
Connected, Respected and Contributing to Their World: The Case of Sexual Minority and Non-Minority Young People in Ireland

 ,
,  and
and 
Abstract
:1. Introduction
1.1. The Human Ecology of Child and Adolescent Health
1.2. Connected, Respected, and Contributing to Their World: The Fifth Outcome of the Better Outcomes, Brighter Futures
1.3. Connectedness, Self-Esteem, and Societal Engagement in Sexual Minority Youth
2. Method
2.1. Procedure
2.2. Measures
2.2.1. Sociodemographic Variables
2.2.2. Romantic Attraction
2.2.3. BOBF Outcome Indicators
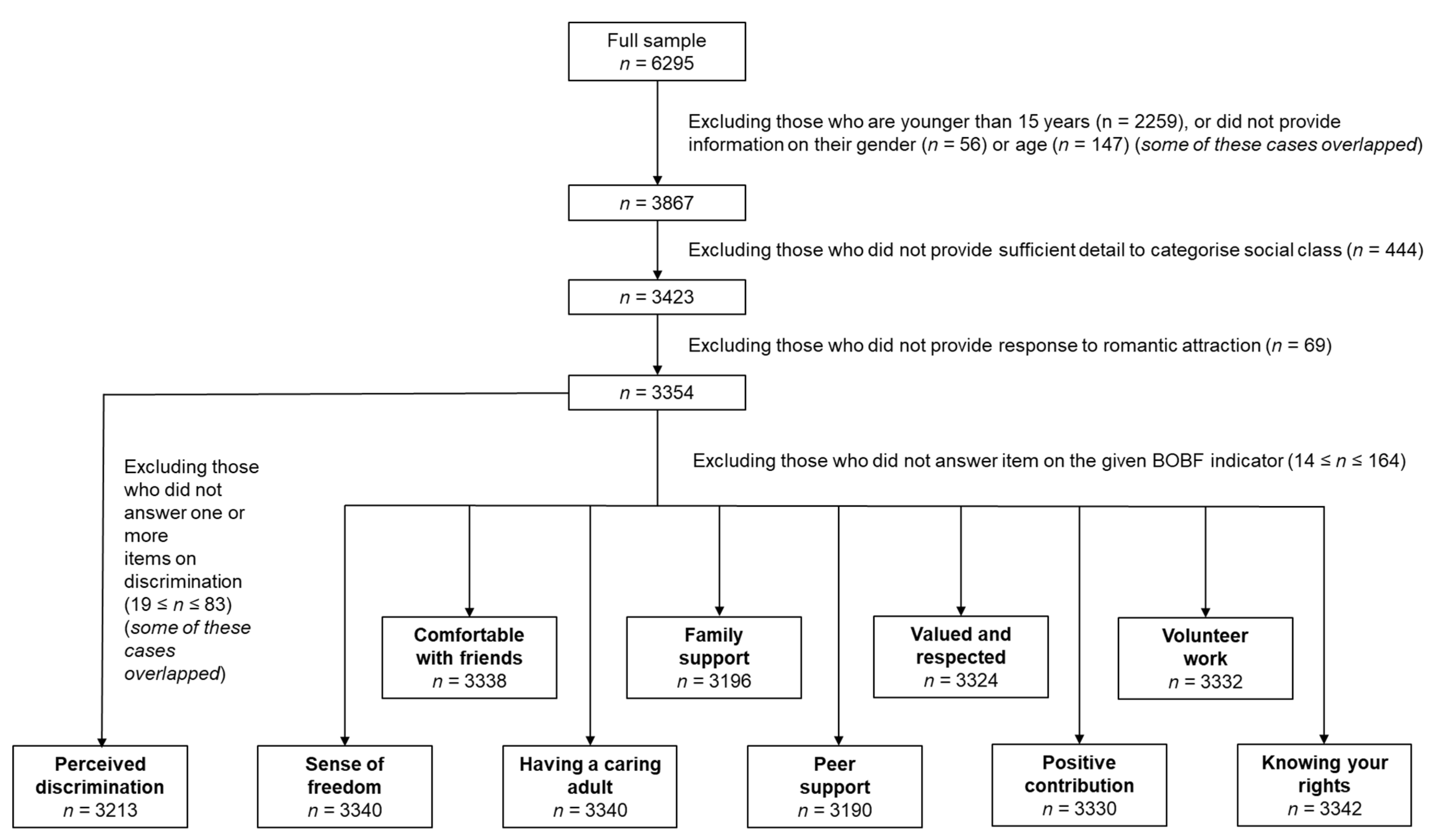
2.3. Sample
2.4. Analytic Approach
3. Results
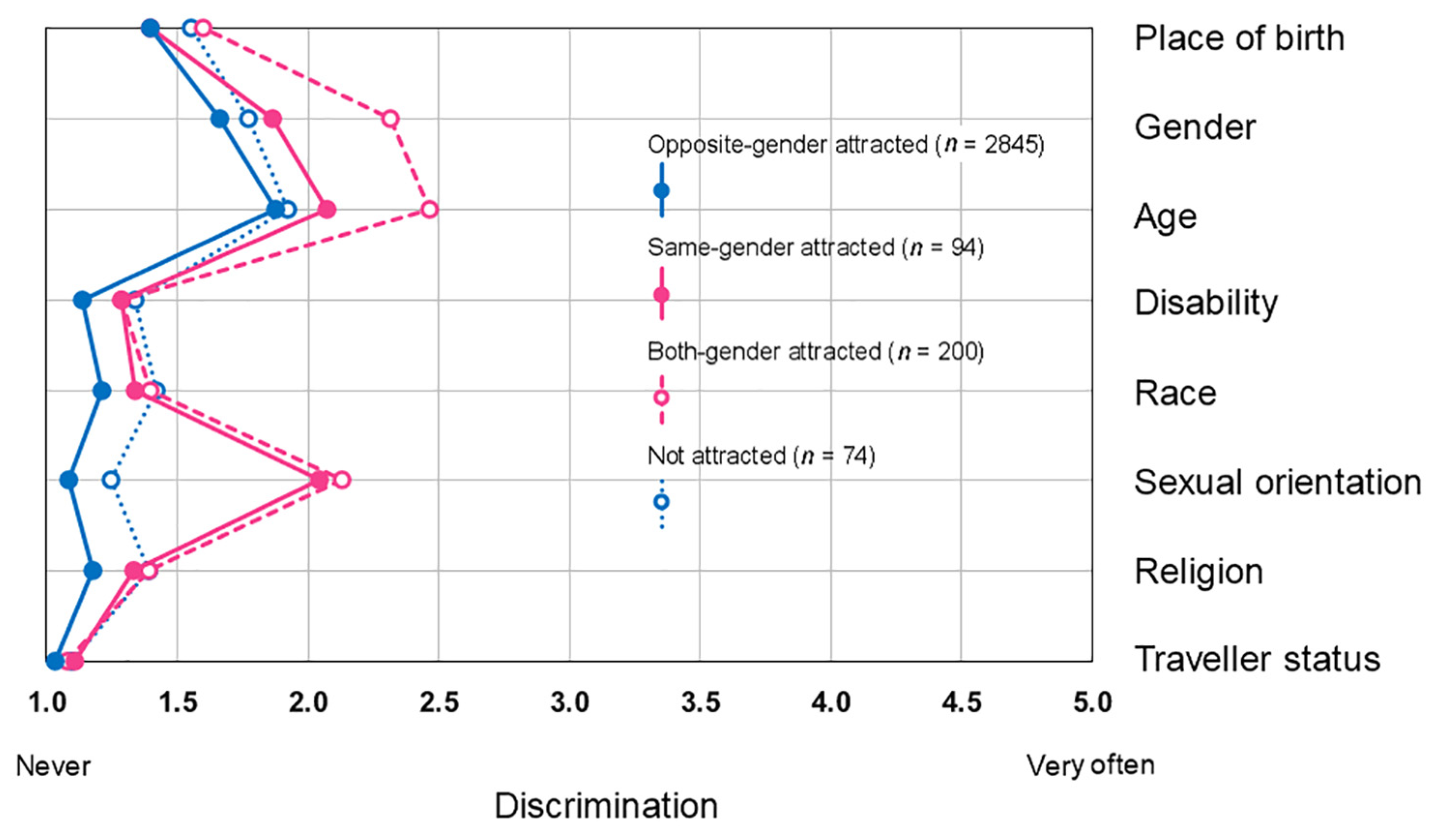
3.1. Descriptive Findings: Discrimination
3.2. Descriptive Findings: Positive BOBF Outcome 5 Variables
3.3. Comparing Sexual Minority and Non-Minority Youth: Discrimination
3.4. Comparing Sexual Minority and Non-Minority Youth: Positive BOBF Outcome 5 Variables
4. Discussion
4.1. Descriptive Findings: Gender and Social Class Have a Moderate Role
4.2. Better Outcomes, Brighter Futures in Sexual Minority Adolescents: Discrimination, Resilience, and Social Agency
4.3. Limitations and Strengths
4.4. Implications for Practice, Policy, and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Keleher, C.; MacDougall, C. Determinants of health. In Understanding Health, 4th ed.; Keleher, C., MacDougall, C., Eds.; Oxford University Press: South Melbourne, Australia, 2016; pp. 19–34. [Google Scholar]
- Baum, F.E.; Begin, M.; Houweling, T.A.; Taylor, S. Changes not for the fainthearted: Reorienting health care systems toward health equity through action on the social determinants of health. Am. J. Public Health 2009, 99, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- McCoy, D.; Sanders, D.; Baum, F.; Narayan, T.; Legge, D. Pushing the international health research agenda towards equity and effectiveness. Lancet 2004, 364, 1630–1631. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Bronfenbrenner, U. Interacting systems in human development. Research paradigms: Present and future. In Persons in Contexts: Developmental Processes; Bolger, N., Caspi, A., Downey, C., Moorehouse, M., Eds.; Cambridge University Press: Cambridge, UK, 1988; pp. 25–49. [Google Scholar]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Borraccino, A.; Berchialla, P.; Dalmasso, P.; Sciannameo, V.; Vieno, A.; Lazzeri, G.; Charrier, L.; Lemma, P. Connectedness as a protective factor in immigrant youth: Results from the Health Behaviours in School-aged Children (HBSC) Italian study. Int. J. Public Health 2020, 65, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.S.; Saucier, D.A.; Hafner, E. Meta-analysis of the relationships between social support and well-being in children and adolescents. J. Soc. Clin. Psychol. 2010, 29, 624–645. [Google Scholar] [CrossRef]
- García-Moya, I.; Brooks, F.M.; Spencer, N.H. School-level factors associated with teacher connectedness: A multilevel analysis of the structural and relational school determinants of young people’s health. J. Public Health 2018, 40, 366–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erol, R.Y.; Orth, U. Self-esteem development from age 14 to 30 years: A longitudinal study. J. Personal. Soc. Psychol. 2011, 101, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Veselska, Z.; Geckova, A.M.; Orosova, O.; Gajdosova, B.; van Dijk, J.P.; Reijneveld, S.A. Self-esteem and resilience: The connection with risky behavior among adolescents. Addict. Behav. 2009, 34, 287–291. [Google Scholar] [CrossRef] [Green Version]
- Ballard, P.J.; Syme, S.L. Engaging youth in communities: A framework for promoting adolescent and community health. J. Epidemiol. Community Health 2016, 70, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Csikszentmihalyi, M. Applications of Flow in Human Development and Education: The Collected Works of Mihaly Csikszentmihalyi; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar] [CrossRef]
- Molcho, M.; Kelly, C.; Gavin, A.; Nic Gabhainn, S. Inequalities in Health among School-Aged Children in Ireland; Department of Health and Children: Dublin, Ireland, 2008. Available online: http://www.nuigalway.ie/hbsc/documents/healthinequalities_1.pdf (accessed on 4 March 2020).
