. [Google Scholar] [CrossRef]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; A Akl, E.; E Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Joanna Briggs Institute (JBI). Joanna Briggs Institute Reviewers’ Manual: 2014 edition Adelaide. South Australia: University of Adelaide. 2014. Available online: http://joannabriggs.org/assets/docs/sumari/ReviewersManual-2014.pdf (accessed on 20 March 2019).
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Sandelowski, M.; Voils, C.I.; Barroso, J. Defining and Designing Mixed Research Synthesis Studies. Res. Sch. 2006, 13, 29. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. Introduction to Meta-Analysis; Wiley: West Sussex, UK, 2009. [Google Scholar]
- Bimali, I.; Adhikari, S.P.; Baidya, S.; Shakya, N.R. Impairment and Functional Status of People with Disabilities Following Nepal Earthquake 2015. Kathmandu Univ. Med. J. 2019, 16, 285–289. [Google Scholar]
- Adhikari, R.P.; Upadhaya, N.; Paudel, S.; Pokhrel, R.; Bhandari, N.; Cole, L.; Koirala, S. Psychosocial and Mental Health Problems of Older People in Postearthquake Nepal. J. Aging Health 2017, 30, 945–964. [Google Scholar] [CrossRef] [PubMed]
- Dahal, H.R.; Kumar, S.; Thapa, D.K. Prevalence and Risk Factors of Post-Traumatic Stress Disorders among the Survivors of 2015 Nepal Earthquake, in Dhading, Nepal. Sleep Hypn. Int. J. 2017, 20, 128–139. [Google Scholar] [CrossRef] [Green Version]
- Baral, I.A.; Bhagawati, K.C. Post traumatic stress disorder and coping strategies among adult survivors of earthquake, Nepal. BMC Psychiatry 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Powell, T.; Li, S.-J.; Hsiao, Y.; Ettari, C.; Bhandari, A.; Peterson, A.; Shakya, N. Investigating the Aftershock of a Disaster: A Study of Health Service Utilization and Mental Health Symptoms in Post-Earthquake Nepal. Int. J. Environ. Res. Public Health 2019, 16, 1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwind, J.S.; Norman, S.A.; Brown, R.; Frances, R.H.; Koss, E.; Karmacharya, D.; Santangelo, S.L. Association Between Earthquake Exposures and Mental Health Outcomes in Phulpingdanda Village After the 2015 Nepal Earth-quakes. Community Ment. Health J. 2019, 55, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- Suhail, K.; Malik, F.; Mir, I.A.; Hasan, S.S.; Sarwar, A.; Tanveer, S. Psychological Health of Earthquake Survivors in Pakistan. Psychol. Dev. Soc. 2009, 21, 183–207. [Google Scholar] [CrossRef]
- Ahmad, S.; Feder, A.; Lee, E.J.; Wang, Y.; Southwick, S.M.; Schlackman, E.; Buchholz, K.; Alonso, A.; Charney, D.S. Earthquake impact in a remote South Asian population: Psychosocial factors and posttraumatic symptoms. J. Trauma. Stress 2010, 23, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Naeem, F.; Ayub, M.; Masood, K.; Gul, H.; Khalid, M.; Farrukh, A.; Shaheen, A.; Waheed, W.; Chaudhry, H.R. Prevalence and psychosocial risk factors of PTSD: 18 months after Kashmir earthquake in Pakistan. J. Affect. Disord. 2011, 130, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Feder, A.; Ahmad, S.; Lee, E.J.; Morgan, J.; Singh, R.; Smith, B.W.; Southwick, S.M.; Charney, D.S. Coping and PTSD symptoms in Pakistani earthquake survivors: Purpose in life, religious coping and social support. J. Affect. Disord. 2013, 147, 156–163. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Kanakamma, L.G.; John, J.; Sunny, G.; Cohen, A.; De Silva, M.J. Post-tsunami mental health: A cross-sectional survey of the predictors of common mental disorders in South India 9-11 months after the 2004 Tsunami. Asia-Pac. Psychiatry 2012, 4, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Pyari, T.T.; Kutty, R.V.; Sarma, P.S. Risk factors of post-traumatic stress disorder in tsunami survivors of Kanyakumari District, Tamil Nadu, India. Indian J. Psychiatry 2012, 54, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Sudaryo, M.K.; Besral; Endarti, A.T.; Rivany, R.; Phalkey, R.; Marx, M.; Guha-Sapir, D. Injury, disability and quality of life after the 2009 earthquake in Padang, Indonesia: A prospective cohort study of adult survivors. Glob. Health Action 2012, 5, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aurizki, G.E.; Efendi, F.; Indarwati, R. Factors associated with post-traumatic stress disorder (PTSD) following natural disaster among Indonesian elderly. Work. Older People 2019, 24, 27–38. [Google Scholar] [CrossRef]
- Wickrama, T.; Ketring, S.A. Change in the health of tsunami-exposed mothers three years after the natural disaster. Int. J. Soc. Psychiatry 2011, 58, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Mamun, M.A.; Huq, N.; Papia, Z.F.; Tasfina, S.; Gozal, D. Prevalence of depression among Bangladeshi village women subsequent to a natural disaster: A pilot study. Psychiatry Res. 2019, 276, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Liu, X.; Liu, Y.; Xue, C.; Zhang, L. A meta-analysis of risk factors for depression in adults and children after natural disasters. BMC Public Health 2014, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Kamel, N. The role of gender and age in fracture distribution following the 2008 Wenchuan earthquake. Nat. Hazards 2011, 59, 1357–1375. [Google Scholar] [CrossRef]
- Liu, Z.; Zeng, Z.; Xiang, Y.; Hou, F.; Li, J.; Li, T.; Hu, X.; Ping, Y. A Cross-sectional Study on Posttraumatic Impact Among Qiang Women in Maoxian County 1 Year After the Wenchuan Earthquake, China. Asia-Pac. J. Public Health 2011, 24, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.B.; Harville, E. Long-Term Mental Health Among Low-Income, Minority Women Following Exposure to Multiple Natural Disasters in Early and Late Adolescence Compared to Adulthood. Child Youth Care Forum 2015, 44, 511–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokoyama, Y.; Otsuka, K.; Kawakami, N.; Kobayashi, S.; Ogawa, A.; Tannno, K.; Onoda, T.; Yaegashi, Y.; Sakata, K. Mental Health and Related Factors after the Great East Japan Earthquake and Tsunami. PLoS ONE 2014, 9, e102497. [Google Scholar] [CrossRef] [PubMed]
- Hamama-Raz, Y.; Palgi, Y.; Shrira, A.; Goodwin, R.; Kaniasty, K.; Ben-Ezra, M. Gender Differences in Psychological Reactions to Hurricane Sandy Among New York Metropolitan Area Residents. Psychiatr. Q. 2014, 86, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Kun, P.; Chen, X.; Han, S.; Gong, X.; Chen, M.; Zhang, W.; Yao, L. Prevalence of post-traumatic stress disorder in Sichuan Province, China after the 2008 Wenchuan earthquake. Public Health 2009, 123, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Farooq, N.; Bhatti, M.A.; Kuroiwa, C. Assessment of prevalence and determinants of posttraumatic stress disorder in survivors of earthquake in Pakistan using Davidson Trauma Scale. J. Affect. Disord. 2011, 136, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Hosain, G.M.; Chatterjee, N.; Ara, N.; Islam, T. Prevalence, pattern and determinants of mental disorders in rural Bangladesh. Public Health 2007, 121, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.; Zitko, P.; Jones, K.; Lynch, J.; Araya, R. Country- and individual-level socioeconomic determinants of depression: Multilevel cross-national comparison. Br. J. Psychiatry 2013, 202, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Calvo, R.; Arcaya, M.C.; Baum, C.; Lowe, S.R.; Waters, M.C. Happily Ever After? Pre-and-Post Disaster Determinants of Happiness Among Survivors of Hurricane Katrina. J. Happiness Stud. 2014, 16, 427–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, C.; Walsh, C.A. Seniors’ disaster resilience: A scoping review of the literature. Int. J. Disaster Risk Reduct. 2017, 25, 259–273. [Google Scholar] [CrossRef]
