
Transdisciplinary Online Health Assessment of an Artisanal and Small-Scale Gold Mining Community during the COVID-19 Pandemic in the Mandalay Region of Myanmar




Abstract
:1. Introduction
2. Materials and Methods
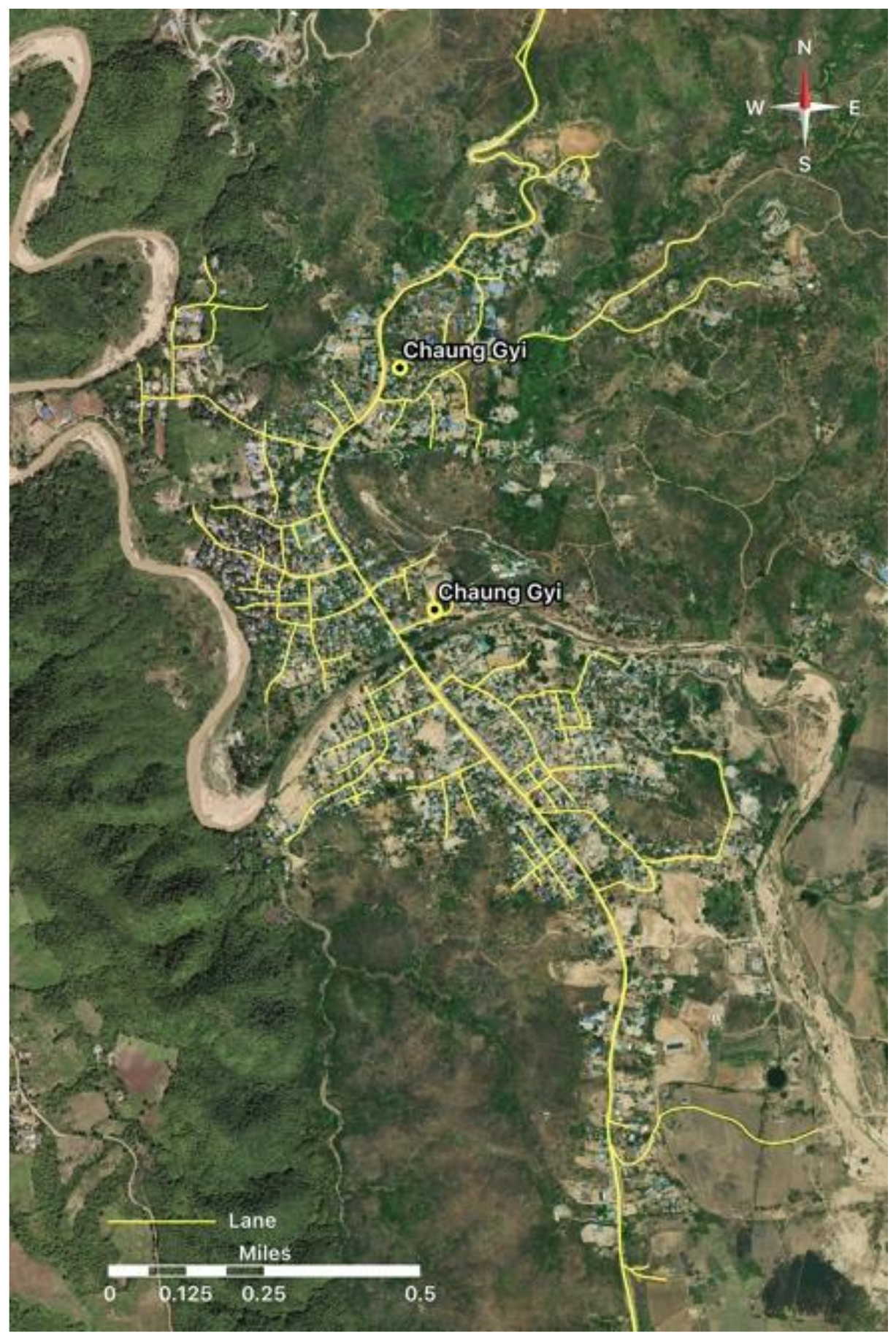
2.1. Study Area
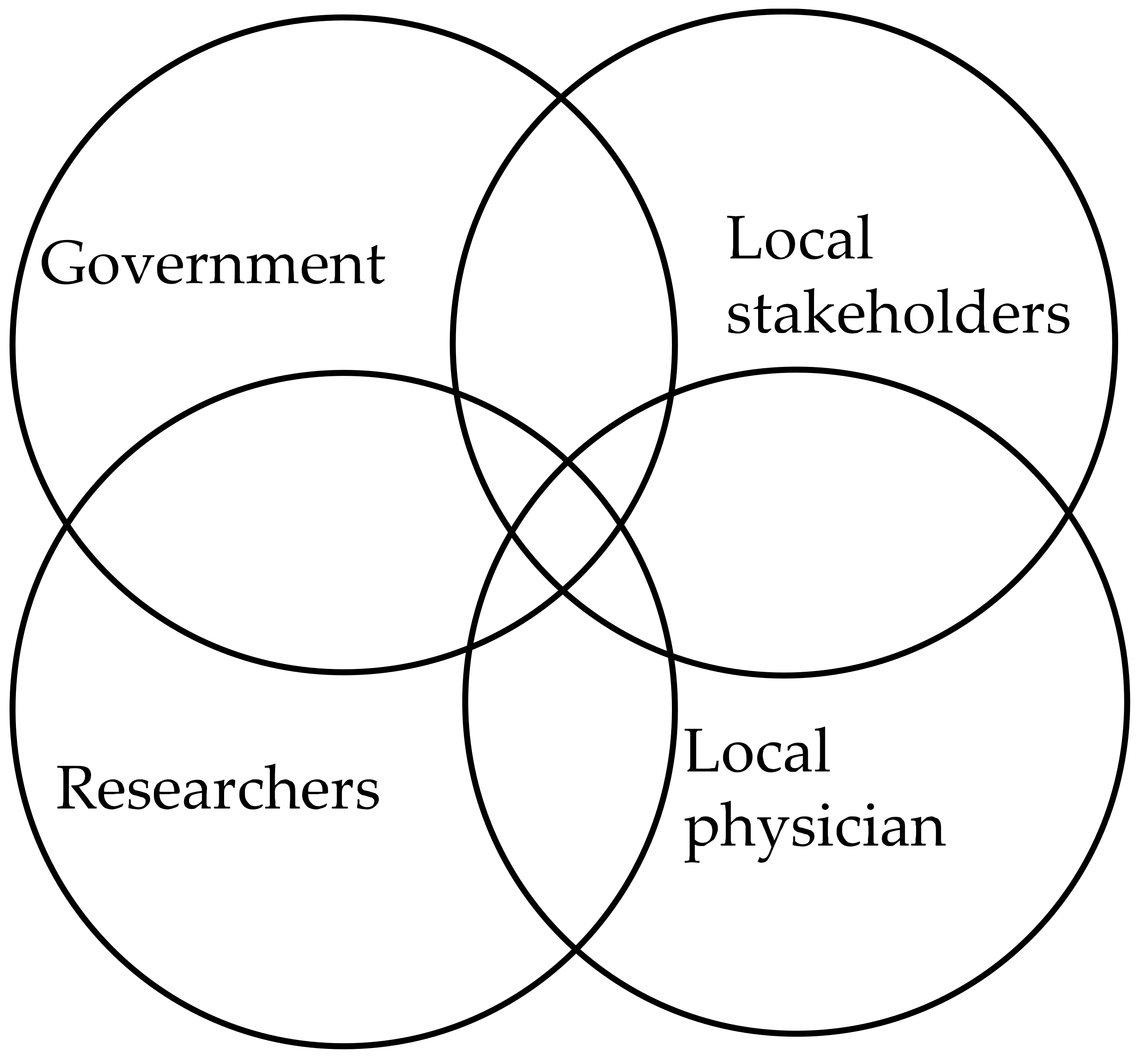
2.2. Transdisciplinary Approach Research Design
2.3. Interview Questions
2.4. Statistical Analysis
3. Results
3.1. Socioeconomic Assessment
3.2. Risk of Exposure to Hg and Other Heavy Metals
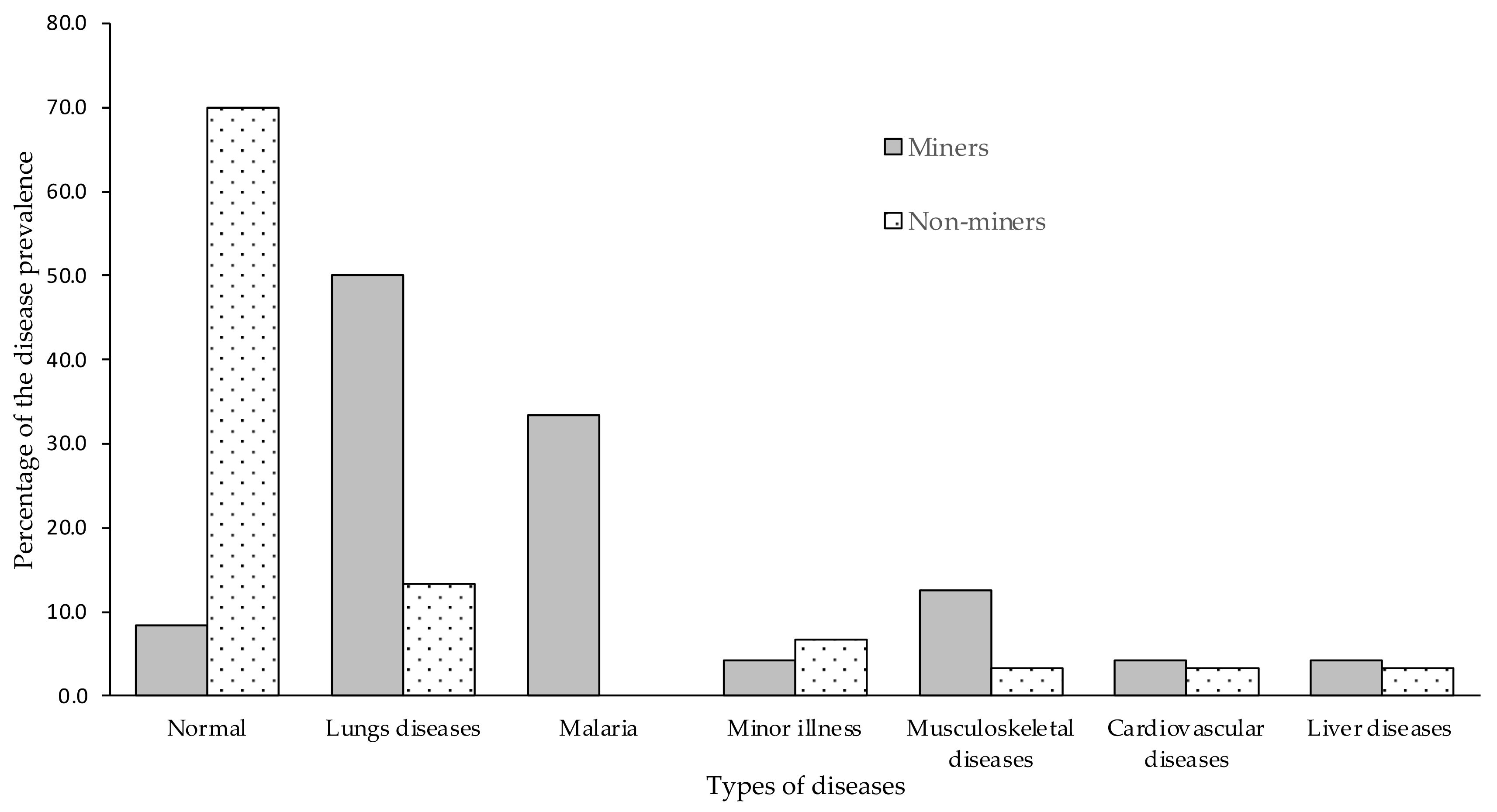
3.3. Disease Prevalence by Occupation
3.4. Chronic Hg Intoxication Signs and Symptoms
4. Discussion
4.1. Factors in the Choice of ASGM as the Main Livelihood in the Study Area
4.2. Community Health Status
4.3. Effectiveness of Online Health Assessment in ASGM Context
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNEP. A Practical Guide to Reducing Mercury Use in Artisanal and Small-Scale Gold Mining; United Nations Environment Policy: Nairobi, Kenya, 2012; 76p. [Google Scholar]
- Steckling, N.; Bose-O’Reilly, S.; Pinheiro, P.; Plass, D.; Shoko, D.; Drasch, G.; Bernaudat, L.; Siebert, U.; Hornberg, C. The burden of chronic mercury intoxication in artisanal small-scale gold mining in Zimbabwe: Data availability and preliminary estimates. Environ. Health A Glob. Access Sci. Source 2014, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yard, E.E.; Horton, J.; Schier, J.G.; Caldwell, K.; Sanchez, C.; Lewis, L.; Gastaňaga, C. Mercury Exposure Among Artisanal Gold Miners in Madre de Dios, Peru: A Cross-sectional Study. J. Med. Toxicol. 