- Meyer, I.H. Prejudice and discrimination as social stressors. In The Health of Sexual Minorities: Public Health Perspectives on Lesbian, Gay, Bisexual and Transgender Populations; Meyer, I.H., Northridge, M.E., Eds.; Springer Science+Business Media: New York, NY, USA, 2007; pp. 242–267. [Google Scholar] [CrossRef]
- Pascoe, E.A.; Smart Richman, L. Perceived discrimination and health: A meta-analytic review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [Green Version]
- Majeno, A.; Tsai, K.M.; Huynh, V.W.; McCreath, H.; Fuligni, A.J. Discrimination and sleep difficulties during adolescence: The mediating roles of loneliness and perceived stress. J. Youth Adolesc. 2018, 47, 135–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burk, J.; Park, M.; Saewyc, E.M. A media-based school intervention to reduce sexual orientation prejudice and its relationship to discrimination, bullying, and the mental health of lesbian, gay, and bisexual adolescents in Western Canada: A population-based evaluation. Int. J. Environ. Res. Public Health 2018, 15, 2447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, M.L.; Way, N.; Pahl, K. Trajectories of perceived adult and peer discrimination among Black, Latino, and Asian American adolescents: Patterns and psychological correlates. Dev. Psychol. 2006, 42, 218–236. [Google Scholar] [CrossRef]
- Birkett, M.; Newcomb, M.E.; Mustanski, B. Does it get better? A longitudinal analysis of psychological distress and victimization in lesbian, gay, bisexual, transgender, and questioning youth. J. Adolesc. Health 2015, 56, 280–285. [Google Scholar] [CrossRef] [Green Version]
- DCYA. Better Outcomes Brighter Futures: The National Policy Framework for Children and Young People 2014–2020; Department of Children and Youth Affairs: Dublin, Ireland, 2014. Available online: https://www.dcya.gov.ie/documents/cypp_framework/BetterOutcomesBetterFutureReport.pdf (accessed on 4 March 2020).
- DCYA. An Indicator Set for Better Outcomes Brighter Futures, the National Policy Framework for Children and Young People 2014–2020; Department of Children and Youth Affairs: Dublin, Ireland, 2017. Available online: https://www.gov.ie/pdf/?file=https://assets.gov.ie/27126/9b1f25ec7da348e6921373e7e91e1ae3.pdf#page=1 (accessed on 18 December 2020).
- Inchley, J.; Currie, D.; Budisavljevic, S.; Torsheim, T.; Jåstad, A.; Cosma, A.; Kelly, C.; Arnarsson, A.M.; Barnekow, V.; Weber, M.M. Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report. Volume 1. Key Findings; WHO Regional Office for Europe: Copenhagen, Denmark, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/332091/9789289055000-eng.pdf (accessed on 24 June 2020).
- CSO. Quarterly National Household Survey, Special Module on Equality; Central Statistics Office: Dublin, Ireland, 2015. Available online: https://www.cso.ie/en/releasesandpublications/er/q-eq/qnhsequalitymodulequarter32014/ (accessed on 18 December 2020).
- Williams, J.; Greene, S.; Doyle, E.; Harris, E.; Layte, R.; McCoy, S.; McCrory, C.; Murray, A.; Nixon, E.; O’Dowd, T.; et al. Growing Up in Ireland National Longitudinal Study of Children: The Lives of 9-Year-Olds; The Economic and Social Research Institute: Dublin, Ireland, 2009; Available online: https://www.esri.ie/system/files/media/file-uploads/2015-07/BKMNEXT154.pdf (accessed on 18 December 2020).
- McKeown, C.; Denner, S.; McAteer, S.; Shiel, G.; O’Keefe, L. Learning for the Future: The Performance of 15-Year-Olds in Ireland on Reading Literacy, Science and Mathematics in PISA 2018; Educational Research Centre: Dublin, Ireland, 2019; Available online: https://www.erc.ie/wp-content/uploads/2020/07/B23321-PISA-2018-National-Report-for-Ireland-Full-Report-Web-4.pdf (accessed on 27 December 2020).
- Bryan, A. Queer youth and mental health: What do educators need to know? Ir. Educ. Stud. 2017, 36, 73–89. [Google Scholar] [CrossRef]
- Bryan, A.; Mayock, P. Speaking back to dominant constructions of LGBT lives: Complexifying ‘at riskness’ for self-harm and suicidiality among lesbian, gay, bisexual and transgender youth. Ir. J. Anthr. 2012, 15, 8–15. [Google Scholar]
- Rasmussen, M.L. Becoming Subjects: Sexualities and Secondary Schooling; Routledge: New York, NY, USA, 2006. [Google Scholar] [CrossRef]
- Talburt, S.; Rasmussen, M.L. ‘After-queer’ tendencies in queer research. Int. J. Qual. Stud. Educ. 2010, 23, 1–14. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Pachankis, J.E. Stigma and minority stress as social determinants of health among lesbian, gay, bisexual, and transgender youth: Research evidence and clinical implications. Pediatr. Clin. N. Am. 2016, 63, 985–997. [Google Scholar] [CrossRef]
- Riggle, E.D.B.; Rostosky, S.S. A Positive View of LGBTQ: Embracing Identity and Cultivating Well-Being; Rowman & Littlefield Publishers, Inc.: Lanham, MD, USA, 2012. [Google Scholar]
- Wilson, C.; Cariola, L.A. LGBTQI+ youth and mental health: A systematic review of qualitative research. Adolesc. Res. Rev. 2020, 5, 187–211. [Google Scholar] [CrossRef] [Green Version]
- Saewyc, E.M. Research on adolescent sexual orientation: Development, health disparities, stigma and resilience. J. Res. Adolesc. 2011, 21, 256–272. [Google Scholar] [CrossRef] [Green Version]
- Bridge, L.; Smith, P.; Rimes, K.A. Sexual orientation differences in the self-esteem of men and women: A systematic review and meta-analysis. Psychol. Sex. Orientat. Gend. Divers. 2019, 6, 433–446. [Google Scholar] [CrossRef] [Green Version]
- Oren Pizmony-Levy; BeLonG To Youth Services. The 2019 School Climate Survey Report: The Experience of Lesbian, Gay, Bisexual and Trans Young People in Ireland’s Schools; BeLonG To Youth Services: Dublin, Ireland, 2019; Available online: http://belongto.org/wp-content/uploads/2019/11/BeLonG-To-School-Climate-Report-2019.pdf (accessed on 4 March 2020).
- Dooley, B.; O’Connor, C.; Fitzgerald, A.; O’Reilly, A. My World Survey 2: The National Study of Youth Mental Health in Ireland; UCD School of Psychology and Jigsaw: Dublin, Ireland, 2019; Available online: http://www.myworldsurvey.ie/content/docs/My_World_Survey_2.pdf (accessed on 4 March 2020).
