
Trends of Total Knee Arthroplasty According to Age Structural Changes in Korea from 2011 to 2018

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Losina, E.; Thornhill, T.S.; Rome, B.N.; Wright, J.; Katz, J.N. The dramatic increase in total knee replacement utilization rates in the United States cannot be fully explained by growth in population size and the obesity epidemic. J. Bone Jt. Surg. Am. 2012, 94, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michael, J.W.; Schlüter-Brust, K.U.; Eysel, P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch. Arztebl. Int. 2010, 107, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T.; Zhang, Y. Epidemiology of osteoarthritis. Rheum. Dis. Clin. 2013, 39, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canovas, F.; Dagneaux, L. Quality of life after Total Knee Arthroplasty. Orthop. Traumatol. Surg. Res. 2018, 104, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Mahomed, N.N.; Barrett, J.; Katz, J.N.; Baron, J.A.; Wright, J.; Losina, E. Epidemiology of total knee replacement in the United States Medicare population. J. Bone Jt. Surg. Am. 2005, 87, 1222–1228. [Google Scholar] [CrossRef]
- Mehrotra, C.; Remington, P.L.; Naimi, T.S.; Washington, W.; Miller, R. Trends in total knee replacement surgeries and implications for public health, 1990-2000. Public Health Rep. 2005, 120, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Nečas, L.; Katina, S.; Křivánek, S.; Uhlárová, J. Slovakian Arthroplasty Register. Review of the annual report of the Slovakian Arthroplasty Register—2010. Acta Chir. Orthop. Traumatol. Cech. 2011, 78 (Suppl. B), 1–59. [Google Scholar]
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Clin. Orthop. Relat. Res. 2009, 467, 2606–2612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vina, E.R.; Kwoh, C.K. Epidemiology of osteoarthritis: Literature update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef]
- Park, I. Population aging and its health implications in Korea. Bogeon. Sahoe. Nonjib. 1993, 13, 96–111. [Google Scholar]
- Jain, N.B.; Higgins, L.D.; Ozumba, D.; Guller, U.; Cronin, M.; Pietrobon, R.; Katz, J.N. Trends in epidemiology of knee arthroplasty in the United States, 1990-2000. Arthritis Rheum. 2005, 52, 3928–3933. [Google Scholar] [CrossRef] [PubMed]