- Herrman, H. Promoting Mental Health and Resilience after a Disaster. J. Exp. Clin. Med. 2012, 4, 82–87. [Google Scholar] [CrossRef]
- Lindell, M.K. Disaster studies. Curr. Sociol. 2013, 61, 797–825. [Google Scholar] [CrossRef]
- Heid, A.R.; Christman, Z.; Pruchno, R.; Cartwright, F.P.; Wilson-Genderson, M. Vulnerable, But Why? Post-Traumatic Stress Symptoms in Older Adults Exposed to Hurricane Sandy. Disaster Med. Public Health Prep. 2016, 10, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Yamaoka, K. Social Factors Associated with Psychological Distress and Health Problems Among Elderly Members of a Disaster-Affected Population: Subgroup Analysis of a 1-Year Post-disaster Survey in Ishinomaki Area, Japan. Disaster Med. Public Health Prep. 2016, 11, 64–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Federation of Red Cross and Red Crescent Societies (IFRC). World Disasters Report: Leaving No One Behind; IFRC: Geneva, Switzerland, 2018; Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/B-WDR-2018-EXECSUM-EN. (accessed on 5 July 2021).
- Guha-Sapir, D.; Hoyois, P.; Wallemacq, P.; Below, R. Annual Disaster Statistical Review 2016: The Numbers and Trends; Centre for Research on the Epidemiology of Disasters (CRED): Brussels, Belgium, 2016; Available online: http://emdat.be/sites/default/files/adsr_2016. (accessed on 21 April 2021).


{kind=link}
| Population | Women OR Woman OR Female OR Females |
|---|---|
| Interest | health (health (vulnerability OR vulnerabilities OR risk OR hazard OR hazards OR hazardous OR psychological OR mental OR physical OR emotion OR emotional OR psychosocial OR reproductive OR sexual)) |
| Context1 | natural disasters (“natural disasters” OR “natural disasters” OR “natural calamities” OR “natural calamity” OR flood OR floods OR flooding OR volcano OR volcanoes OR volcanic OR earthquake OR earthquakes OR cyclone OR cyclones OR hurricane OR hurricanes OR drought OR droughts OR tornado OR tornadoes OR landslide OR landslides OR mudslide OR mudslides OR (“wild fire” OR “wild fires” OR “wildfire” OR “wildfires” OR bushfire OR bushfires) |
| Context2 | “south asia” OR “southeast asia” OR bangladesh OR srilanka OR sri Lanka OR india OR bhutan OR nepal OR pakistan OR maldives OR afghanistan OR brunei OR burma OR mayanmar OR cambodia OR timo-leste OR indonesia OR laos OR malaysia OR phillippines OR singapore OR thailand OR vietnam |
| Reference/Location | Sample Size/Age/Gender | Context/Type of Participants | Study Design/Methods | Quality |
|---|---|---|---|---|
| Bimali et al., (2018), Nepal [27] | Total sample: 199 Female: 25 to 80 Male: 9 to 79 Male: 65% Female: 35% | Earthquake Individuals with physical disabilities caused by the earthquake | Cross-sectional descriptive study Quantitative | HQ |
| Adhikar et al., (2018), Nepal [28] | Total sample: 30 Age range not reported Women: 7 Men: 23 | Earthquake Disaster-affected older people and key informant | Qualitative | HQ |
| Dahal et al., (2018), Nepal [29] | Total sample: 535 Age: 18+ Female: (n = 247, 46.2%), Male: (n = 288, 53.8%) | Earthquake Earthquake experienced survivors | Cross-sectional study Quantitative | HQ |