- Reygan, F. The school-based lives of LGBT youth in the Republic of Ireland. J. Lgbt Youth 2009, 6, 80–89. [Google Scholar] [CrossRef]
- DCYA. LGBTI+ National Youth Strategy 2018–2020; Department of Children and Youth Affairs: Dublin, Ireland, 2018. Available online: https://www.gov.ie/en/publication/a6f110-lgbti-national-youth-strategy-2018-2020/ (accessed on 4 March 2020).
- Bowen, N. Needs Analysis of Young People Identifying as LGBT* in Co. Tipperary, Ireland. 2019. Available online: http://youthworktipperary.ie/wp-content/uploads/2019/02/LGBT-Needs-Analysis-2018-1.pdf (accessed on 4 March 2020).
- Mannix-McNamara, P.; O’Grady, E.; Devaney, E.; Jourdan, D. Tackling social and health inequalities: Vulnerability among the young lesbian, gay and bisexual population in Ireland. Psychol. Sex. 2013, 4, 268–282. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Cosma, A.; Samdal, O. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2017/18 Survey; Children and Adolescent Health Research Unit (CAHRU), University of St Andews: St Andrews, UK, 2018; Available online: http://www.hbsc.org/methods/ (accessed on 5 October 2020).
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Stangl, A.L.; Earnshaw, V.A.; Logie, C.H.; van Brakel, W.; Simbayi, L.C.; Barre, I.; Dovidio, J.F. The Health Stigma and Discrimination Framework: A global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. 2019, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L. How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychol. Bull. 2009, 135, 707–730. [Google Scholar] [CrossRef]
- Dürrbaum, T.; Sattler, F.A. Minority stress and mental health in lesbian, gay male, and bisexual youths: A meta-analysis. J. Lgbt Youth 2020, 17, 298–314. [Google Scholar] [CrossRef]
- Költő, A.; Gavin, A.; Molcho, M.; Kelly, C.; Walker, L.; Nic Gabhainn, S. The Irish Health Behaviour in School-aged Children (HBSC) study 2018; The Department of Health and Health Promotion Research Centre, National University of Ireland: Dublin, Ireland; Galway, Ireland, 2020; Available online: https://aran.library.nuigalway.ie/handle/10379/15675 (accessed on 9 June 2020).
- Jelsma, J.; Burgess, T.; Henley, L. Does the requirement of getting active consent from parents in school-based research result in a biased sample? An empirical study. J. Empir. Res. Hum. Res. Ethics 2012, 7, 56–62. [Google Scholar] [CrossRef]
- CSO. Census of Population 2016—Profile 11 Employment, Occupations and Industry; Central Statistics Office: Dublin, Ireland, 2016. Available online: https://www.cso.ie/en/releasesandpublications/ep/p-cp11eoi/cp11eoi/ioscs/ (accessed on 5 October 2020).
- Költő, A.; Young, H.; Burke, L.; Moreau, N.; Cosma, A.; Magnusson, J.; Windlin, B.; Reis, M.; Saewyc, E.M.; Godeau, E.; et al. Love and dating patterns for same- and both-gender attracted adolescents across Europe. J. Res. Adolesc. 2018, 28, 772–778. [Google Scholar] [CrossRef] [Green Version]
- Equal Status Act. Stationary Office: Dublin, Ireland. 2000. Available online: http://www.irishstatutebook.ie/eli/2000/act/8/enacted/en/print.html (accessed on 18 December 2020).
- Költő, A.; Harrington, A.; Kavanagh, A.; Tyrrell, L.; Nic Gabhainn, S. New Questions for the Health Behaviour in School-Aged Children (HBSC) Study in Ireland: Pilot 2018; Health Promotion Research Centre, National University of Ireland Galway: Galway, Ireland, 2018; Available online: http://www.nuigalway.ie/media/healthpromotionresearchcentre/hbscdocs/shortreports/2018---AK-HBSC-2018-PILOT-REPORT.pdf (accessed on 5 October 2020).
- Daniels, N.; Burke, L.; O’Donnell, A.; McGovern, O.; Kelly, C.; D’Eath, M.; Nic Gabhainn, S. Expanding the role of young people in research: Towards a better understanding of their lives. Zdr. Publiczne I Zarz. 2014, 12, 36–44. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Costa, P.T.; McCrae, R.R. NEO Personality Inventory-Revised; Psychological Assessment Resources: Odessa, FL, USA, 1992; Available online: https://www.parinc.com/Products/Pkey/276 (accessed on 27 December 2020).
- Carver, S.S.; Scheier, M.F. Perspectives on Personality, 7th ed.; Pearson Education Ltd.: Harlow, UK, 2014. [Google Scholar]
- Turan, J.M.; Elafros, M.A.; Logie, C.H.; Banik, S.; Turan, B.; Crockett, K.B.; Pescosolido, B.; Murray, S.M. Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Med. 2019, 17, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- North, M.S.; Fiske, S.T. An inconvenienced youth? Ageism and its potential intergenerational roots. Psychol. Bull. 2012, 138, 982–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, H.D. Gender, grade, and relationship differences in emotional closeness within adolescent friendships. Adolescence 2004, 39, 243–255. [Google Scholar]
- Kelly, L.L. A snapchat story: How black girls develop strategies for critical resistance in school. Learn. Media Technol. 2018, 43, 374–389. [Google Scholar] [CrossRef]
- Flanagan, C.A.; Bowes, J.M.; Jonsson, B.; Csapo, B.; Sheblanova, E. Ties that bind: Correlates of adolescents’ civic commitments in seven countries. J. Soc. Issues 1998, 54, 457–475. [Google Scholar] [CrossRef]
- Moore, C.W.; Allen, J.P. The effects of volunteering on the young volunteer. J. Prim. Prev. 1996, 17, 231–258. [Google Scholar] [CrossRef]
- Marta, E.; Pozzi, M. Young people and volunteerism: A model of sustained volunteerism during the transition to adulthood. J. Adult Dev. 2008, 15, 35. [Google Scholar] [CrossRef]
- Kawachi, I.; Subramanian, S.; Kim, D. Social capital and health: A decade of progress and beyond. In Social Capital and Health, Kawachi, I., Subramanian, S., Kim, D., Eds.; Springer: New York, NY, USA, 2008; pp. 1–26. [Google Scholar] [CrossRef]
- Romijnders, K.A.; Wilkerson, J.M.; Crutzen, R.; Kok, G.; Bauldry, J.; Lawler, S.M. Strengthening social ties to increase confidence and self-esteem among sexual and gender minority youth. Health Promot. Pract. 2017, 18, 341–347. [Google Scholar] [CrossRef]
- Burton, C.L.; Wang, K.; Pachankis, J.E. Psychotherapy for the spectrum of sexual minority stress: Application and technique of the ESTEEM treatment model. Cogn. Behav. Pract. 2019, 26, 285–299. [Google Scholar] [CrossRef]
- Craney, R.S.; Watson, L.B.; Brownfield, J.; Flores, M.J. Bisexual women’s discriminatory experiences and psychological distress: Exploring the roles of coping and LGBTQ community connectedness. Psychol. Sex. Orientat. Gend. Divers. 2018, 5, 324–337. [Google Scholar] [CrossRef]
- Geary, R.S.; Tanton, C.; Erens, B.; Clifton, S.; Prah, P.; Wellings, K.; Mitchell, K.R.; Datta, J.; Gravningen, K.; Fuller, E.; et al. Sexual identity, attraction and behaviour in Britain: The implications of using different dimensions of sexual orientation to estimate the size of sexual minority populations and inform public health interventions. PLoS ONE 2018, 13, e0189607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takács, J.; Mocsonaki, L.; P. Tóth, T. Social Exclusion of Lesbian, Gay, Bisexual and Transgender (LGBT) People in Hungary; Institute of Sociology, Hungarian Academy of Sciences: Budapest, Hungary, 2008; Available online: http://hatter.hu/sites/default/files/dokumentum/kiadvany/kutatas2007-angol.pdf (accessed on 4 March 2020).