2012, 8, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harari, R.; Harari, F.; Gerhardsson, L.; Lundh, T.; Skerfving, S.; Strömberg, U.; Broberg, K. Exposure and toxic effects of elemental mercury in gold-mining activities in Ecuador. Toxicol. Lett. 2012, 213, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Tomicic, C.; Vernez, D.; Belem, T.; Berode, M. Human mercury exposure associated with small-scale gold mining in Burkina Faso. Int. Arch. Occup. Environ. Health 2011, 84, 539–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bose-O’Reilly, S.; Drasch, G.; Beinhoff, C.; Tesha, A.; Drasch, K.; Roider, G.; Taylor, H.; Appleton, D.; Siebert, U. Health assessment of artisanal gold miners in Tanzania. Sci. Total Environ. 2010, 408, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.M.; Nyland, J.F.; Silva, I.A.; Ventura, A.M.; de Souza, J.M.; Silbergeld, E.K. Mercury exposure, serum antinuclear/antinucleolar antibodies, and serum cytokine levels in mining populations in Amazonian Brazil: A cross-sectional study. Environ. Res. 2010, 110, 345–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bose-O’Reilly, S.; Lettmeier, B.; Gothe, R.M.; Beinhoff, C.; Siebert, U.; Drasch, G. Mercury as a serious health hazard for children in gold mining areas. Environ. Res. 2008, 107, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.A.; Nyland, J.F.; Gorman, A.; Perisse, A.; Ventura, A.M.; Santos, E.C.O.; De Souza, J.M.; Burek, C.L.; Rose, N.R.; Silbergeld, E.K. Mercury