| Baral et al., (2019), Nepal [30] | Total sample: 291 Age: 20 and above Female: (n = 125, 43%) Male: (n = 166, 57%) | Earthquake Earthquake experienced adult survivors | Cross-sectional descriptive study Quantitative | HQ |
| Powell et al., (2019), Nepal [31] | Total sample: 750 Age range not mentioned Female: (n = 532, 70.9%) Male: (n = 218, 29.1%) | Earthquake Disaster-affected individuals | Cross-sectional study Quantitative | HQ |
| Schwind et al., (2019), Nepal [32] | Total sample: 238 Age: 18–85 Female: (n = 145, 65%) Male: (n = 78, 35%) | Earthquake earthquake experienced adult survivors | Cross-sectional study Quantitative | HQ |
| Suhail et al., (2009), Pakistan [33] | Total sample: 125, response rate of 98.45%. Age: 18–70 Women: 73 Men: 52 | Earthquake Earthquake survivors | Mixed-method | M |
| Ahmad et al., (2010), Pakistan [34] | Sample size: 1st wave: 44, 2nd wave: 51 Mean age: 1st wave; 35.3, 2nd wave: 31.2 1st wave Female 12 (27.3%), Male 32 (72.7%) 2nd wave Female: 0 Male: 51 (100.0%) | Earthquake Earthquake survivors | Cross-sectional study Quantitative | M |
| Naeem et al., (2011), Pakistan [35] | Total sample: 1298 Age: 18+ Female: (n = 779, 60.3%) Male: (n = 512, 39.7%) | Earthquake Disaster-affected residents in earthquake area | Cross-sectional study Quantitative | HQ |
| Feder et al., (2012), Pakistan [36] | Total sample: 200 Age range not reported but study on adult survivors Female: 39 Male: 161 | Earthquake Adult earthquake survivors | Cross-sectional study Quantitative | HQ |
| George et al., (2012), India [37] | Total sample: 533 Age: 18+ Female: (n = 303, 57%) Male: (n = 229, 43%) | Tsunami Tsunami-affected residents | Cross-sectional study Quantitative | HQ |
| Pyari, et al., (2012), India [38] | Total sample: 485 Age: 19 to 81 Female: (n = 178) Male: (n = 121) | Tsunami Tsunami survivors with PTSD | Quantitative | HQ |
| Sudaryo et al., (2012), Indonesia [39] | Injured: 184 Non-injured: 93 Age: 18+ Injured Men: 53, Women: 131 Non-injured Men: 22, Women: 71 | Earthquake Adult injured earthquake survivors | Cohort study Quantitative | HQ |
| Aurizki et al., (2020), Indonesia [40] | Total sample: 152, response rate 100% Age: 60 and above Females (n = 113, 74%) Males (n = 39, 26%) | Earthquake Adults experienced or witnessed the disaster directly | Cross-sectional study Quantitative | HQ |
| Wickrama et al., (2011), Sri Lanka [41] | Sample size: wave 1: 195, wave 2: 160 Age: 29 to 60, Female | Tsunami Tsunami-exposed mothers | Longitudinal Study Quantitative | HQ |
| Mamun et al., (2019), Bangladesh [42] | Total sample: 111 Age: 18 and above Female | Cyclone Women, permanent residents of the Cyclone Mora-affected village | Quantitative | HQ |
| Risk Factors | Health Outcomes of Women Following Disasters | Total Studies (and %) Naming These Stress Affecting Women’s Health |
|---|---|---|
| Socio-demographic risk factors | ||
| Adult Age [27,28,29,30,31,36,37,38,40,41] | PTSD, depression, anxiety, CMD, disability, poor physical health, depressive symptoms, psychosocial and mental health problems | 10 (63%) |
| No education/lower level of education [29,30,32,34,36,37,39,40,41] | PTSD, poor physical health, depressive symptoms, depression, disability from injury, CMD | 9 (57%) |
| Poverty/low income/economic hardship [28,31,37,39,40,41] | Anxiety, poor physical health, depressive symptoms, psychosocial and mental health problems, disability from injury, PTSD, CMD | 6 (38%) |
| Marital status (single/divorced/widowed) [32,36,37,38] | PTSD, depression, CMD | 4 (25%) |
| Lower age group (18–30) [33,39,42]; religious minorities [29,32,37]; | Depression, injured, PTSD, CMD | 3 (19%) |