- Drummond, R.J.; Jones, K.D. Assessment Procedures for Counselors and Helping Professionals; Pearson: Upper Saddle Riveer, NJ, USA, 2010. [Google Scholar]
- Thorndike, E.L. A constant error in psychological ratings. J. Appl. Psychol. 1920, 4, 25–29. [Google Scholar] [CrossRef] [Green Version]
- La Greca, A.M.; Mackey, E.R. Adolescents’ anxiety in dating situations: The potential role of friends and romantic partners. J. Clin. Child. Adolesc. Psychol. 2007, 36, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Corliss, H.L.; Rosario, M.; Birkett, M.A.; Newcomb, M.E.; Buchting, F.O.; Matthews, A.K. Sexual orientation disparities in adolescent cigarette smoking: Intersections with race/ethnicity, gender, and age. Am. J. Public Health 2014, 104, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, B.A.; Turner, B.C.; Beach, L.B.; Korpak, A.K.; Phillips, G. Racial/ethnic differences in mental health, substance use, and bullying victimization among self-identified bisexual high school-aged youth. Lgbt Health 2019, 6, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Blais, M.; Bergeron, F.A.; Duford, J.; Boislard, M.A.; Hébert, M. Health outcomes of youth sexual-minorities in Canada: An overview. Adolesc. E Saude 2015, 12, 53–73. [Google Scholar]
- Költő, A.; Cosma, A.; Young, H.; Moreau, N.; Pavlova, D.; Tesler, R.; Thorsteinsson, E.B.; Vieno, A.; Saewyc, E.M.; Nic Gabhainn, S. Romantic attraction and substance use in 15-year-old adolescents from eight European countries. Int. J. Environ. Res. Public Health 2019, 16, 3063. [Google Scholar] [CrossRef] [Green Version]
- Költő, A.; Cosma, A.; Moreau, N.; Young, H.; Thorsteinsson, E.B.; Gobina, I.; Godeau, E.; Saewyc, E.M.; Nic Gabhainn, S. Self-reported health and patterns of romantic love in adolescents from eight European countries and regions. Lgbt Health 2020, 7, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Russell, S.T. Bisexuality and adolescence. J. Bisexuality 2011, 11, 434–438. [Google Scholar] [CrossRef]
- Bostwick, W.; Hequembourg, A. ‘Just a little hint’: Bisexual-specific microaggressions and their connection to epistemic injustices. Cult. Health Sex. 2014, 16, 488–503. [Google Scholar] [CrossRef]
- Poteat, T.; Stahlman, S. Global health/LGBTQ health. In LGBTQ Health Research: Theory, Methods, Practice; Stall, R., Dodge, B., Bauermeister, J.A., Poteat, T., Beyrer, C., Eds.; Johns Hopkins University Press: Baltimore, MD, USA, 2020; pp. 37–48. [Google Scholar]
- Flores, A.R. Social Acceptance of LGBT People in 174 Countries, 1981 to 2017; The Williams Institute: Los Angeles, CA, USA, 2019; Available online: https://williamsinstitute.law.ucla.edu/wp-content/uploads/GAI-Update-Oct-2019.pdf (accessed on 4 March 2020).
- Doan Van, E.E.; Mereish, E.H.; Woulfe, J.M.; Katz-Wise, S.L. Perceived discrimination, coping mechanisms, and effects on health in bisexual and other non-monosexual adults. Arch. Sex. Behav. 2019, 48, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Költő, A.; Vaughan, E.; Ravikumar, D.; Kelly, C.; O’Sullivan, L.; Saewyc, E.; Nic Gabhainn, S. Pre-Registered Protocol for the LGBTI+ Two Phased Study: A Landscape and Knowledge Gap Analysis of Research Conducted on Sexual and Gender Minority Youth in Ireland and Europe; Department of Children and Youth Affairs, National University of Ireland Galway: Galway, Ireland; Dublin, Ireland, 2019; Available online: https://osf.io/46q8f (accessed on 27 December 2020).
- Carolan, F.; Redmond, S. The Needs of Young People in Northern Ireland Who Identify as Lesbian, Gay, Bisexual and/or Transgender; YouthNet: Belfast, UK, 2003; Available online: http://archive.belongto.org/attachments/233_shOUT_Main_Report.pdf (accessed on 4 March 2020).
- Schubotz, D. Young Life and Times Survey, 2017. Dataset. SN: 8422; UK Data Service: Colchester, UK, 2017; Available online: https://beta.ukdataservice.ac.uk/datacatalogue/doi/?id=8422#!#1 (accessed on 27 December 2020).
- Neill, G.; Meehan, D. Still Shouting: The Needs and Experiences of Young People in Northern Ireland Who Identify as Lesbian, Gay, Bisexual and/or Transgender (LGBT); Cara-Friend and YouthAction: Belfast, Northern Ireland, 2017; Available online: https://cara-friend.org.uk/wp-content/uploads/2018/08/Still-Shouting-2017.pdf (accessed on 4 March 2020).