- Khatod, M.; Inacio, M.; Paxton, E.W.; Bini, S.A.; Namba, R.S.; Burchette, R.J.; Fithian, D.C. Knee replacement: Epidemiology, outcomes, and trends in Southern California: 17,080 replacements from 1995 through 2004. Acta Orthop. 2008, 79, 812–819. [Google Scholar] [CrossRef]
- Crowninshield, R.D.; Rosenberg, A.G.; Sporer, S.M. Changing demographics of patients with total joint replacement. Clin. Orthop. Relat. Res. 2006, 443, 266–272. [Google Scholar] [CrossRef]
- Singh, J.A.; Vessely, M.B.; Harmsen, W.S.; Schleck, C.D.; Melton, L.J., III; Kurland, R.L.; Berry, D.J. A population-based study of trends in the use of total hip and Total Knee Arthroplasty, 1969–2008. Mayo Clin. Proc. 2010, 85, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Robertsson, O.; Bizjajeva, S.; Fenstad, A.M.; Furnes, O.; Lidgren, L.; Mehnert, F.; Odgaard, A.; Pedersen, A.B.; Havelin, L.I. Knee arthroplasty in Denmark, Norway and Sweden. A pilot study from the Nordic Arthroplasty Register Association. Acta Orthop. 2010, 81, 82–89. [Google Scholar] [CrossRef]
- Cho, H.J.; Chang, C.B.; Kim, K.W.; Park, J.H.; Yoo, J.H.; Koh, I.J.; Kim, T.K. Gender and prevalence of knee osteoarthritis types in elderly Koreans. J. Arthroplast. 2011, 26, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.W.; Noh, J.H.; Kim, D.-J. The prevalence of and demographic factors associated with radiographic knee osteoarthritis in Korean adults aged ≥50 years: The 2010–2013 Korea national health and nutrition examination survey. PLoS ONE 2020, 15, e0230613. [Google Scholar] [CrossRef]
- Kim, H.A.; Kim, S.; Seo, Y.I.; Choi, H.J.; Seong, S.C.; Song, Y.W.; Hunter, D.; Zhang, Y. The epidemiology of total knee replacement in South Korea: National registry data. Rheumatology (Oxf.) 2008, 47, 88–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.J.; Chang, C.B.; Yoo, J.H.; Kim, S.J.; Kim, T.K. Gender differences in the correlation between symptom and radiographic severity in patients with knee osteoarthritis. Clin. Orthop. Relat. Res. 2010, 468, 1749–1758. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.K. Demographic transition and population aging in Korea. Korea J. Popul. Dev. 1996, 25, 27–40. [Google Scholar]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Kim, J.A.; Yoon, S.; Kim, L.Y.; Kim, D.S. Towards Actualizing the Value Potential of Korea Health Insurance Review and Assessment (HIRA) Data as a Resource for Health Research: Strengths, Limitations, Applications, and Strategies for Optimal Use of HIRA Data. J. Korean Med. Sci. 2017, 32, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Robertsson, O.; Knutson, K.; Lewold, S.; Lidgren, L. The Swedish Knee Arthroplasty Register 1975-1997: An update with special emphasis on 41,223 knees operated on in 1988-1997. Acta Orthop. Scand. 2001, 72, 503–513. [Google Scholar] [CrossRef]
- Mitsuyasu, S.; Hagihara, A.; Horiguchi, H.; Nobutomo, K. Relationship between total arthroplasty case volume and patient outcome in an acute care payment system in Japan. J. Arthroplast. 2006, 21, 656–663. [Google Scholar] [CrossRef]
- Lavernia, C.J.; Guzman, J.F.; Gachupin-Garcia, A. Cost effectiveness and quality of life in knee arthroplasty. Clin. Orthop. Relat. Res. 1997, 345, 134–139. [Google Scholar] [CrossRef] [Green Version]
- Kye, B.; Arenas, E.; Teruel, G.; Rubalcava, L. Education, elderly health, and differential population aging in South Korea: A demographic approach. Demogr. Res. 2014, 30, 753–794. [Google Scholar] [CrossRef] [Green Version]
- Yan, C.H.; Chiu, K.Y.; Ng, F.Y. Total Knee Arthroplasty for primary knee osteoarthritis: Changing pattern over the past 10 years. Hong Kong Med. J. 2011, 17, 20–25. [Google Scholar]
- Cao, Z.; Mai, X.; Wang, J.; Feng, E.; Huang, Y. Unicompartmental Knee Arthroplasty vs High Tibial Osteotomy for Knee Osteoarthritis: A Systematic Review and Meta-Analysis. J. Arthroplast. 2018, 33, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Prodromos, C.C.; Amendola, A.; Jakob, R.P. High tibial osteotomy: Indications, techniques, and postoperative management. Instr. Course Lect. 2015, 64, 555–565. [Google Scholar] [PubMed]
- Blatter, S.C.; Koch, P. Unicompartmental knee arthroplasty—A solution? Ther. Umsch. 2020, 77, 475–479. [Google Scholar] [CrossRef]