exposure, malaria, and serum antinuclear/antinucleolar antibodies in amazon populations in Brazil: A cross-sectional study. Environ. Health A Glob. Access Sci. Source 2004, 3, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drake, P.L.; Rojas, M.; Reh, C.M.; Mueller, C.A.; Jenkins, F.M. Occupational exposure to airborne mercury during gold mining operations near EL Callo, Venezuela. Int. Arch. Occup. Environ. Health 2001, 74, 206–212. [Google Scholar] [CrossRef]
- Drasch, G.; Böse-O’Reilly, S.; Beinhoff, C.; Roider, G.; Maydl, S. The Mt. Diwata study on the Philippines 1999—Assessing mercury intoxication of the population by small scale gold mining. Sci. Total Environ. 2001, 267, 151–168. [Google Scholar] [CrossRef]
- Eisler, R. Health risks of gold miners: A synoptic review. Environ. Geochem. Health 2003, 25, 325–345. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, W.T.; Kuang, X.; Sakakibara, M. Health Impact Assessment of Artisanal and Small-Scale Gold Mining Area in Myanmar, Mandalay Region: Preliminary Research. Int. J. Environ. Res. Public Health 2020, 17, 6757. [Google Scholar] [CrossRef] [PubMed]
- NIOSH. Health Effects of Occupational Exposure to Respirable Crystalline Silica; NIOSH: Washington, DC, USA, 2002. [Google Scholar]
- Calvert, G.M.; Rice, F.L.; Boiano, J.M.; Sheehy, J.W. Occupational silica exposure and risk of various diseases: An analysis using death certificates from 27 states of the United States. Occup. Environ. Med. 2003, 60, 