- Blackburn, M.V.; McCready, L.T. Voices of queer youth in urban schools: Possibilities and limitations. Theory Into Pract. 2009, 48, 222–230. [Google Scholar] [CrossRef]
- Mayock, P.; Bryan, A.; Carr, N.; Kitching, K. Supporting LGBT Lives in Ireland: A Study of the Mental Health and Well-Being of Lesbian, Gay, Bisexual and Transgender People: Policy Report; GLEN & BeLonG To Youth Services: Dublin, Ireland, 2009; Available online: https://www.hse.ie/eng/services/publications/mentalhealth/suporting-lgbt-lives.pdf (accessed on 4 March 2020).
- Kulkin, H.S. Factors enhancing adaptive coping and mental health in lesbian youth: A review of the literature. J. Homosex. 2006, 50, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, M.D.; Waehler, C.A. Coming out growth: Conceptualizing and measuring stress-related growth associated with coming out to others as a sexual minority. J. Adult Dev. 2010, 17, 94–109. [Google Scholar] [CrossRef]
- Johns, M.M.; Liddon, N.; Jayne, P.E.; Beltran, O.; Steiner, R.J.; Morris, E. Systematic mapping of relationship-level protective factors and sexual health outcomes among sexual minority youth: The role of peers, parents, partners, and providers. LGBT Health 2018, 5, 6–32. [Google Scholar] [CrossRef]
- ILGA-Europe. 10th Rainbow Map. Reflecting the Legal and Policy Human Rights Situation of Lesbian, Gay, Bisexual, Trans and Intersex (LGBTI) People in Europe. 2019. Available online: https://www.ilga-europe.org/sites/default/files/Attachments/rainbowmap2019online_0_0.pdf (accessed on 4 March 2020).
- Crenshaw, K. Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanf. Law Rev. 1991, 43, 1241–1300. [Google Scholar] [CrossRef]
- European Commission. Union of Equality: LGBTIQ Equality Strategy 2020–2025; Publications Office of the European Union: Brussels, Belgium, 2020; Available online: https://ec.europa.eu/info/sites/info/files/lgbtiq_strategy_2020-2025_en.pdf (accessed on 28 December 2020).
- Jones, T. Re-doing research: Best practices for asking about gender and sexuality in education studies. In Uplifting Gender and Sexuality Education Research; Jones, T., Coll, L., van Leent, L., Taylor, Y., Eds.; Palgrave Macmillan: Cham, Switzerland, 2019; pp. 185–230. [Google Scholar] [CrossRef]
- Marshall, D. Popular culture, the ‘victim’ trope and queer youth analytics. Int. J. Qual. Stud. Educ. 2010, 23, 65–85. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| BOBF: Aims under Outcome 5 | BOBF: Indicator Areas | Data Sources | HBSC Indicators (Items and Response Options) | HBSC Indicators (Variables and Coding) |
|---|---|---|---|---|
| Aim 5.1: Sense of own identity, free from discrimination | Discrimination and stigmatization |
| How often are you treated unfairly or negatively... a
| Continuous variables/Discrimination profiles:
|
| Experience of sense of freedom |
| In general, do you feel you have freedom in your life? a 1 (Not at all)/2/3/4 (Very much) | Dichotomous variable (1 = Very much, 0 = Less than very much) | |
| Peer acceptance and respect |
| Do you feel comfortable being yourself while with your friends? b Always/Often/Sometimes/Never | Dichotomous variable (1 = Always, 0 = Less often than always) | |
| Aim 5.2: Part of positive networks of friends, family, and community | Having at least one caring and consistent adult to confide in |
| In general, do you have a caring adult you can tell anything to? a 1 (Not at all)/2/3/4 (Very much) | Dichotomous variable (1 = Very much, 0 = Less than very much) |
| Positive parent and family relationships |
| MSPSS, Family subscale c
| Scores ≥ 5.5 indicate high family support [42] (1 = High family support, 0 = Low family support) | |
| Positive relationships with peers |
| MSPSS, Friends subscale c
| Scores ≥ 5.5 indicate high peer support [42] (1 = High peer support, 0 = Low peer support) | |
| Perceptions of being valued and respected |
| In general, do you feel you are valued and respected? a 1 (Not at all)/2/3/4 (Very much) | Dichotomous variable (1 = Very much, 0 = Less than very much) | |
| Aim 5.3: Civically engaged, socially and environmentally conscious | Belief in being able to make a positive contribution to the world |
| In general, do you feel that you make a positive contribution to the world? a 1 (Not at all)/2/3/4 (Very much) | Dichotomous variable (1 = Very much, 0 = Less than very much) |
| Volunteering and altruism |
| In general, do you take part in volunteer work? a 1 (Not at all)/2/3/4 (Very much) | Dichotomous variable (1 = Very much, 0 = Less than very much) | |
| 18–24-year-olds who vote in local, regional, national, or European elections and referenda |
| – | – | |
| Aim 5.4: Aware of rights, responsible and respectful of the law | Children and young people’ awareness of their own rights |
| In general, do you know your rights as a young person? a 1 (Not at all)/2/3/4 (Very much) | Dichotomous variable (1 = Very much, 0 = Less than very much) |