- Arirachakaran, A.; Choowit, P.; Putananon, C.; Muangsiri, S.; Kongtharvonskul, J. Is unicompartmental knee arthroplasty (UKA) superior to Total Knee Arthroplasty (TKA)? A systematic review and meta-analysis of randomized controlled trial. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 799–806. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Mehl, J.; Imhoff, A.B.; Beitzel, K. Osteoarthritis of the shoulder: Pathogenesis, diagnostics and conservative treatment options. Orthopade 2018, 47, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Bert, J.M.; Endres, N.K.; Tucker, C.J.; Davey, A.P. The Conservative Treatment of Osteoarthritis of the Knee. Orthopedics 2018, 41, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J. Osteoarthritis and rheumatoid arthritis: Conservative therapeutic management. J. Hand. Ther. 2012, 25, 163–171. [Google Scholar] [CrossRef]
- Dalury, D.F. Cementless Total Knee Arthroplasty: Current concepts review. Bone Jt. J. 2016, 98-b, 867–873. [Google Scholar] [CrossRef] [Green Version]
- Klug, A.; Gramlich, Y.; Rudert, M.; Drees, P.; Hoffmann, R.; Weißenberger, M.; Kutzner, K.P. The projected volume of primary and revision Total Knee Arthroplasty will place an immense burden on future health care systems over the next 30 years. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 3287–3298. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Year 1 | Time Trend | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| TKA—Model 1 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | IRR 2 | 95%CI | |
| Lower | Upper | ||||||||||
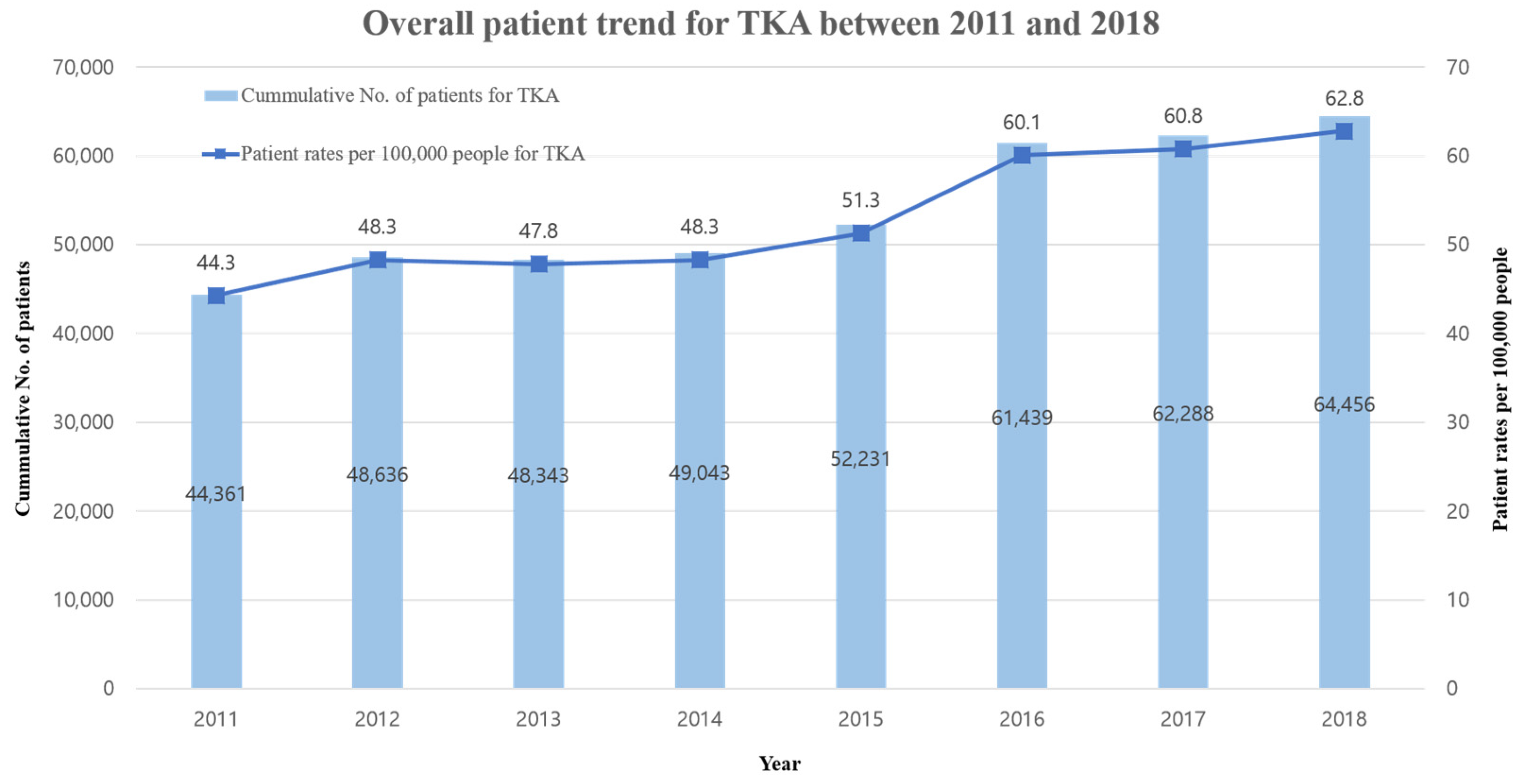
| All | 44.3 | 48.3 | 47.8 | 48.3 | 51.3 | 60.1 | 60.8 | 62.8 | 1.05 | 1.04 | 1.06 |
| Year with Age Adjustment | 0.99 | 0.97 | 1.00 | ||||||||
| Year with Sex Adjustment | 1.05 | 1.04 | 1.06 | ||||||||
| Year with Hospital Adjustment | 1.05 | 1.04 | 1.06 | ||||||||
| Year with Area Adjustment | 1.05 | 1.05 | 1.06 | ||||||||
| Year 1 | Time Trend | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TKA—Model 2 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | IRR 2 | 95%CI | ||
| Lower | Upper | |||||||||||
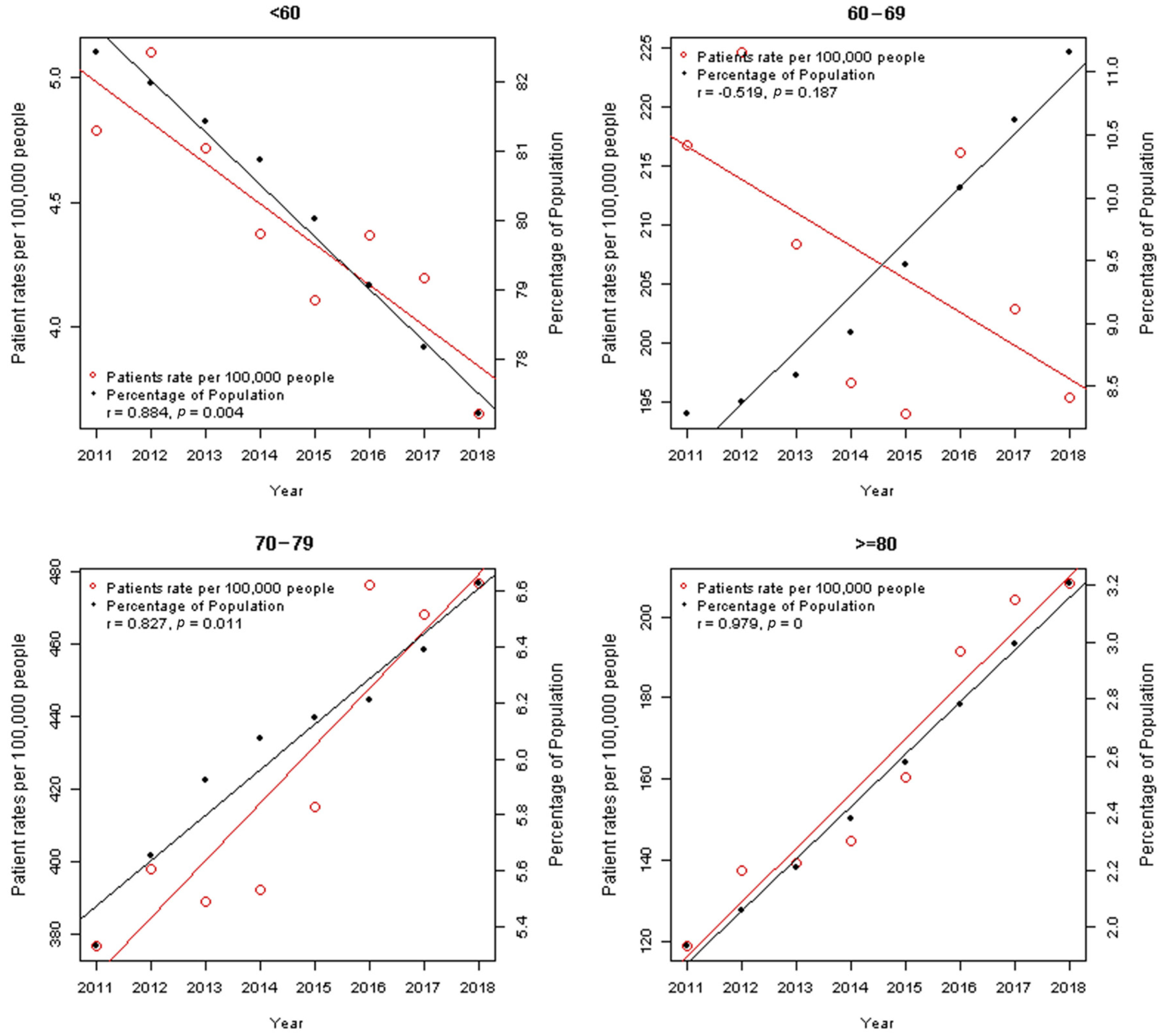
| Year × Age 3 | <60 | 4.8 | 5.1 | 4.7 | 4.4 | 4.1 | 4.4 | 4.2 | 3.6 | Reference | ||
| 60–69 | 216.8 | 224.6 | 208.4 | 196.6 | 194.1 | 216.2 | 203 | 195.5 | 0.97 | 0.95 | 0.99 | |