122–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Soe, T.N.; Zhao, Y.; Than, A.; Cho, C.; Aung, P.L.; Li, Y.; Wang, L.; Yang, H.; Li, X.; et al. Geographical heterogeneity in prevalence of subclinical malaria infections at sentinel endemic sites of Myanmar. Parasites Vectors 2019, 12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Category | 54 Respondents (%) | Miners | Non-Miners |
|---|---|---|---|---|
| Sex | Male vs. Female | 59.3 | 18 vs. 6 | 14 vs. 16 |
| Age (years) | Mean ± SD | 37.3 ± 11.7 | 36.5 ± 14.2 | |
| Age (years) | 20–29 | 38.9 | 9 (n) | 12 (n) |
| 30–39 | 24.1 | 4 (n) | 9 (n) | |
| 40–49 | 16.7 | 6 (n) | 3 (n) | |
| 50–69 | 20.3 | 5 (n) | 6 (n) | |
| Living status | Native vs. migrant | 59.3 | 13 vs. 11 | 19 vs. 11 |
| Education status | Monastic School Education | 7.4 | 1 (n) | 3 (n) |
| Primary School | 51.9 | 8 (n) | 20 (n) | |
| Middle School | 16.7 | 7 (n) | 2 (n) | |
| High School Completed | 13 | 4 (n) | 3 (n) | |
| * Income per day (USD) | Mean ± SD | 14.7 ± 10.8 | 2.5 ± 1.5 | |
| Income per day (USD) | Range (minimum–maximum) | $6–$31 | $1–$8 |
| Risk Factor | Numbers (n) |
|---|---|
| Living distance from ASGM activity of all respondents | |
| <1 km | 14 |
| 1–5 km | 17 |
| 5–10 km | 23 |
| >10 km | 0 |
| Miner-Specific Risk Factor of miners | |
| Hg use | 12 |
| Cyanide use | 3 |
| Personal protection use during mining activity of miners | |
| Yes | 9 |
| No | 15 |
| Mining activities of miners | |
| Working across all areas of mining | 6 |
| Excavation and crushing ores primarily | 10 |
| Panning and amalgamation only | 4 |
| Refining (burning amalgam) only | 2 |