| Respect for laws and the judicial process |
| – | – | |
| Perception of fairness of the law |
| – | – |
| Sociodemographic Variables | Discrimination Based on | |||||||
|---|---|---|---|---|---|---|---|---|
| Birth-Place a | Gender | Age | Disability | Race | Sexual Orientation | Religion | Traveller Status | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
| Gender | ||||||||
| Boy (n = 1446) | 1.45 (0.86) | 1.34 (0.75) | 1.62 (0.96) | 1.17 (0.61) | 1.24 (0.73) | 1.17 (0.65) | 1.19 (0.65) | 1.06 (0.37) |
| Girl (n = 1767) | 1.38 (0.82) | 2.01 (1.08) | 2.16 (1.15) | 1.14 (0.53) | 1.23 (0.71) | 1.19 (0.64) | 1.20 (0.64) | 1.02 (0.25) |
| Difference p | 0.024 | <0.001 | <0.001 | 0.076 | 0.674 | 0.521 | 0.600 | 0.006 |
| Difference rES b | 0.040 | 0.336 | 0.246 | < 0.001 | <0.001 | <0.001 | <0.001 | 0.048 |
| Social class | ||||||||
| High (n = 1797) | 1.37 (0.79) | 1.73 (1.00) | 1.93 (1.10) | 1.14 (0.55) | 1.23 (0.71) | 1.15 (0.57) | 1.21 (0.66) | 1.03 (0.25) |
| Med. (n = 1103) | 1.44 (0.87) | 1.70 (1.02) | 1.93 (1.13) | 1.17 (0.60) | 1.22 (0.71) | 1.23 (0.74) | 1.18 (0.62) | 1.05 (0.37) |
| Low (n = 313) | 1.53 (0.97) | 1.63 (0.97) | 1.84 (1.03) | 1.15 (0.54) | 1.28 (0.80) | 1.17 (0.69) | 1.20 (0.63) | 1.06 (0.40) |
| Difference p | 0.002 | 0.265 | 0.379 | 0.423 | 0.345 | 0.004 | 0.518 | 0.027 |
| Difference ω2 c | 0.003 | <0.001 | <0.001 | <0.001 | <0.001 | 0.003 | <0.001 | 0.002 |
| Sociodemographic Variables and Romantic Attraction | Freedom in Your Life, % (n) | Comfortable with Friends, % (n) | Having a Caring Adult, % (n) | High Family Support, % (n) | High Peer Support, % (n) | Feeling Valued and Respected, % (n) | Making a Positive Contribution, % (n) | Taking Part in Volunteering, % (n) | Knowing Your Rights, % (n) |
|---|---|---|---|---|---|---|---|---|---|
| Overall sample | |||||||||
| Total n | 3340 | 3338 | 3340 | 3196 | 3190 | 3324 | 3330 | 3332 | 3342 |
| Positive answer | 23.1% (772) | 67.3% (2246) | 56.7% (1895) | 56.4% (1802) | 59.3% (1892) | 36.2% (1203) | 21.2% (706) | 11.5% (384) | 26.3% (880) |
| Gender | |||||||||
| Boy | 24.5% (367) | 68.5% (1023) | 54.1% (810) | 57.7% (820) | 50.0% (703) | 36.0% (537) | 23.6% (352) | 10.0% (149) | 26.6% (399) |
| Girl | 22.0% (405) | 66.3% (1223) | 58.9% (1085) | 55.3% (982) | 66.7% (1189) | 36.3% (666) | 19.2% (354) | 12.8% (235) | 26.1% (481) |
| Association p | 0.094 | 0.172 | 0.005 | 0.177 | <0.001 | 0.870 | 0.002 | 0.011 | 0.719 |
| Association V a | 0.029 | 0.024 | 0.048 | 0.024 | 0.169 | 0.003 | 0.053 | 0.044 | 0.006 |
| Social class | |||||||||
| High | 23.4% (437) | 65.8% (1231) | 56.7% (1062) | 59.0% (1059) | 59.8% (1066) | 36.9% (688) | 21.9% (409) | 11.9% (223) | 25.8% (483) |
| Medium | 21.8% (250) | 71.1% (815) | 55.9% (639) | 53.2% (583) | 59.4% (657) | 35.5% (404) | 20.4% (233) | 11.3% (129) | 27.6% (316) |
| Low | 26.3% (85) | 62.7% (200) | 60.1% (194) | 52.5% (160) | 56.3% (169) | 34.4% (111) | 19.9% (64) | 9.9% (32) | 25.2% (81) |
| Association p | 0.222 | 0.002 | 0.403 | 0.004 | 0.535 | 0.578 | 0.532 | 0.562 | 0.474 |
| Association V | 0.030 | 0.061 | 0.023 | 0.059 | 0.020 | 0.018 | 0.019 | 0.019 | 0.021 |
| Romantic attraction | |||||||||
| Opposite-gender attracted | 23.7% (699) | 68.5% (2020) | 58.0% (171) | 57.8% (1634) | 60.0% (1689) | 37.6% (1105) | 21.5% (632) | 11.1% (326) | 26.1% (771) |
| Same-gender attracted | 17.2% (17) | 65.0% (65) | 49.0% (49) | 48.9% (46) | 60.8% (59) | 30.3% (30) | 23.2% (23) | 21.0% (21) | 35.0% (35) |
| Both-gender attracted | 18.6% (39) | 56.3% (117) | 43.5% (91) | 42.6% (86) | 54.0% (109) | 20.5% (43) | 14.9% (31) | 13.9% (29) | 26.2% (55) |
| Not attracted | 21.3% (17) | 55.7% (44) | 53.8% (43) | 48.0% (36) | 44.9% (35) | 31.3% (25) | 25.0% (20) | 10.0% (8) | 23.8% (19) |
| Association p | 0.164 | <0.001 | <0.001 | <0.001 | 0.020 | <0.001 | 0.111 | 0.013 | 0.239 |
| Association V | 0.039 | 0.074 | 0.076 | 0.084 | 0.056 | 0.091 | 0.042 | 0.057 | 0.036 |
| Means, Medians and Comparison Across Romantic Attraction | Discrimination Based on… | |||||||
|---|---|---|---|---|---|---|---|---|
| Birthplace a | Gender | Age | Disability | Race | Sexual Orientation | Religion | Traveller Status | |
| Romantic attraction: Means | M (SE) | M (SE) | M (SE) | M (SE) | M (SE) | M (SE) | M (SE) | M (SE) |
| Opposite-gender attracted | 1.39 (0.02) | 1.66 (0.02) | 1.88 (0.02) | 1.13 (0.01) | 1.21 (0.01) | 1.08 (0.01) | 1.18 (0.01) | 1.03 (0.01) |
| Same-gender attracted | 1.39 (0.09) | 1.86 (0.10) | 2.07 (0.11) | 1.29 (0.06) | 1.34 (0.07) | 2.04 (0.06) | 1.33 (0.07) | 1.11 (0.03) |
| Both-gender attracted | 1.60 (0.06) | 2.32 (0.07) | 2.47 (0.08) | 1.29 (0.04) | 1.40 (0.05) | 2.13 (0.04) | 1.39 (0.05) | 1.08 (0.02) |
| Not attracted | 1.55 (0.10) | 1.77 (0.12) | 1.92 (0.13) | 1.34 (0.07) | 1.42 (0.08) | 1.24 (0.07) | 1.39 (0.07) | 1.10 (0.04) |