| Having children or no children [38,42] | Depression, PTSD | 2 (13%) |
| Family structure, housing type [37], socially disadvantaged group [32]; being an income earner [42]; rural residence [38] | Depression, CMD, PTSD | 1 (7%) |
| Disaster exposure | ||
| Disaster related physical injury [28,30,32,38,39,42] | Depression, PTSD, psychosocial and mental health problems | 6 (38%) |
| Resource loss (financial loss or loss of food, shelter, property)/completely damaged house [29,32,35,37,38,39] | PTSD, CMD, depression, disability | 6 (38%) |
| Humanitarian loss [29,34,36,37,38] | PTSD, CMD | 5 (32%) |
| Relocation or displacement/living in tent [34,35,38] | PTSD, CMD | 3 (19%) |
| Distance from epicentre [34,36]; position (staying home) during earthquake [27,35] | PTSD, CMD, disability from injury | 2 (13%) |
| Source of information for health issues [31]; public health centre utilisation [40]; injury to family members [38]; difficulty in communication, witnessing death [29]; threat to life/panic during disaster; community destruction; separation from family [38] | PTSD, anxiety, depression | 1 (7%) |
| Post-disaster risk factors | ||
| Loss of job/income generation activities [29,37]; low social support [29,38]; negative religious coping [36,37] | PTSD, CMD | 2 (13%) |
| Poor physical health [41]; access to healthcare facility [31]; dependence on others [32]; absence from work/work absenteeism [42] | Depression, anxiety, poor physical health, depressive symptoms | 1 (7%) |
| Fear of re-experiencing disaster [33]; blaming [28]; inadequate resources, mental health support system, involvement in rescue work; substance abuse [38] | Depression, psychosocial and mental health problems, PTSD | 1 (7%) |
| Pre-disaster risk factors | ||
| Pre-disaster stress and exposure to violence, family adversities/conflict (secondary stressors) [28,29,41]; chronic illness [37,38,40] | PTSD, CMD, poor physical health, depressive symptoms, psychosocial and mental health problems | 3 (19%) |
| Exposure of family history of mental illness [29,38] | PTSD | 2 (13%) |
| Low quality marital relationship [37]; poor socioeconomic background; history of substance use [38] | PTSD, CMD | 1 (7%) |
| Themes | Sub-Themes | |
|---|---|---|
| 3.4 | Health impact of natural disasters on women |
|
| 3.5 | Risk factors affecting women’s health following natural disasters |
|
| 3.6 | Association between physical and mental health | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fatema, S.R.; East, L.; Islam, M.S.; Usher, K. Health Impact and Risk Factors Affecting South and Southeast Asian Women Following Natural Disasters: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11068. https://doi.org/10.3390/ijerph182111068
Fatema SR, East L, Islam MS, Usher K. Health Impact and Risk Factors Affecting South and Southeast Asian Women Following Natural Disasters: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(21):11068. https://doi.org/10.3390/ijerph182111068
Chicago/Turabian StyleFatema, Syadani Riyad, Leah East, Md Shahidul Islam, and Kim Usher. 2021. "Health Impact and Risk Factors Affecting South and Southeast Asian Women Following Natural Disasters: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 21: 11068. https://doi.org/10.3390/ijerph182111068
APA StyleFatema, S. R., East, L., Islam, M. S., & Usher, K. (2021). Health Impact and Risk Factors Affecting South and Southeast Asian Women Following Natural Disasters: A Systematic Review. International Journal of Environmental Research and Public Health, 18(21), 11068. https://doi.org/10.3390/ijerph182111068