| Carrying gold ores only | 2 |
| Mining experience of miners | |
| <10 years | 8 |
| 10–20 years | 14 |
| >20 years | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyaw, W.T.; Myint, Y.M.; Kuang, X.; Sakakibara, M. Transdisciplinary Online Health Assessment of an Artisanal and Small-Scale Gold Mining Community during the COVID-19 Pandemic in the Mandalay Region of Myanmar. Int. J. Environ. Res. Public Health 2021, 18, 11206. https://doi.org/10.3390/ijerph182111206
Kyaw WT, Myint YM, Kuang X, Sakakibara M. Transdisciplinary Online Health Assessment of an Artisanal and Small-Scale Gold Mining Community during the COVID-19 Pandemic in the Mandalay Region of Myanmar. International Journal of Environmental Research and Public Health. 2021; 18(21):11206. https://doi.org/10.3390/ijerph182111206
Chicago/Turabian StyleKyaw, Win Thiri, Yee Mon Myint, Xiaoxu Kuang, and Masayuki Sakakibara. 2021. "Transdisciplinary Online Health Assessment of an Artisanal and Small-Scale Gold Mining Community during the COVID-19 Pandemic in the Mandalay Region of Myanmar" International Journal of Environmental Research and Public Health 18, no. 21: 11206. https://doi.org/10.3390/ijerph182111206
APA StyleKyaw, W. T., Myint, Y. M., Kuang, X., & Sakakibara, M. (2021). Transdisciplinary Online Health Assessment of an Artisanal and Small-Scale Gold Mining Community during the COVID-19 Pandemic in the Mandalay Region of Myanmar. International Journal of Environmental Research and Public Health, 18(21), 11206. https://doi.org/10.3390/ijerph182111206