| Romantic attraction: Medians | Median | Median | Median | Median | Median | Median | Median | Median |
| Opposite-gender attracted | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Same-gender attracted | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 |
| Both-gender attracted | 1 | 2 | 2 | 1 | 1 | 2 | 1 | 1 |
| Not attracted | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Comparison of means | ||||||||
| Kruskal–Wallis χ2 (df = 3) | 16.776 | 72.511 | 44.975 | 18.829 | 18.821 | 705.610 | 39.146 | 2.655 |
| Kruskal–Wallis p | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.448 |
| Parametric F (df = 3) | 4.564 | 28.048 | 18.805 | 9.056 | 6.724 | 281.405 | 10.679 | 3.877 |
| Parametric p | 0.003 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.009 |
| Effect size ω2 | 0.003 | 0.025 | 0.016 | 0.007 | 0.005 | 0.207 | 0.009 | 0.003 |
| Statistical power | 0.888 | ~1.000 | ~1.000 | 0.996 | 0.976 | ~1.000 | 0.999 | 0.827 |
| Pairwise comparison (p < 0.05) | BGA > OGA | BGA > OGA, BGA > SGA, BGA > NA | BGA > OGA, BGA > SGA, BGA > NA | BGA > OGA, NA > OGA | BGA > OGA | SGA > OGA, BGA > OGA, SGA > NA, BGA > NA | BGA > OGA, NA > OGA | – |
| Positive BOBF Indicators | n | OR | p | 95% CI |
|---|---|---|---|---|
| Freedom in your life | 3340 | |||
| Opposite-gender attracted | 2951 | 1 a | ||
| Same-gender attracted | 99 | 0.73 | 0.150 | 0.47–1.12 |
| Both-gender attracted | 210 | 0.78 | 0.101 | 0.59–1.05 |
| Not attracted | 80 | 0.90 | 0.618 | 0.59–1.38 |
| Comfortable while being with friends | 3338 | |||
| Opposite-gender attracted | 2951 | 1 | ||
| Same-gender attracted | 100 | 0.95 | 0.487 | 0.82–1.10 |
| Both-gender attracted | 208 | 0.82 | 0.002 | 0.73–0.93 |
| Not attracted | 79 | 0.81 | 0.041 | 0.67–0.99 |
| Having a caring adult | 3340 | |||
| Opposite-gender attracted | 2951 | 1 | ||
| Same-gender attracted | 100 | 0.85 | 0.102 | 0.69–1.03 |
| Both-gender attracted | 209 | 0.75 | <0.001 | 0.64–0.88 |
| Not attracted | 80 | 0.93 | 0.467 | 0.75–1.14 |
| High family support | 3196 | |||
| Opposite-gender attracted | 2825 | 1 | ||
| Same-gender attracted | 94 | 0.85 | 0.117 | 0.69–1.04 |
| Both-gender attracted | 202 | 0.74 | <0.001 | 0.63–0.87 |
| Not attracted | 75 | 0.83 | 0.124 | 0.65–1.05 |
| High peer support | 3190 | |||
| Opposite-gender attracted | 2813 | 1 | ||
| Same-gender attracted | 97 | 1.01 | 0.876 | 0.86–1.19 |
| Both-gender attracted | 202 | 0.90 | 0.110 | 0.79–1.02 |
| Not attracted | 78 | 0.75 | 0.021 | 0.58–0.96 |
| Feeling valued and respected | 3324 | |||
| Opposite-gender attracted | 2935 | 1 | ||
| Same-gender attracted | 99 | 0.81 | 0.159 | 0.60–1.09 |
| Both-gender attracted | 210 | 0.54 | <0.001 | 0.42–0.71 |
| Not attracted | 80 | 0.83 | 0.266 | 0.60–1.15 |
| Making a positive contribution | 3330 | |||
| Opposite-gender attracted | 2943 | 1 a | ||
| Same-gender attracted | 99 | 1.08 | 0.672 | 0.75–1.56 |
| Both-gender attracted | 208 | 0.69 | 0.031 | 0.50–0.97 |
| Not attracted | 80 | 1.16 | 0.440 | 0.79–1.71 |
| Taking part in volunteer work | 3332 | |||
| Opposite-gender attracted | 2943 | 1 | ||
| Same-gender attracted | 100 | 1.90 | 0.001 | 1.28–2.81 |
| Both-gender attracted | 209 | 1.25 | 0.211 | 0.88–1.78 |
| Not attracted | 80 | 0.90 | 0.763 | 0.46–1.76 |
| Knowing your rights | 3342 | |||
| Opposite-gender attracted | 2952 | 1 a | ||
| Same-gender attracted | 100 | 1.34 | 0.036 | 1.02–1.76 |
| Both-gender attracted | 210 | 1.00 | 0.982 | 0.79–1.27 |
| Not attracted | 80 | 0.91 | 0.639 | 0.61–1.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Költő, A.; Gavin, A.; Vaughan, E.; Kelly, C.; Molcho, M.; Nic Gabhainn, S. Connected, Respected and Contributing to Their World: The Case of Sexual Minority and Non-Minority Young People in Ireland. Int. J. Environ. Res. Public Health 2021, 18, 1118. https://doi.org/10.3390/ijerph18031118
Költő A, Gavin A, Vaughan E, Kelly C, Molcho M, Nic Gabhainn S. Connected, Respected and Contributing to Their World: The Case of Sexual Minority and Non-Minority Young People in Ireland. International Journal of Environmental Research and Public Health. 2021; 18(3):1118. https://doi.org/10.3390/ijerph18031118
Chicago/Turabian StyleKöltő, András, Aoife Gavin, Elena Vaughan, Colette Kelly, Michal Molcho, and Saoirse Nic Gabhainn. 2021. "Connected, Respected and Contributing to Their World: The Case of Sexual Minority and Non-Minority Young People in Ireland" International Journal of Environmental Research and Public Health 18, no. 3: 1118. https://doi.org/10.3390/ijerph18031118
APA StyleKöltő, A., Gavin, A., Vaughan, E., Kelly, C., Molcho, M., & Nic Gabhainn, S. (2021). Connected, Respected and Contributing to Their World: The Case of Sexual Minority and Non-Minority Young People in Ireland. International Journal of Environmental Research and Public Health, 18(3), 1118. https://doi.org/10.3390/ijerph18031118