| 70–79 | 376.6 | 397.9 | 388.6 | 392.3 | 415 | 476.2 | 468 | 476.5 | 1.04 | 1.02 | 1.06 | |
| ≥80 | 118.9 | 137.5 | 139.5 | 144.9 | 160.4 | 191.5 | 204.3 | 208.2 | 1.04 | 1.02 | 1.06 | |
| Year × Sex 3 | Male | 10.9 | 12.2 | 13.1 | 13.7 | 14.6 | 17.7 | 18.5 | 20.6 | Reference | ||
| Female | 77.7 | 84.5 | 82.5 | 82.9 | 87.9 | 102.4 | 102.9 | 104.9 | 1.09 | 1.09 | 1.10 | |
| Year × Hospital 3 | Tertiary | 5.4 | 5.8 | 5.6 | 6.3 | 6.6 | 8 | 6.6 | 7.3 | Reference | ||
| General | 10.7 | 10.9 | 11.9 | 12.1 | 13.6 | 16.3 | 16.7 | 18 | 1.04 | 1.02 | 1.06 | |
| Clinic | 28.2 | 31.7 | 30.4 | 29.9 | 31.1 | 35.8 | 37.6 | 37.5 | 1.05 | 1.04 | 1.05 | |
| Year × Area 3 | Seoul | 130.1 | 139.1 | 131.4 | 135.6 | 139 | 168.2 | 167.1 | 175.1 | Reference | ||
| Gyeonggi | 56.4 | 62.4 | 64 | 67.1 | 70.5 | 76.4 | 81.1 | 84.1 | 0.99 | 0.98 | 1.00 | |
| Others | 87.1 | 96 | 96.5 | 95.7 | 103.7 | 123 | 124.1 | 127.7 | 1.00 | 0.99 | 1.02 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-B.; Choi, H.-S.; Kang, E.M.; Park, S.; Seo, G.-W.; Chun, D.-I.; Min, T.-H. Trends of Total Knee Arthroplasty According to Age Structural Changes in Korea from 2011 to 2018. Int. J. Environ. Res. Public Health 2021, 18, 13397. https://doi.org/10.3390/ijerph182413397
Kim Y-B, Choi H-S, Kang EM, Park S, Seo G-W, Chun D-I, Min T-H. Trends of Total Knee Arthroplasty According to Age Structural Changes in Korea from 2011 to 2018. International Journal of Environmental Research and Public Health. 2021; 18(24):13397. https://doi.org/10.3390/ijerph182413397
Chicago/Turabian StyleKim, Yong-Beom, Hyung-Suk Choi, Eun Myeong Kang, Suyeon Park, Gi-Won Seo, Dong-Il Chun, and Tae-Hong Min. 2021. "Trends of Total Knee Arthroplasty According to Age Structural Changes in Korea from 2011 to 2018" International Journal of Environmental Research and Public Health 18, no. 24: 13397. https://doi.org/10.3390/ijerph182413397
APA StyleKim, Y. -B., Choi, H. -S., Kang, E. M., Park, S., Seo, G. -W., Chun, D. -I., & Min, T. -H. (2021). Trends of Total Knee Arthroplasty According to Age Structural Changes in Korea from 2011 to 2018. International Journal of Environmental Research and Public Health, 18(24), 13397. https://doi.org/10.3390/ijerph182413397